
Abstract
Abstract
Background: Premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) are common conditions causing significant impairment in various domains of life. Both the conditions are associated with physical, emotional, and behavioral symptoms. There is dearth of studies regarding symptomatology and severity of the condition in Indian college students.
Aim: Aim of this study is to categorize and rank the symptoms and severity of PMDD in college students in India.
Materials and methods: A cross-sectional survey was conducted in various colleges of Mysuru. A total of 600 girls were approached over a period of 1 year. Confidentiality was assured and written informed consent was taken. Girls with irregular periods and those who had an absence of menstruation since last 3 consecutive menstrual cycles were excluded. A total of 571 filled up forms were taken for analysis. Data was analyzed using SPSS 22 version software. Chi-square test was used as the test of significance for qualitative data.
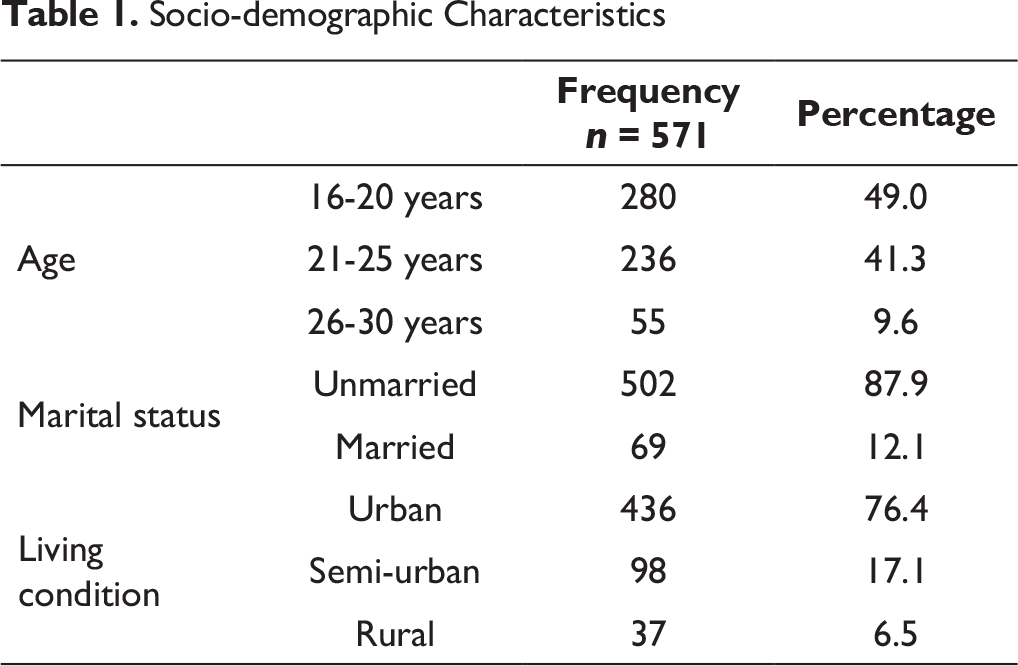
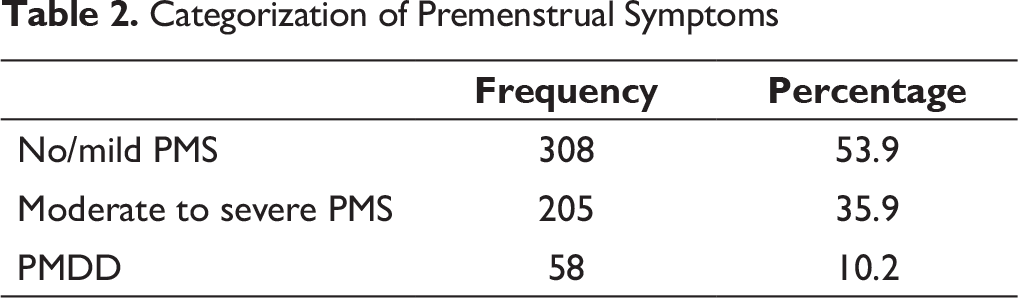
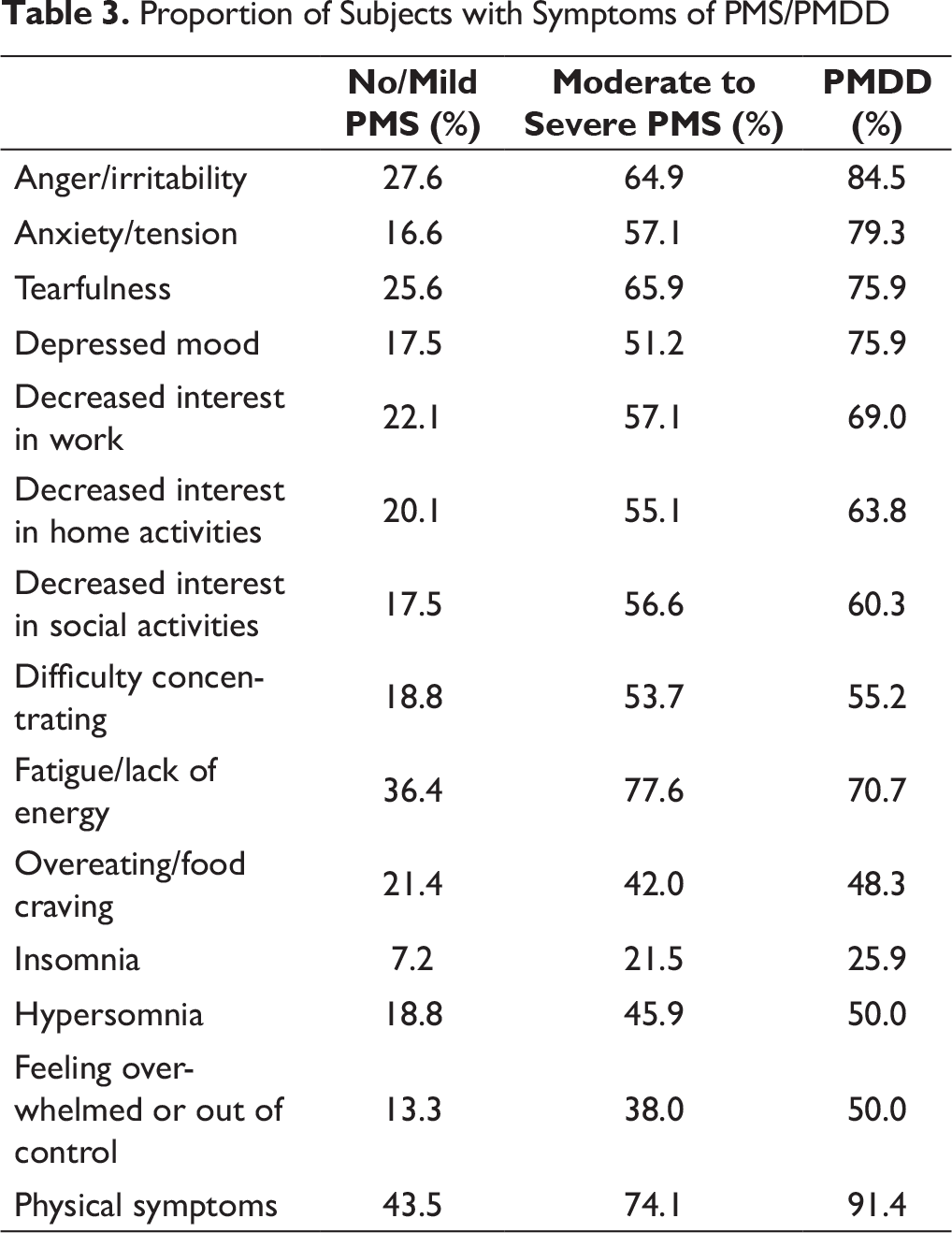
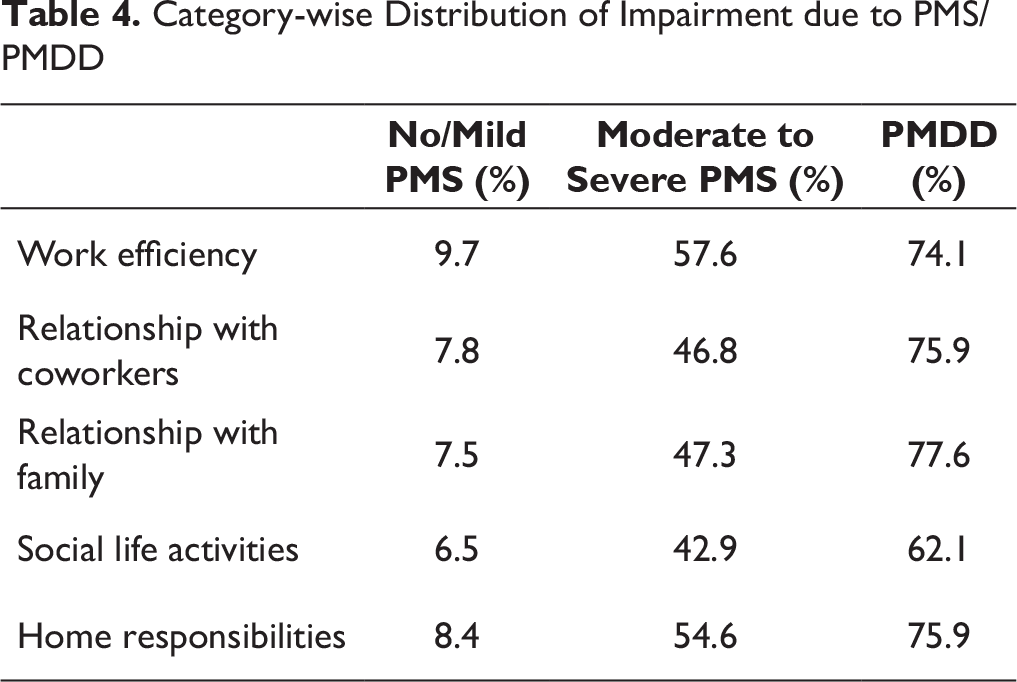
Results: The mean age of participants was 21.12 ± 2.6 years. Majority of the subjects were unmarried and were from urban background. The prevalence of PMS/PMDD was 46.1%, out of which 10.2% met the criteria for PMDD. Physical symptoms (91.4%) were the most commonly reported symptom domain in the PMDD category, followed by anger or irritability (84.5%). Almost half of the subjects with no or mild PMS had reported physical symptoms. The least reported symptom was insomnia. PMDD group had reported maximum impairment in the domain of relationship with family members (77.6%), followed by home responsibilities and relationship with coworkers.
Conclusion: This study suggests that the prevalence of clinically relevant PMS/PMDD is higher than widely cited estimates and is a cause of concern for health care authorities in India. Physical complaints are the most commonly reported among all the symptoms in all groups. There is a need to actively assess for premenstrual symptoms in young women for comprehensive treatment and good outcome.
Introduction
The premenstrual syndrome (PMS) is a common clinical condition affecting many women during reproductive years. According to estimates by epidemiological surveys 1 as many as 80% of women experience some vexing symptoms related to the premenstrual period. The worldwide prevalence of premenstrual dysphoric disorder (PMDD) is estimated to be 3% to 9%. 2 According to the western literature, there is an enormous amount of health care and economic burden associated with PMS and PMDD. In India, more than one-fourth (27.7%) of the female population falls in the 15 to 29 year age-group. 3 Worldwide literature shows that women are more likely to develop depression and anxiety disorders.4, 5 Still, there is a lack of gender-specific studies in terms of mental disorders. Also, most of the studies pertaining to women mental health in India focus on postpartum depression or older age-group.6, 7 Premenstrual syndrome and PMDD comprise the understudied areas in the Indian context. The reproductive period with menstruation has increased in the life of an average Indian woman, owing to the early onset of menarche, contraceptive methods, and better nutrition. It is crucial to study the levels of impairment and distress due to premenstrual symptoms. The objectives of this study were to identify the prevalence, categorize and rank the symptoms, and grade the levels of severity and impairment in PMS/PMDD among Indian college students.
In the earlier literature, it has been referred to as premenstrual tension. In mid-1980s the term “late luteal phase dysphoric disorder” was also used. ICD-11 does not include it in Chapter 06 (“Mental, behavioural or neurodevelopmental disorders”). It has been classified as premenstrual disturbances (GA34.4) in Chapter 16 (“Diseases of the genitourinary system”). This is not used in research or clinical diagnostics, because it is not defined by any specific criteria and lacks any specification of the severity. DSM-IV had first attempted to define the condition by a specific criterion and included PMDD in Appendix B “Criterion sets and axes provided for further study.” DSM-V has included PMDD 8 as a separate diagnostic entity with alphanumerical coding 625.4 (N94.3). It is widely used for the research on epidemiology, pathogenesis, phenomenology, and treatment of the disorder. Most of the screening and diagnostic tools are adapted from this set of criteria.
PMS is considered as a less severe form of PMDD. Both the conditions are associated with physical, emotional, and behavioral symptoms. The physical symptoms of PMS include lower back aches, breast tenderness (mastalgia), swelling, bloating, headaches, etc. Irritability and mood swings and are some of the most commonly reported symptoms of PMS. There can also be anxiety, tension, sadness, feeling of being overwhelmed, or being out of control. The mood symptoms can be very debilitating and may lead to marked impairment in the occupational, social, and interpersonal domains of a woman’s life. Sleep disturbance, which can either be insomnia or hypersomnia, is among the commonly reported behavioral symptoms. There can be a loss of appetite or episodes of binge eating or particular food cravings. The other behavioral symptoms include social withdrawal, lack of concentration or decreased interest in various activities. All the symptoms of PMS/PMDD may be present for few days or even weeks in some women. Symptoms often worsen markedly 6 days before the onset of menstruation and peak at 2 days before the start of menses. Anger and irritability might start somewhat earlier than the other symptoms. The symptoms may linger into the next menstrual cycle, but the presence of a symptom-free interval before ovulation is required.
The levels of morbidity associated with PMDD are due to its involvement in all domains of life—social, occupational, and interpersonal. It can be the reason for absenteeism from classes and a decline in the academic performance in young girls. This condition can be managed by lifestyle modification, exercise, and medication in more severe cases. Hence, this study was planned to explore this obscure area of prime importance.
Materials and Method
The study was approved by the ethical committee of JSS Medical College and Hospital, Mysuru. Female students in different colleges of Mysuru were chosen as the population for this study. These students were pursuing different courses including arts, commerce, pharmacy, law, and medicine. The study population consisted of students from different states across the country. A total of 600 girls were approached for this cross-sectional study over a period of 1 year (September 2017 to August 2018). Convenient sampling method was used. The sample size was calculated using OpenEpi Version 2 open source epidemiological calculator. The hypothesized prevalence of PMS and PMDD was taken as 15% ± 4% at 99% confidence level. The design effect was kept as one. Participants were briefed about the nature and purpose of the study and were asked verbally about the regularity of their periods. They were educated about the symptoms of PMS, and the questionnaires were distributed. Confidentiality was assured and written informed consent was taken. Girls with irregular periods and those who had absence of menstruation since last 3 consecutive menstrual cycles were excluded. A total of 592 questionnaires were collected back, out of which 13 forms were incomplete and 8 girls had mentioned in the form that their periods were not regular. A total of 571 filled-up forms were taken for analysis. Data were entered into Microsoft excel data sheet and were analyzed using SPSS 22 version software. Categorical data was represented in the form of frequencies and proportions. Continuous data was represented as mean and standard deviation. Chi-square test was used as the test of significance for qualitative data. P value < .05 was taken as statistically significant.
PSST
The premenstrual symptoms screening tool (PSST) was developed by Meir Steiner in 2003. 1 It translates the categorical DSM-IV criteria into a rating scale. It is a self-reporting questionnaire and includes a list of premenstrual symptoms, both psychological and physical, as well as a measure of impairment with degrees of severity. It consists of 2 sections and 19 questions. The first section has 14 questions based on symptoms of PMS/PMDD. Participants are asked to rate the degree to which they experience each symptom during the late luteal phase and the degree to which the symptoms interfere with each functional domain. Items are rated on a Likert scale as “not at all,” “mild,” “moderate,” or “severe.” A total of 13 questions pertain to mood and behavioral symptoms of PMS/PMDD. One question is regarding the physical symptoms. The second section enquires about the interference due to premenstrual symptoms in various domains of life, on a Likert scale ranging from “not at all” to “severe.” It has 5 questions (A, B, C, D, and E) regarding different domains such as work efficiency, relationship with family and coworkers, social life activities, and home responsibilities. According to the scoring of the symptoms, 1 subjects were divided into 3 categories “mild/no PMS,” “moderate to severe PMS,” and “PMDD.”
Results
Socio-demographic Characteristics
Categorization of Premenstrual Symptoms
Proportion of Subjects with Symptoms of PMS/PMDD
Category-wise Distribution of Impairment due to PMS/PMDD
Discussion
The sample size of this study is comparable to previous studies 9 - 11 conducted in this area, with similar characteristics of being unmarried and hailing from an urban background. The prevalence of PMS in this study is in accordance with international data. A 2014 meta-analysis 12 by Dirkevand et al showed the pooled prevalence of PMS to be 47.8%. However, this finding is not in agreement with Steiner et al 13 who reported the prevalence of PMS to be 21.3%. Other independent studies conducted in Asian population also showed a lower prevalence of PMS.14, 15 The prevalence of PMDD in this study was found to be 10.2%. Banerjee et al 16 reported prevalence of PMDD to be 6.4%. However, this study had a small sample size. Most of these studies have methodological differences, using different tools and methods for assessment of premenstrual symptoms. This study suggests that the prevalence of clinically relevant PMS/PMDD is higher than widely cited estimates, and is a cause of concern for health care authorities in India. The symptoms were taken as present if marked moderate or severe in the questionnaire. Most commonly reported symptom in PMDD category was physical complaints, reported by 91% of the students, followed by anger/irritability (Table 3). Students in moderate to severe category of PMS also reported physical symptoms and lack of energy as the most common symptoms. Almost half of the students with no/mild PMS also reported experiencing physical symptoms. This is in accordance with most of the retrospective studies, 17 - 19 where physical symptoms are reported more commonly, as the individual tends to remember it more clearly. But it also points toward the need for more recognition of physical symptoms in our diagnostic criteria and assessment tools. American College of Obstetricians and Gynecologists acknowledges that one of the physical symptoms along with mood/behavioral symptoms must be present to diagnose PMS 20 But according to DSM-V, diagnosis can be made even in the absence of physical symptoms if the other symptoms are present in significant severity. 8 The level of impairment in various domains of life due to premenstrual symptoms was found to be high (Table 3). More than half of the women with moderate to severe PMS reported impairment across all domains of life (Table 4). This percentage was even higher for the PMDD group. These levels of impairment indicate the high levels of burden of PMS/PMDD. Despite the substantial number of college students being affected, this condition goes mostly unrecognized. There is a general lack of awareness and sensitivity among general as well as the medical population. The recognition and diagnosis of the disorder can provide considerable relief to many students. This will also have a positive impact on academic performances as well as overall well-being of these women. There are many efficacious treatments available for premenstrual symptoms. Aerobic exercise 21 and cutting down dietary sugar are the lifestyle modifications found to be helpful. Pharmacotherapeutic options are also available. Intermittent selective serotonin reuptake inhibitors (SSRIs) 22 have been touted as a very effective treatment, with minimal side effects. However, there is a concern regarding the use of SSRIs in patients presenting with only anger outbursts, mood swings, and irritability as presenting complaints. The risk of an antidepressant-induced switch should be kept in mind, especially because bipolar affective disorder is one of the known comorbidity of PMS. Keeping a record of premenstrual symptoms through a diary or mobile apps can prove to be very useful. This will aid in recognition as well as individualized management of the symptoms. Sample size and prospective or retrospective recording also affect the results regarding prevalence of PMS/PMDD. Prevalence rates tend to be inflated if they are based on retrospective reporting rather than prospective daily recordings. The premenstrual symptom screening tool used in this study is based on DSM-IV criteria, which has an arbitrary cutoff point of at least 5 severe symptoms, a point which is controversial for many researchers. This criterion of PMDD is considered a bit restrictive by some authors, as women meeting the criterion in one cycle may not meet it in the next cycle wherein they have lesser number of symptoms but still with high severity. So there is a further need to design scales to address these shortcomings, as well as scales standardized for the Indian population.
Conclusion
PMS and PMDD are widely prevalent among college students in India. Physical complaints are the most commonly reported among all the symptoms in all groups. There is a need to actively assess for premenstrual symptoms in young women for comprehensive treatment and good outcome. Awareness programs should be conducted for young women to educate them regarding symptoms of PMS and prevention through lifestyle modification.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.