
Abstract
Intraductal biliary lesions can involve the main hepatic confluence. Assessment of the extension of pedunculated biliary lesions during per-oral cholangioscopy (POCS) can optimize and personalize the surgical strategy. Four consecutive cases of pedunculated biliary lesions were analysed. Cholangioscopy was performed with a disposable single-operator cholangioscope. POSC was successfully performed in four patients (three female, mean age 50 years), showing involvement of the main biliary confluence in three of four pedunculated biliary lesions; direct biopsy sampling was diagnostic in two of three cases (in one patient, biopsy were not performed due to the smooth appearance of the intrabiliary lesion). No adverse events occurred after POCS. Surgery required excision of the main hepatic confluence in two of three cases (one patient was not resectable). POCS can diagnose intrabiliary extension of protruding biliary lesions, providing important information to plan the surgical intervention.
Introduction
Protruding biliary lesions are uncommon findings during radiological or endoscopic evaluation of the biliary tree. Arising with abdominal pain, jaundice, fever, itching and cholestasis, the clinical presentation can mimic neoplastic biliary obstruction or biliary stones. Therefore, diagnosis of these lesions can be challenging. In the past, these were usually discovered as incidental findings during surgery. Nowadays, they can be detected and characterized by peroral cholangioscopy (POCS), which provides direct vision of the biliary tree. 1 Targeted biopsies for pathological characterization can be also performed. Furthermore, POCS can define the anatomical extension of the lesions within the bile duct, which is important to plan the appropriate surgical strategy.
In this paper, the role of POCS for a target approach to four cases of unusual protruding biliary lesions will be discussed. Retrospective review of cholangioscopy cases was approved from the Ethical Committee of the Catholic University of Rome on 27 September 2021 (ID 4304).
Case 1
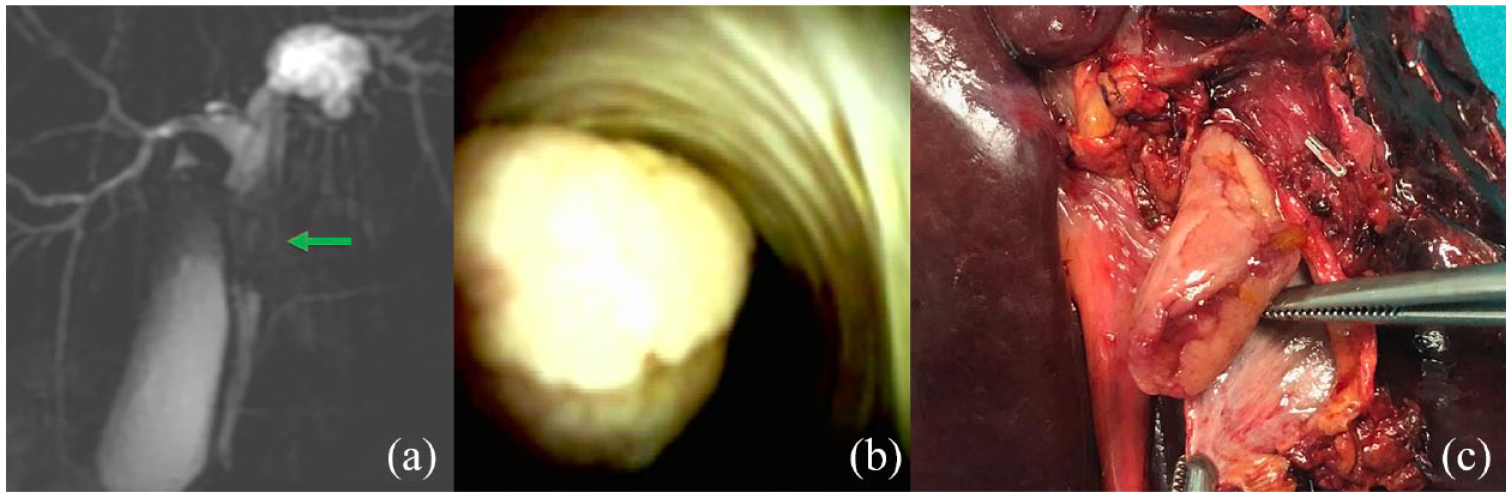
A 56-year-old female was admitted for a right upper quadrant colicky abdominal pain radiating to the right shoulder. Abdominal ultrasound (US) revealed dilatation of the left hepatic duct without biliary stones. Liver functions tests (LFT) showed normal bilirubin and mild cholestasis. A significant dilatation of the left biliary ducts due to the presence of a protruding biliary lesion with contrast enhancement and obstructing the left hepatic duct were evident on magnetic resonance cholangiopancreatography (MRCP) [Figure 1(a)]. The lesion was close to the biliary confluence, and the right biliary ducts were not dilated. After multidisciplinary discussion, endoscopic retrograde cholangiopancreatography (ERCP) with cholangioscopy was performed to obtain biopsy of the lesion and define the involvement of the confluence. POCS (SpyGlass DS, Boston Scientific, USA) showed a protruding lesion with an adenomatous appearance [Figure 1(b)] originating from the left hepatic duct and invading the proximal common bile duct; the biliary confluence was involved by the lesion without extension into the right sectorial ducts. Targeted biopsies with SpyBite (Boston Scientific, USA) were performed. Biliary stenting was not needed due to the absence of bile ducts stenosis. Pathology diagnosed a papillary villous adenoma [intraductal papillary neoplasms of the bile duct (IPNB)] with high-grade dysplasia. Left hepatectomy with resection of the biliary confluence [Figure 1(c)] was performed. Final pathology showed foci of adenocarcinoma in IPNB with high-grade dysplasia (pT1a pN0 pMx).

Magnetic resonance cholangiography shows a filling defect of the left hepatic duct (arrow) (a); cholangioscopy confirms the pedunculated lesion (b) which was treated by left hepatectomy and excision of the biliary confluence (c).
Case 2
A 50-year-old female with a history of epigastric pain underwent abdominal ultrasonography (US). A 3-cm lesion of uncertain definition was diagnosed in the common bile duct. LFTs were normal. MRCP [Figure 2(a)] showed no biliary stones but confirmed the presence of tissue protruding into the mid common bile duct. Left and right intra-hepatic ducts were not dilated. Cholangioscopy (SpyGlass DS, Boston Scientific, USA) showed a protruding polypoid lesion with a fibrotic aspect originating from the left hepatic duct and invading the biliary confluence [Figure 2(b)]. Biopsy with the SpyBite forceps (Boston Scientific, USA) revealed fibrotic tissue with mucosal inflammation. Biliary stents placement was not needed due to the spontaneous and complete drainage of contrast from the intra-hepatic radicles. Left hepatectomy with resection of the biliary confluence [Figure 2(c)] was performed. Final pathology showed a pyloric gland adenoma without lymph nodes metastases.
Magnetic resonance cholangiography shows a filling defect the common bile duct (arrow) (a); cholangioscopy confirms the intrabiliary lesion (b); surgery required left hepatectomy and resection of the biliary confluence (c).
Case 3
A 29-year-old female was admitted for epigastric pain complaining of recurrent mild epigastric pain and occasional itching. Blood tests showed raised bilirubin and cholestasis. Abdominal US revealed a 6.5-cm multilocular cyst in the IV hepatic segment. Serology for major hepatotropic viruses, echinococcus and autoimmune hepatitis were negative. MRCP [Figure 3(a)] and computed tomographic (CT) scan showed right and left intra-hepatic radicles dilatation and an 8 × 6 × 6 cm complex cyst of segment IVb with contrast enhancement and suspicious appendix filling the left hepatic duct. POCS (SpyGlass DS, Boston Scientific, USA) diagnosed a polypoid lesion with a smooth and normal mucosa [Figure 3(b)], protruding from the left hepatic duct into the proximal common bile duct, without involvement of the biliary confluence; biopsies were not performed due to the normal appearance of the mucosa. The lesion appeared an appendix of the liver cyst protruding into the biliary ducts. Based on the cholangioscopy, a left hepatectomy [Figure 3(c)] was performed preserving the biliary confluence; the intrabiliary appendix of the cyst was easily extracted together with the left liver lobe. Final pathology diagnosed a mucinous cystic neoplasia with low-grade dysplasia.

Magnetic resonance cholangiography shows a cyst of liver segment IV (arrowhead) and common bile duct filling defect (arrow) (a) as confirmed from cholangioscopy (b); left hepatectomy obtained cyst removal together with its biliary protrusion (arrow) (c).
Case 4
A 66-year-old male was admitted to the hospital due to epigastric pain, fever and rising LFTs; CT scan and MRCP showed multiple intra and extra-hepatic filling defects compatible with stones with diffuse bile tree dilation [Figure 4(a)]. ERCP was attempted to remove biliary stones, cholangiography confirmed the MRCP findings (filling defects with a biliary stones appearance), but surprisingly fragments of tissue were extracted with a Dormia basket; the tissue was retrieved for histology which revealed papillary villous adenoma (IPNB) with high-grade dysplasia. Cholangioscopy (SpyGlass DS, Boston Scientific, USA) was performed and showed multifocal protruding papillary lesions in the distal common bile duct and in the biliary confluence [Figure 4(b)] involving also the right intra-hepatic ducts. After multidisciplinary discussion, the patient was candidate, due to the POCS findings, to duodenopancreatectomy and right hepatectomy with excision of the biliary confluence after right portal vein embolization. However, due to the risks of this major surgery, the patient refused the treatment and is still on follow-up.

Magnetic resonance cholangiography and multiple bile ducts filling defects (a); cholangioscopy shows papillary lesion involving the biliary confluence (b) and the distal common bile duct.
Discussion
POCS may represent a useful tool for the diagnosis of protruding biliary lesions. Up to date, only few cases of lesions protruding into the biliary tree have been published, mainly case reports or case series. Most of these cases have been described on surgical specimens. 2 Only few series evaluated the role of POCS to diagnose protruding biliary lesions.3,4
Since its introduction in 1970, cholangioscopy gained progressive attention. 5 While the mother–baby system was heavily burdened by the fragility of the scope, the poor quality of the images and the inconvenience of requiring two operators, the novel peroral cholangioscope (SpyGlass DS, Boston Scientific, USA) is currently a feasible single-operator instrument for high-resolution visualization of the biliary tree. 6
Providing a direct visualization of the lesion, POCS can easily discriminate between stones and protruding lesions, and target biopsies can be performed under visual control. Moreover, POCS provides important information to personalize the appropriate surgical resection strategy, giving a detailed evaluation of the extent within the biliary tree.
Most of the lesions described in this series are IPNBs, which have been recently described as pre-invasive tumours of the bile ducts preceding cholangiocarcinoma (CCA).7–9 Reported malignant transformation into CCA range from 41% to 83%.10,11 Due to the high risk of malignancy and recurrent biliary obstruction, a prompt surgical intervention of IPNB is recommended. Surgery is planned according to the location of the lesion. Extrahepatic IPNBs are usually removed by Whipple resection, while intrahepatic or perihilar lesions are managed by hepatobiliary resection. 12 Local excision for the middle part of the extrahepatic bile duct has also been described. 13
While cholangiocarcinoma is usually characterized by a narrow and hard stenosis which may be difficult to pass, in our cases the protruding lesions were movable, soft and could be easily passed with the cholangioscope thus exploring the origin of the protruding lesion and its longitudinal extension. Involvement of the intra-hepatic ducts and main confluence was always evaluated to give precise anatomical information for surgery. In case 3, it was possible to perform a left hepatectomy preserving the biliary confluence. On the other hand, case 4 had a massive extension of the disease with multiple synchronous lesions in the common bile duct, in the confluence and in the intrahepatic ducts which required a complex surgical approach, which was refused by the patient.
Biliary stenting was never necessary in our series because the protruding lesions were never rigid and only partially obstructing the bile ducts, as documented by the absence of jaundice in all cases. POCS was tolerated in all patients, and no adverse events related to procedure were recorded. Patients 1, 2 and 3 underwent surgery without episodes of cholangitis after cholangioscopy and patient 4 was in good clinical condition 5 months after POCS.
An interesting finding of this series is the rare histology of case 2. Only few pyloric gland adenomas of the bile duct have been discussed in the literature so far. First, described by Kurt Elster in 1976, it was initially not recognized as a neoplasm. In the stomach, it accounts for <3% of gastric polyps. 14 It is also relatively common in the gallbladder, where it represents the most common type of benign epithelial neoplasm. 15 However, it rarely occurs in the extrahepatic bile ducts. 2
Hatzibougias et al. 16 reported a case of a protruding lesion located at the main hepatic confluence and extending into the left hepatic duct. Similarly, Vieth et al. 2 described three cases of pyloric gland adenoma located in the common bile duct; in one case a transition to well-differentiated adenocarcinoma was shown. Schaefer et al. 17 also reported a case of a 2 cm lesions protruding from the cystic duct to the common bile duct in a 62-year-old male patient. Histology revealed pyloric gland adenoma with transition into well-differentiated adenocarcinoma and high-grade biliary intraepithelial neoplasia. Due to the risk of neoplastic progression, a prompt diagnosis is needed to plan the appropriate surgical treatment. POCS was effective and safe also for diagnosis of this rare lesion.
Summary
In this series, protruding biliary lesions were caused by IPNBs or other rare precancerous conditions (i.e. pyloric gland adenoma). Due to the risk of neoplastic progression, a precise and prompt diagnosis is required. Providing a direct access to the bile ducts for targeted biopsies and direct inspection of the extent of the disease, POCS may represent a promising tool for diagnosis of protruding biliary lesions and planning the appropriate surgical strategy.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.