
Abstract
Background:
Colonoscopic polypectomy significantly reduces the incidence of colorectal cancer, but it carries potential risks, with colonic perforation being the most common and associated with significant morbidity.
Objectives:
This study evaluated the clinical outcomes and risk factors of microperforation during colonoscopic polypectomy.
Design:
A retrospective cohort study.
Methods:
We retrospectively reviewed the patients’ records who underwent colonoscopic polypectomy and subsequent plain radiographic examination to monitor perforation. Patients with pneumoperitoneum detected on plain radiography were enrolled. Patients who underwent adverse event-free colonoscopic polypectomies within 1 week of each case and were matched 2:1 by age and sex to the cases were selected as controls.
Results:
Microperforations occurred in 12 patients (8 males; age: median 64.5 years). Polyps with microperforations were more frequent in the right colon (83.3% vs 33.3%). Endoscopic mucosal resection with precutting (EMR-P; 16.7% vs 0.0%) or hot-snare polypectomy (8.3% vs 0.0%) was more frequently performed in the microperforation group. Muscle fibers at the polypectomy site were more frequently visible in the microperforation group (58.3% vs 8.3%). By multivariate analysis, right colon location and visible muscle fibers were independent risk factors for microperforation. All patients with microperforation received intravenous antibiotics and were advised to fast. Patients responded well to these conservative treatments and were discharged after a median of 3 (2–6.75) days of hospital stay.
Conclusion:
Our data suggest that conservative treatment is feasible and could be the primary management option for selected patients with microperforations postcolonoscopic polypectomy. Right-sided colonic polyps and visible muscle fibers predispose to microperforations.
Introduction
The incidence of colorectal cancer is markedly reduced, from 76% to 90%, by colonoscopic polypectomy. 1 This frequently performed procedure is relatively safe but is associated with adverse events such as bleeding, perforation, and postpolypectomy coagulation syndrome.2 –5 Among these, colonic perforation is the most common and is associated with considerable morbidity.
Colonoscopic perforations can present as overt or microperforations. Microperforation is similarly defined as benign pneumoperitoneum, asymptomatic free intra-abdominal air, or pneumoperitoneum without peritonitis after the procedure. 6 Typically, microperforations that are associated with colonoscopic polypectomy are not detected during the procedure itself but rather through postprocedural imaging. Characteristic radiolucency is observed below the diaphragm on chest radiography or in a superiorly dependent location on abdominal X-ray imaging after polypectomy. 7 The specific mechanism underlying the development of polypectomy-associated microperforation remains unclear. However, given the weaker muscle propria layer of the colonic wall, the main cause of microperforation may be a cautery injury sustained during the procedure. 8
Colonoscopic perforation resulting from therapeutic procedures is rare, 9 but it leads to serious adverse events with a high rate of morbidity and, in some cases, mortality.10 –12 Although early identification and prompt endoscopic closure of the suspected microperforation are important to prevent poor clinical outcomes, microperforation is difficult to detect during the polypectomy. Microperforation may occur following colon polypectomy. Nevertheless, the management of microperforation remains controversial,13,14 and the clinical outcomes for this adverse event are not well known.
This study aimed to analyze the clinicopathological characteristics, clinical outcomes, and risk factors of postpolypectomy microperforation. To the best of our knowledge, no previous study has evaluated the clinical outcomes and risk factors of postpolypectomy microperforation.
Materials and methods
Patients and methods
This study evaluated consecutive patients who developed microperforations after colonoscopic polypectomy between January 2008 and November 2013 at Gangnam Severance Hospital, Seoul, Korea. The medical records of patients who underwent colonoscopic polypectomy and subsequent plain X-ray examination to assess perforation were retrospectively reviewed. This study was performed in accordance with the principles stated in the Declaration of Helsinki and approved by the Institutional Review Board of the Gangnam Severance Hospital (3-2018-0232). This study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational studies. This study follows the STROBE guidelines for reporting observational studies. 15
The baseline patients for recruitment into the patient or control groups included those with larger polyps requiring inpatient monitoring after polypectomy or those who underwent abdominal X-rays due to postprocedural abdominal symptoms during the study period. All hospitalized patients underwent abdominal X-rays. Patients with pneumoperitoneum detected on plain radiography after colonoscopic polypectomy were enrolled in this study as the patient group. Patients with other polypectomy-induced adverse events, including immediate or delayed bleeding, postpolypectomy coagulation syndrome, or overt perforation detected by an endoscopist, were excluded. Additionally, patients with inflammatory or hereditary bowel diseases, those who did not undergo plain radiographic examination after polypectomy, and those who underwent colonoscopic procedures other than polypectomy were excluded. Cases with incomplete data or missing key variables necessary for analysis were also excluded. Patients who underwent colonoscopic polypectomy within 1 week of each case without adverse events were enrolled as potential controls. Controls were matched to cases by age (±2 years) and sex, using a 2:1 matching ratio.
Colonoscopic polypectomy
All polypectomies were performed by experienced staff or fellows who had performed more than 1000 cases of colonoscopic polypectomies. CF-Q260AI or CF-Q290AI (Olympus Optical, Tokyo, Japan) endoscopes were used. An ERBE ICC200 electrocautery device (ERBE Electromeidzin, Tubingen, Germany) was used for polypectomy. The cutting mode and total time of the current application were almost the same in each polypectomy (effect 1–2, output limit 50–60 W, 1 to 3 s). An epinephrine solution (a mixture of epinephrine diluted 1/10,000 in saline with Indigo Carmine) was injected submucosally for polypectomy.
Data collection
Data on polyps and polypectomy-related factors were collected retrospectively. When multiple polypectomies were performed, the data related to the largest polyps were used. Polyp characteristics included their number, location, size, gross type, and histology. Polyp location was categorized into right colon (cecum, ascending colon, and transverse colon) and left colon (descending colon, sigmoid colon, and rectum). The size and gross appearance of the polyps were determined based on colonoscopic images and medical records, using the diameter of the snare sheath as a reference. The gross appearance was classified according to the Japanese classification. 16 Histological diagnoses were made by pathologists using specimens according to the World Health Organization classification. 17 Polyps were categorized based on their most advanced pathological type. Visible muscle fiber was defined as exposure of muscle fiber at the polypectomy site, as detected on endoscopic image reviews (Figure 1).

Visible muscle fiber (red arrow) at the polypectomy site.
Data on clinical presentation, therapeutic assessment, and clinical outcomes were collected from each patient with a microperforation. Subjective symptoms included fever and abdominal symptoms, such as nausea, vomiting, and localized abdominal pain. Laboratory data included white blood cell count, neutrophil count, and C-reactive protein levels. Therapeutic data included the use of fasting, Levin tube insertion, and intravenous antibiotics. The total duration of antibiotic use was defined as the period of both oral and intravenous antibiotic use. Clinical outcomes included the duration of hospital stay and conversion to surgery.
Statistical analysis
Pearson’s chi-square test was used to analyze categorical variables. The Mann–Whitney U test was used to compare continuous variables, which are presented as mean ± standard deviation (SD). Univariate and multivariate regression analyses were performed to evaluate the risk factors associated with microperforation. For all comparisons, two-sided p-values of <0.05 were considered statistically significant. Statistical analyses were performed using SPSS software (version 18.0; SPSS, Chicago, IL, USA).
Results
Baseline characteristics and clinical outcomes of patients with postpolypectomy microperforation
Figure 2 shows the patient flowchart. During the study period, 1912 patients underwent a colonoscopic polypectomy. Among them, 12 (0.6%) were diagnosed with microperforation after polypectomy and were hospitalized for management. In all patients diagnosed with microperforation, abdominal-pelvic CT (APCT) was performed, and no bowel wall defects were detected in any of them (Figure 3). Preventive clipping of the polypectomy site was performed more frequently in the microperforation group compared to the control group (41.7% vs 20.8%, p = 0.247), but this difference was not statistically significant. No overt perforation was observed in any of the patients at the time of clipping. Table 1 shows the baseline characteristics and clinical outcomes of the patients with postpolypectomy microperforations. The patient population consisted of eight males and four females, with a mean age of 64.9 ± 8.7 years. Abdominal symptoms and fever were found in most and about one-third of patients with microperforations, respectively. Patients with microperforations show relatively high levels of inflammatory markers, including white blood cells, C-reactive protein, and neutrophils. Treatment was bowel rest for most and intravenous antibiotics for all patients. The mean duration of oral and intravenous antibiotic administration was 5 days. All patients with microperforations recovered completely without additional endoscopic or surgical intervention, and no mortality occurred. The median duration of hospitalization was 3 days (Table 1).
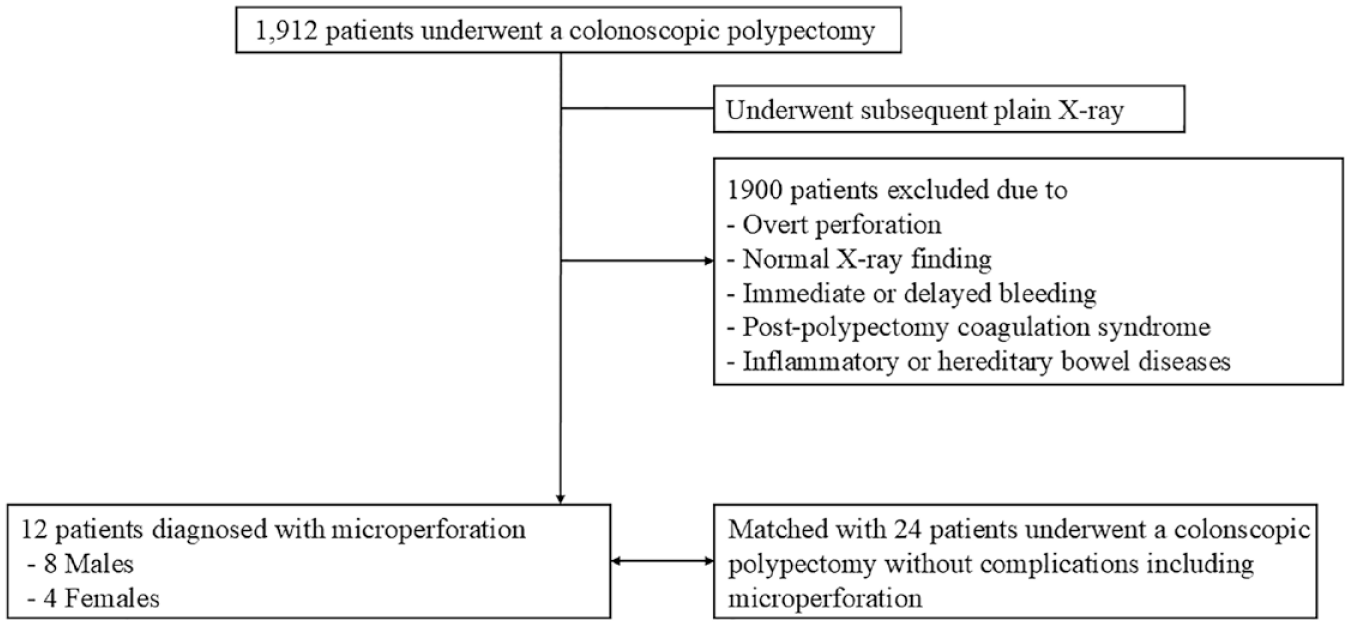
Patient flowchart.

Endoscopic and radiologic findings of two patients with microperforation after endoscopic polypectomy for colorectal polyps. (a) Prepolypectomy endoscopic view showing the polyp. (b) Postpolypectomy endoscopic view after removal of the polyp, with no clear evidence of perforation at the resection site. (c) Abdominal X-ray after polypectomy, showing the presence of free air below the diaphragm in the peritoneal cavity, indicative of microperforation. (d) Abdominal CT scan demonstrating intraperitoneal air shadows, with no wall defect of the colonic wall suggestive of perforation.
Clinical characteristics and outcomes of 12 patients with postpolypectomy microperforation.
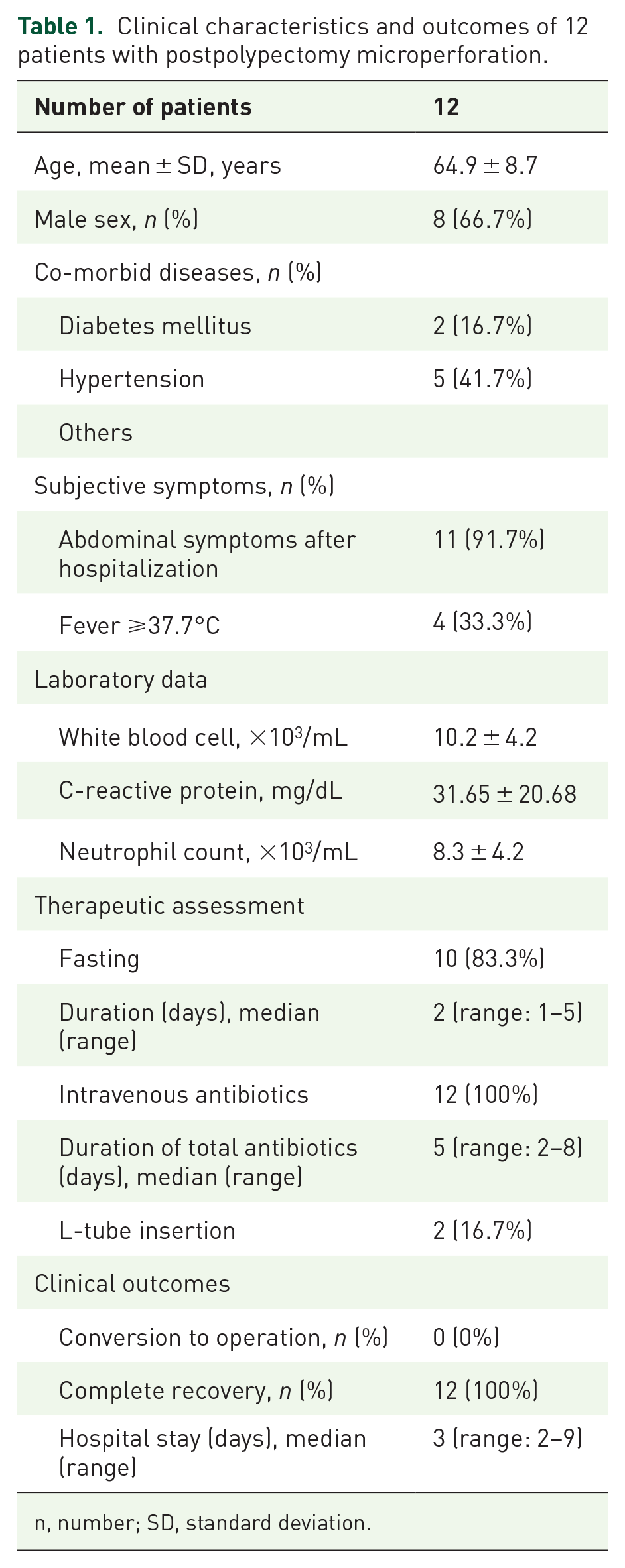
n, number; SD, standard deviation.
Endoscopic and histopathological features of patients with postpolypectomy microperforation
Table 2 shows the endoscopic and histopathological features of the polyps in patients with postpolypectomy microperforation. Two-thirds of patients required multiple polypectomies. Laterally spreading tumors (LST) were slightly more common than sessile polyps (Is), while mixed-type pedunculated polyps were found in one-quarter of patients. The mean size of the largest polyp was 15.7 ± 5.8 mm. Polyps were predominantly located in the right colon. Most polyps were pathologically diagnosed as adenomas with low-grade dysplasia (LGD), while others were adenomas with high-grade dysplasia (HGD), cancer, and nonneoplastic polyps.
Endoscopic and histopathologic data of the 12 patients with postpolypectomy microperforation.
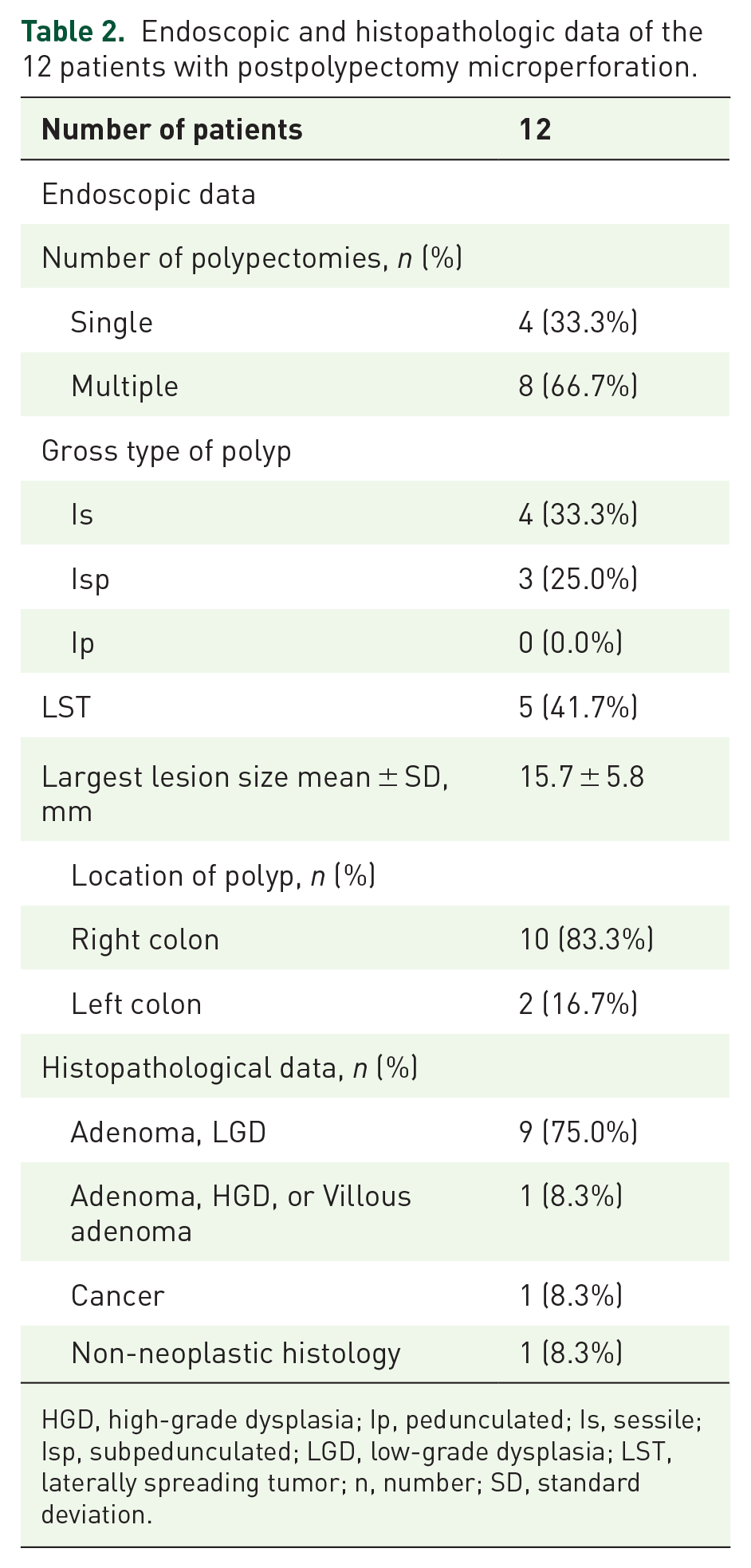
HGD, high-grade dysplasia; Ip, pedunculated; Is, sessile; Isp, subpedunculated; LGD, low-grade dysplasia; LST, laterally spreading tumor; n, number; SD, standard deviation.
Comparison of characteristics between patients with and without postpolypectomy microperforation
Table 3 shows a comparison of various variables in patients with and without postpolypectomy microperforations. Polyp location, resection method, and presence of visible muscle fibers differed significantly between patients with and without microperforations. Patients with microperforations had a significantly higher frequency of right colon-located polyps (p = 0.005). Compared with conventional endoscopic mucosal resection (EMR), EMR with precutting (EMR-P) and hot-snare polypectomy were performed more frequently in patients with than in those without microperforations (p = 0.038). Visible muscle fibers at the polypectomy site were more frequently identified in patients with microperforations (p = 0.001). In addition, LST tended to be more common in patients with microperforations than in patients without microperforations (p = 0.052).
Comparison of clinicopathologic characteristics between patients with and without microperforation.
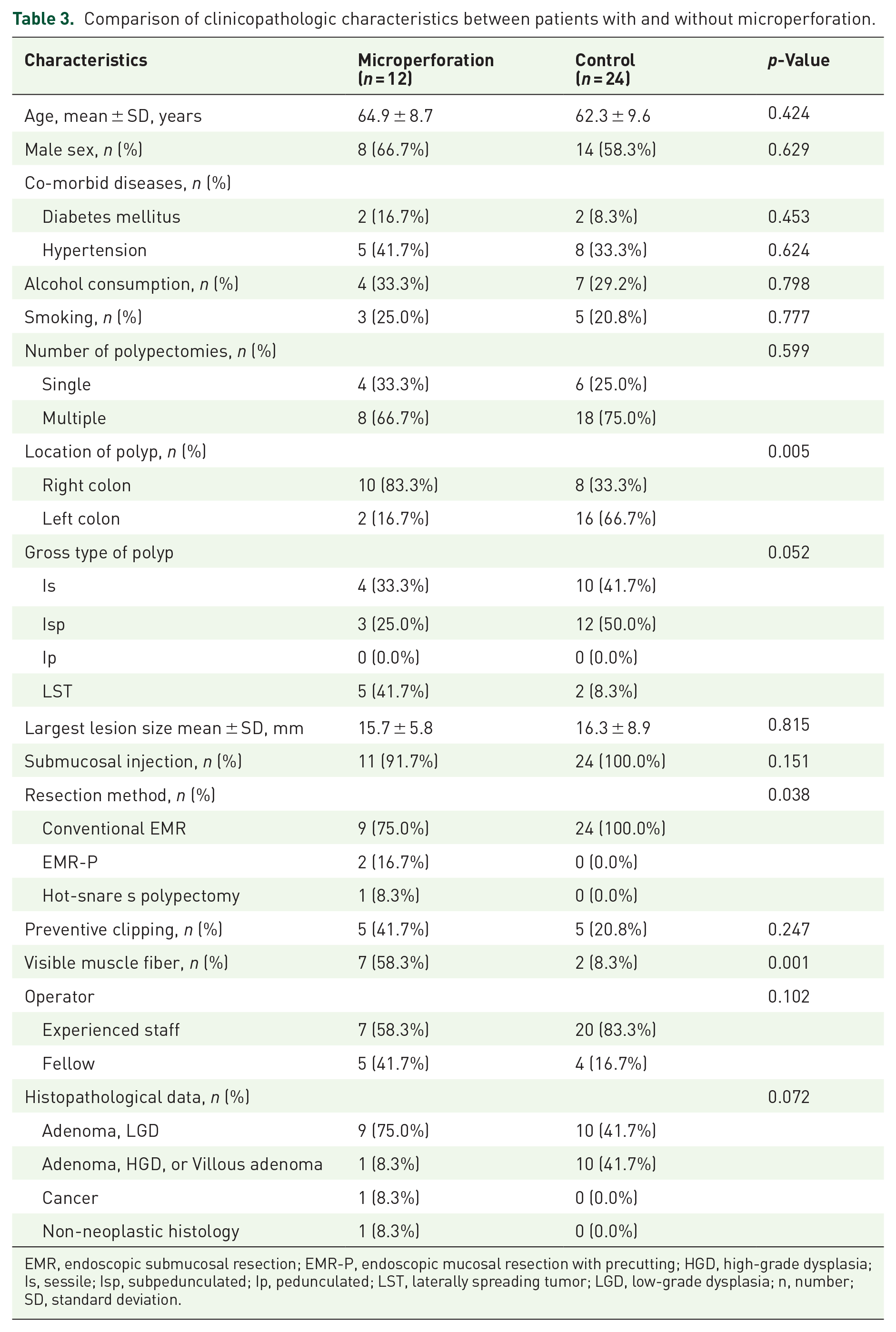
EMR, endoscopic submucosal resection; EMR-P, endoscopic mucosal resection with precutting; HGD, high-grade dysplasia; Is, sessile; Isp, subpedunculated; Ip, pedunculated; LST, laterally spreading tumor; LGD, low-grade dysplasia; n, number; SD, standard deviation.
Multivariate analysis for risk factors of postpolypectomy microperforation
For multivariate analysis, the cutoff value for the largest lesion polyp size was set at 14 mm, which was associated with the largest area under the receiver operating characteristic curve. The gross type of the polyps was categorized into LST and other polypoid lesions (Is, pedunculated, and sub-pedunculated). The results showed that the location of the right colon (odds ratio (OR) 16.891, 95% confidence interval (CI) 1.1330–214.429) and visible muscle fiber (OR 13.850, 95% CI 1.045–183.632) were independent factors associated with postpolypectomy microperforation. Size, gross type, histopathology, preventive clipping, and resection methods were not significantly associated with postpolypectomy microperforations (Table 4).
Risk factors of postpolypectomy microperforation in multivariate analysis.

EMR, endoscopic mucosal resection; EMR-P, endoscopic mucosal resection with precutting; LST, laterally spreading tumor.
Discussion
In this study, we examined the clinical outcomes and risk factors for postpolypectomy microperforation. Most patients with these microperforations had localized abdominal pain and showed elevated inflammatory markers on laboratory examination. However, all patients recovered after conservative management, including fasting and intravenous antibiotics, without the need for surgical intervention. Their median hospital stay was relatively short (3 days; range: 2–9 days). The right-sided location and visible muscle fibers at the polypectomy site were independent risk factors for postpolypectomy microperforation.
Colonoscopy and polypectomy are relatively safe procedures with a low incidence of severe adverse events. 18 Colonic perforation occurring during diagnostic colonoscopy has various causes and a reported incidence of <0.1%.19 –21 However, the incidence can increase by up to 5% with colonoscopic interventions. 9 Nevertheless, the incidence of microperforations has rarely been reported. One retrospective study reported it to be 0.3% (1/274), 22 and no cases of pneumoperitoneum were detected on postprocedure upright abdominal and chest radiographs in a previous pilot study of 100 patients. 6 We here examined a larger number of subjects than previous studies and demonstrated that the incidence of postpolypectomy perforation was approximately 0.6% (12/1912).
The management of colonic perforation may include conservative, endoscopic, and surgical approaches. The therapeutic strategy varies according to the clinical setting and includes factors such as the timing of perforation diagnosis (intra- or postcolonoscopy), perforation characteristics (size, location, and etiology), the patient’s general condition, and the skill level of the operator.23,24 Prompt surgical intervention is not usually recommended in patients with subdiaphragmatic free air and no signs of peritoneal irritation or abdominal sepsis.25,26 Concomitant administration of intravenous fluids, broad-spectrum antibiotics, and close monitoring of vital signs are recommended to prevent clinical deterioration when colonic perforation is suspected. 27 However, in clinical settings, microperforation occasionally progresses to overt perforation,perforation 28 which may cause physicians to hesitate to continue conservative therapy and raise concerns about whether patients should be referred for surgical intervention. In our study, none of the patients with postpolypectomy microperforations underwent surgery, and they recovered completely over a relatively short period through conservative treatment, such as bowel rest and intravenous antibiotics. This finding suggests that conservative treatment is feasible and could be the primary management option for selected patients with microperforations after colonoscopic polypectomy. Although the duration of antibiotic therapy for colonic perforation or intra-abdominal infection has not been established, antibiotic therapy was likely shortened in those patients who demonstrated a favorable response to treatment. 29 Sawyer et al. reported that, in patients with intraabdominal infections who had undergone an adequate source-control procedure, the outcomes after fixed-duration antibiotic therapy (approximately 4 days) were similar to those after a longer course of antibiotics that extended until after the resolution of physiological abnormalities (approximately 8 days). 30 In line with these observations, the median duration of total antibiotic therapy in our study was 5 days, suggesting that long-term antibiotic therapy may not be required for the management of postpolypectomy microperforation.
Early diagnosis of colonic perforation has been found to influence outcomes after perforation substantially. 31 At a later stage, colonic perforation is associated with more severe symptoms or signs, including a systemic inflammatory response, hypotension, and mental confusion. More invasive treatments, such as surgery, are required when the diagnosis is delayed by more than 24 h.32,33 A previous study showed that 66.7% (6/9) of patients who required surgery for colonic perforation had been diagnosed after more than 24 h. 33 Early suspicion of iatrogenic perforation should be prompted by unusual abdominal pain with distension, chest pain, subcutaneous emphysema, or shortness of breath. 27 However, in contrast to overt colonic perforations, microperforations are more difficult to recognize during colonoscopy, and the patients’ complaints are usually vague and nonspecific in the early stages. Therefore, identifying the risk factors for microperforation in high-risk groups is important for early recognition and prevention of these adverse events. This study demonstrated that polyps in the right colon and visible muscle fibers at the polypectomy site were more frequent in the microperforation group than in the control group. Similar to our results, a right-sided colonic location was reported as a significant risk factor for colonoscopy-related adverse events in several previous studies. In a prospective multicenter study performed in Germany, major adverse events, including bleeding and bowel perforation, were significantly more frequent when the polyp was located in the right colon. 34 Additionally, a study on endoscopic submucosal dissection (ESD) reported that postpolypectomy coagulation syndrome was more common in the right-sided colon, further supporting the increased vulnerability of this region. 35 The right hemicolon location also appears to be an independent and substantial risk factor for delayed postpolypectomy bleeding. 36 Although the reason for this finding is currently unclear, several studies have suggested that the thinner wall of the right colon, combined with the high air pressure trapped in the luminal area, makes the right colon more vulnerable to adverse events.37,38 Fresh ileal fluids containing digestive enzymes and bile acid, which can dissolve clots and other protective products, have also been suggested as the cause of adverse events in the right colon. 36 Results from animal experiments have suggested that specific power settings and electrocautery duration are associated with microperforation, 8 while even the same electrocautery current may be more prone to causing damage when applied in the right colon than in the left.
This study also revealed that visible muscle fibers at the polypectomy site, as shown in Figure 1, were an independent risk factor for microperforation; this has not been reported previously. Unintentional muscle tears caused by ESD knives are a common mechanism of colonic ESD-related perforation, and a long duration of electrocauterization during colonic ESD is also considered a risk factor for delayed perforation due to coagulation injury. 39 The visibility of muscle fibers indicates that the polyp was resected closer to the muscle layer than is typical, suggesting the application of excessive electrocautery to the colon wall. This implies that applying excessive electrocautery closer to the muscle layer may induce microperforations. Considering the increased risk of microperforation when the muscular layer is exposed, if visible muscle fibers are observed at the resection site after colon polypectomy, procedures, such as prophylactic clip ligation, can be considered to reduce the potential risk of perforation. Notably, while electrocautery is also associated with postpolypectomy coagulation syndrome, our study specifically focused on microperforation. Microperforation is distinct from postpolypectomy coagulation syndrome, which involves localized inflammation and thermal injury to the bowel wall, causing symptoms such as abdominal pain and fever, but without pneumoperitoneum on imaging. Patients diagnosed with postpolypectomy coagulation syndrome were excluded from this study.
Although the resection method was not an independent risk factor for postpolypectomy microperforation in multivariate analysis, EMR-P and hot-snare polypectomy were significantly associated with microperforation in univariate analyses. EMR-P is a modified EMR technique in which a circumferential incision is made using a snaring tip or ESD knife. In previous studies, the frequency of perforation during endoscopic resection for colorectal LSTs was reported to be significantly higher in the EMR-P groups than in the conventional EMR groups during endoscopic resection for colorectal LST. 40 This result suggests that the risk of perforation may increase during precutting in EMR-P. Similarly, in our study, microperforations may have occurred because of minor damage to the muscular layer during circumferential incision using EMR-P. In hot-snare polypectomy procedures, the lack of a fluid cushion at the base contributes to the occurrence of microperforations.
In accordance with these findings, it has been proposed that a fluid cushion should be placed beneath colonic polyps to enhance the separation of the mucosal layer, thereby diminishing the risk of perforation following polypectomy. 41 A lack of experience is considered to be a major risk factor for perforation during the procedure. Multiple studies have observed that the rates of adverse events in general and of perforations in particular decrease with increasing experience, as well as with the improvement of devices and techniques.42,43 However, in this study, the rate of microperforation did not differ significantly between the experienced and fellow staff. These findings suggest that procedural experience is not associated with the risk of microperforation, and the cause remains unclear. Nevertheless, both experienced staff and fellows must be cautious of the occurrence of microperforations.
Our study had some limitations. First, this was a retrospective single-center study, and the number of cases of microperforations was small due to the low microperforation rate. First, it was a retrospective, single-center study with a small number of microperforation cases due to the low incidence of this complication. Given the retrospective nature of the study and the relatively low occurrence of postpolypectomy microperforations, a formal power analysis or sample size calculation was not conducted prior to data collection. Additionally, while the control group was matched by age and sex, we were unable to consistently collect data on other polyp characteristics, such as submucosal fibrosis and narrow-band imaging classification, due to the retrospective nature of the study. Second, only inpatient data from one university hospital were analyzed. A prospective study, including both inpatient and outpatient settings, should be conducted in the future. Third, although plain X-ray was used as the initial imaging modality, it may not detect smaller amounts of free air. However, all patients with free air detected on plain X-ray underwent APCT for confirmation. Additionally, all cases were reviewed by experienced staff to minimize the possibility of undetected perforation. Despite these limitations, to the best of our knowledge, this is the first study to analyze the predictive factors for postpolypectomy microperforation during colon polypectomy. Finally, the polypectomy method was not standardized, and the polypectomy approach varied according to each endoscopist’s preference, which might have introduced bias. Despite these limitations, this study provides valuable insights into the management of postpolypectomy microperforation.
Conclusion
Conservative management, including bowel rest and antibiotics, is a feasible and effective primary treatment option for selected patients experiencing microperforation after colonoscopic polypectomy. This study identified right-sided colonic polyps and visible muscle fibers at the polypectomy site as significant risk factors for postpolypectomy microperforation. Special caution is advised during procedures involving these risk factors to mitigate the likelihood of microperforation complications.