
Abstract
With the trend away from long-term psychiatric hospitalization, rates of repeated admission to inpatient care have increased [1], [2]. Although inpatient care is indicated when patients can no longer be managed safely or treated appropriately in the community, hospitalization is costly, resource intensive and entails risks such as the exposure to violence [3], the contagious effects of illness-related behaviours such as deliberate self-harm [4] and the development of institutional dependence [5]. Consequently, a substantial body of research has developed to identify variables associated with or predictive of readmission, with a view to informing the development of interventions intended to reduce the incidence of rehospitalization. However, in contrast to an extensive adult readmission literature, relatively few studies have focused on adolescents.
Three recent studies contribute to an emerging literature examining factors predicting readmission in an adolescent population. First, in a study which examined factors related to psychiatric readmission among children and adolescents in state custody, Romansky et al. [2] concluded that ‘enabling factors’ such as posthospital service hours and living arrangements were important predictors of rehospitalization. The authors suggest that prevention of readmission in this population should focus on the provision of ‘sophisticated and comprehensive’ community services. Second, in a 10-year follow-up of patients initially hospitalized between the ages of 12 and 19 years, Arnold et al. [6] found that rehospitalization was predicted by younger age and the presence of an affective disorder at the index admission. Further, the authors suggest that clinicians should examine the risk of rehospitalization before discharge, especially for patients with these risk factors. Finally, Enns et al. [7] examined personality predictors of outcome for adolescents hospitalized with suicidal ideation, and found that severity of baseline suicidal ideation and the personality trait of neuroticism were predictive of readmission within 1 year of discharge.
These studies notwithstanding, there are substantial gaps in the literature pertaining to psychiatric readmission during adolescence. In particular, it is not yet clear as to what extent the factors associated with adult readmissions, such as medication non-adherence and substance abuse [1],[8–10], apply to adolescents and what developmental factors might be associated with adolescent readmissions in contradistinction to adults. As a result, it is unclear how to reduce the risk of rehospitalization for adolescents, which is of concern given that in our experience the rate of readmission among adolescents between 16 and 18 years old is quite high.
The Youth Inpatient Unit (YIU), located in Christchurch, New Zealand, is an eight-bed tertiary mental health facility for the assessment and treatment of youth aged between 16 and 18 years, who have severe psychiatric disorders unable to be effectively treated or managed in other mental health care settings. During its first 2 years of operation, YIU had 250 admissions, of which 157 were readmissions (65%). Readmissions were predominantly of two types: treatment admissions in the context of a relapsing psychiatric illness and brief 24–48 hour admission for the purpose of crisis stabilization. This distinction is important because different variables may be associated with these different types of readmission, with corresponding implications for interventions seeking to reduce the incidence of rehospitalization. In addition, brief admissions have a purpose in containing or defusing a crisis, potentially preventing relapse and therefore circumventing longer admissions which may disrupt the young person's social and educational environment. Previous research has not distinguished between different types of readmission.
This study aims to investigate factors associated with readmission to adolescent psychiatric inpatient care in the context of relapse. Diagnostic and demographic variables are compared between patients readmitted within 12 months of discharge from their first psychiatric admission and patients who were not readmitted within this time. In addition, the most common precipitating events to admission to YIU are identified and investigated. These precipitating events are of interest because they may represent proximal risk factors for readmission, not previously identified in the adult literature, that may hold particular developmental relevance to adolescents. Finally, the study includes history of childhood sexual abuse (CSA) because a history of CSA represents a diathesis for chronic psychiatric difficulties [11]. Individuals with such a history are at increased risk of becoming depressed or suicidal during adolescence [12] and depressed adolescent outpatients with CSA are more likely to require hospitalization and are more likely to relapse [13].
Method
Participants
Participants were drawn from 109 patients admitted to the YIU between 19 March 2001 and 19 March 2003. Thirty-four patients who were rehospitalized within 12 months of discharge in the context of a relapsing DSM-IV axis I illness and 37 patients whowere not readmitted within 12 months of initial hospitalization were included for analysis. Patients readmitted for brief 24–48 hour crisis admissions only (n=20), and four patients who were admitted to YIU as an interim measure before being transferred to other units (such as the child inpatient unit or intellectual disability service), were excluded from the present study. Also excluded was one patient with a frontal lobe head injury, one patient who died and regional patients (n=12) for whom follow-up data were unavailable. The study included, as part of the readmitted group, patients who had been admitted to inpatient psychiatric services other than YIU in the previous 12 months.
Variable selection
Variables included DSM-IV diagnoses on axis I and axis II, sex, age at first psychiatric admission, a history of CSA and the precipitating events identified by outpatient and inpatient clinicians at the time of admission.
Data collection
All data were gathered retrospectively by reviewing patients' electronic clinical files on the mental health patient information system of the Canterbury District Health Board. The review included all available local inpatient, outpatient and psychiatric emergency service records as contained in a single electronic clinical file for each patient.
Diagnoses were derived clinically using DSM-IV criteria, as is the clinical policy of the unit and based on information obtained as part of a comprehensive clinical assessment by the unit's multidisciplinary team. This comprises two child and adolescent psychiatrists, a psychiatric registrar, nursing staff, a social worker, a cultural advisor, an occupational therapist and a clinical psychologist. Diagnostic information was obtained from interviews with patients, significant others, referring clinicians, psychometric assessment and review of previous files. Diagnoses were made by the YIU multidisciplinary team at the time of assessment, clarified during treatment where appropriate and recorded in the electronic clinical file. For the purposes of the investigation, diagnoses were coded into the following DSM-IV categories: major depressive disorder, bipolar-affective disorder, posttraumatic stress disorder (PTSD), other anxiety disorder, psychosis (either schizophrenia or schizoaffective disorder), substance-use disorder and the presence of axis II personality disorder or significant traits.
Childhood sexual abuse was considered present if prior disclosure of abuse had been documented, or disclosure of abusewas made during the course of admission. Abuse history is routinely assessed at YIU as part of the comprehensive clinical assessment by the unit'smultidisciplinary team. Psychometric assessment with the Millon Adolescent Clinical Inventory and the Trauma Symptom Checklist for Children are regularly administered as part of this process. These instruments allow clinicians to identify when a history of sexual abuse is likely to be present and to assess further using a clinical interview.
The seven most common classes of precipitating event were identified using a line-by-line analysis of the clinical records for each admission. Medication non-adherence, either discontinuation of medication without medical advice or failure to take medication as prescribed, was commonly identified by clinicians preceding admission. Also identified were service-related change (either change in case manager or the transition to adult services), parent–child physical or verbal conflict, covert family dynamics (rejection or scape-goating), interpersonal relationship difficulties with peers and romantic partners, unstable accommodation and personal loss including death or separation.
Data analysis
Patients readmitted within 12 months of discharge were compared with patients not readmitted over this time with respect to sex, age at first admission, diagnosis, history of CSA and precipitants to admission. Where patients had more than one readmission within 12 months of discharge, the precipitants of the first readmission were included for comparison with single-admission patients. With the exception of age of first admission, which was analysed using the Student's t-test, variables were coded into categorical binary data and analysed using Pearson's χ2 test, or Fisher's exact test where appropriate. Due to the number of comparisons made, a Bonferroni adjusted p value of 0.05/16=0.003 was used as the point of statistical significance. Analyses were conducted with the Statistical Package for the Social Sciences (SPSS v 10.05).
Results
The mean interval to readmission was 4.6 months (median=3.5 months). Readmitted and single-admission patients did not differ with respect to sex with 22 females in each group, 65 and 60%, respectively.
Readmitted patients displayed a strong trend toward younger age at first psychiatric admission than single-admission patients (mean=16.10 years vs 16.79 years, t=2.704, df=69, p=0.009). We questionedwhether this resultwas influenced by the fact that some readmitted patients had their original admission in a child unit catering for patients under the age of 16 years, whereas YIU typically admits youth between the ages of 16 and 18 years. However, there was no demonstrable difference between the groups in terms of patients who had admissions before the unit's acceptance age of 16 years (χ2 =2.041, df=1, p=0.153).
Table 1 compares readmitted patients with single-admission patients in terms of diagnosis, history of CSA and the precipitating events to admission. No effects were found for diagnosis; however, compared with single-admission patients, readmitted patients were more likely to have a history of CSA (59% vs 24%, χ2 =8.728, df=1, p=0.003). In addition, readmissions were significantly more likely than single admissions to have medication non-adherence identified as a precipitant (47% vs 11%, χ2 =11.506, df=1, p=0.001) and significantly less likely to have personal loss identified as a precipitant (6% vs 35%, χ2 =9.099, df=1, p=0.003).
DSM-IV diagnoses and childhood sexual abuse (CSA) history of adolescent readmitted patients compared to single-admission patients and the events precipitating admission
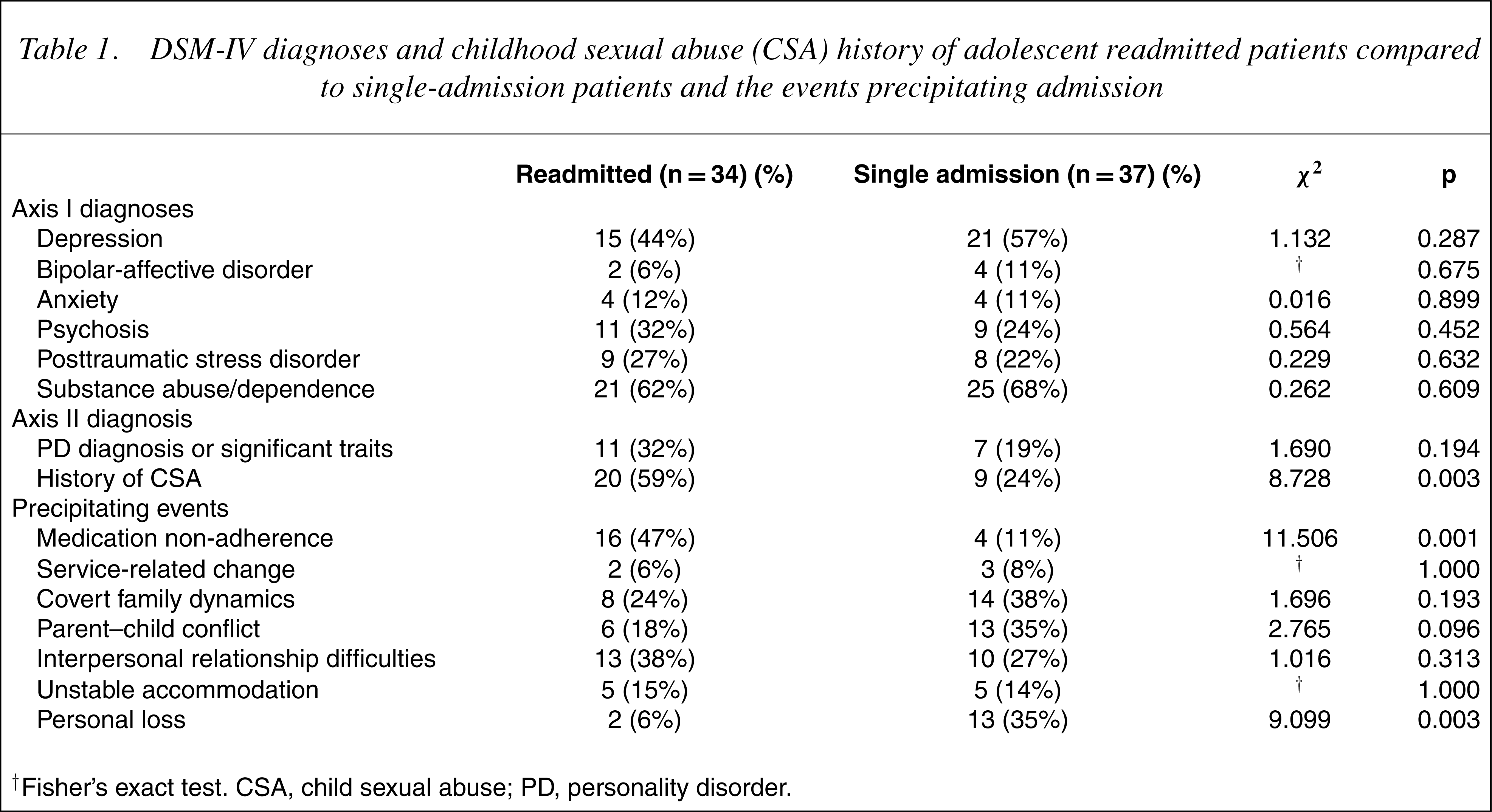
† Fisher's exact test. CSA, child sexual abuse; PD, personality disorder.
Post-hoc analyses conducted using the Student's t-test and χ2 analysis found no associations among age at first psychiatric hospitalization and medication non-adherence, or medication non-adherence and a history of CSA. Interestingly, however, patients with a history of CSA were slightly younger (mean=16.172) than patients without a history (mean=16.667) at the time of first admission, although this difference was not significant (t=1.845, df=1, p=0.069).
Discussion
This study investigated factors associated with readmission in the context of psychiatric relapse in an adolescent sample and contributes to the emerging readmission literature in this population. Results showed that readmission was positively associated with medication non-adherence and a history of CSA and negatively associated with personal loss. In addition, a trend emerged for readmitted patients to be younger at age of first-psychiatric admission.
To our knowledge, this is the first study in an adolescent population to find a positive association between readmission and medication non-adherence. This result is unsurprising and is commensurate with numerous adult studies which have established medication non-adherence as an important predictor of readmission [1],[14–17] and relapse [17–19] and suggests that clinicians working with adolescents should give consideration to supporting the maintenance of medication adherence post-discharge.
In the general psychiatric literature medication nonadherence is viewed as multidetermined [17], [20] and has been consistently associated with severity of illness, substance abuse, adverse side-effects of medication, inadequate social support and the unavailability of family or friends to support the appropriate use of medication [17]. We identified only two studies examining medication non-adherence in adolescents post-hospital discharge. The first of these [21] investigated adolescents who had been hospitalized with depression, anxiety, or disruptive behaviour disorders and found that post-discharge medication non-adherence was not predicted by diagnosis, medication type or number, severity of depression, age, race, sex, socio-economic status, or family living arrangement. The authors concluded that medication non-adherence is both common and difficult to predict in adolescents. The second study [22] investigated adolescents hospitalized with affective disorder, conduct disorder, or substance abuse, and found that medication non-adherence was predicted by post-discharge substance abuse and general non-compliance with treatment, but was not predicted by side-effects from medication.
To support the maintenance of medication adherence post-discharge, a comprehensive evaluation of the risk of non-adherence should be conducted for each patient as part of their discharge planning [17], [21]. This should consider factors such as insight, substance-abuse comorbidity, environmental influences, family and social support, socioeconomic considerations and the prospects for good therapeutic alliance [17], [23]. Interventions can then be implemented to address those factors putting the patient at risk of medication non-adherence.
Further research in adolescent samples relating tomedication non-adherence and interventions aimed at improving adherence is warranted. In particular, future studies should include patients with psychosis and evaluate the contribution of adverse side-effects to antipsychotic medication. Neither of the adolescent studies we identified included patients with psychosis and adult patients with psychosis who discontinue their medication commonly cite undesirable side-effects of medication as the reason for non-adherence [17], [20], [24], [25]. Furthermore, weight gain associated with atypical antipsychotics [26] is likely to be a major disincentive to adherence [27] for adolescents [28], for whom issues of self-image and body size are especially sensitive. In addition, evaluations of interventions proven helpful in adult populations, such as developing positive attitudes to medication, optimizing medication regimens, providing patients with the practical skills necessary for adherence and involving significant others [19], [24] should be trialled in adolescent populations.
In contrast to medication adherence, CSA has received little attention from researchers as a potential predictor of readmission. A literature search using MEDLINE and PSYCINFO located only one reference that investigated CSA within the context of rehospitalization. In this study, Hurt [29] found that readmission among adult patients was positively associated, on an univariate analysis, with a known history of sexual abuse, younger age of first admission, frequency of prior hospitalization, PTSD, borderline personality disorder and lower global assessment of function score for the past year.
Our finding of a positive association between a history of CSA and readmission is consistent with Hurt's results. This finding is not unreasonable as CSA is associated with a number of factors which may contribute to a greater risk of rehospitalization. First, evidence from a number of studies indicates that adolescents with a history of CSA are at an increased risk of engaging in suicidal behaviour [30–32] and are over 15 times more likely to make repeated suicide attempts than their non-abused peers [12]. Second, CSA is associated with a heterogeneous range of chronic disorders and difficulties. These include depression, substance-abuse disorder, borderline personality disorder, somatization disorder, PTSD, dissociative-identity disorder, bulimia, sexualized behaviour, early pregnancy and a cluster of problems including affect dysregulation, impulsivity, somatization, disturbed self-functions, cognitive distortions and socialization difficulties [11]. Finally, recent research from a clinical trial for adolescent depression found that sexual abuse was predictive of poorer longterm prognosis, including an increased risk for hospitalization and depressive relapse [13].
Clinicians working with distressed adolescents should ensure that CSA is asked about and that the ongoing impacts of CSA are identified and considered in the treatment plan. Although there is no single established intervention for children or adolescents who have experienced sexual abuse, there is some consensus that abusespecific cognitive behavioural therapy (CBT) is beneficial [11], [33]. Moreover, the heterogeneity of this group requires that treatment plans be individualized in relation to a patient's clinical presentation and incorporate multimodal interventions [33].
Given the paucity of research investigating CSA in the context of hospital readmission, replication of this finding in other adolescent samples is required and should include the systematic measurement and analysis of the parameters of abuse that have been shown to differentially influence risk of psychopathology [34]. Additionally, given that abuse-specific CBT shows some benefits in addressing the psychological and psychiatric sequelae of CSA, the effectiveness of this intervention in reducing readmission rates could be evaluated usefully. Overall, future research is needed to provide a better understanding of the relationship between CSA and readmission with a view to informing interventions to reduce the risk of relapse and readmission for adolescents with a history of CSA.
An interesting finding of this study is that readmission was less likely to be associated with personal loss, a variable which encompassed the termination of a romantic relationship and death of a family member or friend. Romantic loss has been identified as significant loss event for adolescents [35] and our results are consistent with results of a study by Monroe et al. who identified relationship loss as a predictive factor for first episode of depression but not recurrence of depression in adolescence [36]. Single-admission patients who experienced a loss event before admission, the majority of whom had a diagnosis of depressive illness, appear to have been suffering from a period of acute stress from which they later recovered without the need for further hospitalization.
Our results show a trend toward younger age of initial psychiatric hospitalization in relapsing, readmitted adolescents. Although consistent with earlier readmission [6], [8], [9], [15], [23], [37] and relapse [38], [39] research, we were surprised to obtain this result given the narrow age range of our sample. Nevertheless, age may be related to readmission for a number of reasons. It is possible that earlier hospitalization is associated with more chronic and severe psychopathology, with a corresponding increase in the need for repeated hospitalization. In addition, the early onset of psychiatric illness may have adverse developmental consequences, such as impaired autonomy, which may increase the likelihood of rehospitalization. Alternatively, early hospitalization may lower the threshold for later admission. Clarifying the significance of this finding requires further investigation.
Anotable null findingwas the absence of an association between substance abuse and readmission. This result is in contrast to numerous studies which have established substance abuse as a predictor of readmission for adult patients with psychotic and affective disorders [1], [9],[15–17],[22], [37], [40], but replicates findings from a 10-year readmission study of adolescents byArnold et al. [6]. The lack of association between substance abuse and readmission in our study is likely to be attributable to the ubiquity of substance abuse in our sample, which is consistent with the high rate of substance abuse in our inpatient population [41].
Limitations
This study is subject to several limitations. The method, a retrospective approach combined with a relatively small sample, precludes the development of a multivariate predictive model. Although this study identifies factors associated with readmission, we cannot comment on variables present but associated with no admission, or precipitants to the first admission of readmitted patients. It is likely that readmitted patients possess vulnerabilities and single-admission patients possess protective factors that have not been measured. Additionally, complex mechanisms beyond the scope of this investigationmay mediate the relationship between the factors identified here and relapse readmission. Medication non-adherence and a history of CSA were measured in their presence or absence, therefore we cannot comment on the levels of adherence, or the parameters of abuse, including severity, chronicity, disclosure or failure in documentation. Finally, the results apply to patients, aged predominantly between 16 and 18 years, who were readmitted within 12 months of discharge in the context of relapse. The generalizability of these findings to younger adolescents or over longer periods of time is open to question.
Conclusions
This study contributes to an emerging literature investigating factors associated with psychiatric readmission during adolescence. We found that medication nonadherence and a history of CSA were positively associated with relapse readmissions in our sample of adolescent inpatients, with a trend toward younger age of first admission in readmitted patients. In contrast, the experience of personal loss was negatively associated with readmission. Although these results concur with adult research in terms of age of first admission, medication nonadherence and one study investigating CSA, replication among other adolescent samples is warranted, as is the use of prospective and multivariate techniques to examine the relative contribution of these factors. Additional research could usefully examine the ways in which medication non-adherence and the psychological sequelae of CSA contribute to psychiatric relapse within the context of adolescent development. Clinicians should attend to risk factors associated with medication non-adherence and to the heterogeneous and multimodal treatment needs of patients with a history of CSA. Overall, an improved understanding of factors leading to readmission and factors which protect against it, is likely to assist in identifying adolescents at risk of repeated hospitalization and to inform treatment and management practices to reduce this risk.
Footnotes
Acknowledgements
The authors thank the Canterbury District Health Board and the staff of the Youth Inpatient Unit, Anne Scott, Harith Swadi, Glenn Richardson and Suzanne Barr.