
Abstract
Background:
The aim of our study was to evaluate the frequency and risk factors of clinical postoperative recurrence in Tunisian patients with Crohn’s disease (CD).
Methods:
Clinical data of 86 patients with CD who underwent ileocolonic resection at University Hospital of Sahloul in Tunisia were retrospectively reviewed. Continuous data are expressed as median (interquartile range), and categorical data as frequencies and percentages. Multivariate Cox proportional hazard regression analysis was conducted to identify the risk factors of postoperative clinical recurrence.
Results:
A total of 86 patients with CD were included in this study. During follow-up, 21 patients (24.4%) had clinical recurrence. The cumulative clinical recurrence rate was 9.3% at 1 year and 20.9% at 5 years. In univariate analysis, predictive factors of postoperative clinical recurrence were active preoperative smoking (p = 0.008), ileal location of the disease (p = 0.01), active CD [Crohn’s Disease Activity Index (CDAI) > 150] (p = 0.04), duration of disease before first surgery <9.5 months (p = 0.027), and limited resection margins (<2 cm) from macroscopically diseased bowel (p = 0.005). In multivariate analysis, only smoking (p = 0.012), duration of disease before first surgery <9.5 months (p = 0.048), and limited resection margins (<2 cm) from macroscopically diseased bowel (p = 0.046) were confirmed to be independent factors of clinical relapse.
Conclusion:
Smoking, duration of disease before first surgery <9.5 months, and limited resection margins (<2 cm) from macroscopically diseased bowel were independent risk factors for clinical recurrence. Based on these factors, patients could be stratified in order to guide postoperative therapeutic options.
Introduction
Crohn’s disease (CD) is a chronic inflammatory disease that can affect any part of the gastrointestinal (GI) tract with unpredictable natural course. Its etiology is still not completely understood. 1 Despite the significant advancement in medical treatment, up to 70–80% of patients with CD would require surgical intervention during their lifetime. 2 As surgical treatment is not curative for CD, postoperative recurrence (POR) is very common and remains challenging for clinicians. It can be defined in different ways as clinical, endoscopic, radiological, histological, or surgical recurrence. 3 Endoscopic recurrence precedes the development of clinical symptoms.
Overall, after ileal or ileocolonic resection, 20–30% of patients will experience a symptomatic recurrence rate in the first years after surgery, with 50–60% of reoperation rates. 2
In population-based studies, Buisson et al. 4 found that symptomatic clinical recurrence occurred in approximately half of patients at 10 years. Evidence of endoscopic recurrence is also high, and several studies showed that up to 70% patients will develop endoscopic recurrence within 1 year. 5
Several factors have been identified to predict early recurrence in the majority of studies, 6 including age at onset of disease, family history of CD, smoking, prophylactic medical treatment, length of resected bowel, presence of granuloma, and involvement of disease at the resection margin.7–9
Identifying the risk factors for CD recurrence is consequently very important in order to select patients at high risk of recurrence and to provide optimal treatment strategy, as multiple surgical resections can lead to short-bowel syndrome.
In Tunisia, there are few published data on factors associated with postoperative clinical recurrence. 10 Determining the risk factors that can be applied to the patients in our country is fundamental, in order to identify patients who may need optimized postoperative management.
Hence, the purpose of our study was to evaluate the rate of clinical POR in CD and to assess the predictive factors of its recurrence after ‘curative’ surgical resection.
Materials and methods
Patients
All data from patients diagnosed with CD who underwent first surgical resection between January 2006 and January 2016 at the University Hospital of Sahloul, Sousse, Tunisia, were retrospectively reviewed. A retrospective chart review was performed on all patients, including general demographic information and perioperative clinical characteristics particularly patient’s age, sex, age at presentation, family history, cigarette smoking, chief complaint, disease duration and location, perianal disease, disease behavior, type of medication before surgery, and indication for surgery.
Only patients who had pathological confirmation of CD, obtained by surgical specimen or endoscopic biopsy, were included in this study.
Patients with the following criteria were excluded: patients with CD who underwent surgery involving other segment of the GI tract than the ileum, patients who had no histological evidence of CD, follow-up period less than 1 year after intestinal resection, and patients with incomplete clinical information.
Definitions
Clinical recurrence was defined as the reappearance of CD-related clinical signs, which confirms recurrence of new lesions or the occurrence of complications such as abdominal abscess, fistula formation, or intestinal obstruction, 11 after complete surgical resection of all macroscopic lesions. Disease activity was quantified by using the Crohn’s Disease Activity Index (CDAI).
Endoscopic recurrence is commonly defined as a Rutgeerts score ⩾ i2. It is usually assessed 6–12 months after index surgery (Table 1).
Rutgeerts scoring system.

Statistical analysis
After data collection, statistical analysis was performed by SPSS® 19.0 software. Descriptive statistics were used to generate frequencies and percentages for categorical variables, and mean with standard deviations for continuous variables. Continuous variables were compared using independent-samples t test, and categorical variables were compared using the chi-square test.
To estimate the impact of the clinical variables above on the cumulative rate of postoperative clinical recurrence, we applied Kaplan–Meier method. Multivariate Cox proportional hazard regression analysis was conducted to evaluate the risk factors associated with postoperative clinical recurrence. All variables with a p value <0.05 were considered statistically significant. Statistical review of the study was performed by a biomedical statistician.
Results
Baseline characteristics
A total of 86 patients with CD, who underwent ileocecectomy or right hemicolectomy, were included in the study. There were 60 men and 26 women (gender ratio: M/F = 2.3). The average age at diagnosis was 32.95 years (range: 16–69 years). At diagnosis, 40 patients (46.5%) were current smokers.
According to the Montreal classification, most patients had disease located in terminal ileum (L1, subtype, 55/64%) and structuring behavior of the disease (B2, 47/54.6%). Perianal lesions were present in 22 patients (34.4%) at diagnosis. Demographic and clinical features of CD cases are summarized in Table 2.
Baseline demographic and clinical characteristics of the patients.

TNF, tumor necrosis factor.
As to the preoperative use of medication, 48 patients (56.5%) were receiving steroids, 59 cases (68.6%) azathioprine, and 2 cases (2.3%) were using anti-TNF agents.
Surgical treatment
The most frequent indications for intestinal resection were intestinal stricture or obstruction in 54 patients (69.3%), followed by intra-abdominal abscess unresponsive to medical treatment in seven patients (10.2%), intestinal fistula in three patients (4.2%), and perforation in four patients (5.8%). Surgical procedures consisted of small bowel resection in 55 patients (64%) and ileocecectomy in 31 patients (36%). The average length of the small bowel resected was 13.2 cm (8–105 cm). The histological examination of the surgical specimen revealed the presence of epithelioid granulomas in 27 cases (30.7%), of myenteric nerve hyperplasia in 18 cases (20.7%), and of both lesions in 11 cases (12.5%).
Clinical recurrence
All patients were followed up clinically with a median follow-up time of 18.4 (12–67) months.
During this period, clinical recurrence occurred in 21 patients (24.4%) with a cumulative rate of 9.3% at 1 year and 20.9% at 5 years after intestinal resection. The interval between the operation and recurrence was 34.6 (8.0–116) months.
After surgery, 47 patients (54.7%) received azathioprine at a dose of 2–2.5 mg/kg/day, 19 patients (22.1%) received 5 aminosalicylates (5 ASA), and 2 patients (2.3%) received anti-TNF agents.
Of the 21 patients with clinical recurrence, 13 underwent a postoperative endoscopy, and of those 12 showed a Rutgeerts score of grade 2 or higher. The localization of the disease was in the ileocolic anastomosis in all cases. Right colonic involvement was found in only one patient.
Overall, 38.1% (8/21) of the patients with symptomatic recurrence underwent surgery. The other patients received medical treatment.
Factors associated with clinical recurrence
In univariate logistic regression analysis, five factors were significantly correlated with clinical recurrence: tobacco consumption (p = 0.008), ileal location of the disease (p = 0.001), active CD (CDAI > 150; p = 0.004), duration of disease before first surgery <9.5 months (p = 0.027), and limited resection margins (<2 cm) from macroscopically diseased bowel (p = 0.005). In multivariate analysis, smoking – odds ratio (OR) = 28, 95% confidence interval (CI) = [6.46–121.30], p = 0,012; duration of disease before first surgery <9.5 months – OR = 26.27, 95% CI = [2.85–241.87], p = 0.048; and limited resection margins (<2 cm) from macroscopically diseased bowel – OR = 0.09, 95% CI = [0.013–0.719], p = 0.046, were independent prognostic factors for clinical recurrence. No impact of age at diagnosis, sex, or disease behavior was found. Results of univariate and multivariate analyses were shown in Tables 3 and 4.
Predictive factors of recurrence in univariate analysis.
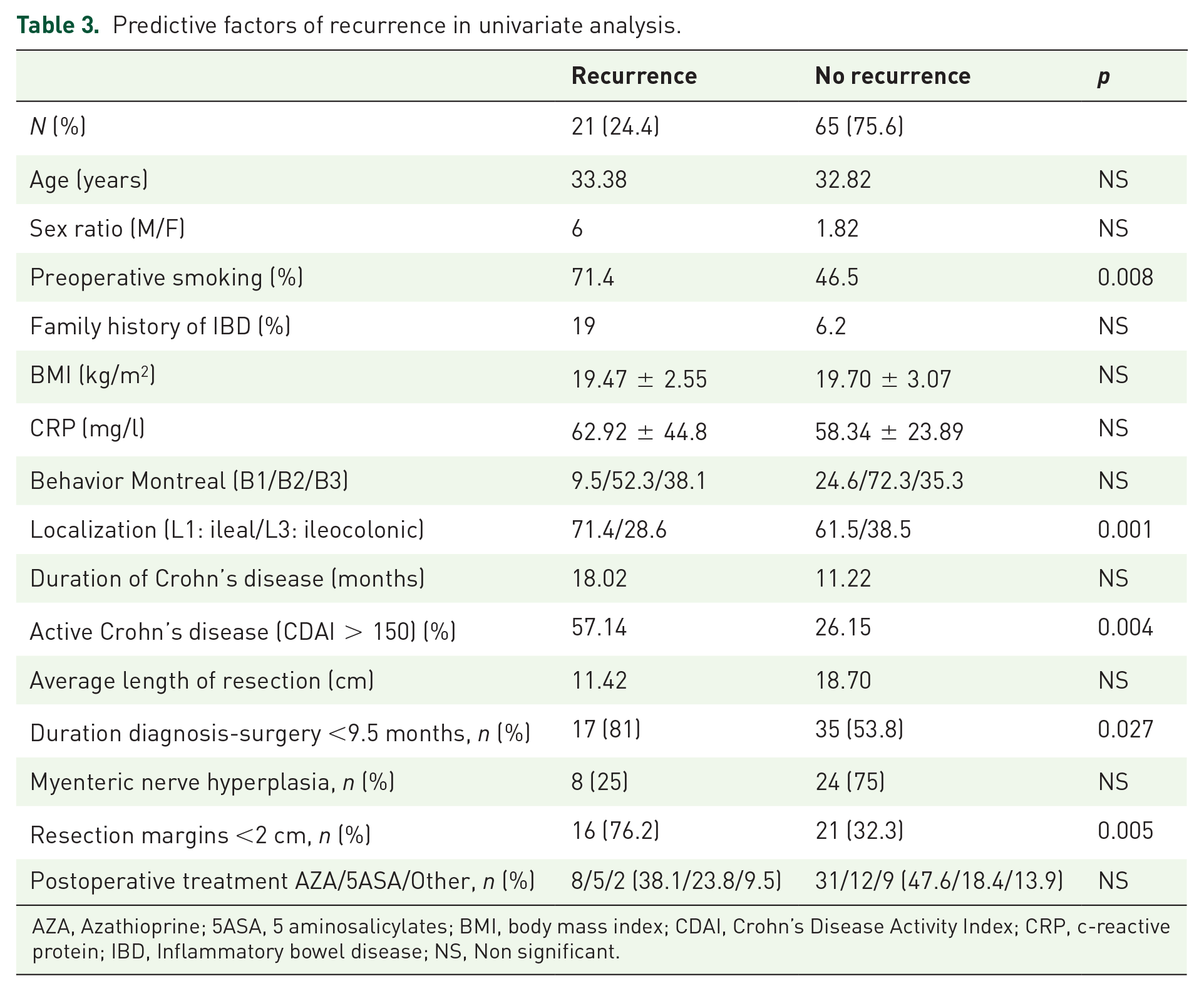
AZA, Azathioprine; 5ASA, 5 aminosalicylates; BMI, body mass index; CDAI, Crohn’s Disease Activity Index; CRP, c-reactive protein; IBD, Inflammatory bowel disease; NS, Non significant.
Predictive factors of recurrence in multivariate analysis.

CDAI, Crohn’s Disease Activity Index; CI, confidence interval; OR, odds ratio.
Predictive factors for endoscopic recurrence could not be analyzed because of the small sample size.
Discussion
CD is a lifelong, progressive, and disabling inflammatory bowel disease with poorly defined etiology and pathogenesis. 12 Despite the increasing use of immunosuppressants and biotherapies, the natural course of CD does not appear to change since almost half of patients will require bowel resection within 10 years of diagnosis of the disease. 13 However, surgery is not curative for CD as recurrence is very common and more than 50% of patients undergo reoperation in a 10-year postoperative period. 14 Therefore, postoperative management focuses on preventing POR and bowel preservation which remains a major challenge for clinicians.
In the literature, the recurrence rates vary widely depending on the modality used for diagnosis: clinical, endoscopic, radiological, or surgical. The highest rates were found when endoscopy is employed as the diagnostic tool for recurrence. 15 Currently, endoscopy is considered the gold standard in the diagnosis of postsurgical recurrence and is recommended during the first year after surgery. 16 Endoscopic recurrence, defined using the Rutgeerts’ score, occurs preferentially in the neoterminal ileum, almost always perianastomotic, in 30–90% of patients within 12 months of surgery. Clinical recurrence is defined as the recurrence of CD-related symptoms, including diarrhea, weight loss, and abdominal pain. It occurs in 20–40% of patients within 12 months of surgery and 35–50% of patients by 5 years.3,4,9,17
Mucosal lesions visualized at endoscopy may occur within few weeks of bowel resection,3,11 which makes it possible to predict evolution to symptomatic clinical relapse. 18
In our study, the cumulative clinical recurrence rate was 9.3% at 1 year and 20.9% at 5 years. Our results were all relatively lower than those previously reported in the literature.
Endoscopic recurrence was noticed in 24.4% of our patients after a mean follow-up period of 34.6 months. However, predictive factors for endoscopic recurrence could not be studied because of the small sample size.
Identifying predictors of POR is of critical importance as it helps select patients who might benefit from prophylactic treatment. Many prognostic factors have been investigated. The following are considered predictors of early POR after ileocolonic resection according to the European Crohn’s and Colitis Organisation (ECCO) consensus: smoking, prior intestinal surgery, absence of prophylactic treatment, penetrating disease at index surgery, perianal location, granulomas in resection specimen, and myenteric plexitis. 15
Several other risk factors for POR were discussed over the past decades,19–21 such as age at onset, 22 sex, 22 family history of CD, duration of disease progression, 23 perforating type, resection margins, 24 and type of surgery. 3 In addition, lack of prophylactic medical treatment is associated with a high risk of recurrence.25,26
In our study, three factors were correlated with clinical recurrence: smoking – OR = 28.00, 95% CI = [6.46–121.30]; diagnosis-surgery delay <9.5 months – OR = 26.27, 95% CI = [2.85–241.87]; and limited resection margins (<2 cm) from macroscopically diseased bowel – OR = 0.09, 95% CI = [0.013–0.719]. None of the other factors was associated with an increased risk for repeat surgery in the present analysis.
Cigarette smoking is the most recognized and the only modifiable risk factor for POR. 27 The impact of active smoking behavior is well established. Several studies have examined the role of active smoking in increasing the risk of CD relapse after surgery. Kane et al. 27 reported that 68% of CD patients had documented clinical recurrence versus 23% of non-smokers, with an OR of 2.96 in the smoking cohort. A meta-analysis including 538 patients that presented CD flares after surgery showed an OR of 1.97, 95% CI = [1.36–2.85] in active smokers compared with non-smokers. 28 Therefore, smoking cessation should be strongly recommended after surgery. A powerful association between duration of disease before surgery and early recurrence has been suggested, and several studies have reported a risk of recurrence inversely proportional to the time between the onset of CD and surgery.28,29 This may be suggestive of more aggressive disease phenotype. However, the definition of ‘short duration’ is still controversial and hampers comparison among the studies. Poggioli et al. 30 found higher recurrence rates in patients with a duration of disease less than 6 years before surgery in comparison with those who had a duration longer than 6 years. Likewise, Chardavoyne et al. 29 reported a significantly higher recurrence rates for duration of CD between 3 and 10 years. These data contrasted with those from more recent studies supporting early surgery, particularly in stenosing ileocecal CD, which appears to be associated with prolonged clinical remission. 31 In our study, duration of disease less than 9.5 months prior to surgery was significantly associated to POR.
Another risk factor of CD relapse after surgical resection is the involvement of the disease at the line of resection. The impact of resection margins on the recurrence of CD has been investigated by several studies. 32 It has long been considered that trying to resect microscopically involved bowel and to gain disease-free margins was fundamental for reducing POR rate. 33 Several studies have reported that the resection of microscopically uninvolved bowel (radical resection) was associated with a lower recurrence rate than non-radical resection.29,33 Our study supported these findings as we found that limited resection margins (<2 cm) from macroscopically diseased bowel were significantly associated to POR of CD. Nonetheless, several studies have shown that extensive resection margins are unnecessary as there was no difference seen in the recurrence rates between patients with radical resection and non-radical resection. 34
As recurrence typically begins at the site of the anastomosis, the question of whether the type of surgical anastomosis could affect recurrence rates has been widely studied, but still controversial. Interestingly, some studies suggested that side-to-side anastomosis was associated to lower incidence of symptomatic recurrence and reoperations compared with end-to-end anastomosis,35,36 while others claim that no differences exist. This may be explained by the fact that end-to-end anastomosis is a narrow anastomosis that leads to fecal stasis and bacterial overgrowth, resulting in early disease recurrence. 37 In recent years, a new antimesenteric, functional, end-to-end, handsewn ileocolic anastomosis (Kono-S) has been described. 38 This technique resulting in a large diameter has significantly reduced postoperative endoscopic recurrence rate compared with side-to-side anastomosis (22.2% versus 62.8%, p < 0.001, OR = 5.91) and decreased the severity of endoscopic recurrence score (13.8% versus 34.8%, P = 0.03, OR = 3.32). 38
Postoperative medication is also well known to be an important predictor for recurrence of CD. If postoperative prophylaxis with mesalazine did not show a significant benefit on preventing POR, 39 purine analogues (6-mercaptopurine/azathioprine) were found independently associated with reduction in surgical rate. Interestingly, the efficacy of anti-TNF agents in preventing clinical and endoscopic recurrence has been reported by several studies.40,41 Their superiority over purine analogues has been documented by two meta-analyses. In our study, the use of postoperative medication was not significantly associated to lower clinical recurrence rates after bowel resection.
In conclusion, this retrospective study of CD in Tunisian patients revealed that smoking, duration of disease before first surgery <9.5 months, and limited resection margins (<2 cm) from macroscopically diseased bowel were independent risk factors for clinical recurrence. The principal limitation to our study is related to its retrospective design limiting our ability to show associations and to have standardized follow-up protocol for the patients after their primary bowel resection. The study size limited our ability to explore predictive factors for endoscopic recurrence in our population.
Footnotes
Acknowledgements
All authors of the manuscript titled ‘Predictors of post-operative recurrence in Tunisian patients with Crohn’s disease’ certify that they qualify for authorship because of substantial contribution to the work submitted. The authors undersigned declare that this manuscript has not been published nor is under simultaneous consideration for publication elsewhere. The final form of the manuscript has been seen and approved by all authors.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local ethics committee of the University Hospital of Sahloul, Sousse, Tunisia.
Informed consent
Informed consent was waived due to the retrospective nature of this study.