
Abstract
Weight recurrence after one-anastomosis gastric bypass (OAGB), the third most common metabolic and bariatric surgery performed worldwide, is observed in a subset of patients due to the chronic, progressive nature of obesity. Endoscopic revision of the OAGB (ER-OAGB) through full-thickness suturing to reduce the gastrojejunal anastomosis and gastric pouch is a potential alternative to surgical revision. Here, we present a case series of ER-OAGB and long-term nutritional support at two international centers with expertise in bariatric endoscopy. Data were retrospectively evaluated from a prospectively maintained database. The primary outcome was total body weight loss (TBWL) at 12 months. Secondary outcomes included TBWL at 3, 6, and 15 months; excess weight loss (EWL) at 3, 6, 12, and 15 months; frequency of new/worsening symptoms of gastroesophageal reflux disease (GERD); and the frequency of serious adverse events. In this series, 17 adults (70.6% female, mean age 46.8 years, mean BMI 39.1 kg/m2) successfully underwent ER-OAGB an average of 8 years (range 2–21 years) after OAGB for a mean weight recurrence of 43.2% (range 10.9–86.9%). TBWL from ER-OAGB was 9.7 ± 1.8% at 3 months, 13.4 ± 3.5% at 6 months, 18.5 ± 2.1% at 12 months, and 18.1 ± 2.2% at 15 months. EWL from ER-OAGB was 30.5 ± 14.7% at 3 months, 42.6 ± 16.2% at 6 months, 54.2 ± 11.3% at 12 months, and 54.2 ± 11.7% at 15 months. There were no instances of new/worsening GERD symptoms or serious adverse events. In this small series of adults who experienced weight recurrence after OAGB, ER-OAGB facilitated safe and clinically meaningful weight loss, without new or worsening GERD symptoms, when performed by experienced bariatric endoscopists in concert with longitudinal nutritional support.
Plain Language Summary
The one-anastomosis gastric bypass (OAGB) is now the third most commonly performed metabolic and bariatric surgery worldwide. As with other weight loss surgeries, the OAGB is associated with weight recurrence over time that prompts patients to seek further treatment; however, revisional surgeries are known to carry increased risk. The endoscopic revision of the OAGB (ER-OAGB) is an incisionless technique that reduces the gastrojejunal anastomosis and gastric pouch to facilitate weight loss after weight recurrence in OAGB. Here, we showed in a series of 17 adults that the ER-OAGB safely helped patients lose over 18% of their body weight within the year following their revision.
Introduction
Developed by Dr. Robert Rutledge in 1997 as a primary metabolic and bariatric surgery, the one-anastomosis gastric bypass (OAGB), formerly called the ‘mini gastric bypass’, involves the creation of a long, sleeve-like gastric pouch that is connected via a wide, 4–5 cm anastomosis to the uninterrupted jejunum approximately 150–200 cm distal to the ligament of Treitz.1–3 Compared to the Roux-en-Y gastric bypass (RYGB), the OAGB is faster, less technically challenging, and facilitates easier postoperative evaluation of both jejunal limbs.4–6 The OAGB has become the third most common bariatric surgery performed worldwide, and in May 2022, the American Society for Metabolic and Bariatric Surgery officially endorsed the surgery. 7 With this endorsement and the rising rate of global obesity, implementation of OAGB is anticipated to increase within the United States and worldwide.
As obesity is a chronic, progressive, relapsing disorder, weight recurrence following metabolic and bariatric surgery is common and expected. 8 Meta-analyses suggest that at least 7% of post-OAGB patients undergo surgical revision for insufficient weight loss response, 6 and weight recurrence comprises approximately 11–34% of cases undergoing revisional surgery after OAGB.9–12 Nevertheless, these interventions – which include conversion to RYGB or biliopancreatic limb elongation – carry heightened risk compared to the original surgery,6,9 in keeping with revisions of other metabolic and bariatric surgeries.13,14 As risk aversion is a formidable barrier for patients seeking surgical forms of weight loss, there is a growing need for safe, minimally invasive tools to address postsurgical weight recurrence as OAGB rates increase in the United States,15,16
Transoral outlet reduction (TORe) using the Overstitch endoscopic suturing system (Apollo Endosurgery, Austin, TX, USA) is FDA-authorized to treat weight recurrence after RYGB in adults with a BMI between 30 and 50 kg/m2. TORe involves full-thickness suturing of the gastrojejunal anastomosis (GJA), which is often dilated in patients with weight recurrence, to provide further restriction of the gastric outlet to promote satiety.17,18 Accordingly, reduction of the GJA in OAGB is a potential target to promote weight loss. A second endoscopic target for weight recurrence after OAGB is full-thickness suturing of the long sleeve-like gastric pouch, as has been successfully performed for weight recurrence following vertical sleeve gastrectomy19,20 and which comports with weight loss success from surgical resizing of a dilated gastric pouch after OAGB. 21
GJA and gastric pouch reduction may allow endoscopic revision of OAGB (ER-OAGB) (Figure 1) to halt and reverse weight recurrence and its associated detrimental metabolic, psychosocial, and economic effects.22–24 To date, ER-OAGB for weight recurrence has not been described in the literature. Further, there are OAGB-specific concerns that restriction of the GJA and/or pouch may be detrimental to pouch clearance and thus promote debilitating symptoms of gastroesophageal reflux from either biliary or gastric acid origin.2,12,25–28 To address these knowledge gaps, we present a case series of 17 adult patients who underwent ER-OAGB at two centers with expertise in bariatric endoscopy to highlight the clinical efficacy and safety of this novel approach in the outpatient setting.
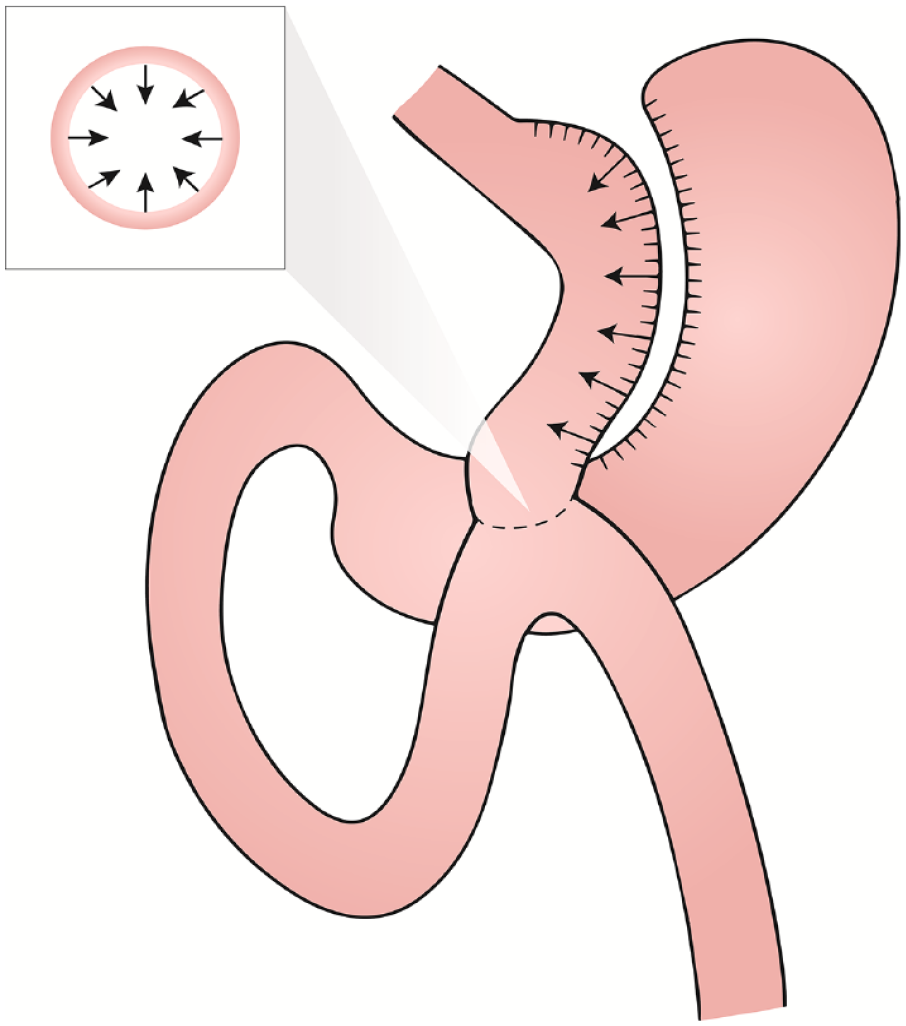
Endoscopic revision of the one-anastomosis gastric bypass (ER-OAGB). As indicated by the arrows, the components of ER-OAGB include circumferential narrowing of the gastrojejunal anastomosis (inset) and reduction of the sleeve-like gastric pouch, both through full-thickness endoscopic suturing.
Methods
Data were retrospectively analyzed from two prospectively maintained center-specific databases of patients who underwent ER-OAGB for the primary indication of weight recurrence. The study was granted an Institutional Review Board exemption (WCG IRB, Puyallup, WA, USA). The reporting of this study conforms to the Case Report (CARE) Guidelines. 29
All procedures were performed under general anesthesia on an outpatient basis by one of two experienced bariatric endoscopists (AH, CM) using a dual-channel therapeutic endoscope (FUJIFILM Medical Systems, Lexington, MA, USA) and the Overstitch endoscopic suturing system (Apollo Endosurgery, Inc., Austin, Texas, USA). Six ER-OAGB cases were performed by CM and 11 by AH at their respective institutions. Prior to ER-OAGB, an endoscopic evaluation with a single-channel gastroscope was performed to assess the gastric pouch and the GJA for size, health, and presence of pathology (including stoma and pouch dilation). Pouch length was measured via standard scope markings, and GJA diameter was estimated visually relative to the endoscope and/or endoscopic tools, as is standard practice in TORe.30,31 If present, visible surgical material was removed from the GJA with forceps and/or endoscopic scissors. If no contraindications to ER-OAGB were identified, gastric tissue surrounding the GJA was circumferentially ablated using argon plasma coagulation (80 W, 1.2 L/min) for a golden-brown effect approximately 5–10 mm in width. A dual-channel therapeutic gastroscope equipped with Overstitch endoscopic suturing system was then used to perform a purse-string outlet reduction as described previously. 32 Outlet reduction was performed with suture tightening over a through-the-scope fluid-filled balloon inserted through the GJA for a consistent final outlet diameter. Further reduction of the dilated gastric pouch was then performed with a series of U-shaped sutures rows placed sequentially from the GJA to the proximal gastric pouch. The endoscopic view of procedural steps is shown in Figure 2. All patients were discharged home same-day and enrolled in a comprehensive lifestyle and nutrition program that included regular follow-up with registered dietitians.

Steps of ER-OAGB. (a) Gastrojejunostomy (outlet) before revision. (b) Argon plasma coagulation of outlet. (c) Purse-string suture of outlet. (d) Gastric pouch before revision and (e) Endoscopic suturing to narrow pouch.
Calculations:
- Total body weight loss (TBWL) = (weight at time of intervention – weight at time point)/weight at time of intervention × 100
- Excess weight loss (EWL) = (weight at time of intervention − weight for BMI of 25)/weight at time of intervention × 100
- Weight recurrence = (weight at time of ER-OAGB − nadir weight after OAGB)/(weight at time of OAGB − nadir weight after OAGB) ×100.
The primary outcome was TBWL at 12 months. Secondary outcomes were technical feasibility (defined as the ability to complete the procedure with reduction of the GJA and gastric pouch); suture number; TBWL at 3, 6, and 15 months; EWL at 3, 6, 12, and 15 months; improvement, worsening or de novo symptoms of gastroesophageal reflux disease (GERD) following ER-OAGB by 12 months (per patient report of symptoms); and safety. Patients were monitored for adverse events throughout the follow-up period, which were graded according to standard definitions. 33 Baseline comorbidities were based on presence of medication used to treat the respective condition; hemoglobin A1c ⩾ 6.5% (type 2 diabetes mellitus); controlled attenuation parameter ⩾248 dB/m via transient elastography (hepatic steatosis); and/or diagnosis from another physician. Continuous variables were reported as means ± standard deviation or ranges, and categorical variables as frequencies and percentages, unless otherwise specified.
Results
A total of 17 patients (70.6% female, mean age 46.8 years, mean BMI 39.1 kg/m2) underwent ER-OAGB from June 2020 to September 2021. Patient characteristics are shown in Table 1. At the time of ER-OAGB, patients had the following obesity-associated comorbidities: hypertension (n = 7), type 2 diabetes mellitus (n = 4), and hepatic steatosis (n = 9). The average time from initial OAGB to ER-OAGB was 8 years (range 2–21 years), with an average weight recurrence at the time of ER-OAGB of 43.2% (range 10.9–86.9%) from post-OAGB nadir. The mean procedure duration was 23 min. All procedures included one purse-string suture, with an average of 2 (range 1–5) sutures for pouch reduction. Technical success was 100%. There were no instances of gastrogastric fistula identified during ER-OAGB. Patient follow-up rates at 3, 6, 12, and 15 months were 94.1% (16/17), 94.1% (16/17), 100% (12/12), and 62.5% (5/8), respectively. TBWL was 18.5 ± 2.1% at 12 months. Overall TBWL trajectory from time of OAGB to 15 months after ER-OAGB is show in Figure 3. As demonstrated in this figure, patients re-approached their post-OAGB weight nadir following ER-OAGB. EWL at 3, 6, 12, and 15 months after ER-OAGB was 30.5 ± 14.7%, 42.6 ± 16.2%, 54.2 ± 11.3%, and 54.2 ± 11.7%, respectively. Data on GERD at baseline and 12 months were available for 12 (70.6%) subjects. Of these, three (25.0%) had GERD at the time of ER-OAGB. At 12 months, GERD symptoms resolved in 2 of the 3 subjects and remained unchanged in 1 of the 3 subjects. There were no reported instances of new or worsening GERD. There were no serious adverse events for any patient during the study duration. Immediate postprocedural symptoms following ER-OAGB are similar to those observed following TORe in RYGB – namely, 1–2 days of mild cramping and substernal pressure/dyspepsia.
Cohort characteristics. Values are presented as median (range) or mean ± standard deviation.

BMI, body mass index; ER-OAGB, endoscopic revision of one-anastomosis gastric bypass; OAGB, one-anastomosis gastric bypass.
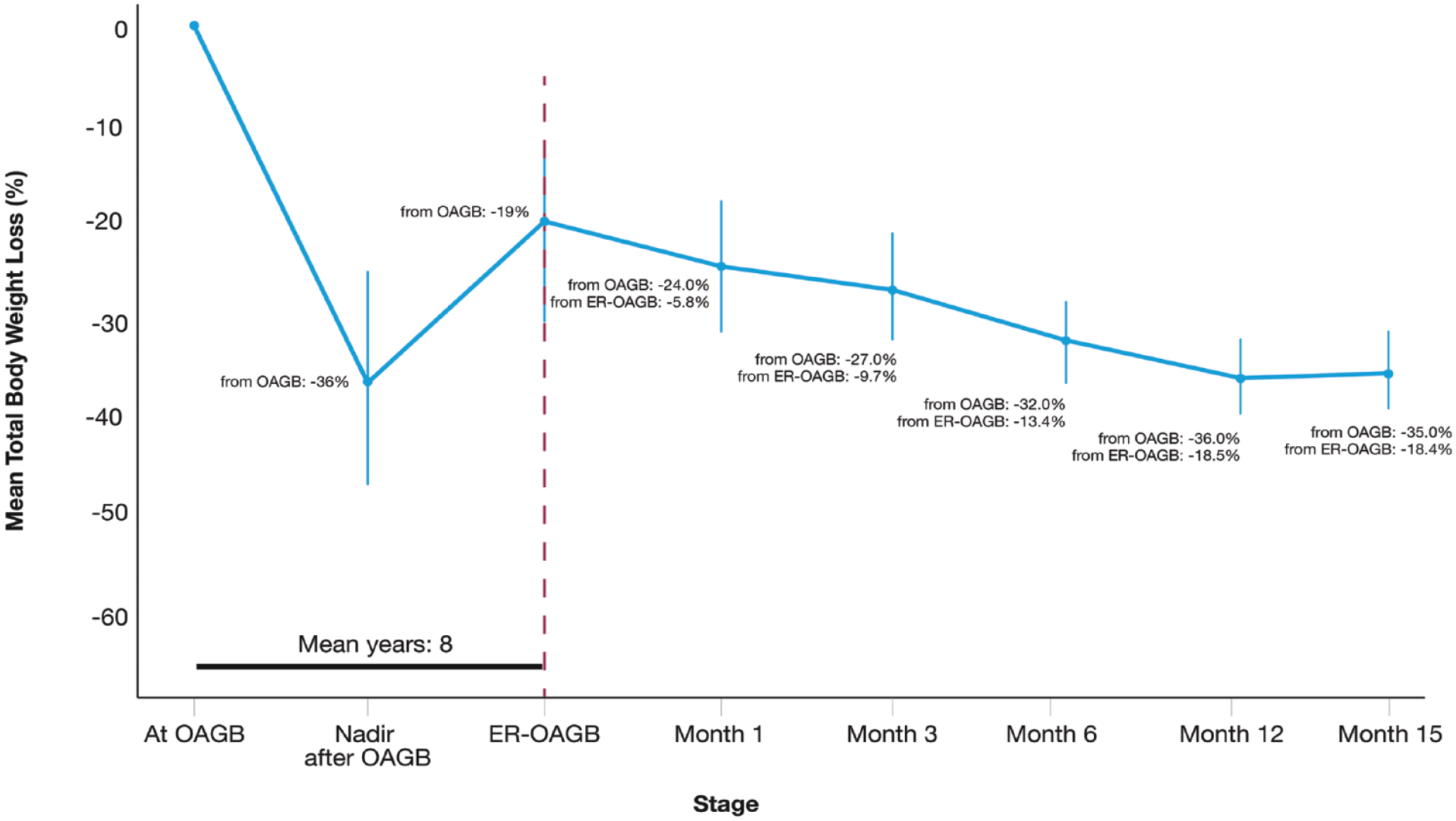
Weight Loss trajectory before and after ER-OAGB. Mean TBWL over time from original OAGB and from ER-OAGB are shown at corresponding time points.
Discussion
Consistent with the paradigm of obesity as a chronic, progressive disorder, OAGB appears to be subject to the same challenges of weight recurrence observed in other metabolic and bariatric surgeries,6,34,35 a phenomenon associated with recrudescence of comorbidities, increased health care cost, and diminished quality of life.22–24,36 Given the rising rates of both obesity and implementation of OAGB, there is a need for minimally invasive revisional therapies for weight recurrence, which may reduce the need for riskier revisional surgeries or life-long anti-obesity pharmacotherapy.37–39 This is the first account documenting the clinical efficacy and safety of full-thickness suturing post-OAGB to treat weight recurrence.
Patients undergoing ER-OAGB experienced similar weight loss to that observed in patients who underwent TORe and endoscopic revisions of sleeve gastrectomy at our centers, as well as similar to those observed in the published literature on these procedures18,19 – namely, modest compared to the initial surgery but satisfying weight loss and safety thresholds outlined in expert-level recommendations for adoption of a novel endobariatric therapy 40 and likely sufficient to improve weight-related medical comorbidities that may accompany weight recurrence. 41 In ER-OAGB, it is unclear whether GJA or pouch reduction contributes more significantly to the degree of weight loss, as both anatomical features can contribute to weight recurrence after metabolic bariatric surgery.42,43 Nevertheless, we suspect tissue ablation with the purse-string approach to GJA narrowing is preferable to tissue ablation alone or interrupted suture technique, as was shown with TORe.32,44 We also suspect that the specific suture pattern of the gastric pouch is less consequential, as it does not appear to be a major determinant of weight loss in the analogous gastric imbrication of endoscopic sleeve gastroplasty. 45 Though none were encountered in this series, as with TORe, gastrogastric fistula must be managed as part of a revision for weight management after OAGB, and this can be attempted endoscopically.46,47
A major concern of OAGB is the risk of GERD, which is observed in 5–10% of patients after OAGB and leads to revision in 2–3%.2,12,28 Historically, the prevailing speculation was that reflux was primarily biliary in nature, owing to surgical technique.27,48 While transient biliary reflux has been demonstrated after OAGB, 26 further study has demonstrated nearly equal frequency of acid reflux. 25 To manage GERD, there is consensus among experts that the gastric pouch should be as long as permitted by the patient’s anatomy, while also avoiding practices that may contribute to impaired pouch clearance of food contents, bile, or acid – such as creating an overly narrowed pouch or GJA. 2 Accordingly, many experts construct the GJA with a diameter between 40 and 50 mm, 2 and in series of patients with more narrowed GJA, there were increased reports of GERD.49,50
In the present series of ER-OAGB, both the pouch and GJA were intentionally narrowed, anatomical modifications that are hypothesized to impede pouch clearance. In this manner, it may be surprising that no patient in this series described new or worsening GERD. The reasons for this are not clear. There are OAGB surgical techniques that ostensibly help prevent reflux of both acid and bile that are unrelated to the modification from ER-OAGB – such as resection of gastric tissue (diminishing acid), as well as dependent-placement and latero-lateral construction of the GJA (attenuating bile reflux). 25 An alternative explanation is that these ER-OAGB modifications are, in some ways, protective against reflux. First, the gastric pouch is exposed to transient, physiologic biliary flow due to lack of a sphincter, and narrowing of the GJA may generate an anatomical barrier. 25 Second, the elasticity of gastric tissue can lead to pouch dilation over time, especially if involving the greater curvature, and this can lead to meal stagnation3,28 – a phenomenon potentially mediated by pouch reduction. Finally, GERD is a comorbidity associated with increased abdominal pressure from central adiposity, and thus, weight loss observed in this case series may itself be a protective factor against GERD. 51 Ultimately, improvement in or worsening of GERD is likely to be multifactorial with ER-OAGB, and future study may include pH-impedance testing to help inform appropriate patient selection based on type and severity of reflux, as has been done to guide surgical revision of OAGB. 28
This case series suggests that ER-OAGB can serve as a promising weight loss tool for patients with weight recurrence after OAGB wishing to avoid surgical revision or long-term anti-obesity pharmacotherapy. However, given the small size of this cohort, further validation is needed to confirm the efficacy and safety of this technique, including the frequency of outlet stenosis, which is observed in approximately 3–4% of patients undergoing the analogous TORe procedure, but which was not observed here. 44 Additionally, further study could expand on this series’ limitations through thorough and objective assessment of the effects of ER-OAGB on weight-related medical conditions and GERD (from bile or acid). Still, given that TORe has FDA authorization for patients with weight recurrence after RYGB, OAGB use is increasing, and there is growing interest from physicians and patients in endobariatric therapies, it stands to reason that patients will seek out ER-OAGB in increasing numbers. Centers offering endobariatric therapies, especially revisional procedures, should be prepared to encounter such patients.
Supplemental Material
sj-jpg-1-cmg-10.1177_26317745231210120 – Supplemental material for Endoscopic revision of one-anastomosis gastric bypass (ER-OAGB) for weight recurrence: a case series of 17 adults
Supplemental material, sj-jpg-1-cmg-10.1177_26317745231210120 for Endoscopic revision of one-anastomosis gastric bypass (ER-OAGB) for weight recurrence: a case series of 17 adults by Daniel B. Maselli, Anna C. Hoff, Ashley Kucera, Areebah Waseem, Chase Wooley, Lauren L. Donnangelo, Brian Coan and Christopher E. McGowan in Therapeutic Advances in Gastrointestinal Endoscopy
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.