
Abstract
Background:
Dysphagia is the most frequent symptom in patients diagnosed with esophageal cancer. Self-expanding metal stents (SEMS) are the current palliative treatment of choice for dysphagia in patients with non-curable esophageal cancer. This study aimed to evaluate the efficacy and adverse events (AEs) of different types of SEMS for palliation of dysphagia.
Methods:
We performed a retrospective cohort study of patients with advanced esophageal cancer and SEMS placement for dysphagia palliation in a tertiary care center. The primary outcome was the clinical success defined as an improvement in dysphagia (reduction of at least 2 points in the Mellow–Pinkas scoring system for dysphagia) after SEMS placement.
Results:
Between January 1999 and May 2020, 295 patients with esophageal cancer were identified. Among them, 75 had a SEMS placement for dysphagia palliation. The mean age of the patients was 61.3 years (standard deviation: 13.4), 69 patients (92%) were men, and the mean Mellow–Pinkas scoring for dysphagia pre- and post-SEMS placement were 3.1 and 1.4 (change from baseline −1.7), respectively. Technical success and clinical success were achieved in 98.6% and 58.9%, respectively. AEs were identified in 35/75 patients (46.7%), and SEMS migration was the most frequent AE in 22/75 patients (29.3%). There were no significant differences in improvement in dysphagia (p = 0.054), weight changes (p = 0.78), and AE (p = 0.73) among fully covered SEMS (fc-SEMS) and partially covered SEMS (pc-SEMS). The median follow-up was 89 days (interquartile range: 29–221).
Conclusion:
SEMS placement was associated with a rapid improvement in dysphagia, high technical success, and a modest improvement in dysphagia with no major AE among fc-SEMS and pc-SEMS.
Introduction
Esophageal cancer is one of the eighth most common cancers and the sixth most lethal cancer worldwide. 1 Dysphagia is the most common symptom, suggesting an advanced stage disease. 2 Patients with malignant dysphagia have a poor quality of life and are often malnourished. One of the main goals in the treatment of these patients is to offer rapid relief of dysphagia and improve their nutritional status. Several options have been described for dysphagia palliation, including esophageal dilatation, 3 radiotherapy/brachytherapy,4,5 cryotherapy, 6 photodynamic therapy, and argon plasma coagulation. 7
Self-expanding metal stent (SEMS) placement is currently considered the treatment of choice for malignant dysphagia palliation according to the European Society of Gastrointestinal Endoscopy (ESGE) 8 and the American Gastroenterological Association (AGA). 9 On average, SEMS reduces dysphagia symptom scores by 2 points in validated dysphagia scales (0–4). 10 However, SEMS placement can be associated with adverse events (AE), the most common are migration, obstruction, bleeding, chest pain, fistula, and perforation. Today, there seems to be no difference in efficacy and AE among partially covered (pc) and fully covered (fc) SEMS, although a recent study suggested that pc-SEMS were associated with lower rates of stent migration, which is the most common AE, and a similar obstruction rate compared to fc-SEMS. 11 Nonetheless, this study was not restricted only to patients with esophageal cancer.
The aim of this real-life study was to evaluate the efficacy and adverse effects of different types of SEMS for palliation of dysphagia in patients with inoperable esophageal cancer.
Patients and methods
Study design
A retrospective cohort study in a tertiary care center during the period from January 2009 to May 2020 was realized. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline for reporting observational studies was followed.
Eligibility criteria
We selected all patients with inoperable esophageal cancer undergoing SEMS placement as palliation for malignant dysphagia identified in the hospital records. The diagnosis of esophageal cancer was confirmed histopathological in biopsies obtained by endoscopy. Patients with other indications for SEMS placement (fistula, perforation, radiation stricture, benign anastomotic stricture) were excluded. Demographic, clinical, and laboratory data were collected from electronic records.
Outcomes
The primary outcome was the improvement in dysphagia, evaluated pre- and post-stent placement with the Mellow–Pinkas scoring system for dysphagia 12 : 0, able to eat a normal diet/no dysphagia; 1, able to swallow some solid food; 2, able to swallow only semisolid food; 3, able to swallow liquids only; and 4, complete dysphagia. The post-stent score was evaluated in the next medical visit as an outpatient.
Clinical success was defined as a reduction of at least 2 points in the Mellow–Pinkas scoring system for dysphagia. Technical success was defined as a deployment of the stent across the stricture with patency visualized both endoscopically and fluoroscopically.
We assessed the weight change pre- and post-stent, using the last recorded weight in the electronic record before SEMS placement and the last recorded weight during the follow-up. We evaluated the following complications or AE taking into account the definitions of the lexicon for endoscopic AEs proposed by the American Society of Gastrointestinal Endoscopy (ASGE) 13 when pertinent: migration, defined as clinically significant dysphagia associated with a displaced stent (proximally or distally) evaluated by endoscopy; bleeding, defined as the presence of hematemesis or melena after SEMS placement with endoscopic evidence of blood in the area covered by the stent; and perforation, defined as evidence of air or luminal contents outside the gastrointestinal tract documented after SEMS placement. Other AE evaluated were food impaction, tumoral obstruction, and fistula.
Endoscopy and SEMS placement
All procedures were done or supervised by expert endoscopists in SEMS placement, under fluoroscopy guidance. All endoscopies were done with a standard diagnostic endoscope (outer diameter: 9.8 mm) to evaluate the characteristics of the stricture. In the cases in which the malignant stricture was not traversable, pediatric endoscopes (Olympus XP160 and XP180, Tokyo, Japan) were used to evaluate the stricture’s extension. The choice of the stent type was at the physician’s discretion.
Statistical analysis
Numerical variables are presented in mean and standard deviation (SD) or median and interquartile range (IQR) as appropriate and categorical variables are reported in frequencies and proportions. The mean change in the Mellow–Pinkas scoring system for dysphagia and in weight before and after SEMS placement was compared using a paired t-test.
The incidence rate of AE was computed by dividing the number of AE over the total person-time at risk after SEMS placement, and its 95% confidence interval was computed by treating the denominator as fixed and estimating 95% confidence limits for the number of events using the Poisson distribution. For patients who died before having a stent-related AE, the time to the AE was censored at the time of death. The cumulative incidence of AE at 30, 90, and 180 days and the median time to an AE were computed using the Kaplan–Meier estimator and compared between patients with fully covered versus partially covered SEMS using the log-rank test (unadjusted comparison). For the adverse effect of migration, time to migration was compared between patients with fully covered (fc) versus partially covered (pc) SEMS using the log-rank test (unadjusted comparison); for this analysis perforation, fistula and tumoral obstruction were considered as censoring events because the stent was replaced, and these events were assumed not informative with respect to having a stent migration. Death was also considered a censoring event for both comparisons and assumed non-informative of having a stent-related AE.
The relationship between SEMS type (partially covered versus completed covered) and AE was assessed more rigorously using an unadjusted and three adjusted Cox proportional hazard Cox models. The first adjusted model controlled for tumor length and malignant stricture (traversable versus not traversable with a standard endoscope), the second model further controlled for pre-stent therapy (chemotherapy ± radiotherapy), and the third model also controlled for post-stent therapy (chemotherapy ± radiotherapy). The proportional hazard assumption was assessed for each model using the Schoenfeld residuals. For patients who died before having a stent-related AE, death was considered a censoring event and assumed non-informative with respect to having a stent-related AE.
The data were analyzed using R version 4.1.2. R is a free software under the terms of the Free Software Foundation’s GNU General Public License in source code form. The confidence level was established as 0.05 at two-tailed.
Results
Patients and demographic characteristics
Between January 2009 and May 2020, 295 patients with a diagnosis of esophageal cancer were identified. Among them, 106 had a SEMS placement, of whom 75 had the SEMS placed as palliation for malignant dysphagia in the context of inoperable cancer and had complete information (Figure 1).

Flow chart.
The demographic and clinical data of all patients are shown in Table 1. The mean age was 61.3 years (SD: 13.4), 92% (n = 69) were male and 67% (n = 50) were in disease stage IV at the time of the procedure. Adenocarcinoma was the most common cancer type presented in 67% (n = 50), followed by squamous cell carcinoma in 32% (n = 24). Thirty-one percent (n = 23) received combined treatment with chemotherapy plus radiotherapy (Ct + Rt) before SEMS placement, 32% (n = 24) received only chemotherapy (Ct), and 5% (n = 4) only radiotherapy. After SEMS placement, 31% (n = 23) were treated with Ct, 5% (n = 4) with Rt, and another 5% (n = 4) with the combination of Ct + Rt.
Baseline characteristics of the patients.

Endoscopic characteristics of the esophageal tumors
The characteristics of esophageal tumors are shown in Table 2. Most tumors were in the lower third of the esophagus (52%, n = 39), 27% (n = 20) affected the middle third and 20% (n = 15) affected both the middle and lower third. The esophagogastric junction (EGJ) was involved in 60% (n = 45) of the cases. Median tumor length was 6 cm (IQR: 4–8). Forty-eight percent (n = 36) of the strictures were not traversable with a standard diagnostic endoscope, of which 81% (n = 29) were traversable with a pediatric endoscope.
Endoscopic tumor characteristics.

EGJ, esophagogastric junction; cm, centimeter; mm, millimeter; IQR, interquartile range; SEMS, self-expanding metal stent.
Efficacy and AE
Technical success was achieved in 99% of the cohort (n = 74). Four patients (5%) required endoscopic dilation immediately before SEMS placement. In total, 52 fc-SEMS (69.3%) and 23 pc-SEMS (30.7%) were placed. The type and frequency of stents models were as follows: 35% (n = 26) Wallflex (Boston Scientific, Marlborough, MA, USA), 27% (n = 20) SX-ELLA Stent Esophageal HV (ELLA-CS, Hradec Králové, Czech Republic), 20% (n = 15) Ultraflex (Boston Scientific), 9% (n = 7) Niti S stent (Taewoong Medical, Seoul, Korea), 5% (n = 4) Microtech Esophageal stent (Micro-Tech Endoscopy, Ann Arbor, MI, USA), and 4% (n = 3) other manufacturers 3/75. Most of the pc-SEMS (n = 19/23, 82.8%) had a diameter of 18 mm, whereas most of the fc-SEMS had a diameter of ⩾20 mm (n = 44/52, 84.6%). For a complete description of the stent’s length and diameter, please see Supplemental Table 1.
Dysphagia has assessed pre- and post-SEMS placement only in 73 patients, of whom 95% (n = 69) reported an improvement after SEMS placement and 59% (n = 43) achieved clinical success (a reduction of at least 2 points in the Mellow–Pinkas scoring system for dysphagia); the average reduction in the scoring system for dysphagia was 1.7 points, 95% confidence interval (CI) from 1.5 to 1.9 points. In patients with fc-SEMS and pc-SEMS, the average reduction in the scoring system for dysphagia was – 1.8 (95% CI: −2.0, −1.6, p < 0.001) and – 1.5 (95% CI: −1.7, −1.2, p < 0.001), respectively, with no significant difference between them (p = 0.054). Regarding the involvement of the EGJ by the tumor, we did not find any significant difference in the improvement in dysphagia among those with and without involvement (Supplemental Table 2).
Information about the weight change before and after SEMS placements was available only for 58 individuals. Mean pre-SEMS and post-SEMS weights were 60 kg (SD: 14.4) and 55.5 kg (SD: 11.2), respectively, and the mean weight change was a loss of 4.5 kg (95% CI: 2.5–6.6 kg). We did not identify any significant difference in weight change among fc-SEMS and pc-SEMS (p = 0.78). Detailed information regarding dysphagia and weight change assessments pre- and post-SEMS placement are shown in Table 3.
Dysphagia and weight changes pre- and post-SEMS placement.
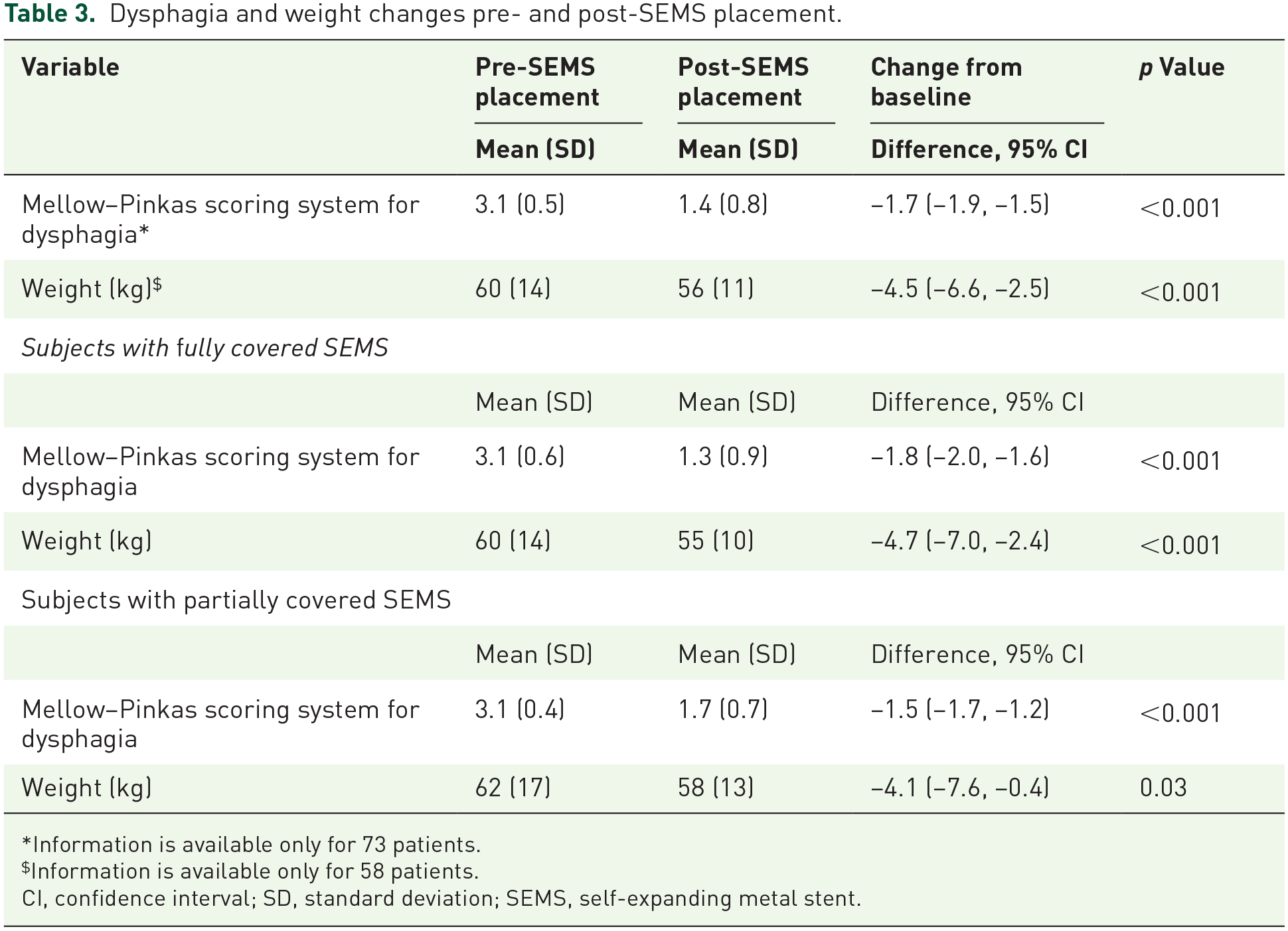
Information is available only for 73 patients.
Information is available only for 58 patients.
CI, confidence interval; SD, standard deviation; SEMS, self-expanding metal stent.
Overall, the studied patients were followed-up after SEMS placement for a median time of 89 days (IQR: 29–221), during which 40% (n = 30) experienced a stent-related adverse effect, being stent migration the most common which happened in 28% (n = 21) of the cohort. Other complications were bleeding in 4% (n = 3), perforation in 4% (n = 3), food impaction in 3% (n = 2), tumoral obstruction in 3% (n = 2), and fistula in another 3% (n = 2; see Table 4). A total of 28 patients in the cohort required a reintervention; the main reason for that was SEMS migration in 64% (n = 18).
Complications and AE.

Four patients had two complications or AEs.
AE, adverse events; SEMS, self-expanding metal stent.
The median time to an AE was 150 days (95% CI: 106–335), the incidence rate was 12.4 events per 100 person-months (95% CI: 8.4–17.5), and the cumulative incidences at 30, 90, and 180 days were 15.5%, 32.8%, and 56.6%, respectively [Figure 2(a)]. The median time to a stent-related AE and the incidences were similar in patients with a partially covered and with a fully covered SEMS [median time to an adverse effect of 90 days versus 150 days, incidence rate of 13.7 versus 11.9 events per 100 person-months, cumulative incidence at 30 days of 19.9% versus 13.9%, at 90 days of 54.2% versus 27.5%, and 180 days of 54.2% versus 57.2%, p = 0.73; see Figure 2(b)].Regarding the incidence of migration, it was similar in patients with a partially covered and with a fully covered SEMS (p = 0.53); however, although not statistically significant, compared with patients with an fc-SEMS, the incidence of stent migration in those with a partially covered SEMS was higher before 90 days and lower afterward (see Figure 3).

Stent-related AE-free survival. (a) Overall. (b) Stratified by SEMS type.
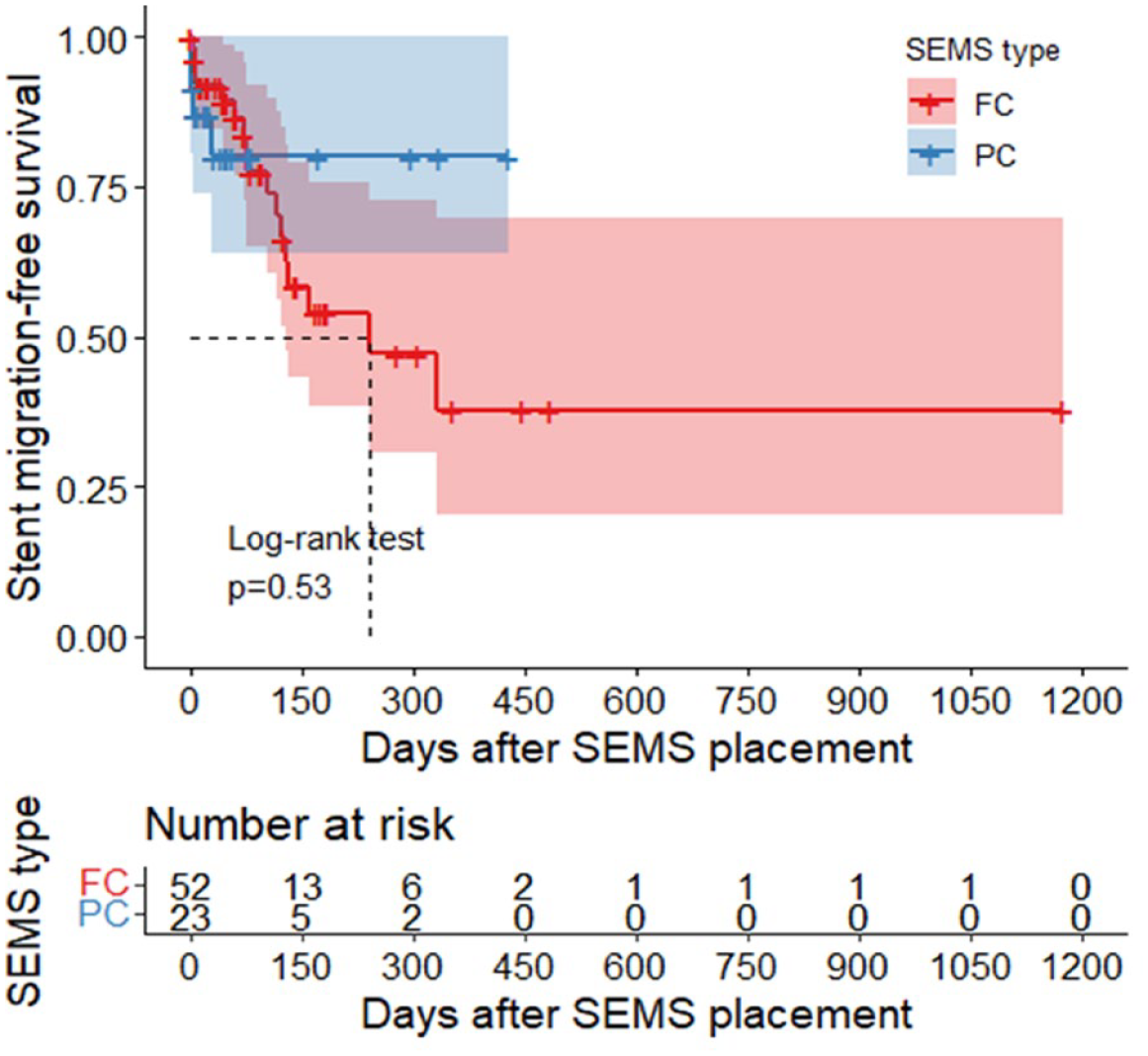
Stent migration-free survival stratified by SEMS type.
In the more rigorous assessment of the relationship between SEMS type and AE (Table 5), neither the unadjusted model nor the models that controlled for potential confounders were able to identify a different hazard of AE between subjects who received a partially covered or a fully covered SEMS. According to the adjusted model 3, controlling for tumor length, malignant stricture, and pre-stent and post-stent therapy, the hazard of adverse effects in subjects with a partially covered SEMS is 1.35 times (95% CI: 0.55–3.30, p = 0.51) the hazard in subjects with a completely covered SEMS.
Hazard ratio of AEs for having a partially covered versus a completely covered SEMS.

AEs, adverse events; CI, confidence interval; HR, hazard ratio; SEMS, self-expanding metal stents.
Discussion
In this retrospective cohort study, we evaluated the experience of SEMS placement in the palliative treatment of malignant dysphagia in patients with esophageal cancer in a National Cancer Center. We observed that technical success in SEMS placement is high and that most patients will obtain some improvement in their dysphagia degree. Our study supports SEMS placement as the first-line palliative treatment of malignant dysphagia in patients with incurable esophageal cancer because of its safety and rapid relief.14,15 Technical success is high in almost all studies, with reported success rates between 91% and 100%.16 –18 In our study, technical success was achieved in 99% and results in congruency with previous studies. Dysphagia is the predominant symptom in patients with advanced esophageal cancer and is generally associated with a dismal prognosis. Improvement in dysphagia is an important outcome in patients with malignant dysphagia. Different dysphagia scores have been developed to evaluate it, with most studies defining clinical success as a reduction of at least 2 points.12,19,20 Alonso-Lárraga et al. reported a decrease of at least 2 points in 90% of the patients. In another study, 16 Didden et al. reported improvement in dysphagia as at least one point reduction in dysphagia score, with a success rate of 83% and 88% in patients with fc-SEMS and partially covered-SEMS, respectively. 17 Finally, Verchur et al. reported an improvement in dysphagia scores from a median of 3–1 with both fc-SEMS and pc-SEMS. 21 In our cohort, most patients expressed an improvement in their dysphagia score after SEMS placement, but only 43/73 (58.9%) met our definition of clinical success (reduction of at least 2 points in the Mellow–Pinkas scoring system for dysphagia), with a mean reduction of −1.7 (95% CI: −1.9, −1.5, p < 0.001) and no significant difference between fc-SEMS and pc-SEMS.
Moreover, weight loss is the second most frequent clinical symptom in patients with advanced esophageal cancer, related to low food intake associated with dysphagia. 22 Median weight loss in patients with esophageal cancer is the highest compared to other oncologic entities. 23 Only a few studies have evaluated weight changes after SEMS placement. 24 Das et al. reported a percentage change from baseline weight at 60 days of −2.98% ± 9.16% after SEMS placement. 11 Lecleire et al. reported a mean weight loss at 3 and 6 months of 2.5 kg and 5.6 kg, respectively. 23 In the present study, we observed a mean weight loss of 4.5 kg during the patient’s follow-up.
SEMS placement is a procedure that can be associated with diverse AE including migration, perforation, bleeding, chest pain, and tumoral obstruction. Overall morbidity associated with SEMS placement in our study was 44%. Migration was the most frequent AE in 28% (21/75). Migration has been reported in 5–40% in the context of palliation of malignant dysphagia. 11 The COPAC study, the first randomized controlled study to compare fc-SEMS versus pc-SEMS, did not show any significant differences in migration rates among these types of stents. 17 In a meta-analysis done by Wang et al., they did not find any differences in terms of migration among both types of stents (fc-SEMS and pc-SEMS) [odds ratio (OR): 0.63, 95% CI: 0.37–1.08, p = 0.09; I 2 = 0%]. 25 More recently, Das et al. reported a lower incidence rate of migration with pc-SEMS in comparison with fc-SEMS (10.9% versus 25.3%, p < 0.003). 11 In a multivariate analysis, they identified that stenosis traversable with standard endoscopes and placement of fc-SEMS are risk factors for stent migration. It is important to consider that in the previous study, almost 30% of the patients had other malignant neoplasms (breast, lung) aside from esophageal cancer. In contrast to the previous study, we compared AE (including migration) rates among fc-SEMS and pc-SEMS only in patients with advanced esophageal cancer using an unadjusted and three adjusted Cox proportional hazard Cox models and including the risk factors associated with SEMS migration (SEMS type, traversable with a standard endoscope, pre- and post-tumor length, and pre-stent and post-stent therapy), with no difference in AE rates.
Our findings must be interpreted in the context of this study’s potential limitations. First, the retrospective design has the probability of bias that we tried to minimize using unadjusted and three adjusted Cox proportional hazard models. Second, the sample is limited to 75 patients. Third, this is a single-center study in a reference national center.
In conclusion, our results support that SEMS placement is associated with an improvement and a rapid relief of dysphagia, with high technical success with no major differences in efficacy and AE among fc-SEMS and pc-SEMS.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745231200975 – Supplemental material for Efficacy and safety of self-expanding metal stents in patients with inoperable esophageal cancer: a real-life study
Supplemental material, sj-docx-1-cmg-10.1177_26317745231200975 for Efficacy and safety of self-expanding metal stents in patients with inoperable esophageal cancer: a real-life study by José Miguel Jiménez-Gutiérrez, Juan Octavio Alonso-Lárraga, Angélica I. Hernández-Guerrero, Leonardo Saul Lino-Silva and Antonio Olivas-Martinez in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.