
Abstract
Background:
This study aimed to analyze the landscape of publications on bariatric metabolic surgery through machine learning and help experts and scholars from various disciplines better understand bariatric metabolic surgery’s hot topics and trends.
Methods:
In January 2021, publications indexed in PubMed under the Medical Subject Headings (MeSH) term ‘Bariatric Surgery’ from 1946 to 2020 were downloaded. Python was used to extract publication dates, abstracts, and research topics from the metadata of publications for bibliometric evaluation. Descriptive statistical analysis, social network analysis (SNA), and topic modeling with latent Dirichlet allocation (LDA) were used to reveal bariatric metabolic surgery publication growth trends, landscape, and research topics.
Results:
A total of 21,798 records of bariatric metabolic surgery–related literature data were collected from PubMed. The number of publications indexed to bariatric metabolic surgery had expanded rapidly. Obesity Surgery and Surgery for Obesity and Related Diseases are currently the most published journals in bariatric metabolic surgery. The bariatric metabolic surgery research mainly included five topics: bariatric surgery intervention, clinical case management, basic research, body contour, and surgical risk study.
Conclusion:
Despite a rapid increase in bariatric metabolic surgery–related publications, few studies were still on quality of life, psychological status, and long-term follow-up. In addition, basic research has gradually increased, but the mechanism of bariatric metabolic surgery remains to be further studied. It is predicted that the above research fields may become potential hot topics in the future.
Introduction
Over the last 30 years, the prevalence of obesity has increased impressively worldwide. 1 Concomitantly, the rise of obesity has brought about a variety of complications, such as diabetes, cardiovascular disease, and stroke. 2 Bariatric metabolic surgery (BMS) should be considered when conservative treatment fails for severe obesity. BMS is currently considered the most effective obesity treatment and is becoming a common surgical practice. 1 With the rapid development of BMS, the number of publications is overgrowing. However, in many research literature, it is difficult for researchers from different fields to grasp the overview and frontiers of BMS. Therefore, it is essential to sort out and present the hot topics, development trends, and overall landscape of BMS.
Bibliometrics is often used to analyze academic literature quantitatively. Previous similar studies have examined the most frequent surgical procedures in each country.1,3–6 Moreover, the relationship between surgical activities and scientific production in the bariatric field has recently been analyzed. 1 However, previous BMS studies mainly focused on a specific field and lacked a comprehensive overview. To promote understanding and collaboration between different disciplines, we integrate publications on BMS from other disciplines or research areas for a complete and multidimensional analysis.
Social network analysis (SNA) and topic modeling can effectively deal with huge literature data. 7 SNA is a prominent bibliometrics method and is often used to detect topics and identify hot spots to guide future research.8,9 However, SNA has not yet been used in the field of BMS. The latent Dirichlet allocation (LDA) is one of the most classical topic modeling methods to describe large amounts of unstructured text in bibliometrics. 10 LDA creates a feature glossary based on how often terms coexist in the document set and then determines the probability of articles belonging to a particular topic based on how often terms occur in each document. 11 It was reported that the LDA was used for thematic analysis in rectal cancer publications and found a lack for basic medical research. 10 However, similar studies on BMS have not been reported.
This study analyzed the themes of publications on BMS indexed by PubMed under the Medical Subject Headings (MeSH) term ‘Bariatric Surgery’. We use machine learning (SNA and LDA) to conduct a more detailed analysis of BMS publications to highlight areas lacking and identify fields in which opportunities will exist in the future.
Materials and methods
Data source and descriptive statistics analysis
The MeSH term ‘Bariatric Surgery’ from 1946 to 2020 was searched on PubMed. Data were downloaded in TXT format on 3 January 2021. Only the retrieval results in English were downloaded for bibliometric analysis. Two surgeons and an engineer analyzed this study. First, the number of publications per year was calculated and the overall growth trend was analyzed. Second, LDA was used to classify the topics of PubMed. A river map was created to represent the change of subjects. In the river map, the river’s width represents the percentage of each subject in the year. In addition, the volume of journal publications was analyzed.
Social network analysis
According to the classification of study subjects, the subjects were clustered and a co-keywords network was constructed to reflect the current research status of BMS. Keywords with a frequency above 20 were selected to build a co-keywords network. VOSViewer was used to draw the timeline graph of topic clustering. 4 Different topics were arranged horizontally in the topic clustering graph and keywords under different topics were arranged vertically according to their publication year. It reflects the trend of various issues over time.
LDA analysis
We used the LDA to identify more specific topics in each article. The number of 50 topics was set and the topics were modeled using Python to analyze abstracts of articles in our records. Topic numbers were selected appropriately based on legibility, perplexity, and redundancy.10,12 Each topic was named by manual inspection based on abstract and MeSH terms. Two surgeons performed the topic naming in a blind manner (with 2 and 10 years of experience, respectively). For each paper, we determined the two topics with the highest attribution probability, calculated the simultaneous occurrence of the two topics, and finally established the links between the topics. To identify the relationships between topics, Louvain algorithm is used for cluster analysis to build a topic network. 10 The software package Gephi was used for network visualization (https://github.com/gephi/gephi). 13 The study did not require ethics committee approval.
Results
Overview data
MeSH retrieved a total of 21,798 publications under the term ‘Bariatric Surgery’. The growth trend of BMS publications is shown in Figure 1.

The trend of bariatric surgery publications growth.
Before 2003, 97 articles were published on average, while the number of literature grew at 8–27% per year from 2004 to 2020. However, the number of publications declined in 2019 and 2020. It may be caused by indexing delays rather than a decline in publications. 14 In addition, the welter of publications on COVID-19 during the same period is also a potential cause. The 21,798 publications can be roughly divided into five research subjects: bariatric surgery intervention, clinical case management, basic research and prognostic study, body contour, and surgical risk study (Figure 2).

The river map of the evolution of bariatric surgery subjects.
Since the 1980s, the basic research, prognosis study, and surgical risk study have gradually increased. However, bariatric surgery intervention has always been a hot topic. The increase in clinical case management may be responsible for the decrease in body contours. The top 10 journals by publication volume are shown in Figure 3.

The top 10 journals in terms of publication.
Obesity Surgery was the highest publication journal. This was consistent with other studies.1,4 Notably, five of the top 10 journals are about plastic surgery.
Co-keyword analysis
Six topics were clustered and the timeline diagram of BMS topic clusters was shown in Figure 4.
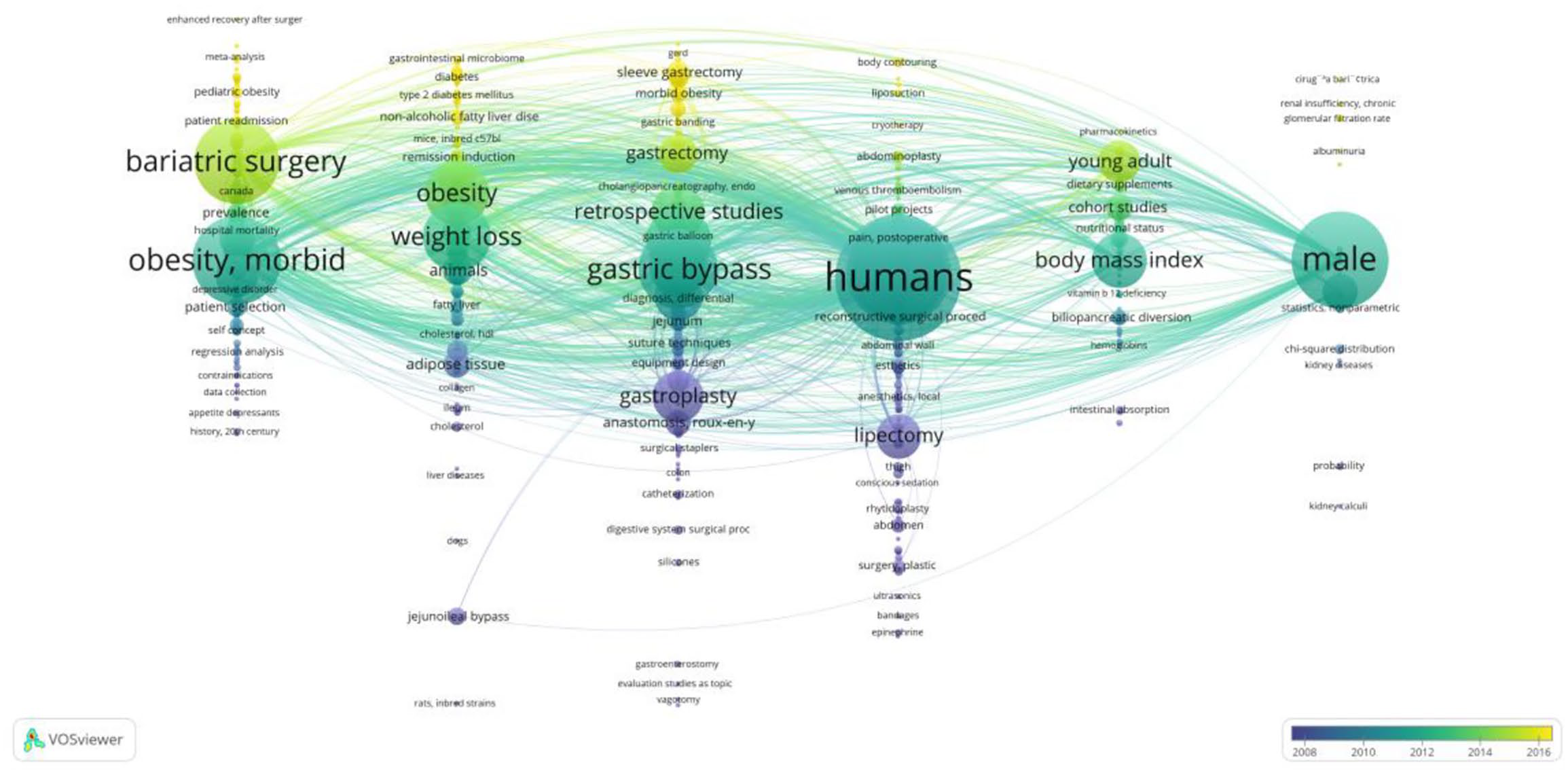
Timeline graph of co-keywords network clustering.
Keywords in each topic were summarized and the main content was shown in Table 1. Topic 1 mainly included morbid obesity, bariatric surgery, enhanced recovery after surgery (ERAS), and so on. It focused on indications, contraindications, and perioperative management of BMS. Topic 2 was mainly related to basic research and obesity-related comorbidities. It reflected the research on the mechanism of BMS. Topic 3 mainly reflected the procedure and techniques of BMS. Topic 4 mainly involved the body contouring after BMS. It showed the important role of plastic surgery after BMS. Topic 5 was mainly related to nutritional status after BMS. Topic 6 mainly reflected the potential relationship between BMS and kidneys.
Main content of topic clustering.

Topic analysis
The topic network analysis by LDA highlighted the cluster of related topics and showed the relationship between the prominent topics. The topic network analysis resulted in five topic network clusters marked by different colors (Figure 5).

Topic cluster network analysis by latent Dirichlet allocation. Purple, bariatric surgery intervention; aqua, clinical case management; blue, basic research; red, body contour; and loden, surgical risk study. The size of each bubble was related to the number of publications. Network lines within and between topic clusters represented weight of connection between the five areas.
The five areas were bariatric surgery intervention (purple), clinical case management (aqua), basic research (blue), body contour (red), and surgical risk study (loden). The size of each bubble was related to the number of publications. Network lines within and between topic clusters represented relationships between the five areas.
In the bariatric surgery intervention cluster (purple area), the main topics of study were surgical experience reports, complications, bariatric procedures, and morbid obesity. The strong relationships between these topics indicated that they were closely related. Again, these topics were well studied in the area. In addition, laparoscopic and endoscopic surgery and tumor have also been gradually concerned. In general, the cluster of bariatric surgery intervention is strongly related to both clusters of basic research and surgical risk study.
In the cluster of clinical case management (aqua area), the main topics were obesity and health intervention, perioperative care and psychosocial intervention, follow-up and influence factor, train, and quality of life. The study of nutritional deficiencies, dietary habits, cost-effectiveness analysis, body composition, and so on is also gradually paid more and more attention after surgery. It is important to note that although the number of publications studying depression was small, there was a strong correlation between quality of life and questionnaire. In addition, the clinical case management cluster was closely related to basic research.
Mechanism research accounted for most publications in the cluster of basic research (blue area). It was noteworthy that mechanism research is closely related to cytokines and hormones, diabetes mellitus, cardiopulmonary function, a gut hormone, and obesity-associated disorders. Gut microbiota, animal experiments, adipose tissue, and genomics are widely used in mechanism studies. In addition, the cluster also contains topics such as gut hormone (GLP-1, ghrelin, cholecystokinin, etc.), nonalcoholic fatty liver disease (NAFLD), and metabolism, suggesting that the cluster is very comprehensive.
Abdominoplasty, redundant skin, plastic surgery, and lipolysis were the main topics of the body contour cluster (red area). There was a strong relationship between these themes. Although there were many publications on the issues of randomized controlled studies and anesthesia, there was a weak association with other topics.
In the surgical risk study (loden), safety and complication rate, Medicare and cost of complications, and risk factors analysis were the most studied topics. The safety and complications of BMS have always been the focus of attention.
Discussion
For the first time, machine learning was used to analyze the literature on BMS. The landscape of BMS was explored by examining the growth of publications and the distribution of research topics and journals. In this study, the research topics of BMS mainly focused on five clusters: bariatric surgery intervention, clinical case management, basic research, body contour, and surgical risk study. Various topics such as treatment outcome, psychosocial intervention, education and training, patient safety, clinical research, and basic research have also been enriched in the development of BMS. BMS is a new subject that still has many problems to be solved. Therefore, this study has important significance for the development of BMS.
According to the number of publications, the development of BMS could be roughly divided into four stages. The first stage was from the 1950s to the mid-1990s. Open bariatric surgery was the main surgical method in this stage. 15 The public poorly accepted BMS. From the mid-1990s to the early 2000s, BMS transitioned from open surgery to laparoscopic surgery.15,16 During this stage, BMS became widely accepted and the number of operations exploded worldwide. In the third stage, from the early 2000s to the mid-2010s, BMS started treating obesity-related metabolic diseases. 17 In addition, surgical safety has been emphasized and improved. The fourth stage is from the mid-2010s to the present. BMS proedures are more diversified, such as robot-assisted surgery, endoscopic surgery, intragastric balloons, and others gradually used in clinical practice.18–20
SNA and LDA results are highly consistent, reflecting the credibility of our research results. Bariatric surgery intervention has always been a controversial topic. Surgical treatment is still improving. Laparoscopic, robotic surgery has completely replaced open surgery. In addition, endoscopic surgery is also becoming popular globally. 21 Currently, adjustable gastric banding (AGB), roux-en-Y gastric bypass (RYGB), and sleeve gastrectomy (SG) are the most common BMS in the world.5,22 Some new surgical procedures are being explored, such as One Anastomosis Gastric Bypass (OAGB) and sleeve Gastrectomy plus duodenal-jejunal bypass (SG + DJB).23,24 However, the indications and benefits of these procedures remain to be validated. Therefore, the new BMS surgical procedures still need to be supported by more clinical research.
Clinical case management plays an increasingly important role in BMS. Good knowledge of disease-specific health is an important prerequisite for patients to lose weight and prevent associated medical problems. 25 Morbid obesity and its related comorbidities such as type 2 diabetes, sleep apnea, and hypertension are common, but few of these patients are currently considered for BMS. 26 Lower level of education and poor health literacy are strongly associated with readmission after BMS. 27 Therefore, health education and obesity intervention are critical in BMS. Cognitive-behavioral therapy can reduce weight regain by reducing risk factors such as disordered eating and depression. 28 Behavioral and psychosocial interventions play an important role in promoting long-term success after BMS. 29 Perioperative care is also an important content of clinical case management. ERAS effectively reduces the length of hospital stay and accelerates patient recovery after BMS. 30 In addition, long-term follow-up is required for pregnancy, quality of life, and nutrition after BMS, which is also the main task of clinical case management.
BMS can alter physiological functions such as adipose tissue, cytokines, gut hormones, and gut microbiota by altering gastrointestinal anatomy. 31 Previous evidence has shown that obesity induces a low-grade chronic inflammation of adipose tissue characterized by infiltration of pro-inflammatory cells, including neutrophils, macrophages, B cells, and natural killer T cells, which play a critical role in insulin resistance and type 2 diabetes. 32 BMS can reduce the degree of inflammation of adipose tissue and improve the metabolic function of adipose cells, which may be one of the mechanisms for the treatment of obesity and its complications. 33 The regulatory role of gut microbiota in BMS has also been gradually popularized. Haange et al. found that after RYGB, the gut microbiota of Actinobacteria, especially Proteobacteria (Pseudomonadota) and Bifidobacteriaceae, was relatively increased, while Firmicutes were decreased. However, another study found an increase in Firmicutes after BMS. 34 Interestingly, BMS does not change the structure and function of gut microbes through weight loss. 35 Therefore, the mechanism of BMS is not completely clear, and with the in-depth study of the mechanism, basic research is still a hot topic in the future.
BMS often leads to excess skin, which can cause physical and psychological impairments. Therefore, body contouring after BMS is becoming more and more important. Postbariatric body contouring surgery (BCS) provides a way to reduce excess loose skin 35 surgically. Toma et al. 36 found that BCS can facilitate the functional and psychosocial consequences of excess skin after BMS and improve patients’ quality of life. With the emphasis on obesity education, BCS may gradually decrease after BMS.
Currently, perioperative mortality and serious adverse events, including bleeding, venous thromboembolism, anastomotic leakage, reoperation, and readmission, are short-term indicators to assess the safety of BMS. In many studies, the risk of serious adverse events within 30 days is generally less than 6%, indicating the safety of BMS in the short term. 26 Reoperation is commonly used to evaluate the long-term safety of BMS. Previous studies have shown that BMS’s reoperation rates range from 5% to 22.1%.26 However, the low completeness of long-term follow-up of BMS may lead to underestimating complications. In addition, there are few studies on 10 years followup following BMS. Cholelithiasis is a common complication after BMS, but the timing of cholecystectomy remains controversial. Morais et al. 37 suggested that asymptomatic patients should not undergo cholecystectomy during BMS. However, another study recommended simultaneous cholecystectomy during BMS. 38 Our results reflect this trend. Therefore, more long-term multicenterstudies on BMS are necessary.
There are some limitations to this study. First, only the PubMed database was selected in this study. The inclusion of other databases, such as Embase, Web of Science, and Scopus, would provide detailed and comprehensive knowledge.39–41 In the future, we will extend the data source. Second, due to the limitation of thesis length, we cannot include all analyses, such as country, author, institution, and citation analysis. Third, MeSH terms related to BMS in this study, such as ‘Gastrectomy’ and ‘Biliopancreatic diversion’, were not used in the retrieval. Some publications related to BMS may not use ‘bariatric surgery’ as a MeSH term. In addition, some publications may not be included in our study due to indexing delays. Finally, only MeSH terms are used in this study and no other search terms are used. This may lead to bias in our study.
In conclusion, for the first time, this study analyzed more than 20,000 publications on BMS through machine learning, which will help scholars in various fields understand the research trends, current situation, and possible future research directions. Although significant progress has been made in BMS, our study has several remarkable findings. First, there are few long-term follow-up studies on BMS. The indications, complications, and safety of BMS still need a lot of clinical research. In addition, there is insufficient emphasis on quality of life and depression. The concern is that while BMS can reduce patient mortality, it may adversely affect mental health and even increase the risk of suicide and self-harm. 42 Second, basic research on BMS is increasing, but the mechanism is still unclear. Advanced technologies such as genomics, proteomics, metabolomics, and radiomics will help uncover the mechanisms of BMS. Finally, our study shows that machine learning such as SNA and LDA can help scientists extract objective and comprehensive clues from large amounts of data.
Footnotes
Acknowledgements
Thanks to scholars in various fields for their contributions to the development of bariatric metabolic surgery.
Authors’ note
The authors have completed the SRQR reporting checklist.