
Abstract
Obesity remains a growing public health epidemic that has increased healthcare costs and related comorbidities. Current treatment guidelines encourage a multidisciplinary approach starting from patient selection, interventions, and long-term follow-up to maintain weight loss. However, these conservative interventions are largely ineffective at reducing body weight due to low adherence to the treatment regimen. Recently, endoscopic bariatric therapies have become an attractive alternative to traditional invasive bariatric surgeries due to their improved efficacy, safety, and cost-effectiveness. Endoscopic bariatric therapies include intragastric balloon placement, endoscopic sleeve gastroplasty, gastric bypass revision, and aspiration therapy. These procedures fall into two separate categories depending on the primary mechanism involved: restrictive or malabsorptive. Restrictive methods, such as the Orbera® and ReShape™ intragastric balloons, increase satiation and delay gastric emptying while decreasing the amount of food that can be ingested. In contrast, malabsorptive devices, such as the EndoBarrier®, interfere with the small intestine’s ability to absorb food while restoring normal gastrointestinal hormone levels regulating satiation. Together, these techniques provide useful alternatives for patients in whom pharmacological or lifestyle modifications have proven ineffective. Despite these advantages, the long-term effects of these procedures on metabolic changes remain to be studied. Furthermore, the management of complications from these procedures continues to evolve. In this review, we aim to elaborate on the clinical indications and efficacy of the endobariatric procedures, together with various types of available endoscopic bariatric therapy procedures.
Introduction
Obesity is a significant public health epidemic with an increasing number of related complications with rising healthcare costs.1–3 The prevalence of obesity has doubled since the 1980s, with the World Health Organization (WHO) 2014 estimates of 600 million obese adults. 1 Studies have shown that bariatric surgery improves obesity-related complications along with the improved quality of life.4–6 Previous methods for controlling obesity and insulin resistance used a combination of pharmacological and lifestyle changes7,8; however, a meta-analysis of these interventions showed limited efficacy in reducing body weight and adherence to the treatment regimen.7–10 Although the precise mechanisms of the effects of conservative approaches for weight loss remain unclear, it could be due to the compensatory increase in ghrelin in response to dietary manipulation. Bariatric surgeries have shown a more robust response in achieving a higher total body weight (TBW) loss and addressing metabolic dysfunction.7–10 Recent developments using endoscopic bariatric therapies (EBTs) have proven safer, cost-effective, and reversible alternative to traditional surgical bariatric procedural methods.1,11,12
Bariatric surgeries are of several types, such as Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, adjustable gastric band, vertical banded gastroplasty (VBG), duodenal switch, and biliopancreatic diversion (BPD). 1 First developed in the 1980s, EBTs include both gastric and small bowel interventions. 1 Gastric intervention stimulates mechanical receptors mostly in the gastric fundus to delay gastric emptying and modify orexigenic hormones, including ghrelin and neuropeptide-Y (NPY).13,14 In contrast, small bowel interventions bypass the stomach to influence satiety and gastrointestinal (GI) motility.13,14 Currently, EBTs include the following endoluminal procedures: intragastric balloon (IGB) placement, endoscopic sleeve gastroplasty (ESG), gastric bypass revision, and aspiration therapy, and so on. 15 These procedures fall into two separate categories depending on the primary mechanism of action involved: restrictive or malabsorptive (Table 1). Both restrictive and malabsorptive methods improve weight loss by altering gastric function, GI hormones, and GI motility.1,7 Restrictive methods, such as the Orbera® and ReShape™ IGBs, increase satiety and delay gastric emptying while decreasing the amount of food that is ingested. 15 In contrast, malabsorptive devices, such as the EndoBarrier®, interfere with the small intestine’s ability to absorb food while restoring normal GI hormone levels regulating satiety. Together, EBTs have provided a useful alternative for patients in whom pharmacological or lifestyle modifications have proven ineffective. 7
Restrictive and Malabsorptive EBT Procedures.

EBT, endoscopic bariatric therapies.
Furthermore, EBTs also improve obesity-related comorbidities, including type 2 diabetes (DM-2), dyslipidemia, and nonalcoholic fatty liver disease (NAFLD). 17 Due to these benefits, endoscopic weight loss therapies are considered another alternative for weight loss because of their lower risk profile, increasing availability, minimal anatomic alteration, and potential of reversibility compared with surgical bariatric procedures. 7 In addition, EBTs have also positively impacted the quality of life and the patients’ psychological aspects. 18 Although bariatric surgical techniques have improved over time, strict preoperative surgical/anesthesia criteria and postoperative complications limit the use of bariatric surgeries.1,19,20 A longitudinal assessment of these procedures found that patient characteristics and past medical history can significantly influence surgical outcomes and complications. 20 Despite all the advances, bariatric surgeries’ adverse event rate remains as high as 17%. 21 Due to these factors, minimally invasive surgical procedures are being actively sought. We explored PubMed, Google Scholar, Embase, Ovid MEDLINE, CINAHL (via ESBSCOhost) databases for articles published in English languages up to July 15, 2020. The following search formula was used with words: ‘Gastroplasty’ or ‘Overstitch’ or ‘Endosleeve’ or ‘Endoscopic sleeve gastroplasty’ or ‘Endoscopic bariatric therapy’ or ‘Endoscopic suturing’ or ‘Bariatric endoscopy’ or ‘Endobariatrics’) AND (‘Weight loss’ or ‘Obesity’ or ‘Bariatric’) AND (‘Endoscopic’). In this article, we will review the indications for different EBTs along with their potential complications. In addition, we will also examine the putative mechanisms of actions and future directions for EBTs.
Molecular mechanisms of endobariatric therapies
The exact mechanism of EBTs remains poorly understood and a subject of controversy. However, it is believed that alterations and reorganization of the GI tract and microbiome may restore homeostatic mechanisms in weight loss, caloric intake, and glycemic control. 22 Similar to previous bariatric surgeries, EBTs increase TBW loss and improve metabolic profile (low-density lipoprotein cholesterol, blood glucose, triglyceride, and blood pressure) in obese patients.14,16 Multiple changes including a decrease in levels of ghrelin, increased insulin sensitivity, and delayed gastric emptying have also been noted.14,23 Ghrelin is a hormone secreted by the stomach, small intestine, pancreas, and brain. Its primary function is to stimulate appetite, increase food intake, and promote fat storage. Hence, reducing the levels of ghrelin might induce weight loss.7–10 In addition, an increase in small intestinal hormones, including glucagon-like peptide 1 (GLP-1), peptide YY (PYY), and oxyntomodulin, was noted. 14 Many obese patients have dysbiosis with significant alterations in the gut microbiota. 14 This dysbiosis negatively impacts the interaction of microbiota, immune system, and host defenses required for protecting and maintaining the normal gut-liver homeostasis. 14 Examination of gut microbiota in clinical and in vivo studies shows a decrease in the ratio of Firmicutes/Bacteroidaceae bacteria after EBTs. The increase in Bacteroides leads to accelerated enzymatic conversion of primary to secondary bile acids, which increased the release of gastric inhibitor peptide and GLP-1 1. 14 Furthermore, EBTs bypass the foregut and accelerate intestinal transit time leading to an increase in secondary bile acids in the distal gut. 14 The increase in secondary bile acids induces the secretion of incretins, which increases insulin levels while reducing blood glucose levels. 14 Therefore, reducing obesity through the above mechanisms and lifestyle modification would reverse the dysbiosis to achieve homeostasis. 14
Costamagna and colleagues conducted a study to assess the role of jejunum in insulin resistance in humans and animals. In humans, 24 subjects with obesity and insulin resistance but normal glucose tolerance undergoing BPD (n = 12) or RYGB (n = 12) were included. In the animal study, four pigs were included; their jejunum was excluded from intestinal continuity and attached its proximal and distal ends to the skin, thus creating a jejunal loop with intact vascular and nerve supply; the remaining bowel was reconnected with an end-to-end anastomosis. The patient underwent an oral glucose tolerance test in the human study before and 1 week after BPD or RYGB. In the animal study, glucose stable isotope was either given in the stomach or the jejunal loop. It showed that whole-body insulin sensitivity (SI.104) increased from 0.54 ± 0.12 to 0.82 ± 0.11 one week after BPD, p = 0.024. Similarly, SI.104 improved from 0.41 ± 0.09 to 0.65 ± 0.09 one week after RYGB, but it was statistically significant. In the animal model, insulin sensitivity was significantly higher when glucose was injected into the stomach than in the jejunal loop (3.25 ± 0.50 vs 1.10 ± 0.32/pM/min, p = 0.0062). It also showed that stimulation of myoblast with plasma from subjects undergoing BPD and pigs during gastric load after jejunectomy increased Ser473-Akt phosphorylation and GLUT 4 expression compared with subjects undergoing RYGB and pig’s jejunal loop. These results showed that jejunum plays a vital role in insulin sensitivity, and BPD may be superior to RYGB regarding improving glycemic control. 24
A summary of the molecular mechanisms is shown in Figure 1.

Mechanisms of Weight Loss After Endoscopic Bariatric Therapy (EBT).
Society guidelines
Although no formal guidelines exist for EBTs in the United States, the American Society for Gastrointestinal Endoscopy (ASGE) has published preliminary recommendations for the use of EBTs in patients with obesity (Table 2). EBTs have been noted to be superior to lifestyle interventions and pharmacotherapy alone, with reduced adverse events in randomized controlled trials (RCTs). 25 EBTs are primarily recommended for patients who have failed non-surgical weight loss or weight maintenance with lifestyle intervention alone and have medical conditions requiring weight loss for additional benefits. Accredited hands-on training programs possibly with formal teaching should be developed in conjunction with GI societies that are focused on the understanding of the management of patients with obesity, establish procedural competency, formal credentialing, and device-specific knowledge.26–28
ASGE Endoscopic Bariatric Surgery Guideline Summary. 25
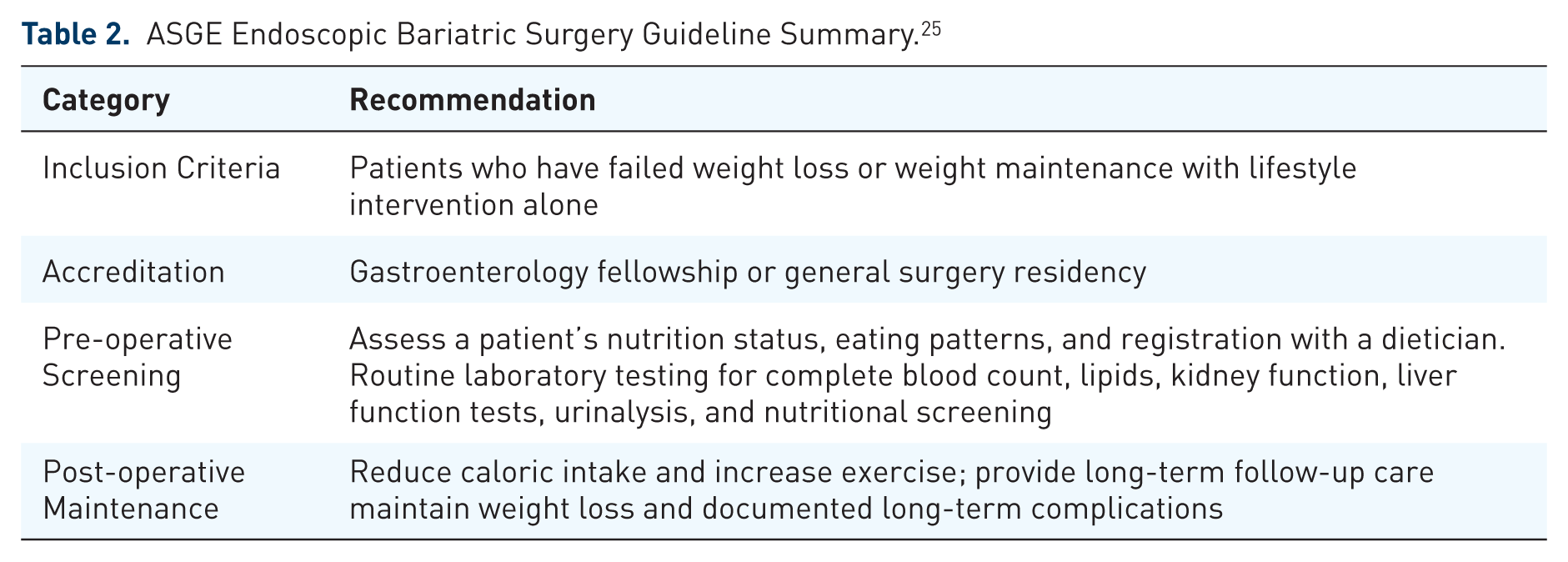
Routine laboratory testing of complete blood count, fasting blood glucose, lipids, kidney function, liver function tests, urinalysis, prothrombin time/international normalized ratio, and nutritional screening (25-hydroxy vitamin D, iron levels, vitamin B12, and folic acid) should be analyzed before consideration for endobariatric procedures. Patients should be evaluated for medical history, physical examination, screening for obesity-related diseases, and lifestyle changes. Further assessment of a patient’s nutrition status, eating patterns, and registration with a dietician is recommended before surgery. Calorie restriction and exercise are an essential step in patients undergoing bariatric interventions. For example, after RYGB, caloric intake should be reduced to 500 to 970 kcal/day in the first 3 months, with a gradual increase to 870 to 1420 kcal/day at 1 year.26–28 Patients are also encouraged to perform 150 min and 200–300 min per week of moderate-intensity exercise to lose weight or maintain weight, respectively. This exercise regime should be complemented with behavior modification, such as slowing the rate of eating, social support, cogni-tive restructuring, and relapse prevention. Post-operatively, patients should be enrolled for long-term follow-up care to determine the extent and maintenance of weight loss and document any long-term complications. Further research and long-term studies in the United States and abroad are needed to establish therapeutic guidelines.
Types of endobariatric procedures
EBTs are mainly categorized into two categories: restrictive or malabsorptive procedures for patients with a body mass index (BMI), mainly between 30 and 45 kg/m2.
Restrictive EBT procedures
In restrictive EBTs, a balloon filled with methylene blue-saline solution or inert gas is placed to fill the stomach to induce early satiety by reducing the available gastric lumen size. One of the first restrictive EBTs was IGB placements. In 1989, the first IGB EBT was developed in the United States, known as the Garren Edwards Gastric Bubble (GEGB). GEGB was initially Food and Drug Administration (FDA) approved in 1985 but was later pulled from the market in 1992 after 7 years because of issues with spontaneous deflation of the bubble needing surgical removal.1,29–31 Moreover, studies showed that GEGB did not have any added benefit compared with sham insertion combined with a standard weight loss program. Therefore, it was taken off the market in 1988.29,31 Later, more effective and safer IGBs, such as the Orbera, ReShape, and Obalon®, were developed and launched.1,29,32–34 Orbera is one of the most effective types of EBTs for TBW loss and associated with fewer adverse events based on clinical studies.32,35,36 Table 3(a) shows different IGBs, and Table 3(b) shows other restrictive EBT studies.
Types of Intragastric Balloons and Their Respective Individual Outcomes.

BMI, body mass index; EWL, excess weight loss; TWL, total weight loss.
The data presented in this table are for representation purposes only. This table, in no manner, depicts the comparison between these devices.
Restrictive Endoscopic Bariatric Therapy (EBT) Studies.

BMI, body mass index; EWL, excess weight loss; TWL, total weight loss.
The data presented in this table are for representation purposes only. This table, in no manner, depicts the comparison between these devices.
Orbera and ReShape
The Orbera IGB (Apollo Endosurgery, Inc., Austin, TX, USA) is a silicone balloon that is endoscopically placed in the gastric fundus, approved by the FDA in 2015. Patients who received Orbera showed a 47% delay in gastric emptying and a 32.1% decrease in excess body weight 6 months after implantation. 50 These balloons are temporary, placed for 6 months, and can be replaced later. The attained weight loss was corresponding to the extent of gastroparesis achieved that, in turn, varied with the volume of the balloon. 51 After 36 months with Orbera, patients had a long-term weight loss of 6%.50,52 A subsequent study in the United States showed a similar reduction in TBW (10.54%) than the control group. 53 The Orbera is relatively safe, with nausea and vomiting as the most common adverse events. Serious events such as bowel obstruction (0.8%) and gastric perforation (0.1%) are rare. 36
A subsequent modification to the Orbera, known as the ReShape IGB (Apollo Endosurgery, Inc.), used two silicone balloons connected with a flexible tube placed endoscopically into the stomach. The initial studies on ReShape showed that patients had a 31.8% increase in excess weight loss (EWL) compared with patients on a behavioral modification program. 53 A larger US study examining 326 patients showed that ReShape had a 25.1% increase in EWL than the control group. 38 FDA has advised for adequate training and close monitoring after Orbera placement.54–56 ReShape balloon is currently not available after its withdrawal from the market.
Spatz®
The Spatz® IGB (Spatz Medical, Great Neck, NY, USA) uses a silicone balloon that is endoscopically inserted and inflated using saline, which can be adjusted to reduce adverse side effects and increase weight loss. 14 This device has not received FDA approval yet. The adjustment also allows the balloon to remain safely inserted in the stomach for a year. 14 Although not approved in the United States, recent studies using the newer version (Spatz3®) IGB showed 26.4% and 38.8% EWL 6 and 12 months after being inserted into the stomach. 39 However, 39% of patients who had the Spatz® balloon removed early developed catheter shear, perforating gastric ulcer, deflation, gastritis, and Mallory-Weiss tears. 39 Another study from the United Kingdom showed that the Spatz3® increased EWL to 45.7% compared with the control. 57 However, nearly 30% of the patients had the Spatz3® IGB inserted for less than 12 months due to intolerance, adjustment refusal, and premature satisfaction. 57
Heliosphere® Bag
Heliosphere Bag is an air-filled double-bag polymer balloon covered with a silicone envelope. It is lighter than a fluid-filled balloon with a weight of approximately 30 g.58,59 In a prospective study of 17 patients with a mean BMI of 46 ± 8 kg/m2 who had endoscopic guided intragastric air-filled balloon placement, patients had achieved a weight loss of 11 ± 9 kg (p = 0.02) and 4 ± 3 kg/m2 (p < 0.01) decrease in BMI from initial weight and BMI. Balloons were removed after 6 months. Balloon removal was more difficult but successful in 15 of 17 patients. One patient required surgery due to balloon fragmentation, and others had distal migration of the balloon. 59 Another study of 82 patients with a mean BMI of 39.1 kg/m2 who underwent placement of heliosphere bag for 6 months showed a mean weight loss of 14.5 kg and a BMI decrease of 5.3 kg/m2. Two patients had spontaneous deflation, with one needing early surgical removal. 40 This device is not FDA approved yet.
End-Ball® (Endalis)
End-Ball (Endalis) IGB is a saline/air-filled spherical elastic balloon made of polyurethane. It allows for various proportions of air and saline. It is not FDA approved. However, it is the most common IGB used in Korea.43,60 A retrospective study of 114 with BMI 33.5 kg/m2 who underwent End-Ball IGB placement showed a 5.5–6.4 reduction in BMI at the time of balloon removal and 4.1 reductions at 1 year after balloon removal. Out of 114, 12 patients had early balloon removal due to intolerance, dissatisfaction, and esophagitis. No serious adverse events were reported. 61 Similarly, another study by Buzga and colleagues showed a significant decrease in body weight (13.9 ± 5.1 kg), glycated hemoglobin (p < 0.001), and triglycerides (p < 0.001). Early abdominal pain, nausea, and vomiting were reported after IGB insertion, which resolved spontaneously in a few days. No serious adverse events were reported. 43
Other IGBs such as MedSil®, LexBal, Medicone®, Semistationary antral balloon, Silimed, and ATIIP (EndogAst®) are also endoscopically implanted. These are not FDA approved. 60
TransPyloric Shuttle®
Previous IGB models had balloons placed in the fundus of the stomach. A recently developed device, which is known as the TransPyloric Shuttle (TPS®) (BAROnova Inc., Goleta, CA, USA), used to have the balloon placed at the transpyloric position between the stomach and duodenum, which was approved by the FDA in 2019.14,62 The TPS consists of a spherical silicone attached to a smaller silicone bulb. 14 The device is inserted with a smaller and larger bulb placed in the duodenum and stomach, respectively, to work as a ‘ball-valve’. 14 The pilot study using the TPS in 20 patients showed an increase in an EWL of 31.3% and 50.0% at 3 and 6 months, respectively. 14 A clinical trial (ENDOBESITY II trial) is currently being conducted in the United States to determine the efficacy and safety of the TPS in a larger sample size (ClinicalTrials.gov Identifier: NCT02518685).
Incisionless anastomosis system
In recent years, other types of EBTs have been developed, including the incisionless anastomosis system (IAM), through which an endoscope is passed, and specialized instruments create full-thickness serosa to serosa plications. 14 However, the IAM is currently not approved by the FDA. 63 The technique is used to perform a procedure known as the Primary Obesity Surgery Endoluminal (POSE) (USGI Medical, San Clemente, CA, USA) procedure. This procedure brings the gastric fundus down to the gastroesophageal junction by placing 8–9 plications in the gastric fundus. Afterward, 3–4 plications are placed in the distal body. 14 This device tabularizes the stomach and hence accelerates gastric emptying. The first report of IAM-POSE in 45 patients showed an increased EWL by 49.4% over 6 months. 64 None of the patients reported serious adverse events. 64 A US clinical trial (ESSENTIAL trial) found the EWL in IAM-POSE was higher (4.95%) than the sham treatment group (1.38%) over 12 months. 47
AspireAssist®
A recent development in the EBTs included introducing a percutaneous gastrostomy tube pump known as the AspireAssist (Aspire Bariatrics, King of Prussia, PA, USA). The device removes part of an ingested meal through an external skin port 20–30 min after consumption. Initial studies found that the AspireAssist showed a 49.0% increase in EWL compared with the controls. 47 The FDA approved the AspireAssist in 2016 for a BMI of 45.63,65 A similar study in the United States (Pathway trial) showed a comparable reduction in excess body weight reduction in patients with the AspireAssist. 66 It is a long-term device and is kept for about 1 year unless desired by the patient to maintain it for the long term. The long-term complications of AspireAssist are nausea or vomiting.
Botulinum toxin A
Recent reports have suggested that Botulinum toxin A (BTX-A) can help lose weight by delaying gastric emptying. BTX-A is a selective acetylcholine inhibitor that blocks smooth and striated muscles across the GI tract. It is believed that BTX-A may improve weight loss by delaying gastric emptying and inducing satiety through inhibition of vagal-mediated intestinal contractions. 14 Despite some initial success, a meta-analysis of eight studies using BTX-A for weight loss was inconclusive on whether BTX-A increased weight loss. Further research and investigation are needed to determine the efficacy and safety of BTX-A compared with current restrictive EBTs.
ESG
Similar to the first IGBs, the VBG had a high failure rate with long-term complications. 48 The VBG was subsequently replaced by the EndoCinch endoluminal vertical gastroplasty (EVG) (C.R. Bard Inc., Murray Hill, NJ, USA) and the TransOral GAstroplasty (TOGA®) system (Satiety Inc., Palo Alto, CA, USA). The FDA approved this device in 2015 for tissue opposition, but the ESG by this device is still not approved by the FDA because of the lack of sufficient trials.63,67
In a multicenter prospective single-arm trial from two tertiary-care medical centers, 67 patients underwent TOGA procedure for morbid obesity and then followed up for 12 months to assess the safety and procedure efficacy. The percentage of EWL was 29.3% ± 11.6, 36.8% ± 15.7, and 38.7% ± 17.1 at 3, 6, and 12 months, respectively. At 12 months, excess BMI also was seen more in patients with baseline BMI of <40 (52.2%) compared with patients with baseline BMI of ⩾40 (41.3%) with a p value of <0.05. Significant improvement in the quality of life was seen at 6 and 12 months. This study showed that TOGA is a safe and efficacious procedure, but further studies needed to examine long-term safety as patients were followed for 12 months, only. 68
Currently, two systems are available for use for ESG: the Apollo OverStitch™ (Figure 2) and Endomina™ [Endomina, Endo Tools SA (STT), Gosselies, Belgium]. Table 4 shows various ESG studies with outcomes.

The Apollo OverStitch™ Suturing System With a Double-Channeled Therapeutic Gastroscope.
Various ESG Studies With Their Individual Outcomes.

BMI, body mass index; EWL, excess weight loss; TWL, total weight loss.
The data presented in this table are for representation purposes only. This table, in no manner, depicts the comparison between these devices.
Apollo OverStitch Suturing System creates a restrictive sleeve. It applies full-thickness sutures alongside the stomach’s greater curvature through a double-channel therapeutic gastroscope79,80 (Figure 3). It reduces the functional capacity of the stomach and increases satiety. 23 In a large prospective observational study, 1000 consecutive patients with BMI 33.3 ± 4.5 kg/m2 underwent ESG with an overstitch system. The mean percentage of total weight loss (TWL) was 8.9 ± 2.9%, 10.5 ± 4.5%, 13.7 ± 6.8%, 15.2 ± 8.3%, 15.0 ± 7.7%, and 14.8 ± 8.5% at 1, 3, 6, 9, 12, and 18 months, respectively. Abdominal pain or nausea (92.4%) was the most commonly reported complaint during the first 5 days after surgery. There was no reported need for emergent intervention or mortality. Revision to sleeve gastrectomy or redo ESG was done in 13 patients. 70 A retrospective analysis of a prospectively maintained database of 248 patients who underwent ESG with the OverStitch system showed a percentage TBW loss of 15.2 [95% confidence interval (CI): 14.2–16.3] and 18.6 (95% CI: 15.7–21.5) at 6 and 24 months, respectively. Five (2%) serious procedure-related adverse events were noted. 74 Another prospective study of 91 patients who underwent ESG with an overstitch system showed a mean percentage of TBWL of 14.4%, 17.6%, and 20.9% at 6, 12, and 24 months, respectively. Mild symptoms like self-limiting nausea lasting < 48 h and mild to moderate abdominal pain lasting < 48 h were experienced by 38% and 27.4% of patients, respectively. In contrast, the serious adverse events occurred in only one patient (1.1%), who had peri-gastric leak management non-operatively. 73 A study conducted in India on the outcomes of 55 patients undergoing ESG showed improved weight loss, TBW loss, and BMI a year after surgery. 49 The authors noted no serious adverse events. 49

AspireAssist® Weight Loss System.
Endomina system is a single-use over-the-scope suturing device assembled in the stomach with an endoscope, and it enables physicians to do large plications with transmural anterior-to-posterior endoscopic sutures. 58 In a multicenter prospective trial, 51 patients with a mean BMI of 35.1 kg/m2 underwent ESG with an endoluminal suturing device and then followed for 1 year. No serious adverse events were reported. At 1-year follow-up, overall EWL and TBWL were 29% and 7.4%, respectively. During a follow-up gastroscopy performed in 30 patients, 88% of sutures were in place. 78 Similarly, two patients with a BMI of 40.5 and 37.7 kg/m2 underwent ESG with Endomina suturing system. Within 3 months of the procedure, BMI was reported to down to 38 and 33.4 kg/m2 in these patients. Both patients reported only mild upper abdomen ache but no major adverse events. 81 In a recent RCT, 71 patients with a BMI of 30–40 kg/m2 were randomized to either lifestyle modification plus ESG with Endomina system (n = 45) or lifestyle modification alone (n = 21). At 6 months, lifestyle modification plus ESG with Endomina system group found to have higher mean EWL (38.6% vs 13.4%, p < 0.001), decrease in mean volume (41% vs 2.5%, p < 0.001), and mean quality of life (52.8% vs 45.1%, p < 0.05) than in the lifestyle modification alone group. Long-term follow-up for ESG with Endomina system used along with lifestyle modification group showed % EWL of 51% and 41.3% at 9 and 12 months, respectively. Although the sample size is small in this study, it showed that quality of life and weight loss improve dramatically when ESG with Endomina system is used along with lifestyle modifications. 82
In June 2019, a consensus meeting of 47 endoscopists experienced in ESG with 1828 procedures was held in Brazil. The published results of this study showed a TBWL of 18.2% in 1 year. Complications were reported in 0.82% of cases, with hematemesis being most common. This consensus group agreed on several consensus statements such as indication, contraindication, procedure techniques, and post-procedure follow-up. 83 A meta-analysis examining 22 cohort studies on ESG showed that the procedures were effective at short-term weight loss with few adverse risk events. 84 However, a recent meta-analysis showed that ESG improved weight loss compared with laparoscopic techniques with fewer side effects. 85 Furthermore, the weight loss continued for up to a year. 85
ESG is a restrictive endoscopic bariatric procedure that is a potentially repeatable and reversible procedure. 23 A retrospective analysis of 120 patients from a prospective database who underwent ESG resulted in mean percentage EWL, mean percentage TBWL, and mean Bariatric Analysis and Reporting Outcome (BAROS) score at 12 months as 44.4% (±19.5), 18.3% (±6.7), and 4.5 (±1.7), respectively. Redo ESG procedure was performed in four patients. New stitches were positioned to avoid overlap with previous stitches, and old stitches were removed during the second procedure. The 6-month follow-up was available for three patients with mean % EWL, % TBWL, BAROS mean score as 44.2% (range: 30.5–59.1%), 20.4% (range: 16.7–24.5%), and 6.3 (range: 6–7), respectively. No peri-procedure complications were reported after the redo procedure, and all four patients reported excellent satiety after this redo procedure. 86 Although this study had a small sample, it showed promising results for a redo procedure.
Modifications to the procedures and devices used in endoscopic sleeve surgery have significantly improved previous EBT surgeries. The procedure utilized a ‘longitudinal compression’ suture pattern, which distributes tension equally across each stitch in the anterior-posterior and craniocaudal dimensions of the stomach. 87 Patients who underwent the longitudinal compression stitches had a significant reduction in body weight, BMI, and TBW loss compared with patients with the traditional stitching method of endoscopic gastric sleeve surgery. 87 This procedure is not approved by the FDA. A recent UK study demonstrated that a modified endoscopic gastric sleeve surgery resulted in superior weight loss compared with previous EBTs and bariatric techniques. 87
EndoZip™ (NitiNotes Surgical, Caesarea, Israel) is a new fully automated, operator-independent, endoluminal-sutured gastroplasty system. By ap-proximating opposing walls of the stomach using the endoscopic technique, it creates multiple internal gastric segmentation. A single-center, first-in-human study involving 11 patients with a BMI of 30–40 kg/m2 was conducted to assess the technical feasibility of EndoZip™ for the treatment of obesity. A median of three sutures were placed, and the technical success of the procedure was 100%. No intraprocedural complications were reported, and only one patient respiratory infection, which was attributed to general anesthesia/and or procedure. The mean ± SD % EWL and TBWL was 46.5 ± 28.6% and 13.5 ± 4.7% at 3 months and 54.3 ± 28.4% and 16.2 ± 6.0 (p < 0.001) at 6 months, respectively. Although this study showed promising results, the sample size was small, so further large studies are needed to study the efficacy and safety of this procedure. 88
Malabsorptive endobariatric procedures
The small intestine is the primary site for nutrient absorption and regulator of glucose homeostasis. The glucose homeostasis is maintained through small peptides released by enteroendocrine cells that modulate satiety and insulin secretion. Given this process, malabsorptive EBTs improve weight loss and insulin secretion by impeding nutrient absorption and improving peptide secretion from enteroendocrine cells. 15 The food bypasses small intestines with these methods improving weight loss and glucose homeostasis. The primary mechanism for a precursor for malabsorptive EBTs is based upon the surgical principles of the RYGB. 15 The RYGB is a malabsorptive EBT procedure that divides that stomach into a small pouch and a large remnant. The smaller pouch is then connected to the jejunal Roux limb, which bypasses the stomach, duodenum, and proximal jejunum.
Patients with RYGB showed a 27% increased reduction in TWL and decreased long-term all-cause mortality rate compared with the control group. 89 Further studies showed that RYGB patients had resolved diabetes and restored ghrelin, GLP-1, PYY, and cholecystokinin (CCK) within normal limits.90–92 Many advances have occurred with the use of RYGB. Given its success, three endoscopic devices/procedures, Endoluminal Bypass, EndoBarrier, and Duodenal Mucosal Resurfacing, were developed to mimic the efficacy of the RYGB. 14 Table 5 shows malabsorptive endobariatric procedures.
Malabsorptive Endoscopic Bariatric Therapy (EBT) Studies.

BMI, body mass index; EWL, excess weight loss; TWL, total weight loss.
The data presented in this table are for representation purposes only. This table, in no manner, depicts the comparison between these devices.
EndoBarrier
A common malabsorptive EBT procedure that mimics the RYBG is the EndoBarrier (GI Dynamics, Inc., Watertown, MA, USA) or duodenal-jejunal bypass sleeve (DJBS), now renamed as duodenal-jejunal bypass linear (DJBL). The device uses a 2-ft-long fluoropolymer sleeve, which extends from the duodenal bulb to the proximal jejunum, thereby bypassing nutrients from being absorbed by the duodenum. Furthermore, pancreatic enzymes and bile acids are prevented from mixing with the nutrients until further down the jejunum. The reduced nutrient absorption allows for weight loss in obese patients. A meta-analysis showed that the EndoBarrier increased EWL by 12.6% compared with current interventions. 93 Furthermore, the EndoBarrier also improved fasting plasma glucose (FPG), which allowed patients to reduce or discontinue the dose of their antidiabetic medications. 93 A US clinical trial found that over 60% of patients had greater than 5% TWL; a third of patients also achieved a hemoglobin A1c level of less than 7%. 94 On average, it brought down the HBA1c by around 1.5%.
However, there have been concerns about sleeve migration/occlusion, pancreatitis, and liver abscesses due to potential biliary occlusion. A systematic review and meta-analysis of 38 studies conducted on adverse events associated with DJBL showed a total of 891 adverse events in 1056 patients. According to ASGE guidelines, 75.8%, 20.5%, and 3.7% of adverse events were classified as mild, moderate, and severe events, respectively. The anchor of DJBL led to 85% of severe adverse events, and it included esophageal and duodenal bulb perforation, DJBL anchor tissue overgrowth, and GI hemorrhage. 95 Betzel and colleagues conducted a study to determine the efficacy and safety of DJBL with 24 months of implantation time. The largest decrease in body weight loss and glycemic control was achieved during the first 9–12 months after implantation of DJBL. Adverse events were observed in 68% of patients. It was found to be better tolerated during the first 12 months as more patients were required early removed during the 12–24 months period due to increased adverse events during this extended period. Given that maximal beneficial effects and fewer adverse events are seen in the first 12 months, this study recommended not to extend implantation time beyond 12 months. 96 Due to safety concerns, the FDA has not approved this device yet, although the CE mark was initially issued but was withdrawn. 97
Endoluminal bypass sleeve
An additional modification to the EndoBarrier was developed with the Endoluminal Bypass device (ValenTx, Inc. Carpinteria, CA, USA). 98 The Endoluminal Bypass consists of a sleeve attached to the gastroesophageal junction to create an endoluminal gastro-duodenojejunal bypass like the RYGB. This device is not yet approved by the FDA. 63 A study of 12 patients with the endoluminal bypass showed a 54% increase in EWL over a year. 98 However, 2 patients could not tolerate the device due to nausea and vomiting, with only 6 of the 10 patients had the Endoluminal Bypass a year later. Despite the intolerance to device, hypertension, diabetes, and hyperlipidemia improved in all the patients. 98
Duodenal mucosal resurfacing
A more invasive approach to the malabsorptive EBTs is the duodenal mucosal resurfacing (DMR) (Fractyl Laboratories, Cambridge, MA, USA) or the Revita™ (Fractyl Laboratories, Cambridge, MA, USA) procedure. 14 This procedure is not FDA approved yet. 64 DMR is a minimally invasive catheter-based upper endoscopic procedure. It involves circumferential hydrothermal ablation of duodenal mucosa via a wire-guided balloon catheter system filled with heated water. 99 It is believed to help the mucosal remodeling and inactivate dysfunctional enteroendocrine cells. 14 The first-in-human study using the DMR in patients with diabetes mellitus type 2 showed a reduction in their hemoglobin A1c levels by 1.2% at 6 months. However, a few patients developed duodenal stenosis requiring endoscopic dilatation. 100 A recent multicenter prospective study of 46 patients with BMI between 24 and 40 kg/m2 and diabetes mellitus type 2 was conducted to evaluate the safety and efficacy of DMR. At 24 weeks after the procedure, glycated hemoglobin, FPG, and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) were reduced by 10 ± 2 mmol/mol, 1.7 ± 0.5 mmol/L, and 2.9 ± 1.1, respectively, compared with baseline with a p value of <0.001. During the first-year follow-up, 52% of patients reported adverse events, but most of these adverse events were mild. 101 In a review of four clinical studies, 79 DMR patients were reported to have significant short-term metabolic effects with statistically significant (p < 0.001) reduction of mean HbA1c, FPG, and HOMA-IR of 0.9 ± 0.2%, 1.7 ± 0.5 mmol/L, and 2.9 ± 1.1 mul/L, respectively. Mild postoperative adverse events were reported in 64% of cases and severe adverse events in 3.7% of cases. 102
Future directions
EBTs are used regularly to treat bariatric surgery complications and for revision of the former when there is weight regain. This combination of weight loss pharmacotherapy (e.g. Liraglutide) and various EBTs has recently gained more traction. 103 The treatment has to be personalized to match the intervention/device to the physiological phenotype of the individual to optimize outcomes. The phenotype may be decided based on gastric emptying, especially when deciding between various restrictive modalities. 17 Likewise, pouch size and outlet size might be utilized to decide between plication and suturing. 104 The newer devices on the horizon include Endosleeve™ by Metamodix to treat metabolic syndrome; the endoluminal magnets would create a side-to-side entero-enteric anastomosis. Beyond treating obesity, EBTs have applications in other medical therapies, including bridging therapy, cosmetic therapy, and bariatric surgery revision. 14 Despite its broad applications, further studies are needed to understand the mechanisms of actions of each EBT and their surgical outcomes for long-term weight loss maintenance and personalized therapy. 103 EBT procedures may provide alternatives for screening obese patients for long-term complications, using minimally invasive endoscopic procedures. For example, transnasal endoscopy (TNE) is competent at evaluating obese patients before bariatric surgery without the need for sedation. 105 EBTs are becoming an essential tool for improving sustained weight loss in obese patients without long-term adverse effects.7,14 Similar to traditional bariatric surgery, EBTs are effective at controlling metabolic comorbidities, lowering adverse risk events, and improving overall weight loss among obese patients.7,14
Several new EBTs are being investigated currently, including Endoscopic Gastric Mucosal Devitaliza-tion (ClinicalTrials.gov identifier: NCT03526263, NCT03638843, and NCT03288259). Similarly, clinical trials are examining new suture devices and techniques, such as the Endoluminal-suturing Device, which will improve EBT outcomes and reduce short- and long-term surgical outcomes (ClinicalTrials.gov identifier: NCT03900481 and NCT01067625). Studies in the future should evaluate the mechanism and long-term treat-ment outcomes for EBTs compared with traditional bariatric surgeries (ClinicalTrials.gov identifier: NCT04006002, NCT01871896, and NCT03705416). Together, all these will advance the efficacy of EBTs and establish accepted guidelines for its more extensive use among obese patients and a global acceptance by the medical community.
Conclusion
EBTs remain an evolving, minimally invasive surgical technique that improves surgical outcomes, prognosis, and surgical complications. It has been shown that the single most important independent predictor of success regardless of the type of endobariatric treatment received was the adherence to outpatient follow-up. Further studies are needed to establish guidelines for EBT devices, surgical techniques, long-term outcomes, and complications. EBTs and surgical protocols may be combined with traditional bariatric surgery techniques to improve surgical outcomes, reduce adverse surgical events, and reduce obesity-related comorbidities. Furthermore, endoscopic procedures can also help screen the anatomy, function, and pathological findings of an obese patient’s foregut for any risk factors influencing the long-term outcome of bariatric surgeries or EBTs. High-quality RCTs are required to examine whether combined EBTs with bariatric surgery or interventions can improve therapeutic outcomes and help establish guidelines for the safe application and success of EBTs in the future.
Footnotes
Acknowledgements
The authors would like to thank AspireAssist® for providing the image of their endobariatric system.
Author contributions
Conception and design: H.G., A.P.; literature search: H.G., J.K., A.P.; first draft: H.G., J.K., A.P.; critical revision and editing: all authors; final approval: all authors.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have made substantive contributions to the study, and all authors endorse the data and conclusions. B.T. serves as a consultant for Boston Scientific.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.