
Abstract
Background:
The optimal choice between fully covered self-expandable metallic stents (FCSEMSs) and uncovered self-expandable metallic stent (USEMS) for managing inoperable malignant distal biliary obstruction (MDBO) remains debatable. This study aims to compare the efficacy of CSEMS and USEMS in patients with MDBO.
Method:
A retrospective analysis was conducted with inoperable MDBO between January 2017 to December 2021 who underwent either USEMS or FCSEMS implantations via endoscopic retrograde cholangiopancreatography (ERCP). Primary outcomes were overall survival and stent patency. Secondary outcomes were stent occlusion rates and postoperative complications.
Results:
This study included 310 patients (235 patients received FCSEMS implantations and 75 received USEMS implantations). Median follow-up duration was 5.2 months. No significant difference was observed in overall survival between the FCSEMS and USEMS groups (167 vs 169 days, p = 0.566). The mean stent patency duration was longer in the FCSEMS group compared to the USEMS group (445 vs 348 days, p = 0.020). There were no significant differences in postoperative complications between the two groups. Multivariate analysis indicated that endoscopic sphincterotomy (EST) (HR = 1.259, 95% CI: 1.167–1.358, p < 0.001), USEMS (HR = 2.277, 95% CI: 1.750–2.963, p < 0.001), stent length (HR = 1.804, 95% CI: 1.662–1.959, p < 0.001), preoperative biliary stent (HR = 1.166, 95% CI: 1.070–1.271, p < 0.001) and non-pancreatic cancer (HR = 1.404, 95% CI: 1.299–1.516, p < 0.001) were independent risk factors for stent occlusion, while BMI ⩾ 24 kg/m2 (HR = 0.600, 95% CI: 0.548–0.657, p < 0.001) was identified as a protective factor. In the subgroup analysis for pancreatic cancer, patients with FCSEMS (n = 109) had an average survival time of 154.14 ± 93.93 days, while those with USEMS (n = 34) had an average survival time of 130.32 ± 57.31 days (p = 0.21). For non-pancreatic cancer, patients with FCSEMS (n = 115) had an average survival time of 194.10 ± 93.40 days, and patients with USEMS (n = 34) had an average survival time of 204.97 ± 93.40 days (p = 0.67).
Conclusion:
Compared to USEMS, FCSEMS provides a longer stent patency duration for patients with MDBO. However, no significant differences were found in overall survival and postoperative complications in this retrospective study.
Introduction
Biliary obstruction and the consequent obstructive jaundice occur when the bile duct is blocked or narrowed, preventing bile secretion into the intestine. 1 Patients with obstructive jaundice due to unresectable malignant distal biliary obstruction (MDBO) typically exhibit poor prognosis and low quality of life, rendering effective biliary drainage critical for symptom alleviation, preservation of organ function, and prolonged survival. 2
Endoscopic and transhepatic stent implantation are established interventions in contemporary clinical practice. Percutaneous transhepatic cholangial drainage (PTBD), an external drainage modality, offers procedural simplicity but disrupts physiological bile flow into the gastrointestinal tract, potentially compromising digestion and absorption.3,4 Depending on the techniques used during endoscopic retrograde cholangiopancreatography (ERCP), biliary stents—both plastic and metallic—are prone to occlusion within 4–6 months, limiting their long-term effectiveness. 5 Self-expandable metallic stent (SEMS) addresses multiple limitations of plastic stents by virtue of their larger luminal diameters, prolonged patency durations, and reduced occlusion rates.5,6 Among SEMSs, fully covered self-expandable metallic stents (FCSEMSs) and uncovered self-expandable metallic stents (USEMSs) are the most commonly used.7,8 Nevertheless, comparative analyses of efficacy, patient survival, stent patency, and complication profiles yield inconsistent conclusions.9–11 For example, while FCSEMSs prevent tissue ingrowth due to their covered design, they may have a higher risk of migration. Paradoxically, despite theoretical advantages for patency extension, certain clinical studies indicate comparable performance between FCSEMS and USEMS. In addition, some studies suggest that USEMS are more prone to occlusion from tumor ingrowth, while others point out that covered stents may remain vulnerable to tumor overgrowth at proximal/distal ends. Furthermore, FCSEMS may block the pancreatic or cystic duct orifices, consequently increasing the risk of pancreatitis and cholecystitis.9,12 Therefore, the optimal selection strategy remains controversial. 13
The primary objective of this study was to compare overall survival time and stent patency duration between FCSEMSs and USEMSs. Secondary objectives included comparative analysis of postoperative complications, including acute pancreatitis, acute cholecystitis, acute cholangitis, postoperative hemorrhage, stent occlusion, and stent migration between the two groups.
Methods
Patients
This single-center retrospective cohort study utilized an endoscopic reporting database to identify consecutive patients who underwent ERCP with either FCSEMS or USEMS implantation for MDBO between January 2017 and December 2021. Inclusion criteria were: age ⩾ 18 years; a confirmed diagnosis of unresectable MDBO (via imaging, pathology, or Multi-disciplinary Treatment discussion); indication for decompression due to jaundice; and primary metallic stent placement. Exclusion criteria included benign obstructions, hilar obstructions, lack of follow-up data, and prior SEMS placement. All eligible patients meeting criteria were consecutively enrolled to mitigate selection bias and ensure cohort representativeness. This study was approved by the hospital’s ethics committee (Supplemental Material).
Stent implantation procedures
ERCP was performed by experienced endoscopists under general intravenous anesthesia with prophylactic antibiotics. Duodenoscopes used were classified as TJF260, TJF240, or JF240, based on the diameter of the working channel. Endoscopic sphincterotomy (EST) or endoscopic papillary balloon dilation (EPBD) was performed at the operator's discretion before stent implantation. Both FCSEMS and USEMS (Boston Scientific, Marlborough, MA, USA, and Shandong Weixin Medical Device, Weihai, China) were used, with diameters of 10 mm and lengths of 40–80 mm. Since this was a retrospective study, the type of stent was determined by the endoscopist based on the patient’s individual circumstances (e.g., economic factors) and intraoperative conditions.
Outcomes and definitions
The primary outcomes were overall survival time and stent patency duration. Overall survival was calculated from stent insertion to death or last follow-up for surviving patients, with censoring at the final documented clinical encounter. Stent patency was defined as the interval between implantation and either recurrent obstruction or study termination. 14 Stent occlusion was defined as confirmed by recurrent jaundice necessitating unplanned reintervention. 15 Patients without obstruction events were censored at death or last follow-up. 14
Secondary outcomes included adverse events (AEs). Stent migration was diagnosed when the SEMS moved more than 2 cm from its initial position, either proximally or distally. 16 Stent occlusion was identified based on symptoms such as cholangitis, jaundice, or cholestasis. 9 Clinical remission was defined as normalization of total bilirubin (⩽1.3 mg/dL) or a reduction of at least 30% within 7 days after stent replacement. 9 Post-ERCP pancreatitis (PEP) was defined as new or worsened abdominal pain with serum amylase levels exceeding three times the normal upper limit. Cholangitis was defined as persistent jaundice with serum bilirubin levels above 30 µ/L and cholestasis lasting more than 24 h, accompanied by fever (>38°C). Cholecystitis was characterized by fever (>38.5°C) for more than 24 h, new right upper abdominal pain, a positive Murphy’s sign, and corresponding imaging findings.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) or median [P 25, P 75], while categorical variables were presented as n (%). Normally distributed continuous variables were compared using the independent sample t-test, and non-normally distributed variables were compared using the Mann–Whitney U test. Categorical variables were compared using the chi-square test or Fisher's exact test. Stent patency and patient survival were assessed using Kaplan–Meier plots with the log-rank test. Risk factors for stent occlusion were analyzed using univariate and multivariate Cox proportional hazards models. Statistical significance was set at p < 0.05. All statistical analyses were conducted using SPSS version 25.0 (IBM Corp., Armonk, New York, USA).
Results
Study population
This retrospective study analyzed 310 patients who underwent biliary stenting, with 235 receiving FCSEMS and 75 receiving USEMS. The demographic and clinical characteristics of the two groups were similar (Table 1; Figure 1).
Patients demographics.

ASA, American Society of Anesthesiologists; BMI, body mass index; CBD, common bile duct; EPBD, endoscopic papillary balloon dilatation; FCSEMS, fully covered self-expandable metallic stents; IQR, interquartile range; PTCD, percutaneous transhepatic cholangial drainage; SD, standard deviation; TBIL, total bilirubin; USEMS, uncovered self-expandable metallic stents.
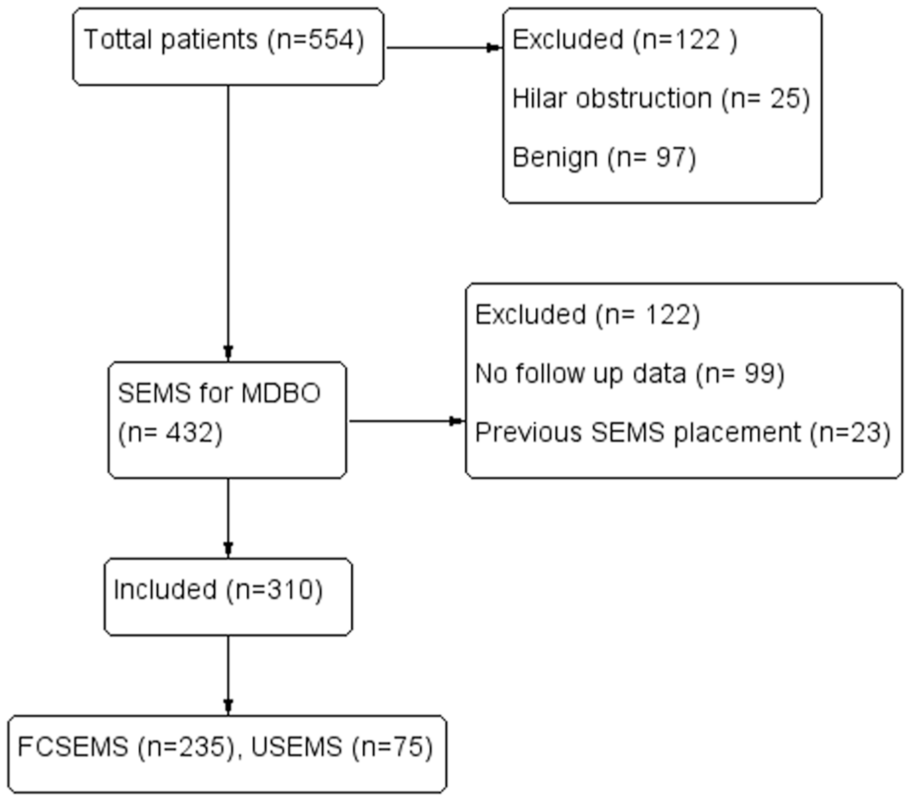
Screening, exclusion, and final study population.
Therapeutic details
In terms of therapeutic interventions (Table 2), both groups had similar proportions of patients receiving endoscopic nasal biliary drainage, pancreatic duct stenting, octreotide, antibiotics, somatostatin analogs, as well as comparable operative times and hospital stays. However, the use of 60 mm stents was significantly higher in the FCSEMS group (56.0% vs 69.8%, p < 0.001). Notably, EST was performed significantly more often in the USEMS group compared to the FCSEMS group (73.3% vs 51.1%, p < 0.001).
Therapeutic details.

ENBD, endoscopic nasobiliary drainage; EST, endoscopic sphincterotomy; FCSEMS, fully covered self-expandable metallic stents; IQR, interquartile range; USEMS, uncovered self-expandable metallic stents.
Primary outcomes
The clinical remission rates were statistically similar between the two groups (85.3% vs 81.3%, p = 0.423) (Table 3). The median stent patency duration favored the FCSEMS group (445 vs 348 days, p = 0.02) (Figure 2). However, no significant difference in overall survival was observed between the groups (167 vs 169 days, p = 0.566) (Figure 3).
Clinical outcomes and adverse events in two groups.

CI, confidence interval; FCSEMS, fully covered self-expandable metallic stents; USEMS, uncovered self-expandable metallic stents.
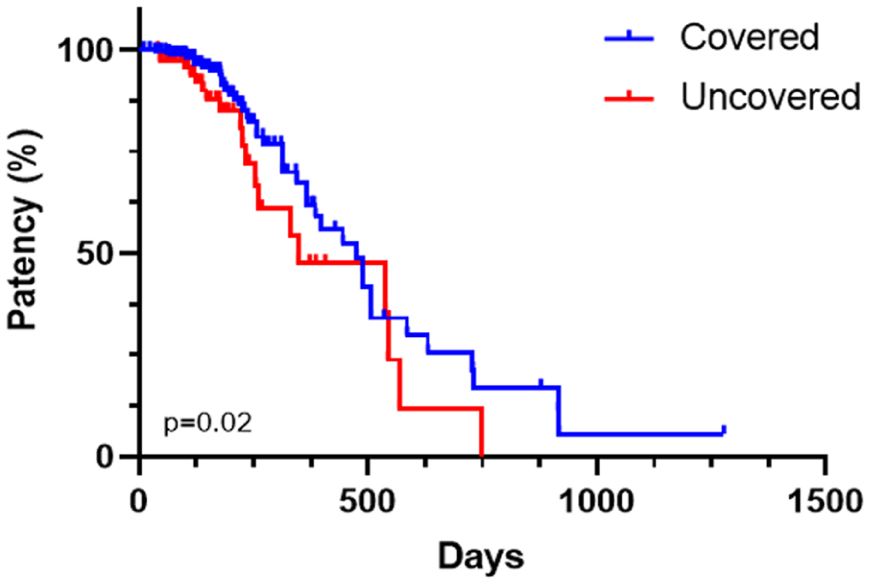
Kaplan–Meier curve of cumulative stent patency. Stent patency was significantly higher (p = 0.020) in covered than in uncovered SEMSs.

Kaplan–Meier plot of cumulative patient survival. No significant difference was observed between covered and uncovered SEMS.
In the subgroup analysis for pancreatic cancer, patients with FCSEMS (n = 109) had a mean survival time of 154.14 ± 93.93 days, while patients with USEMS (n = 34) had a mean survival time of 130.32 ± 57.31 days (p = 0.21) (Figure 4). For non-pancreatic cancer, patients with FCSEMS (n = 115) had a mean survival time of 194.10 ± 93.40 days, while patients with USEMS (n = 34) had a mean survival time of 204.97 ± 93.40 days (p = 0.67) (Figure 5).

Kaplan–Meier curve for pancreatic tumors.

Kaplan–Meier curve for non-pancreatic tumors.
Secondary outcomes
Acute pancreatitis occurred in 23 patients (7.4%): 5 of 75 (6.7%) in the USEMS group and 18 of 235 (7.7%) in the FCSEMS group (p = 0.775). Three patients underwent EST, and pancreatic duct stenting was required in two USEMS patients and nine FCSEMS patients. (Table 3, Figure 6)
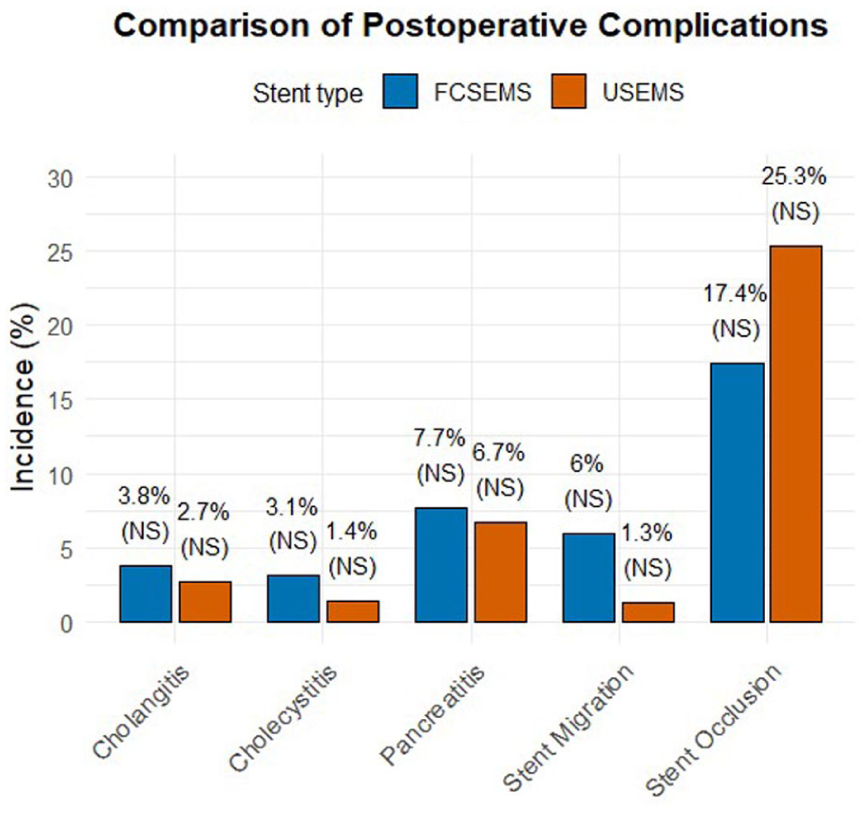
Postoperative complications in covered and uncovered SEMS.
The incidence of cholecystitis was 2.7% (8/298) in all patients with the gallbladder in situ, with 1 patient in the USEMS group (1.4%) and 7 in the FCSEMS group (3.1%; p = 0.716). No significant difference was found between the groups (1.4% vs 3.1%, p = 0.684). Except for one patient who underwent percutaneous transhepatic gallbladder drainage (PTGD), all other cases were successfully managed conservatively.
Postoperative cholangitis occurred in 11 patients (3.5%): 2 patients in the USEMS group and 9 in the FCSEMS group (2.7% vs 3.8%, p = 0.908). All patients received successful conservative management, and no postoperative bleeding events were recorded.
Stent migration was numerically higher in the FCSEMS group (6% vs 1.3%), though this difference was not statistically significant (p = 0.188), likely due to the low incidence and limited sample size. For early migrations (within 1 month postoperatively), repositioning, including balloon adjustment and stent retrieval with re-implantation, was considered. For persistent displacement, placement of a new stent was suggested. Given the technical challenges of removing USEMS, re-implantation of a new stent is generally preferred.
Stent occlusion occurred in 20% of all patients (62/310), with 19 patients (25.3%) in the USEMS group and 43 patients (17.4%) in the FCSEMS group (p = 0.132) (Table 3). In cases of stent obstruction due to tumor overgrowth or ingrowth, a new stent should be placed. If obstruction is due to gallstones, the stones should be removed, and the stent should be retained.
A univariate analysis followed by a multivariate analysis was performed on variables that showed statistically significant differences to explore risk factors for stent occlusion. In the univariate analysis, EST (HR 1.233, 95% CI: 1.147–1.303, p < 0.001), BMI > 24 kg/m2 (HR 0.689, 95% CI: 0.637–0.745, p < 0.001), USEMS (HR 2.20, 95% CI: 1.749–2.768, p < 0.001), stent length >70 mm (HR 1.89, 95% CI: 1.752–2.043, p < 0.001), and non-pancreatic cancer (HR 1.470, 95% CI: 1.376–1.571, p < 0.001) were associated with stent occlusion. In the multivariate Cox regression analysis, EST (HR 1.259, 95% CI: 1.167–1.358, p < 0.001), USEMS (HR 2.277, 95% CI: 1.750–2.963, p < 0.001), stent length >70 mm (OR 1.804, 95% CI: 1.662–1.959, p < 0.001), preoperative biliary stent (HR 1.166, 95% CI: 1.070–1.271, p < 0.001), and non-pancreatic cancer (HR 1.404, 95% CI: 1.299–1.516, p < 0.001) were identified as independent risk factors for stent occlusion. BMI > 24 kg/m2 emerged as an independent protective factor against stent occlusion (HR 0.600, 95% CI: 0.548–0.657, p < 0.001) (Table 4). This may be due to the secretion of inflammatory factors and cytokines from adipose tissue, which could offer protection to the biliary mucosa and inhibit stone and precipitate formation.
Analysis of factors associated with stent occlusion.

ENBD, endoscopic nasobiliary drainage; EST, endoscopic sphincterotomy; FCSEMS, fully covered self-expanding metal stent; GB, gallbladder; HR, hazard ratio; USEMS, uncovered self-expandable metal stent.
Discussion
Endoscopic stent implantation via ERCP has been widely adopted for managing MDBO, providing a more physiologically compatible solution and enhancing the quality of life. SEMS offer a larger diameter and higher patency rates compared to plastic stents. 5 While USEMS are effective, they carry a risk of occlusion due to tumor ingrowth. 17 FCSEMS incorporating specialized coatings to prevent tumor ingrowth. 9 However, some issues remain unclear, such as tumor overgrowth and sludge accumulation. It is important to acknowledge that this retrospective, single-center design of this study introduces potential selection biases, and the criteria for selecting FCSEMS or USEMS were influenced by both the endoscopist’s preference and the patient’s financial situation, potentially introducing group imbalances. To address this, we conducted multivariate regression adjusting for baseline confounders. Importantly, our cohort reveals significant geographic variations in patient demographics compared to Western populations, with national health insurance policies critically impacting stent selection—a contextual determinant underrepresented in existing literature.
This study demonstrated comparable overall survival between FCSEMS and USEMS cohorts, with equivalent therapeutic response rates consistent with prior reports.2,12,18 As hypothesized, FCSEMS exhibited significantly prolonged stent patency compared to USEMS (445 vs 348 days, p < 0.05). This finding contrasts with several high-quality studies reporting non-superior patency for FCSEMS.14,17,19,20 Three meta-analyses yield divergent conclusions: two support FCSEMS patency advantage, while another shows a 32% risk reduction in stent failure with FCSEMS, though this difference was not statistically significant.13,21,22 Subgroup analysis revealed a pronounced advantage for FCSEMS in patients with pancreatic malignancies and cholangiocarcinoma, but no significant difference was found for ampullary cancer or gallbladder cancer.13,21 Our cohort's predominant pancreatic cancer composition which consistent with epidemiological patterns. Therefore, we performed subgroup analyses stratified by tumor type (pancreatic vs non-pancreatic), which showed consistent outcomes across subgroups. However, these efforts could not entirely mitigate the potential bias. We hypothesize that tumor biology contributes to the heterogeneity in stent patency outcomes.
Regarding postoperative complications, no significant differences were observed between the FCSEMS and USEMS groups. The incidence of postoperative cholecystitis in previous studies ranges from 1% to 7.8%.14,20 Jang et al. 14 reported a higher incidence of acute cholecystitis in the FCSEMS group; other studies found no significant differences between the two groups, which is consistent with our results.9,15,19 Theoretically, complete mesh coverage by FCSEMS may impede bile drainage from the gallbladder, while USEMS could reduce this complication due to the uncovered mesh. However, the plasticity of soft tissue must also be considered: compression of the cystic duct opening by USEMS may lead to gallbladder dysfunction, causing cholecystitis. 15 Although the incidence of cholecystitis was nearly twice as high in the FCSEMS group compared to the USEMS group (3% vs 1.3%), the difference was not significant (p = 0.716), likely due to the low number of cases observed (1/74 and 7/224), and which is potentially related to the study's sample size and retrospective nature, limits the statistical power to detect significant differences in relatively rare complications.
Furthermore, neither stent occlusion nor stent migration showed significant intergroup differences. While two randomized controlled trials (RCTs) indicated higher stent occlusion rates in USEMS due to tumor ingrowth susceptibility, other studies reported similar incidences, suggesting multifactorial pathogenesis involving stent occlusion, such as tumor ingrowth, tumor overgrowth, sludge formation, mechanical tumor extrusion, and gallbladder stones.9,20 Conversely, FCSEMS demonstrate theoretical migration vulnerability due to absent tissue embedding, though clinical evidence remains conflicting. A recent meta-analysis refuted the superiority of USEMS in preventing migration, as migration is influenced not only by stent type but also by factors, such as EST application and primary tumor types. 13 It is noteworthy that due to the retrospective nature of this study, we were unable to collect detailed information on tumor ingrowth, overgrowth, gallbladder stones, reintervention rates, and biliary inflammation, which would have been beneficial for further subgroup analysis. Future studies, including RCTs or large-scale real-world studies, are needed to provide more definitive results.
Conclusion
Both FCSEMS and USEMS provide effective palliation for unresectable MDBO. While demonstrating comparable median overall survival (169 vs 167 days, p = 0.67), FCEMS significantly prolonged stent patency (445 vs 348 days, p = 0.02). No major disparities in postoperative complications were identified. Multivariate analysis indicated that EST, USEMS, stent length >70 mm, preoperative biliary stent, and non-pancreatic cancer were independent risk factors for stent occlusion. Tumor-stratified subgroup analyses (pancreatic vs non-pancreatic) demonstrated outcome homogeneity across cohorts.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745251376845 – Supplemental material for Comparison of fully covered versus uncovered self-expandable metallic stents in treating inoperable malignant distal biliary obstruction: a retrospective study
Supplemental material, sj-docx-1-cmg-10.1177_26317745251376845 for Comparison of fully covered versus uncovered self-expandable metallic stents in treating inoperable malignant distal biliary obstruction: a retrospective study by Di Zhang, Ting Luo, Feng Gao, Yong Sun, Zihao Dai, Jiao Liu, Jiangning Gu and Zhuo Yang in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.