
Abstract
Background:
Reports suggest that the rate of adverse events (AEs) post-endoscopic sphincterotomy (ES) to be as high as 10%, with gastrointestinal bleeding being most common after post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis.
Objective:
The aim of this study was to characterize the incidence of bleeding in patients with thrombocytopenia following ES.
Design:
Retrospective observational cohort study.
Methods:
Patients with thrombocytopenia (defined as <150,000 platelets/μL) who underwent ES between May 2017 and December 2020 were identified at a tertiary care medical center. The incidence of immediate (intraprocedural oozing >5 min or requiring intervention) or delayed (clinical bleeding with associated hemoglobin drop within 14 days) post-ES bleeding was determined via manual chart review.
Results:
A total of 221 patients with a mean platelet count of 108,000 ± 13,000 platelets/μL underwent ERCP with ES. Immediate bleeding occurred in 11 (5%) patients with no significant drop in hemoglobin or transfusion requirement. Two patients (0.9%), both of whom were noted to have immediate bleeding, also developed delayed bleeding. Presence of malignancy was associated with an increased risk of bleeding (36.4% versus 11.4%, p = 0.037) while platelet count was not.
Conclusion:
In a cohort of patients with thrombocytopenia, rates of immediate and delayed bleeding are similar to previously reported AE rates of ES in the general patient population. Careful attention should be given to patients with a history of active malignancy as well as those who develop immediate bleeding as they appear to be at increased risk for bleeding complications.
Plain language summary
The sphincter that controls the flow of bile into the small bowel is often cut for a variety of clinical indications (sphincterotomy) during a procedure called endoscopic retrograde cholangiopancreatography (ERCP). One of the complications of this maneuver is bleeding. The physiology of bleeding is complex, and the risk of bleeding cannot be well captured by a single condition or laboratory test. It was presumed that low platelet counts would increase a patient’s risk of bleeding during a procedure, but emerging data suggests that many endoscopic procedures are safer than previously understood in these patients. However, there is limited data for sphincterotomy and ERCP. This study from a single, academic center evaluates the outcomes of all patients who underwent sphincterotomy with platelets that were below the normal threshold. Overall, the data shows that sphincterotomy appears to be as safe in patients with low platelets as the general population. Patients with active cancer may be at slightly higher risk for bleeding. Additional precautions may be needed in this group, however further studies are needed to confirm this finding.
Introduction
Endoscopic sphincterotomy (ES) at the ampulla of Vater was first described in 1974 using electrosurgical techniques originally developed for polypectomy. 1 Since its introduction, ES has become a cornerstone of therapeutic endoscopic retrograde cholangiopancreatography (ERCP), facilitating stone extraction, stenting, and other pancreaticobiliary interventions. Published data suggest that at least 150,000 sphincterotomies are performed annually; however, this number has increased with almost half a million ERCPs now performed annually in the United States alone.2,3 Despite its relative safety compared to surgery, the rate of adverse events (AEs) post-ES is as high as 10% and includes post-ERCP pancreatitis, cholangitis, perforation, and bleeding. 3 Clinically significant bleeding has been noted in 1–3% of patients undergoing ES when prospectively assessed. However, predicting which patients will develop bleeding is difficult given the heterogeneity of studies, procedure indications, and patient populations.4,5
Platelet count is frequently used to assess procedural bleeding risk at the point of care as patients with thrombocytopenia seem to be at an increased risk of gastrointestinal bleeding overall. 6 Thrombocytopenia has traditionally been considered a definitive risk factor for post-sphincterotomy bleeding but only when broadly defined as coagulopathy which included renal-disease-associated platelet dysfunction and elevated international normalized ratio (INR). 7 Current guidelines recommend a minimum platelet count of 50,000/μL for high-risk endoscopic procedures for bleeding, such as ERCP with ES, with rapid correction if a procedure is unable to be postponed.8,9 These recommendations are based largely on expert opinion.
Recent studies suggest that common endoscopic procedures including biopsy, polypectomy, and hemostatic interventions are safe in thrombocytopenic patients, but there is a paucity of data on ERCP in this setting.10–12 The purpose of the current study is to characterize the risk of post-sphincterotomy bleeding in a modern cohort of patients with thrombocytopenia. As a secondary outcome measure, we examined cases of bleeding to determine the presence of other risk factors and provide real-world data on bleeding management.
Materials and methods
Patient identification
Consecutive patients with thrombocytopenia who underwent ERCP with ES between May 2017 and December 2020 were identified through an electronic medical record database query from a single tertiary care center. Thrombocytopenia was defined as a platelet count <150,000/μL with confirmatory platelet count measurement within 7 days of the procedure. Degree of thrombocytopenia was further classified as mild (101,000–150,000 platelets/μL), moderate (51,000–100,000 platelets/μL), or severe (⩽50,000 platelets/μL). Patients were excluded if they were less than 18 years old, pregnant, did not have platelet count data available within 7 days of the procedure, had a pre-procedure platelet count ⩾150,000/μL without transfusion, or ES was not performed.
Data were abstracted through individual chart review. Clinical data obtained included level of care, etiology of thrombocytopenia, coexisting comorbidities (e.g. chronic kidney disease, end-stage renal disease, active malignancy, heart failure), and concern for cholangitis. The use of anticoagulant or antiplatelet medications and medication class were recorded. Discontinuation times for anticoagulants are generally 4 h for heparin, 12 h for low molecular weight heparin, 5–7 days for warfarin with goal INR <1.5, and 48–72 h for direct oral anticoagulants. Regarding antiplatelet agents, aspirin is continued and clopidogrel held 72 h when possible. Procedure reports were reviewed to determine procedure indication, duration, and whether any interventions were performed in addition to sphincterotomy. Sphincterotomy details included anatomic location, technique, and length. Sphincterotomy length was visually estimated by the performing endoscopist.
Outcomes
The primary outcome measured was the incidence of post-sphincterotomy bleeding, further classified as immediate or delayed. Immediate bleeding was defined as intraprocedural oozing lasting more than 5 min or requiring intervention. Delayed bleeding was defined as clinical bleeding (melena, hematochezia, hematemesis) with associated hemoglobin drop within 14 days of index procedure. Severity of the bleeding was classified as per prior consensus criteria from Cotton et al. 13 and included mild (hemoglobin drop <3 g/dL without transfusion), moderate [⩽4 units packed red blood cells (PRBC) transfused and no angiographic or surgical intervention], or severe bleeding (>4 units PRBC transfused or requiring angiographic or surgical intervention). Additional outcomes of interest were changes in hemoglobin pre- and post-procedure, an upgrade to intensive care unit (ICU) level of care, and the need for interventional radiology or surgical intervention.
Statistical analysis
Quantitative variables were described with mean value and standard deviation (SD). Categorical data were reported as relative proportions (%). Univariate analysis was performed to compare clinically relevant variables between patients who developed bleeding and those who did not. Data management, analysis, and visualization was performed using BlueSky Statistics software (version 7.10, BlueSky Statistics LLC, Chicago, IL, USA).
Results
Baseline clinical characteristics
The initial database query identified 238 patients with 221 meeting inclusion criteria. Ten patients were found not to have thrombocytopenia and seven did not have a platelet count performed within 7 days of the procedure. Clinical information regarding the 221 analyzed patients is outlined in Table 1. Patients were predominantly male (68%) with a mean age of 71 years (SD ±15) and body mass index (BMI) of 30 kg/m2 (SD ±7). The mean platelet count was 108,000 platelets/μL (SD ±13,000). Severe thrombocytopenia was seen in 11 (5%) patients with three receiving pre-procedure platelet transfusions, moderate in 63 (29%), and mild in 147 (67%) (Figure 1). Cirrhosis was present in 25 patients (11%) with most thrombocytopenia attributed to a non-cirrhotic etiology (n = 196, 89%). A total of 62 patients (28%) had chronic kidney disease, 6 (3%) had end-stage kidney disease, 28 (13%) had active malignancy, and 33 (15%) had heart failure. Antiplatelet and anticoagulant use is shown in Table 2. Of the five patients on a thienopyridine (all clopidogrel), four were on dual therapy with aspirin, and one was on monotherapy.
Baseline clinical characteristics of patients with thrombocytopenia who underwent endoscopic sphincterotomy.
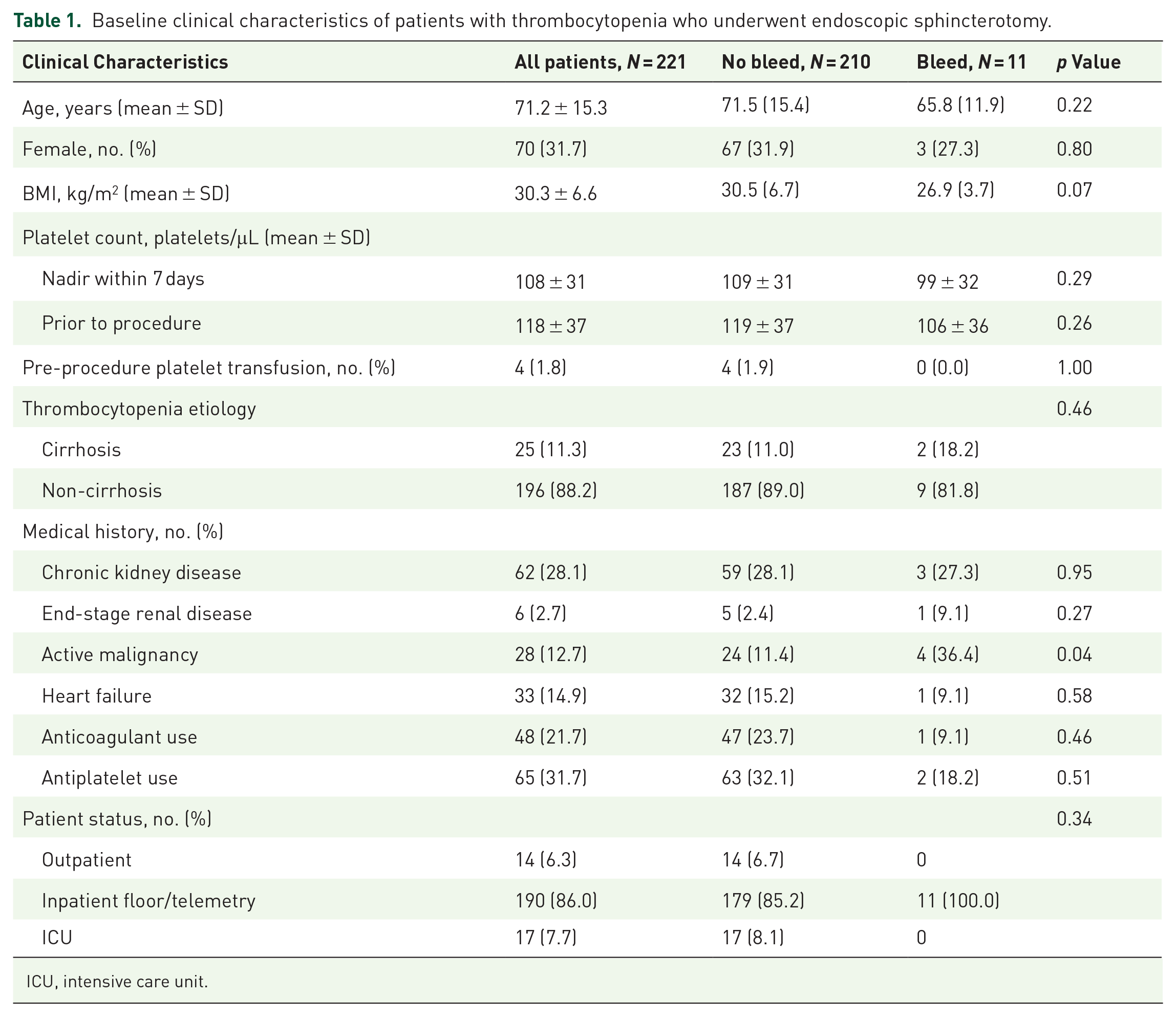
ICU, intensive care unit.

Incidence of bleeding stratified by the degree of thrombocytopenia.
Anticoagulant use in patients who did not versus did experience bleeding after endoscopic sphincterotomy.

DOAC, direct oral anticoagulant; LMWH, low molecular weight heparin.
Procedural characteristics
The majority of ERCPs were performed on inpatients from a standard hospital unit (n = 190, 86%) (Table 3). Choledocholithiasis was the most common indication (n = 184, 83%) followed by biliary stricture (n = 16, 7%). There was clinical concern for cholangitis in 81 (37%) cases. Biliary sphincterotomy was technically successful in all cases with an average procedure duration of 40 min (SD ±34). Three patients (1%) underwent dual pancreaticobiliary sphincterotomy. Standard traction technique was utilized in 209 (95%) cases with an average incision length of 7 mm (SD ±2) documented in the 109 (49%) procedure reports. Removal of choledocholithiasis was performed in 119 (54%) cases, and stents were placed in 19 (9%) (8 biliary, 9 pancreatic, 2 both). There were no significant differences in the above procedural characteristics on univariate analysis when compared between patients who did and did not develop bleeding.
Procedure characteristics.

Immediate bleeding
Immediate bleeding occurred in 11 (5%) patients with pre-procedure platelet counts ranging from 51,000 to 144,000 platelets/μL. None of the patients in this cohort with platelet count less than 50,000 platelets/μL experienced post-ES bleeding. The only difference between patients who developed bleeding and those who did not on univariate analysis was the presence of malignancy (11.4% patients without bleeding versus 36.4% patients with bleeding, p = 0.037). When further specified for patients with malignant biliary obstruction, this association persisted (1.4% without bleeding versus 18.2% with bleeding, p = 0.02). However, no sphincterotomy was performed through malignant tissue. Notably, platelet count was not significantly associated with the development of bleeding. There was no significant difference in sphincterotomy length between patients who experienced bleeding and those who did not (5.9 ± 2.4 cm versus 7.3 ± 2.4 cm, p = 0.07).
Hemostatic intervention was performed in 9 of the 11 cases and most frequently involved the use of epinephrine (7/9); however, APC and clip placement were also used (Table 4). Post-procedure hemoglobin decreased only slightly by an average of 0.6 g/dL (SD ±0.4) in patients who experienced immediate bleeding. None required administration of blood products or change in level of care.
Clinical details on patients who experienced bleeding.

Reported as 103 platelets/μL.
AC, anticoagulant; AKI, acute kidney injury; APC, argon plasma coagulation; ASA, aspirin C cirrhosis; CHF, congestive heart failure; CKD, chronic kidney disease; Epi, epinephrine; ESRD, end-stage renal disease; FCMS, fully covered metal stent; NC, non-cirrhosis; PC, platelet count; POD, post-operative day.
Delayed bleeding
Delayed bleeding was seen in two cases (1%), both of which had immediate bleeding noted during index ERCP. One patient who underwent ERCP for choledocholithiasis with a platelet count of 137,000/μL had a history of chronic kidney disease and heart failure. Hematochezia developed on post-procedure day 2 and required 14 units of PRBC, 2 packs of platelets, and transfer to the ICU. Bleeding was controlled with fully covered self-expanding metal stent (FCSEMS) placement without rebleeding. The other patient had an end-stage renal disease and a platelet count of 56,000/μL. Melena developed 14 days after undergoing ERCP for biliary obstruction, requiring 8 units of PRBC, 1 pack of platelets, and transfer to the ICU. Bleeding was controlled with FCSEMS and epinephrine injection. In this patient, there was concern for rebleeding 2 days later, but repeat endoscopy showed no signs of recurrent hemorrhage.
Discussion
The incidence of post-sphincterotomy bleeding in this high-risk cohort with thrombocytopenia was 5% for immediate bleeding and 1% for delayed bleeding. These results are similar to previous results of ERCP and sphincterotomy in a general population.4,14 With a strict definition of clinically significant bleeding (e.g. melena or hematochezia with a hemoglobin drop >2 g/dL), rates are closer to 1–2%.3,7,13 Studies that include endoscopic bleeding defined by oozing lasting greater than 2–5 min report rates closer to 10–12%, slightly higher than the rates seen here.15–17
ES is considered a high-risk procedure which is typically defined by a procedural bleeding risk ⩾1%.18,19 In a review on the subject, Freeman 7 outlined ‘definitive’ risk factors for post-sphincterotomy bleeding to include anticoagulation within 3 days, cholangitis, bleeding during the procedure, low endoscopist case volume, and broadly defined coagulopathy, which included patients with a platelet count less than 80,000 platelets/μL. While thrombocytopenia has been shown to increase the risk of gastrointestinal bleeding by almost 2.5-fold at a population level, its role in post-sphincterotomy bleeding has not been fully examined. 20 In one analysis of 783 endoscopies performed in neutropenic or thrombocytopenic patients, 35 ERCPs were included with 31 sphincterotomies performed. 21 Zero bleeding AEs were reported within the ERCP cohort; however, specific clinical data on these individuals was not available. In our study cohort, the presence of thrombocytopenia alone did not seem to increase the risk of post-ES bleeding. Rather, the only clinical factor associated with bleeding was the presence of malignancy.
Malignancy has been associated with hematologic disturbances and a disruption of normal coagulation that place patients at increased risk of both thrombosis and hemorrhage. 22 While malignancy has not been formally described as a risk factor for post-sphincterotomy bleeding, patients with cancer are at an increased risk of developing clinically relevant bleeding overall. 23 The reason for this is likely multifactorial, including issues with impaired coagulation factor synthesis, preexisting mild factor deficiencies, vessel wall erosion, or disseminated intravascular coagulation (DIC). 24 Our findings support the current understanding that hemostasis is much more complex than any single laboratory value, and it is important that risk assessment extend beyond laboratory parameters with careful attention given to relevant comorbidities like cancer.
The target of 50,000 platelets/μL currently suggested in clinical guidelines is based on expert opinion with some limited data from bone marrow transplant patients, but it is not clear that platelet transfusion to this threshold decreases the risk of bleeding.25–27 With over 2 million performed annually in the United States, platelet transfusions are resource intensive and carry multiple risks, including sepsis from a contaminated product, anaphylaxis, and hemolysis. Furthermore, blood products are a limited commodity and should only be used when deemed absolutely necessary. Given the constrained availability, better data are needed to identify those at risk for bleeding and optimize the use of this limited resource. 9 Emerging studies suggests that endoscopy can be performed safely in those with lower platelet counts, including interventions like biopsy, polypectomy, and hemostasis.11,12,21 Nevertheless, guidelines continue to recommend a threshold of 50,000 platelets/μL.8,28,29 The European Society for Gastrointestinal Endoscopy defined a platelet count of less than 50,000/μL as a risk factor for post-ES bleeding, but the cited study only included four patients with a platelet count below this threshold.19,30 All of the patients in our study with severe thrombocytopenia safely underwent sphincterotomy without any AEs and the majority did not receive pre-procedure platelet transfusion. Additional studies assessing the safety of endoscopic sphincterectomy in patients with <50,000 platelets/uL would help minimize unnecessary transfusions along with their associated risk and cost to the healthcare system.
When bleeding did occur, there was significant variation in endoscopic management, particularly with immediate bleeding. We suspect that this accurately represents real-world practice as there is no clear data on an optimal therapeutic approach. Epinephrine alone is often sufficient to control immediate bleeding, but thermal and mechanical therapies can also be used.16,17,31 FCSEMSs have shown particular promise with up to 100% efficacy in some series.32,33 All these therapeutic modalities were employed in varying combinations despite the relatively low incidence of bleeding in our study. The two patients who developed severe delayed bleeding were both effectively treated with FCSEMSs without recurrence. Notably, prior to this, both patients treated for immediate bleeding with epinephrine and epinephrine with clip. While this sample size is too small to draw prescriptive conclusions, immediate bleeding was more closely associated with the development of delayed bleeding than severe thrombocytopenia. This highlights the need for more rigorous data regarding the optimal management of immediate bleeding and how best to prevent clinically significant hemorrhage, particularly in high-risk patients like those with thrombocytopenia undergoing ES.
Limitations of this study include its retrospective, single-center design as well as the small number of delayed bleeding events which prevented a more robust analysis of predictive factors. Patients may have experienced AEs post-discharge and presented locally, which would not necessarily be recorded in the electronic medical record. However, we are confident that almost all events were captured as post-procedural AEs and, at a minimum, communicated to the performing facility or, more commonly, transferred back. In addition, there is no true control group in this study, and extensive previously published data on the risk of post-ES bleeding was utilized for comparison. All procedures were performed at a high-volume tertiary care center with experienced endoscopists, which alone may decrease the risk of AEs when compared to the general population. 34
While thrombocytopenia has traditionally been considered a significant risk factor for periprocedural bleeding, this study has demonstrated similar rates of immediate and delayed bleeding post-ES in patients with thrombocytopenia compared to historical data in average patients. Ultimately, thrombocytopenia alone did not seem to correlate with an increased risk of post-sphincterotomy bleeding and data from this cohort of patients showing relative safety with any degree of thrombocytopenia should encourage further investigation. Attention should be given to the patient’s comorbidities like the presence of malignancy rather than any individual laboratory value, including platelet count. Additional prospective studies are needed to validate the safety of high-risk endoscopic procedures in this cohort.