
Abstract
Numerous factors can contribute to a difficult colonoscopy, potentially leading to an incomplete procedure and overlooked lesions. Alternative strategies for handling difficult and incomplete colonoscopies should be considered. We present the case of an 85-year-old male who underwent a difficult colonoscopy, during which two expert endoscopists spent 1.5 h attempting various techniques but failed to intubate the cecum. Subsequently, colonic transendoscopic enteral tubing (TET) was performed. Abdominal plain film revealed tortuosity of the TET tube in the left abdomen corresponding to the distribution of the descending colon. Retrograde colon imaging was conducted by injecting a mixture of contrast medium and air into the colon via the TET tube. X-ray demonstrated well-developed visualization of the entire colon and terminal ileum. And evident elongation and tortuosity of the descending colon resembled an N-type folding pattern. The final diagnosis was determined as descending colon redundancy. Colonic TET combined with retrograde colon imaging through the TET tube may serve as an effective supplementary approach for identifying causes of difficult colonoscopy and improving diagnostic accuracy for bowel diseases when complete visualization is not achieved.
Keywords
Introduction
Colonoscopy is a crucial diagnostic tool for colorectal diseases. In comparison to gastroscopy, the procedure of colonoscopy presents greater challenges. Numerous factors have been documented as being associated with difficulties encountered during colonoscopy, including inadequate bowel preparation, severe diverticulosis, redundant colon, looping, adhesions, young and female patients, patient discomfort, and the expertise of the endoscopist. 1 Difficult colonoscopy may frequently occur in clinical practice. In such circumstances, an incomplete colonoscopy procedure may ensue, leading to potential missed diagnoses of colonic diseases. 2 Therefore, alternative approaches to difficult and incomplete colonoscopies must be considered.
Colonic transendoscopic enteral tubing (TET), a novel colon-specific drug delivery method for multiple fecal microbiota transplantations or frequent colonic medication administration, is a technique in which a specially designed tube is inserted through the colonic biopsy channel and maintained in the colon. 3 In addition to the fecal microbiotic solution that can be injected into the colon through the colonic TET tube, other liquids such as contrast agents can also be injected into the colon through the tube, which may help to achieve retrograde imaging of the colon.
In this study, we attempted to perform colonic TET for a challenging colonoscopy case in which two experienced endoscopists were unable to intubate the cecum. Subsequently, retrograde colon imaging was conducted through the TET tube, revealing a well-developed colon and ultimately aiding in identifying the cause of the difficult colonoscopy.
Case presentation
An 85-year-old male was admitted with complaints of chronic constipation. He had a history of femoral head replacement surgery but denied any abdominal surgeries. His BMI was recorded as 16.6 kg/m2. To investigate the cause of his constipation, a colonoscopy was scheduled for him. Prior to the procedure, he underwent bowel preparation using 1 L of PEG-4000 fluid on the day before and an additional 2 L 6 h prior to the colonoscopy. Adequate bowel preparation was confirmed when he passed clear and watery stool.
The sedated colonoscopy was performed by an expert endoscopist with over 8 years of experience in endoscopy. A pronounced angulation was observed in the colonic lumen approximately 45 cm from the anus, posing significant challenges for further insertion of the colonoscope. Despite several attempts, the operator reluctantly managed to navigate past the angulation, however, encountered difficulties again due to loop formation within the abdomen during deeper intubation. Another highly experienced endoscopist took over but faced similar obstacles despite employing techniques such as abdominal pressure, body repositioning, adding a transparent cap, and immersing the colonic lumen with water. The procedure lasted approximately 1.5 h for both endoscopists involved. Due to repeated friction and traction caused by colonoscopy, localized mucosal bleeding occurred in the intestine. Concerns regarding complications associated with colonoscopy and anesthesia led to discontinuation of routine colonoscopy.
After obtaining consent from the patient’s family, colonic TET was performed. A TET tube (FMT-DT-F-27/1350; FMT Medical, Nanjing, China) was inserted into the intestinal lumen through the biopsy channel of the colonoscopy under direct endoscopic visualization. The distal end of the tube was advanced through the colonic angulation approximately 45 cm from the anus (Figure 1). The colonoscope was then withdrawn while leaving the TET tube in place within the colon. Subsequently, second colonoscopy intubation was performed arriving at the target angulation. The second loop of the TET tube was secured to the colonic mucosa near the colonic angulation using an endoclip (ROCC-D-26-230-C, Micro-Tech, Nanjing, China) (Figure 2). The structure of the TET tube is depicted in Figure 3.
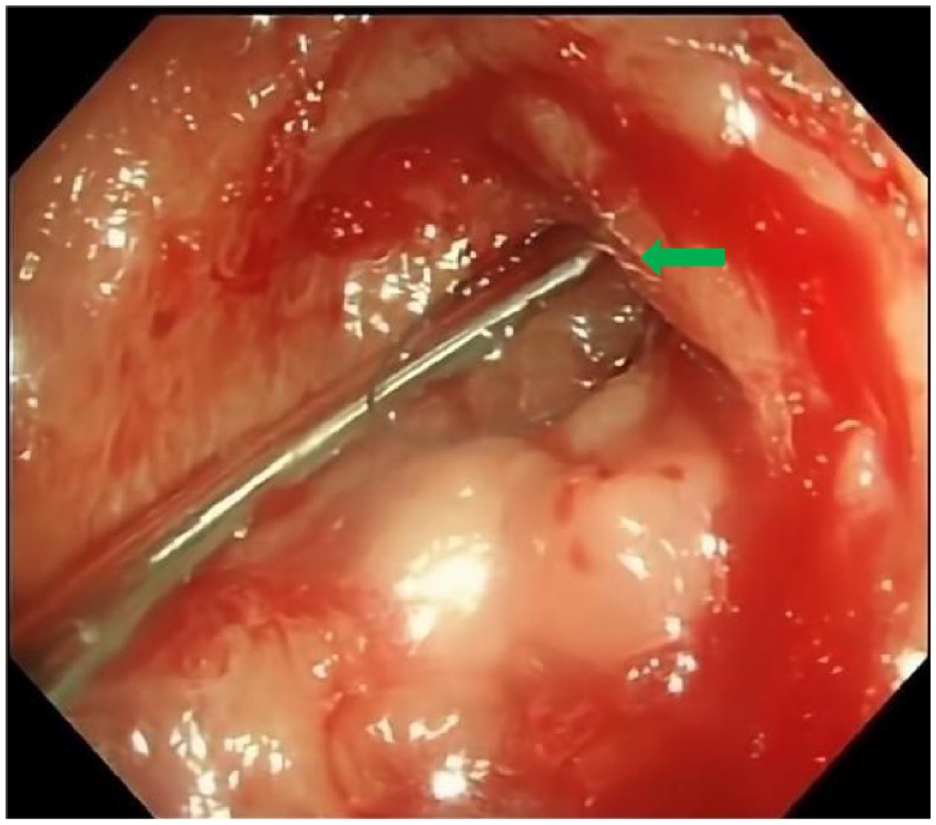
Blood seeped because of long-time friction and attraction by the colonoscope. The tip of the TET tube was inserted passing through the colonic angulation (green arrow).

An endoclip (green arrow) was utilized to secure the second loop (blue arrow) of the TET tube to the colonic mucosa near the angulation.

The structure of the colonic TET tube consists of two parts. The main part of the tube is indicated by the red arrow, measuring 1350 mm in length with a diameter of 2.7 mm, and featuring three loops at its terminal end (green arrow), which can be fixed to the colonic mucosa using endoclips. The temporarily connected extended part of the tube is shown by blue arrow, providing convenience for exchange.
Abdominal plain film revealed tortuosity of the TET tube in the left abdomen corresponding to the distribution of descending colon. The visualized endoclip in the film indicated the location of sharp flexure impeding passage during colonoscopy evaluation (Figure 4). Furthermore, retrograde colon imaging was performed by injecting a mixture consisting of 600 mL normal saline, 200 mL iohexol, and 100 mL air via the colonic TET tube. X-ray imaging demonstrated well-developed entire colon and terminal ileum without evidence of mass lesions, stenosis, or ulcers. Descending colon exhibited obvious tortuosity and elongation resembling an N-type folding pattern (Figures 5 and 6).
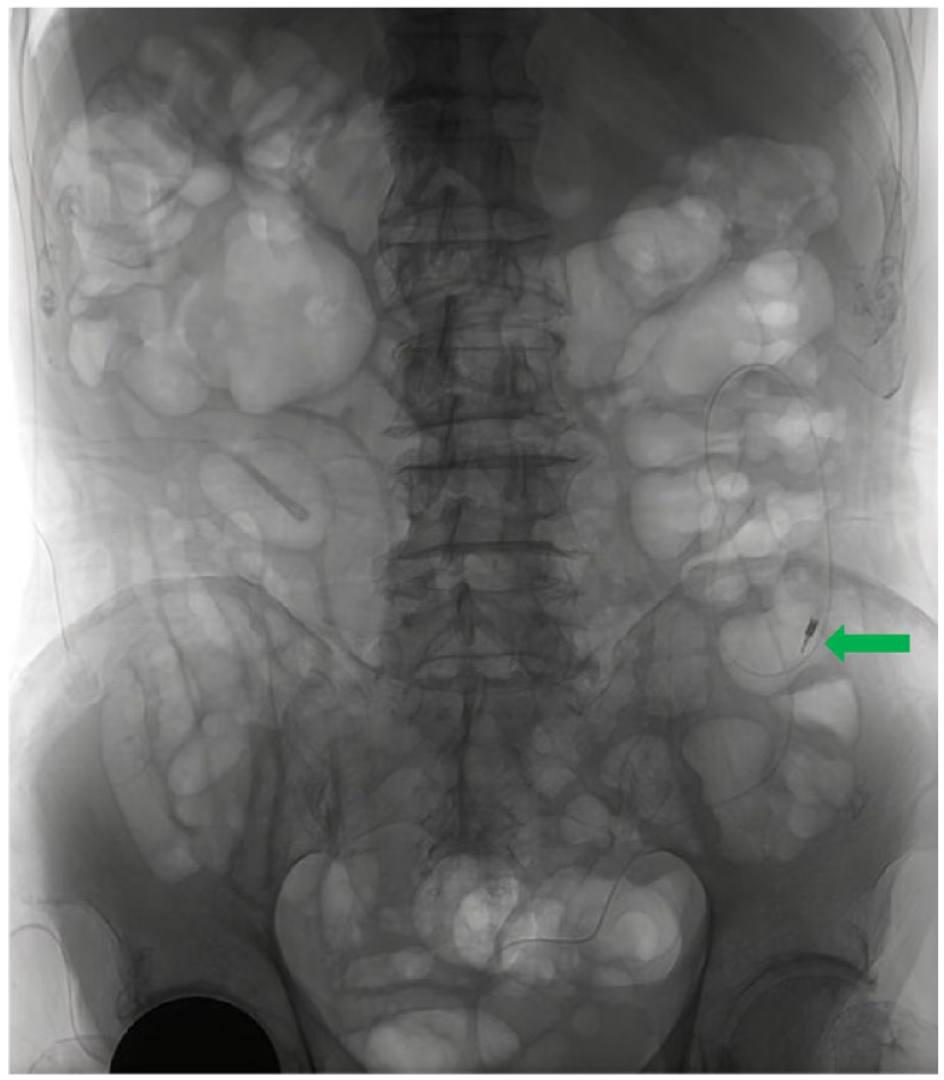
X-ray imaging revealed tortuosity of the TET tube in left abdomen region. The location where an endoclip was placed indicates a sharp flexure where colonoscopy could not pass through (green arrow).
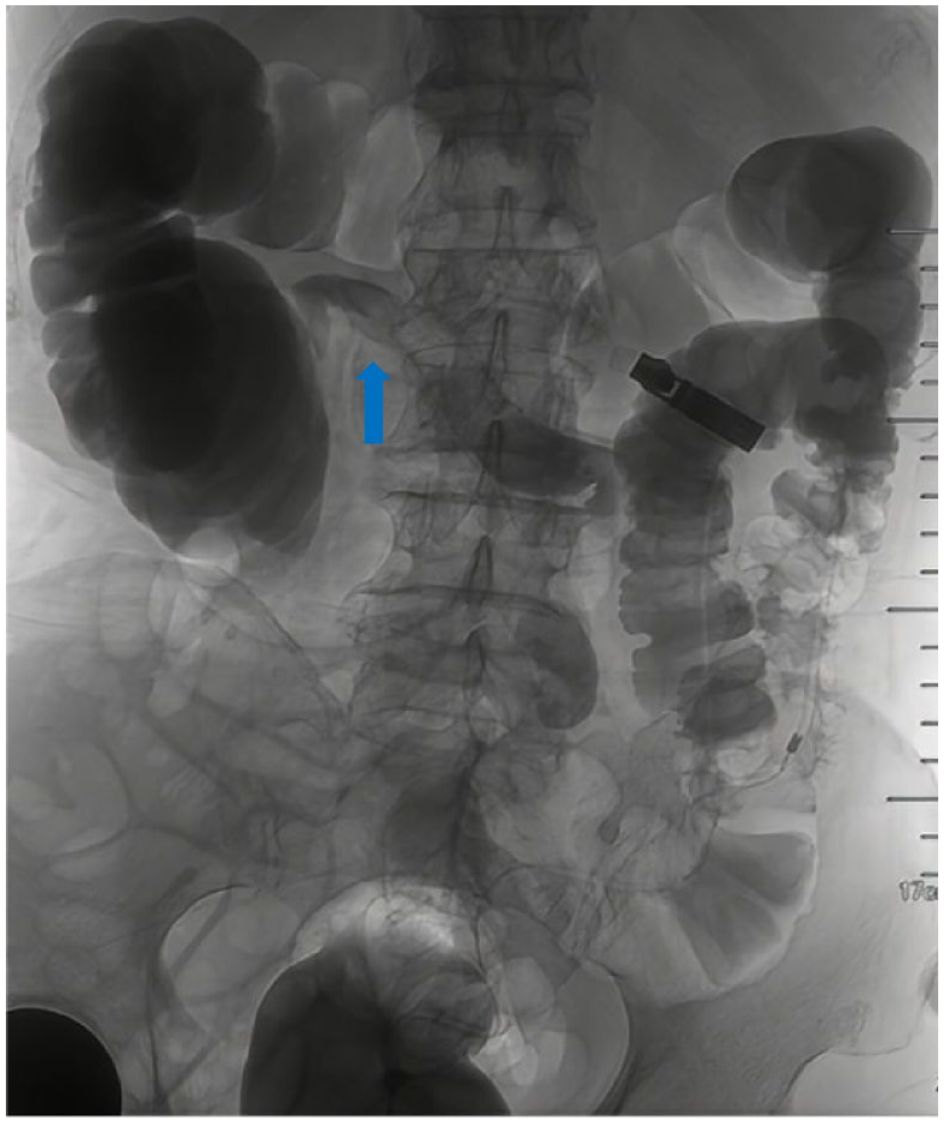
Retrograde colon imaging via the colonic TET tube demonstrated well-developed entire colon and terminal ileum (blue arrow).

The descending colon exhibited obvious tortuosity and elongation, resembling an N-type fold.
Based on retrograde colon imaging findings, final diagnosis for this patient is descending colon redundancy which may be associated with constipation symptoms and difficulty encountered during previous attempted colonoscopy.
Four hours after retrograde colon imaging, the colonic TET tube was removed. The patient complained of no particular discomfort. Oral medications for constipation were given to him.
The reporting of this study conforms to the CARE checklist (Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D; the CARE Group. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Development).
Discussion
A successful cecal intubation, defined as the insertion of the colonoscope to the terminal ileum proximal to the ileocecal valve and/or the cecum, 4 is essential for a thorough and complete colonoscopy. It is important to avoid incomplete colonoscopies as they may result in missed lesions. 2 The most commonly used indicators for assessing competency in colonoscopy are cecal intubation time (CIT) and cecal intubation rate (CIR).5,6 Difficult colonoscopy is typically characterized by a CIT exceeding 10 min or an incomplete examination using a standard scope. 7
According to recommendations from the American Society for Gastrointestinal Endoscopy, competent endoscopists should achieve a CIR >95% for screening healthy adults and >90% for all cases. 8 However, it has been estimated that up to 10%–20% of real-world colonoscopies may encounter difficulties with cecal intubation. 9 A recent study involving 1281 unsedated colonoscopies reported a proportion of difficult cecal intubations at 27.2%. 10 In cases where difficult colonoscopy is anticipated, CIR ranged from 90% to 96%, while CIT varied between 21.00 and 23.42 min. 11 Increasing CIR and reducing CIT remain crucial objectives for difficult colonoscopy.
Predicting the difficulty level of an upcoming examination before performing a colonoscopy can be challenging. However, several factors have been identified that might influence its difficulties, including age, gender, BMI, bowel preparation status, prior abdominal or pelvic surgery history, bowel anatomy variations, and endoscopist experience.10,12 Among these factors, the impact of bowel anatomy on difficulty levels during both pre-examination prediction and actual performance remains uncertain due to colonoscopy limitations in observing bowel distribution or redundancy compared with visualizing lesions within the bowel lumen.
Colonic TET is an interventional therapeutic procedure for the intestine. 13 Since 2015, it has been demonstrated that colonic TET is a novel, safe, and convenient technique for transplanting washed fecal microbiota and administering medication into the colon.14,15 Recent studies have shown that colonic TET can be used to rescue endoscopy-related perforations and manage intestinal obstruction by draining colonic air and fluid through the TET tube.16,17 Based on its two-way fluid exchange function, the colonic TET tube may be attempted to inject contrast agents for retrograde colon imaging. The TET Study Group in China in 2023 published the experts’ recommendation that retrograde administration of contrast agent via the colonic TET tube may improve clinical diagnosis by imaging stenosis, ulceration, masses, and fistulas using fluoroscopy or computed tomography (CT), compensating for deficiencies in diagnostic efficiency compared to CT scans with or without contrast. 13 As we know, colonic TET has never been used for patients with difficult colonoscopy previously.
For this difficult colonoscopy case, a variety of methods were attempted to aid insertion including changing experts, applying abdominal pressure, adjusting body position, adding a transparent cap, and water immersion. However, further advancement was hindered due to constant flexure formation and looping. During colonoscopy it was unclear what caused these difficulties, perhaps there was excessive angulation within the bowel lumen or localized luminal strictures. To determine the cause of difficulty during colonoscopy as well as any potential lesions in proximal lumen areas, the colonic TET tube placement followed by retrograde colon imaging was performed.
The abdominal plain film clearly showed the bent shape of the radiopaque material comprising the colonic TET tube which corresponded with distribution of the descending colon. The endoclip was visualized on the plain film, indicating the site of colonic flexure beyond which colonoscopy could not proceed. Retrograde colon imaging via the colonic TET tube provided excellent visualization of the entire colon and terminal ileum, facilitating exclusion of colorectal cancer and other lesions in this patient. The overall distribution pattern of the colon was also clearly demonstrated, particularly with a distinct N-shaped appearance observed in the descending colon. Therefore, based on findings obtained using the colonic TET tube, a diagnosis of descending colon redundancy was established as the underlying cause for difficult passage during colonoscopy.
Conclusion
The utilization of colonic TET and retrograde colon imaging through this technique may serve as an effective approach to identify causes contributing to difficult colonoscopies and enhance diagnostic accuracy for bowel diseases when a complete examination of the entire colon is unattainable. However, it should be noted that this is only a case report, and further studies with larger sample sizes are required to confirm the effectiveness of colonic TET in difficult colonoscopy.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745241270568 – Supplemental material for Retrograde colon imaging through colonic transendoscopic enteral tubing helps to confirm the cause of difficult colonoscopy: a case report
Supplemental material, sj-docx-1-cmg-10.1177_26317745241270568 for Retrograde colon imaging through colonic transendoscopic enteral tubing helps to confirm the cause of difficult colonoscopy: a case report by Xiaomeng Jiang, Runqing Wang, Haibo Sun and Faming Zhang in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.