
Abstract
Background:
Colorectal cancer (CRC) screening programmes commonly use the Faecal immunochemical test (FIT) followed by colonoscopy. When colonoscopy is not feasible, computed tomography colonography (CTC) serves as an alternative. However, CTC has limitations, such as lower sensitivity for smaller polyps and radiation exposure. Colon capsule endoscopy (CCE) is a non-invasive alternative that may improve polyp detection in FIT-positive individuals.
Objectives:
To evaluate the feasibility of CCE in FIT-positive participants from the Dutch CRC screening programme who are unable or unwilling to undergo colonoscopy.
Design:
Prospective multicentre, interventional study.
Methods:
FIT-positive participants ingested the PillCam® Colon 2 capsule. Colonoscopy was recommended if polyp(s) ⩾6 or suspected malignancy were detected. The primary outcome was the per-patient polyp detection rate (PDR) for polyps ⩾6 mm.
Results:
Of 169 FIT-positive participants unable to undergo colonoscopy, 54.4% were ineligible for CCE due to contraindications. CCE was performed in 13 participants, with a completion rate of 69.2% and adequate bowel preparation in 38.5. A total of 54 polyps were detected, 46.3% of which were ⩾6 mm. The per-patient detection rate for polyps ⩾6 mm was 76.9%. In 84.6% of cases, follow-up colonoscopy was advised. CCE findings matched colonoscopy in 66.7% of cases; in the remaining 33.3%, polyps were found to be < 6 mm during colonoscopy. One participant was diagnosed with a pT4bN0M0 adenocarcinoma after CCE revealed a tumorous obstruction.
Conclusion:
Despite a high per-patient PDR, this study indicates that CCE is less suitable for FIT-positive individuals unable or unwilling to undergo colonoscopy due to high comorbidity and frequent contraindications. Inadequate bowel preparation, likely due to reduced gastrointestinal motility, further limited feasibility. Given the elevated risk of advanced neoplasia in this population, many still required follow-up colonoscopy. Therefore, CCE may be better suited for lower-risk populations with fewer procedural limitations.
Trial registration:
Overview of Medical Research in the Netherlands, NL-OMON55511.
Introduction
To reduce colorectal cancer (CRC) incidence and mortality, many countries worldwide have implemented national population-based CRC screening programmes. In most European countries, the Faecal immunochemical test (FIT) serves as the primary screening tool, followed by colonoscopy in case of a positive FIT result. Colonoscopy is the most accurate imaging test for detecting colorectal advanced neoplasia (AN).1,2 When colonoscopy is not feasible due to patient comorbidities, preferences, or incomplete procedures, computed tomography colonography (CTC) is offered as an alternative. CTC is a minimally invasive modality for colon examination, demonstrating high sensitivity in detecting CRC and polyps of ⩾10 mm.3–5 However, sensitivity decreases for smaller polyps, ranging from 52 to 75% for polyps 6–9 mm, markedly lower than that of colonoscopy.4,6,7 A recent study has shown that CTC in FIT-positive participants of the Dutch CRC screening programme resulted in a lower AN detection rate and a higher proportion of post-CTC CRCs compared to colonoscopy within the same population. 8 Other limitations of CTC are the radiation exposure and incidental findings that may lead to overdiagnosis. Additionally, the procedure requires patient repositioning on the CT table and rectal insufflation via a catheter, which can be particularly challenging in some individuals.
Colon capsule endoscopy (CCE) is a non-invasive technique using an ingestible, wireless, and disposable capsule to explore the colon without the need for sedation or air insufflation. 9 The second-generation CCE (CCE-2) is equipped with dual cameras, enabling image acquisition from both ends of the capsule and providing nearly 360° visualisation of the colonic mucosa. It incorporates adaptive frame rate technology, which dynamically adjusts image capture frequency from four to 35 frames per second depending on capsule movement. Bidirectional communication between the capsule and external data recorder enables real-time modification of imaging parameters, allowing the capsule to respond to transit events. Image analysis is performed by trained readers using dedicated software platforms that facilitate systematic review of the video footage for polyps, masses, and mucosal abnormalities. Polyp size measurement in CCE-2 is performed by software-assisted tools that estimate lesion dimension by comparing polyps to known anatomical landmarks or by using the capsule’s dual cameras to triangulate size. CCE has demonstrated high diagnostic accuracy for polyps⩾ 6 millimetres (mm) and is superior to CTC in identifying colorectal polyps ⩾6 mm in average-risk CRC populations.10–12 Sensitivity and specificity of CCE-2 for polyps ⩾6 mm range from 79 to 96% and 66 to 97%, respectively, with improved performance observed for polyps ⩾10 mm.13–15 European guidelines suggest that CCE might be considered in organised population screening programmes for FIT-positive individuals. 12 However, the evidence supporting these recommendations remains weak. While several studies have evaluated the diagnostic value of CCE compared to CTC and/or colonoscopy in an average-risk population with low comorbidity, fewer have focused on individuals with a positive FIT who are unable or unwilling to undergo colonoscopy. These individuals are at increased risk of AN and typically present with a higher burden of comorbidities compared to average-risk individuals, making them unsuitable patients for colonoscopy. One study comparing CCE and CTC in FIT-positive individuals unwilling to undergo colonoscopy revealed a significantly higher adenoma detection rate for CCE (60%) versus CTC (28.6%). 16 These findings suggest that CCE could be a preferred alternative to CTC in FIT-positives. However, the participation rate for both modalities was low. Another study showed promising potential for CCE with a 66% participation rate when CCE was offered to individuals who refused colonoscopy. 17 This finding was supported by another study, where the accuracies for CTC and CCE were similar, with a sensitivity of 88.2% for both modalities, but a patient preference in favour of CCE. 5
In the Dutch national CRC screening programme, the majority of FIT-positives undergo colonoscopy. In approximately 6% of cases, around 4.000 FIT-positives annually, colonoscopy is averted, typically due to comorbidities or patient refusal, and in 1.3%, a CTC was performed instead. 18 In addition, a subset of individuals experience incomplete colonoscopy procedures, leaving part of the colon unexamined and subsequent referral for CTC. For these individuals, CCE might be a more suitable option, as it provides a diagnostic examination that can be performed at home with a higher polyp detection rate than CTC. Therefore, the aim of this study was to evaluate the applicability of CCE in FIT-positive participants of the Dutch national CRC screening programme who have a contraindication for colonoscopy, a prior incomplete colonoscopy, or who are unwilling to undergo colonoscopy.
Methods
Study setting
In the Netherlands, a nationwide population-based CRC screening programme has been implemented since 2014. The programme invites all individuals between 55 and 75 years of age to participate. Participants receive a FIT kit accompanied by an information leaflet, delivered directly to their homes. The provided FIT and postal shipping to send the FIT to the laboratory are free of charge. FIT-positive participants (FIT cut-off 47 μg Hb/g faeces) are referred to a certified colonoscopy centre for a pre-colonoscopy counselling visit. For FIT-positive participants who are either unable to undergo a colonoscopy due to comorbidities or unwilling to undergo a colonoscopy, a CTC is offered as an alternative. Each year, approximately 6% of FIT-positive individuals, around 4000 participants, who attend the outpatient clinic, do not proceed with subsequent colonoscopy. Within this group, 1.3% opt for CTC, while the remaining participants do not undergo any additional colonic examination. 18
Study design and participants
This prospective, multicentre, interventional cohort study was conducted between April 2021 and April 2024 across five centres in the Netherlands, consisting of one academic and four regional hospitals. All FIT-positive participants of the Dutch screening programme with a contraindication for colonoscopy, who were unwilling to undergo colonoscopy, or who had an incomplete screening colonoscopy were eligible for inclusion. Exclusion criteria included inability or refusal to provide informed consent, as well as contraindications to CCE and its bowel preparation regimes. These included a life-expectancy of less than 5 years, allergies or contraindications to study medications (Bisacodyl, Metoclopramide, Moviprep, Eziclen and/or Gastrografin), estimated glomerular filtration rate < 30 ml/min/1.73 m2, congestive heart failure NYHA class III or IV, dysphagia or other swallowing disorder, inflammatory bowel disease, medical history of gastrointestinal surgery (excluding those procedures that are unlikely to lead to bowel stenosis or obstruction), cardiac pacemakers or implanted electromedical equipment, scheduled magnetic resonance imaging (MRI) within 14 days after capsule ingestion, congenital long QT syndrome, use of medication that prolong the QT interval, manifest hyperthyroidism, and allergies or hypersensitivities for iodinated agents. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 19
Study procedure
Eligible FIT-positives were invited to participate in the study. During the outpatient visit, study information was given, and patients received a patient information folder. After obtaining informed consent, colon capsule ingestion was scheduled at the outpatient clinic. Colon capsule ingestion was guided by one of the researchers (F.E.M. or S.M.). Demographic characteristics and reasons for non-participation were collected from those who did not participate in the study. For this study, the PillCam® Colon 2 capsule (Medtronic Ltd, Brussels, Belgium) was used. CCE bowel preparation consisted of a low volume laxative solution (Moviprep®) in combination with Eziclen® and Gastrografin® . The selection of this bowel preparation protocol was informed by evidence from previous research.20–23 The preparation protocol is provided in Supplemental Table 1. CCE images were evaluated by two trained researchers (FEM and SM) who were qualified (PillCam™ Colon 2 capsule e-learning) to read the CCE video. If no abnormalities were detected, participants were referred to the screening programme and re-invited for a new FIT after ten years, unless they were older than 75 years at that time. This approach aligns with the current Dutch policy, whereby individuals with a negative colonoscopy or CTC following a positive FIT are re-invited for FIT screening after ten years. For polyps smaller than 6 mm, a CTC was recommended three years later. For polyps measuring 6 mm or larger, more than five polyps irrespective of size, or suspected CRC, patients were referred for subsequent colonoscopy (Figure 1). If participants had contraindications for colonoscopy or sedation, gastroenterologists assessed whether the benefits of endoscopic removal outweighed the risks of the procedure. In cases of incomplete CCE procedures, where the capsule was not excreted within the battery time and therefore did not result in images of the entire colon, additional CTC, sigmoidoscopy, or colonoscopy was performed. The chosen additional modality in these cases was based on clinical judgement.

Study follow-up flowchart. Follow-up of study participants based on CCE findings.
Study outcomes
The primary outcome was the per-patient polyp detection rate (PDR) of CCE, defined as the proportion of FIT-positive participants with at least one polyp measuring ⩾6 mm or a suspected neoplastic lesion identified upon CCE review. This cut-off was selected based on current guidelines for CTC, which consider polyps ⩾6 mm significant and recommend additional colonoscopy for polypectomy. 12 Accuracy of CCE was assessed by comparing its findings with those of the subsequent colonoscopy and was defined as the proportion of participants with polyps measuring ⩾6 mm or⩾10 mm detected by CCE that were also identified by colonoscopy at corresponding sizes. All polyps found during colonoscopy were considered true positive findings. Polyps detected by CCE were matched to colonoscopy findings based on size using a per-patient approach. Participants were categorised according to the size of the largest polyp detected: ⩾6 mm, ⩾10 mm, or no polyps. These analyses were conducted for all participants who underwent both CCE and colonoscopy.
Secondary outcomes included the feasibility of CCE, assessed through participation rate and reasons for non-participation, and CCE quality. Quality was evaluated based on bowel cleansing, CCE completion, and image review time. Bowel cleansing was scored for each colon segment and overall, using a four-point scale (poor, fair, good and excellent), and the bubbles effect scale was scored as either significant or insignificant. 24 CCE completion was defined as the excretion of the capsule within the battery time, ensuring visualisation of the entire colon. Baseline characteristics such as age, sex, American Society of Anesthesiologists (ASA) classification, and reasons for declining colonoscopy were also collected.
Statistical analysis
Descriptive statistics were used to assess baseline characteristics, polyp detection rates, participation and CCE quality parameters. Numerical data were presented as means with standard deviation or medians with interquartile range, while categorical data were shown as counts with percentages. The accuracy of polyp detection by CCE compared to colonoscopy and subsequent histopathology findings was presented as percentages with 95% confidence intervals. All analyses were performed using IBM SPSS v.25 (IBM Corp., Armonk, NY, USA).
Results
During the study period, 169 FIT-positive individuals from the CRC screening programme were unable or unwilling to undergo a screening colonoscopy or had a prior incomplete colonoscopy. The majority (60.4%) of FIT-positive participants were classified with an ASA score of ⩾3. Among them, 72 (42.6%) were unable to undergo colonoscopy due to comorbidities, such as the presence of significant pulmonary or cardiac conditions. Furthermore, 21 (12.4%) were unwilling to undergo colonoscopy or the corresponding bowel preparation, two (1.2%) had an incomplete colonoscopy and in 74 (43.8%) participants, the reason for not performing colonoscopy was unknown. Of these 169 FIT-positives, 13 individuals (7.7%) were eligible for inclusion and agreed to participate in CCE. The participants who underwent CCE had a median age of 68 years, and 12 (92.3) were male. Table 1 provides an overview of the patient characteristics, including all FIT-positive individuals who did not undergo screening colonoscopy during the study period, as well as those who consented to undergo CCE.
Patient characteristics of all FIT-positive individuals who were unable or unwilling to undergo screening colonoscopy.

ASA, American Society of Anaesthesiologists; CCE, colon capsule endoscopy.
Participation
Of all 169 FIT-positives, the majority (n = 85; 50.3%) were deemed ineligible for CCE based on at least one exclusion criterion. The most common reasons for ineligibility included contraindications to CCE bowel preparation, heart failure, and the presence of a pacemaker or implantable cardioverter-defibrillator (ICD). After excluding these individuals, 84 FIT-positives remained eligible. Of these, 13 consented to undergo CCE, while 10 (11.9%) actively declined participation, resulting in an overall study participation rate of 15.3%. A detailed overview of reasons for non-participation in CCE is provided in Table 2.
Categorised reported reasons for not participating in colon capsule endoscopy (N = 156).

Medication that prolongs QT-time.
Includes immobility or problems with understanding bowel preparation instructions.
ICD, implantable cardioverter-defibrillator.
CCE quality
Quality parameters of CCE are summarised in Table 3. In 9 (69.2%) out of 13 procedures, CCE reached completion within the battery time. In three procedures, the capsule was not excreted within the battery time, and in one participant, the colon capsule could not pass a tumorous obstruction in the colon. Overall bowel preparation was rated good in five (38.5%) participants, fair in five (38.5%), and poor in three (23.1%). No serious adverse events related to the CCE were reported. The median image review time of the colon was 60 min.
Quality parameters of colon capsule endoscopy.
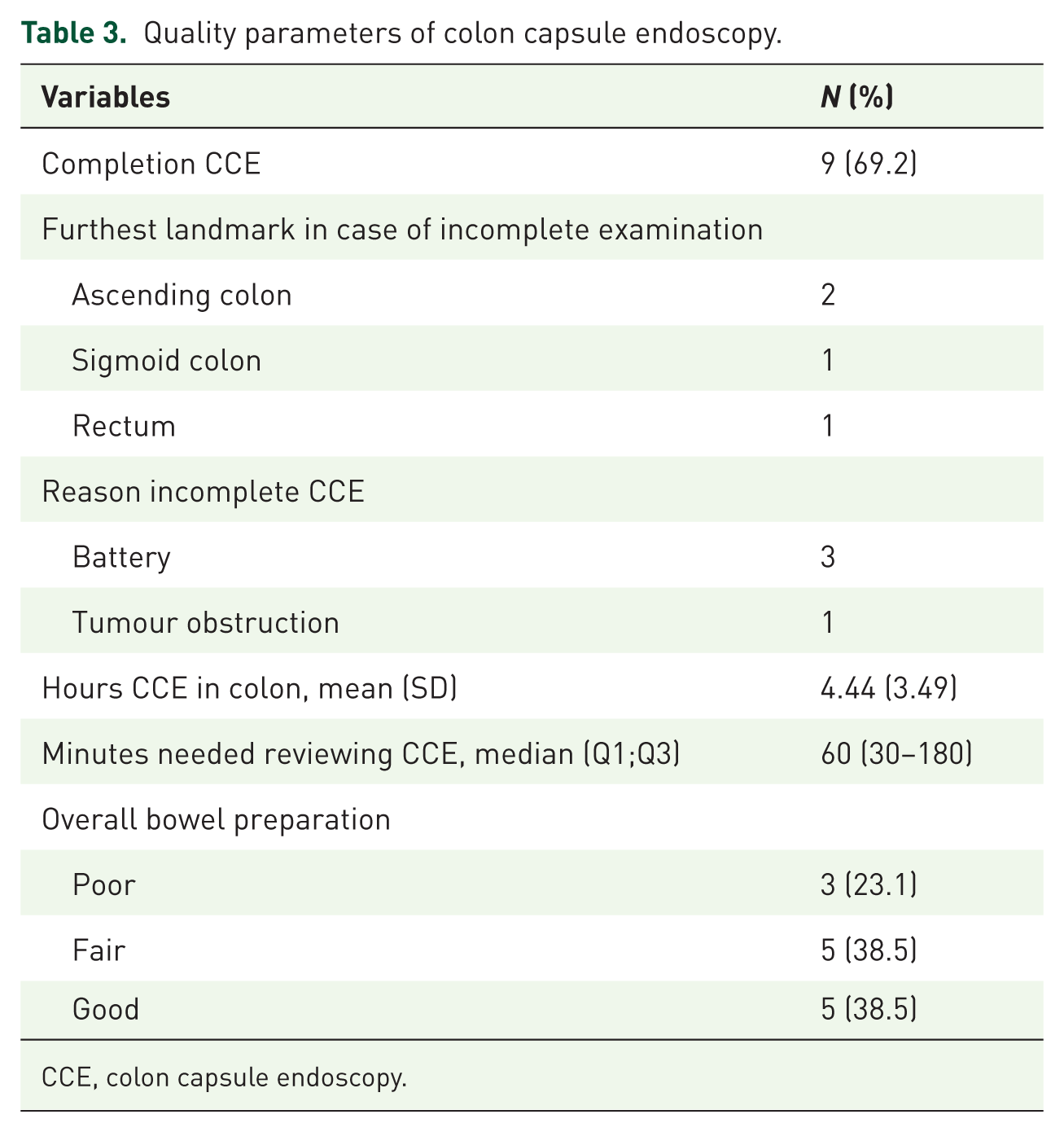
CCE, colon capsule endoscopy.
CCE polyp detection rate
CCE detected a total of 54 polyps. The majority of polyps were smaller than 6 mm (53.7%) and predominantly located on the left side of the colon (59.3%). One case of suspected CRC was identified based on CCE findings. Of the detected polyps, 25 (46.3%) measured 6 mm or larger. Detailed characteristics of CCE findings are shown in Table 4.
Yield of colon capsule endoscopy and colonoscopy.

CCE, colon capsule endoscopy.
The per-patient PDR was 76.9% (95% CI 49.1–92.5) for polyps ⩾ 6 mm or suspected CRC and 38.5% (95% CI 17.6–64.6) for polyps ⩾ 10 mm or suspected CRC (Table 5). In 11 participants, an additional colonoscopy was recommended: four due to polyps of 10 mm or larger, five due to polyps of 6–9 mm and one due to suspected CRC. In an additional participant, a colonoscopy was advised due to poor bowel preparation, which hindered proper image review.
Detection and accuracy rates of colon capsule endoscopy.

All per patient and in relation to colonoscopy.
CCE, colon capsule endoscopy; CI, confidence interval.
Accuracy of CCE
Of the 11 participants referred for colonoscopy after CCE, eight underwent follow-up endoscopy. Two participants refused the procedure, and another proceeded directly to surgery after oncological staging for suspected CRC. During endoscopy, a total of 18 polyps were detected, including three (16.7%) advanced adenomas, defined as polyps ⩾10 mm and/or with high-grade dysplasia and/or ⩾25% villous histology, and 13 (72.2%) non-advanced adenomas. Two polyps were removed but not retrieved for histopathological analysis. All advanced adenomas were identified in participants who had an indication for colonoscopy based on CCE findings, namely the presence of polyps of 6 mm or larger. A flowchart summarising colonoscopy-detected lesions, categorised by the most advanced lesion per participant, is presented in Figure 2. When comparing CCE findings to colonoscopy and surgery on a per-patient basis using the most advanced lesion, CCE accurately identified six (66.7%) participants with polyps ⩾6 mm. For polyps ⩾10 mm, CCE was accurate in only one participant (25.0%) (Table 5).

Diagnostic findings flowchart.
Neoplastic lesions
One FIT-positive participant with contraindications for both colonoscopy and CT-colonography was referred for colon capsule endoscopy. Prior to this, a diagnostic abdominal CT had been performed for bowel symptoms, which did not reveal any explanatory findings. At CCE, a semicircular tumorous colonic lesion was suspected, blocking the colon capsule to pass (Figure 3). Besides this, some blood was observed in the stomach, along with a questionable mass in the stomach. Further diagnostics, including a gastroscopy and thoracic-abdominal CT scan were performed. The patient was diagnosed with a pT4bN0M0 colonic adenocarcinoma in the transverse colon with fistulation from the splenic flexure and the transverse colon to the stomach and subsequently underwent curative surgery.
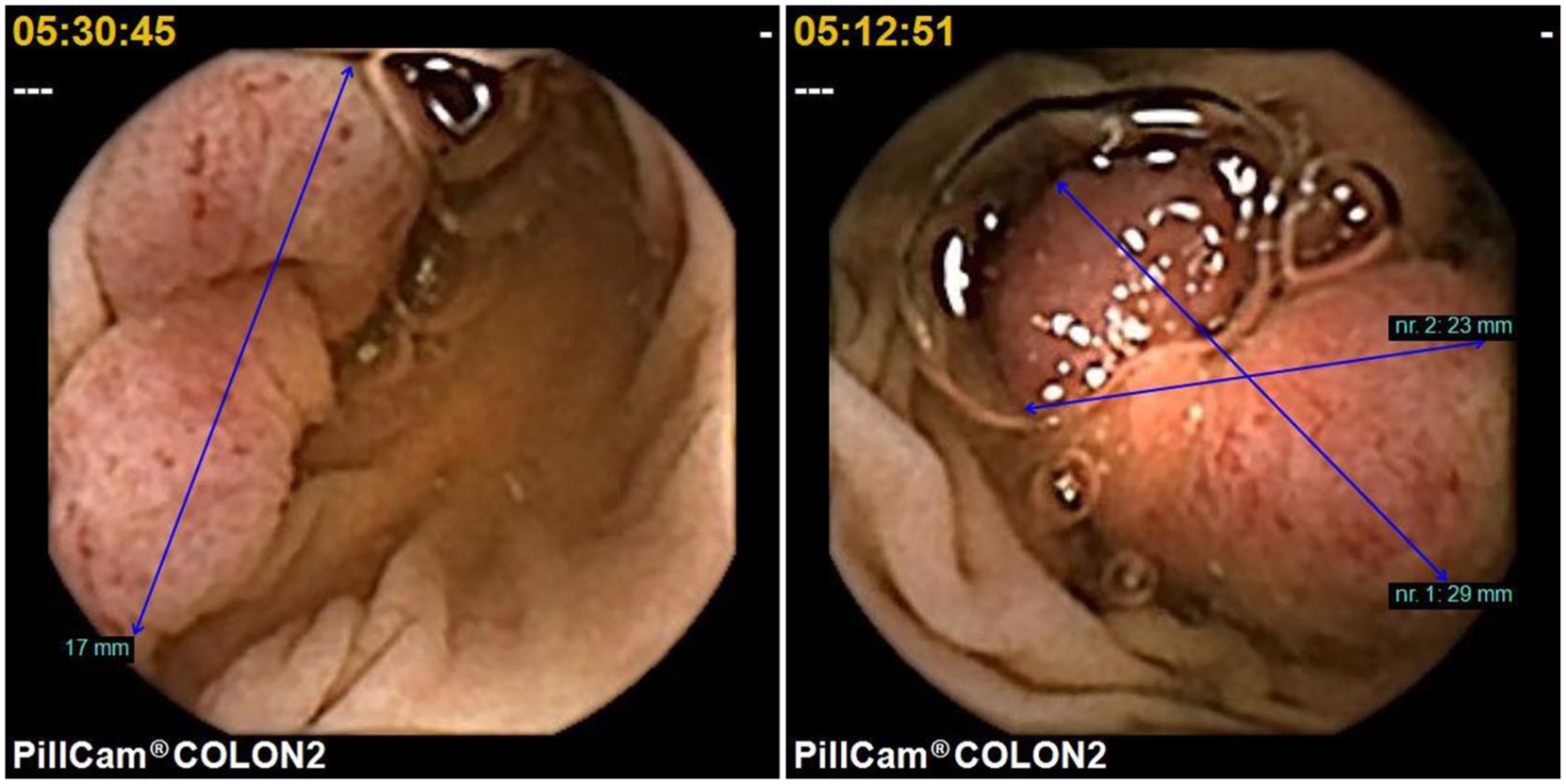
CCE images of a semicircular neoplastic colonic lesion.
Discussion
This prospective multicentre study evaluated the feasibility and diagnostic yield of CCE in FIT-positive individuals from the Dutch CRC screening programme who were unable or unwilling to undergo colonoscopy. Our findings showed that more than half of this population was ineligible for CCE due to comorbidities or contraindications for CCE evaluation. Among those who underwent CCE, the completion rate was moderate (69.2%), and adequate bowel preparation was achieved in only 38.5% of cases. Despite these limitations, CCE achieved a high per-patient polyp detection rate (76.9% for polyps ⩾6 mm), which led to a substantial number of colonoscopy referrals.
Previous studies have suggested that CCE may outperform CTC in detecting AN, demonstrating higher sensitivity for detecting small lesions in high-risk patients.20,25 However, other studies have found no significant difference between the two modalities.5,16 A recent study evaluating CTC in FIT-positives of the Dutch Colorectal Cancer Screening programme reported the detection of polyps ⩾6 mm or suspected CRC in 37.5% of FIT-positives who underwent CTC. 8 In contrast, our study found a notably higher detection rate with CCE (76.9%). Importantly, all participants with CCE-suspected polyps ⩾6 mm or CCE-suspected CRC were found at subsequent colonoscopy, although lesion size estimation by CCE was not always accurate. However, the performance of CCE in our study cannot be reliably assessed due to the low number of CCE participants and the fact that additional endoscopy was only performed with suspected lesions ⩾6 mm. Moreover, given the higher risk of AN in FIT-positive individuals compared to the general population, a substantial proportion of patients still required follow-up colonoscopy, limiting the standalone utility of CCE. These findings align with a recent study, reporting a 69.9% referral rate for subsequent colonoscopies, leading to the conclusion that CCE is not recommended in a FIT-based CRC screening setting. 26 Bowel preparation quality in our cohort was substantially lower than reported in average-risk populations. This may be attributed to reduced gastrointestinal motility in patients with higher ASA classifications, likely related to age and comorbid conditions. Taken together, our findings suggest that CCE may be better suited for individuals with a lower pre-test probability of AN and fewer procedural limitations, rather than high-risk screening populations. Potential applications include symptomatic individuals where an invasive colonoscopy can be averted by a negative CCE, or as part of a pan-endoscopic strategy. For example, in patients undergoing evaluation for anaemia or gastrointestinal bleeding who would otherwise undergo upper endoscopy followed, if negative, by colonoscopy as separate procedures. 27 In such cases, CCE could streamline diagnostic work-up and reduce the burden of hospital-based care. These scenarios, however, represent a different clinical context from the FIT-positive population studied here. For FIT-positive individuals who are unable or unwilling to undergo colonoscopy, high comorbidity, frequent contraindications, and the need for follow-up endoscopy substantially limit the suitability of CCE. For this population, efforts should instead focus on implementing a structured quality assurance programme for CTC, similar to the approach adopted in the United Kingdom. Such programmes may improve the diagnostic performance of CTC and provide a more reliable alternative in this context. Furthermore, for patients with significant comorbidities, participation in FIT-based CRC screening itself may warrant reconsideration. In this vulnerable population, the risks and burdens associated with follow-up diagnostic evaluation, such as colonoscopy, may outweigh the potential benefits.
This study has several limitations. First, the small number of participants who underwent CCE restricts the generalizability of our findings, and, therefore, diagnostic accuracy results should be interpreted with caution. No formal sample size calculation was performed, as this study was designed as a feasibility study primarily aimed at evaluating the practical applicability of CCE within this specific screening context rather than diagnostic performance. Although the sample size was insufficient to evaluate diagnostic accuracy, it realistically reflects the challenges of implementing CCE in a CRC screening programme and suggests that CCE is not suitable for populations with high comorbidity. The low uptake may partly be due to our strict eligibility criteria for CCE, such as exclusion of patients with implanted cardiac devices, although recent studies indicate that CCE-2 is generally safe in such patients. 28 However, this accounted for less than 10% of exclusions, and absolute contraindications, primarily related to bowel preparation or severe comorbidities, remained the main reasons for exclusion, underscoring that this population is inherently less suitable for CCE. Second, colonoscopy was not used as a reference standard, which limited the ability to calculate sensitivity and specificity. Third, Interobserver variability in CCE interpretation was not assessed due to the small cohort size. Despite these limitations, the overall sample size for feasibility assessment was sufficient to provide meaningful insights into the practical applicability of CCE in FIT-positive individuals who are unable or unwilling to undergo colonoscopy. Importantly, the challenges encountered, including high comorbidity, frequent contraindications, and inadequate bowel preparation, reflect real-world conditions and highlight that this population is fundamentally less suited for CCE.
Conclusion
In conclusion, CCE is not a suitable alternative to CTC for FIT-positive individuals in the Dutch CRC screening programme due to high rates of comorbidity, contraindications, and inadequate bowel preparation. Its utility may lie in other patient populations with a lower risk of AN and fewer procedural limitations.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745251415118 – Supplemental material for Applicability of colon capsule endoscopy in FIT-positive individuals unable or unwilling to undergo colonoscopy within a colorectal cancer screening programme: a prospective multicentre study
Supplemental material, sj-docx-1-cmg-10.1177_26317745251415118 for Applicability of colon capsule endoscopy in FIT-positive individuals unable or unwilling to undergo colonoscopy within a colorectal cancer screening programme: a prospective multicentre study by Fleur E. Marijnissen, Sarah Moen, Conny C. G. van Enckevort, Ivonne Leeuwenburgh, Ruud W. M. Schrauwen, Leonieke Wolters and Manon C.W. Spaander in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.