Obesity is a leading cause of preventable death in developed countries, with a rising incidence over time. Lifestyle modification, pharmacotherapy, and bariatric surgery are the mainstays of bariatric therapy, even though burdened by several limitations in terms of efficacy or safety. Bariatric endoscopy has been developed in the last decades as a minimally invasive alternative, aimed to bridge the gap between conservative and interventional conventional therapies. This review aims to provide an updated overview of the bariatric and metabolic available endoscopic procedures and to drive the choice of the right procedure for the right patient.
Obesity is a chronic, relapsing, multifactorial disease defined as abnormal or excessive adipose tissue accumulation that may impair health and significantly increase disease risk.1–3 In the clinical setting, obesity is defined as body mass index (BMI) of 30 kg/m2 or above.2 Obesity is a major risk factor for several chronic diseases, including diabetes, cardiovascular diseases, sleep apnea, gastrointestinal and endocrine disorders, bone and joint diseases, and malignancies.2 Notably, the prevalence of obesity is rising over time; in the United States in 2016, 39.8% of adults and 18.5% of young aged 2–19 years were obese.4 Treatment for obesity include dietary and lifestyle interventions, pharmacology, endoscopy, and surgery. A multidisciplinary team should be involved in order to maximize the efficacy of each intervention through a personalized approach.2,5,6 While dietary monitoring, lifestyle interventions and medications are still considered as the cornerstone of bariatric treatments, nevertheless, their efficacy alone is often temporary and/or inadequate.7–11 Bariatric surgery has been shown to be the most effective treatment for obesity.8 However, inclusion criteria for surgery are BMI over 40.0 kg/m2 or of 35–39.9 kg/m2 with comorbidities,9 and less than 2% of surgical candidates finally undergo intervention, due to contraindications, patient preference or inaccessibility.7,12,13 Therefore, in the last decades, there has been a trend in developing minimally invasive and potentially long-lasting approaches for the treatment of obese patients for whom conservative strategies fail (Figure 1).2
Bariatric noninvasive endoscopic techniques.
Choosing the right procedure among this wide variety of endoscopic techniques for the right patient may be challenging, also considering that specific guidelines that may drive the choice are still lacking. The aim of this review is then to provide an updated overview of the current bariatric endoscopic interventions and to help drive the choice among the available strategies.
Review of the literature
A comprehensive review of the English-language literature on bariatric and metabolic endoscopic interventions was performed using the MEDLINE (Via PubMed) database up to September 2019 by two authors (B.O. and I.B.), using the keywords “Bariatric endoscopy,” “Metabolic endoscopy,” and “Obesity AND endoscopy.” Hand-search of bibliographies of included studies and previous reviews was also performed to search for additional relevant studies. The following data were recorded: number of patients, follow-up duration, total body weight loss (TBWL), excess weight loss (EWL), metabolic outcomes such as fasting plasma glucose (FPG), glycated hemoglobin A1c (Hb1Ac), rate and type of severe adverse events (SAEs).
Restrictive procedures
Space-occupying devices
Restrictive procedure by space-occupying devices is one of the mainstays of endoscopic bariatric treatments. There is a large body of evidence suggesting the efficacy and safety of space-occupying devices so far.
Intragastric balloons
Intragastric balloons (IGBs) are minimally invasive and temporary weight loss systems associated with a reduction of the gastric volume and with alteration of gastric motility.14 Alteration in gut hormones and peptides levels such as leptin, ghrelin, cholecystokinin, and pancreatic polypeptide, seems to be implicated in the weight loss process as well.15,16 IGBs have shown to improve most metabolic outcomes, including FPG, Hb1Ac, triglycerides, cholesterol, thyroid-stimulating hormone, waist circumference or blood pressure.17–22 All the IGBs have to be removed after 6–12 months to reduce the risk of spontaneous deflation.12 Considering that obesity is a chronic disease, this short-time application may be a downside; however, this procedure is repeatable over time.23 Scientific evidence deriving from main pivotal clinical trials regarding follow-up outcomes (%EWL and %TBWL mainly) for each type of IGB is reported in Table 1.20,24–26 Several systematic reviews and meta-analysis have evaluated the efficacy and safety of IGBs: Tate and Geliebter27 reported a main %TBWL of 9.7% and a rate of SAEs of 10.5%, including acute pancreatitis at 6-month follow-up. In 2018, the US Food and Drug Administration (FDA) issued an alert concerning the Orbera and ReShape Duo IGBs being implicated in 33 deaths, 27 of which being specifically associated with Orbera.27 Among such fatalities, at least six occurred within 1 month after IGB placement, four were linked to esophagogastric perforation, one to massive aspiration, whereas the others were due to unspecified causes.28–31 Recommendations on adequate endoscopic training and strict supervision after IGB placement have been stated thereafter,31–33 whereas Apollo Endosurgery has stopped selling and distributing ReShape Balloon since January 2019.
BMI, body mass index; EMA, European marketing approval; EWL, excess weight loss; IGB, intragastric balloon; TBWL, total body weight loss.
In January 2019, Apollo Endosurgery stopped selling and distributing the ReShape Balloon.
The latest balloon available in the market is the Elipse balloon (Allurion Technologies, Wellesley, MA). This is a swallowable device that can be externally filled up with saline solution and that has the peculiarity of self-emptying after a period of 4 months, allowing spontaneous excretion through the GI tract. The device received European marketing approval (EMA) and is waiting for FDA approval. The evidence available on Elipse device are still scanty; however, in the last 2 years, one prospective series on 135 patients and one on 112 patients were published.35,36 The first study reported a mean %TBWL of 15.1% at 4-month follow-up, while in the latter found a mean %TBWL of 10.9% at 6 months.35,36
Non-balloon space-occupying device
TransPyloric Shuttle (TPS) Device (BARONova, San Carlos, CA) is a silicone spherical device connected to a smaller cylindrical bulb by a flexible catheter. The shape of this device is designed to take place across the pylorus, inducing a delayed gastric emptying. TPS has been approved by the FDA in 2019 for patients with a BMI of 35–40 kg/m2 or 30–34.9 kg/m2 with at least one obesity-related comorbidity.37 Early results on TPS were retrieved from a pilot study on 20 patients, who achieved mean %EWL of 41.0% and mean %TBWL of 14.5% at 6 months.38 More recently, a randomized clinical trial showed a mean difference of 6.7% in %TBWL between the TPS group and the controls at 12-month follow-up (%TBWL of 9.5% and %EWL of 30.9% at 12 months in the TPS group). SAEs were rare (2.8%) and included: esophageal rupture, device impaction, upper abdominal pain, gastric ulcer, vomiting, pneumothorax. Premature balloon removal occurred in 22.7% (46/203) of the cases.38
SatiSphere (Endosphere, Columbus, OH) is a 20–25 cm long device composed of mesh spheres mounted on a nitinol wire with pigtails ends, which self-anchors in the distal part of the stomach or in the proximal duodenum and which is designed to delay the duodenal transit. SatiSphere received CE Mark regulatory approval but did not achieve FDA approval. Despite the mild effect on %TBWL, positive metabolic outcomes such as delay of glucose absorption and insulin secretion, or increasing in alterations of glucagon-like peptide 1 (GLP-1) kinetics were reported in a small cohort of patients. The trial was prematurely interrupted due to a high percentage of device migration (48%).39
Plenity (Gelesis, Boston, MA) is an orally administered capsulated device containing hydrogel particles that expand inside the stomach after water absorption, with consequent early satiety, delayed gastric emptying, and delayed glucose absorption. Plenity has recently obtained FDA approval for patients with a BMI of 25–40 kg/m² in association with dietary interventions.40 The pilot study on 128 non-diabetic overweight patients showed that Plenity 2.25 g twice daily was associated with significant weight loss compared to the placebo group.41 These results were confirmed in the Gelesis Loss Of Weight (GLOW) study, which showed a significant reduction of Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) and greater weight loss in patients treated with Plenity over placebo, with a mean %TBWL of 6.4% versus 4.4% at 6 months.42 Better results were achieved in patients with untreated type-2 diabetes or elevated FPG.41 No SAEs were reported.42 More recently, the compatibility of Plenity with metformin was demonstrated in a 24-patient cohort.43
Suturing/stapling devices
Suturing or stapling techniques aim to reduce the gastric capacity by changing the anatomy of the stomach.23
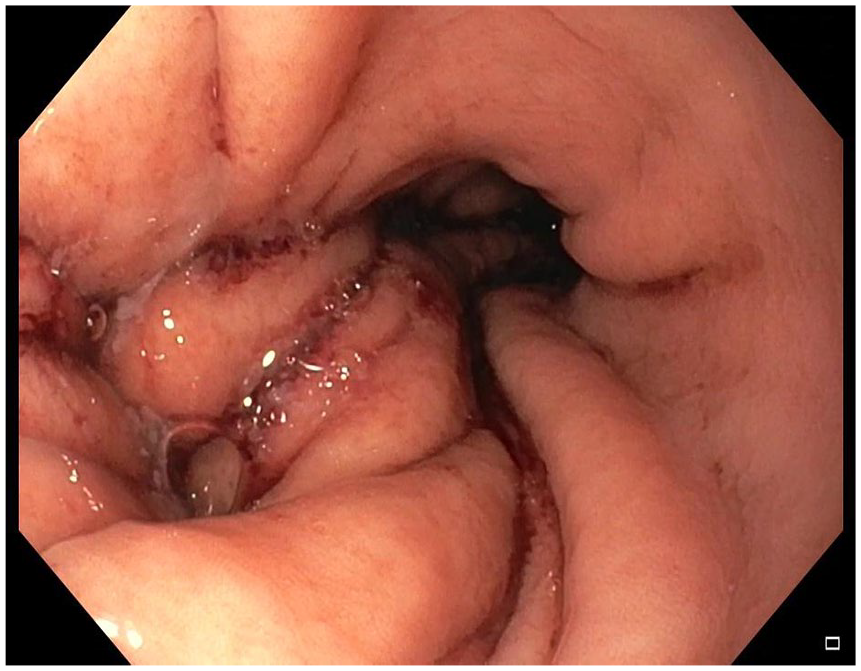
Endoscopic Sleeve Gastroplasty (ESG) with Apollo OverStitch Suturing System is a technique aimed to restrict the gastric cavity into a sleeve-like configuration using the FDA-approved full-thickness suturing device (OverStitch; Apollo Endosurgery, Austin, TX) aided by a helix grasp through a double-channel therapeutic gastroscope (Figure 2).44,45 ESG procedure is potentially reversible and repeatable to achieve extra weight loss.46 Its mechanism of action induces alteration in gastric capacity and motility, increases satiety and seems to induce ghrelin reduction.46 In 2014, Sharaiha and colleagues47 published the first results of ESG on 10 patients, showing a mean %EWL of 30% at a 6-month follow-up. More recently, the same authors reported a %TBWL of 14.4% at 6 months on 73 patients treated with ESG. A significant reduction in values of systolic blood pressure, HbA1C, triglycerides, and alanine aminotransferase were reported in patients treated with ESG at a 12-month follow-up.48 Consistent results in terms of %TBWL at 6 months were reported in recent retrospective or prospective series.45,49–51 In the largest cohort published so far, Alqahtani and colleagues45 reported a %EWL of 64.3% at 6 months (n = 369) and of 67.5% at 12 months (n = 216). A higher rate of %EWL was reported by Graus Morales and colleagues,52 namely 75.4 ± 85% at 12 months, while Sartoretto and colleagues50 and Barrichello and colleagues51 described a %EWL of 50.3% and 56.1% at 6-month follow-up, respectively. Long-term data were available in the series by Lopez-Nava and colleagues,53 who reported a mean %EWL of 60.4% at 24 months. A recent meta-analysis concluded that ESG is associated to a mean %EWL of 57.7% (95% CI, 52.0–63.4) and a mean %TBWL of 15.1% (95% CI, 14.3–16.0) at 6-month follow-up.54 ESG procedure has shown to be relatively safe, with a pooled rate of SAEs of 2.2% (95% CI, 1.6–3.1%), including perigastric fluid collection or leak, bleeding, and abdominal pain.54 Incidence of less-severe adverse events (AEs) such as abdominal pain and nausea was variable, ranging from 20 to 90% across different series.45,48,51 When compared to surgery, two studies pointed out similar results in terms of efficacy and safety. Fayad and colleagues55 and Novikov and colleagues,56 in fact, reported a significantly higher %TBWL in patients treated with laparoscopic sleeve gastrectomy compared to ESG but a lower rate of SAEs in the ESG cohort. Table 2 summarizes ESG outcomes considering the most impactful studies.
Endoscopic sleeve gastroplasty with the Apollo OverStitch endoscopic suturing system. Endoscopic appearance immediately after the procedure.
BMI, body mass index; NA: not available; %TWL: total body weight loss.
18-month follow-up.
%EWL.
20-month follow-up.
Primary Surgery Endoluminal (POSE) consists of full-thickness tissue plications performed in the fundus and in the distal gastric body using an incisionless operating platform (IOP; USGI Medical, San Clemente, California, USA) (FDA approved for tissue apposition, received CE mark). The POSE procedure was shown to increase the sense of satiety by temporarily retarding the gastric emptying and to improve leptin levels and glucose homeostasis at the 15-month follow-up.57 The efficacy of POSE was evaluated in a randomized multicenter trial, in which mean %TBWL in the POSE cohort (n = 221) was 4.9% compared with 1.4% in the lifestyle intervention group (n = 111). The co-primary endpoint of the study, namely the achievement of a %TBWL greater than 5% in more than 50% of patients, was not reached, but improvement of glycemic control, hypertension, and cholesterol levels were reported in the POSE group.58 Better results were achieved in a European multicenter study, which reported a %TBWL of 13% and a %EWL of 45% in the active group versus 5.3% and 18.1% in the lifestyle group, respectively.59 Consistent results with this trial were previously published by two observational Spanish cohorts.60,61 No SAEs were reported, except in the first trial, where one case of extra-gastric bleeding requiring surgical intervention and one case of hepatic abscess requiring interventional drainage were reported (overall SAEs rate of 4.7%).58 A recent systematic review and meta-analysis by Gys and colleagues analyzed the efficacy and safety of ESG and POSE procedure. The authors concluded that pooled %EWL at 12 months was 68.3% for ESG and 44.9% for POSE procedure.62 The superiority of ESG over POSE procedure was confirmed in the recently published meta-analysis by Khan and colleagues.63 In terms of safety, bleeding was described for both techniques, but ESG was associated to a higher number of perigastric collection, pulmonary complications, and leakage.62 Of note, Cohen and colleagues64 recently questioned the scientific quality of studies evaluating the gastroplasty procedure, suggesting the need for more robust evidence. Recently, a POSE II procedure has been developed, and this consists of placing stitches at the level of the greater gastric curvature, and not at the fundus.
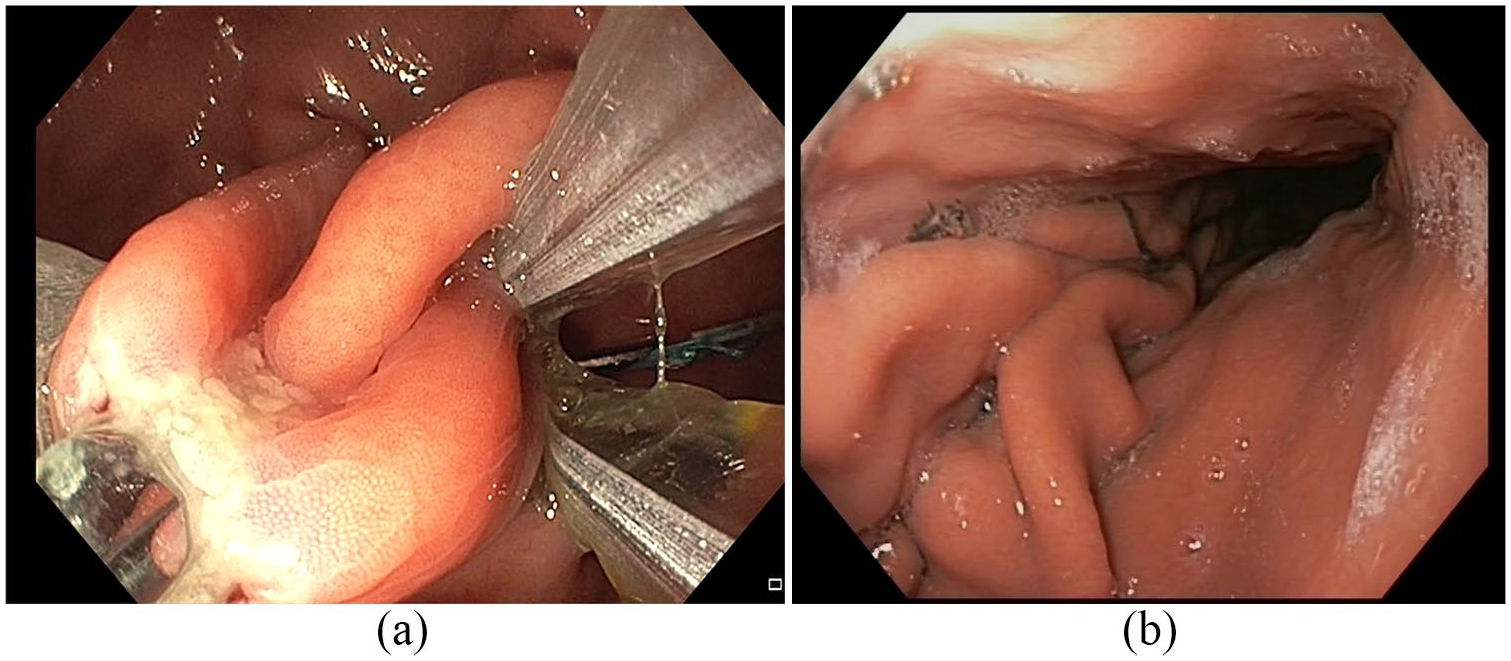
ESG with Endomina suturing system (Endo Tools Therapeutics, SA-ETT, Gosselies, Belgium) (not FDA approved, received CE mark) is a single-use over-the-scope device that allows creating a double plicature of the greater curvature through the use of interrupted sutures, transmural anterior-to-posterior endoscopic suture (Figure 3). The safety and feasibility of Endomina were evaluated in two studies by Huberty and colleagues,65,66 reporting %EWL of 31% at 6 months and 29% at 12 months. No SAEs occurred.
(a) Endoscopic sleeve gastroplasty with the endomina suturing system. (b) Endoscopic sleeve gastroplasty with the endomina suturing system: endoscopic appearance one.
The articulating circular endoscopic device (ACE) (Boston Scientific Corporation, Natick, MA) (not FDA approved) consists of an endoscopic rotatable and retroflexable stapler creating full-thickness gastric volume reduction. Early results have shown technical feasibility and safety of this device on 17 patients, in which the main %EWL was 34.9% at 12 months.67 Accordingly, in a multicenter study on 69 patients, similar results were achieved at a 12-month follow-up, while %EWL at 24 months was 21.0%.68 No SAEs were reported in both series.67,68
Malabsorptive techniques
Malabsorptive endoscopic techniques aim to physically prevent the contact between nutrients and the upper intestinal mucosa, emulating anatomical alterations of Roux-en-Y gastric bypass.
Duodenal-Jejunal Bypass liner Endobarrier (DJBL) (GI Dynamics, Lexington, Massachusetts, USA) (not FDA approved, withdrawal of CE mark) is a 60-cm-long fluoropolymer sleeve anchored in the duodenal bulb and extending into the proximal jejunum. This system is contained within a capsule and is deployed under endoscopic and fluoroscopic control. Endoscopic removal is performed after 3–12 months, thanks to a specially designed hook that grasps the device inside a protective hood. Since its introduction in 2010, a wide number of studies have shown conflicting results in terms of efficacy and safety for this device. Five pivotal trials have compared DJBL with control or placebo group.69–73 The systematic review and meta-analysis conducted by the ASGE Bariatric Endoscopy Task Force concluded that DJBL induced a mean %EWL of 35.3% (95% CI, 24.6–46.1%) at 12 months.74 Mean additional %EWL over the control group, however, was shown to be 9–12%, therefore unable to meet the expected 15% difference.74,75 In parallel, several reports have shown that DJBL system was associated with significant improvement in glycemic parameters in patients with type-2 diabetes,74–79 but one meta-analysis failed to demonstrate statistically significant differences in terms of HbA1c in comparison with the control group.80 The mechanisms associated with a positive metabolic effect are yet to be elucidated, but they may be similar to those already investigated in the Roux-en-Y gastric bypass.78 Concerning the safety of this system, abdominal pain and nausea have been the most common mild AEs reported.78 The most recent systematic review calculated a 3.7% rate of more severe SAEs, mainly including GI bleeding, hepatic abscess, and esophageal perforation.81 The rate of SAEs has been proved to significantly increase after 1 year of treatment.82 Early removal of the device was necessary in 24.1% of patients treated with DJBL.81 Of note, one multicenter, randomized, sham-controlled pivotal trial named ENDOtrial was prematurely abandoned after enrolment of 325/500 patients due to a relatively high incidence of hepatic abscess formation (3.5%).83 For safety reasons, the device did not receive FDA approval, whereas CE mark was achieved in 2009, then withdrawn in 2017.84
Gastroduodenojejunal bypass sleeve (GJBS) (ValenTx Inc, Carpinteria, CA) (not FDA approved) is a malabsorptive device 60 cm longer than EndoBarrier anchored at the gastroesophageal junction. In a small cohort of 22 patients, Sandler and colleagues found that 17/22 patients had the device correctly positioned at the 12-week follow-up. In this cluster of patients, GJBS induced a %EWL of 39.7%.85 The same authors published the results of GJBS at 12 months on 13 patients. Among the six patients having fully attached functional devices, GJBS achieved a mean %EWL of 54% without experiencing any SAE.86 Significant improvement of comorbidities was reported in both series;85,86 however, more robust data are needed to confirm these results.
Revita duodenal mucosal resurfacing procedure (DMR) (Fractyl Laboratories, Cambridge, MA) (not FDA approved, received CE mark) consists of thermal ablation of duodenal mucosa through a balloon filled with heated water. This approach has shown to achieve only mild effects as a bariatric treatment but positive outcomes in terms of glycemic control in patients with type-2 diabetes. In the pilot study by Rajagopalan and colleagues, 39 patients with type-2 diabetes underwent DMR procedure, with consequent improvement of 1.2% in mean HbA1c at 6-month follow-up, without statistically significant difference depending on the length of the ablation at 6 months. Three cases of duodenal stenosis were reported, all managed with endoscopic dilation.87 We might presume that adequate submucosal lift and avoidance of overlapping ablations might reduce the risk of this complication, but further data are needed. More recently, a prospective study on 46 patients was published by van Baar and colleagues. After the exclusion of 20% of patients due to technical failure, the procedure was associated with significant improvement of HbA1c, FPG, and HOMA-IR at 12 months. Mild to moderate AEs were reported in 52% of patients, while any patient experienced procedure-related SAEs.88 Ongoing clinical trials are aimed to clarify the effects of DMR in patients with type-2 diabetes and other chronic diseases such as polycystic ovary syndrome.89
Incisionless Anastomosis System (IMAS) (GI Windows, W. Bridgewater, Massachusetts, USA) (not FDA approved) consists of self-assembling magnets delivered through the endoscope into the terminal ileum and proximal jejunum to create an enteral diversion. The magnets are self-eliminated through the stools. A pilot study on 10 patients showed significant improvements of HbA1c and blood glucose levels in diabetic and pre-diabetic patients, as well as promising results in terms of weight loss: %TBWL and %EWL at 12 months of 14.6% and 40.2%, respectively. No device-related SAEs were reported.90 More reliable studies are needed.
Other techniques
The AspireAssist Aspiration therapy (AA) (Aspire Bariatrics, King of Prussia, PA, USA) consists of a percutaneous gastrostomy A-tube coupled with a SkinPort and an aspiration tube, aimed to partially drain the ingested food. This system was approved by FDA in 2016 for long-term use in patients aged over 22 years with BMI of 35–55 kg/m², after the failure of nonsurgical strategies, in association with lifestyle counseling and cognitive behavior therapy.91,92 Positive association between AspireAssist (AA) device and cardio-metabolic improvement (including HbA1C, triglycerides, high-density lipoprotein cholesterol, and blood pressure values) was reported.93,94 Several pivotal studies have investigated the AA system as a weight-loss strategy.94 Of these, the pivotal aspiration therapy with adjusted lifestyle therapy (PATHWAY) study showed higher weight loss in the AA group (n = 111) compared with the lifestyle counseling group (n = 60): %TBWL 12.1% versus 3.5% and %EWL 31.5% versus 9.8% at 52 weeks.93 Recently, the 4-year long-term maintenance study was published on 58 participants who completed 1 year of treatment. Of these, 43 patients withdrew the study before the fourth year, due to adequate weight loss (58%), lack of efficacy, or local irritation (42%). Patients achieved a mean %EWL of 50.82% and mean %TBWL of 18.7% at 4-year follow-up.95 In the meta-analysis by Khan and colleagues, AA system was associated with a mean %EWL of 50.85% (range 46–55.7%) and to a mean %TBWL of 15.4% (range 9–21.7%) at 12 months. No statistically significant difference was found in terms of %EWL and %TBWL between patients treated with AA, ESG, and POSE.63 Concerning safety, SAEs were shown to be infrequent, including severe abdominal pain, pre-pyloric ulceration, peritonitis, secondary fistula, and A-tube replacement.93,95 No significant eating disorders or malnutrition were reported after AA treatment in the available series.93–95
Botulinum toxin A (BTA) (not FDA approved) injection has been used in BE because of its effect on blocking the acetylcholine release that induces a transitory delay of the gastric emptying and reduction in maximal gastric capacity.96,97 A systematic review by Bustamante and colleagues98 stated against the use of BTA as not effective in achieving a significant TBWL greater than placebo. These results were confirmed in a very recent randomized clinical trial.99
Absorbable biocompatible material injection has been recently introduced as a complementary treatment together with IGB placement. The procedure involves the injection of hyaluronic acid (HA) at the level of the esophagogastric junction. In a prospective multicenter randomized trial, 101 patients were treated either (A) with IGB alone, (B) with IGB followed by HA at IGB removal, or (C) with HA and IGB at 6 months. The study showed a significantly lower weight loss in the HA group (%TBWL 5.8%) compared with the IGB cohorts at 6 months (%TBWL 8% and 10.8%). Combined treatment with HA was significantly superior at 18 months only compared with IGB alone. One hepatic abscess was recorded in the IGB followed by the HA injection group.100
Choosing the right procedure in bariatric endoscopy
Obesity is a chronic systemic disease that requires a multidisciplinary approach in prevention, treatment, and follow-up.2,5,101 Before recommending a bariatric procedure, we suggest to evaluate the patient in a multidisciplinary team composed by the endoscopist, the gastroenterologist, the surgeon, the anesthesiologist, the psychiatrist, the nutritionist, and the endocrinologist. All patients addressed to our center are usually evaluated by the endocrinologist first, for setting the diagnostic work-up that is tailored according to each patient’s characteristics. As for any other major abdominal surgical procedures, preoperative assessment includes medical history and physical examination, laboratory tests including fasting blood glucose, serum lipid profile, thyroid hormones, and liver function tests, chest X-ray, electrocardiography.5,102,103 Moreover, all patients undergo a glucose-tolerance test and insulin test, abdominopelvic ultrasound, barium swallow radiographic study, upper GI endoscopy with Helicobacter pylori research.5,102,103 Of note, these examinations allow a baseline reference to make the comparison in the posttherapeutic period and to highlight the benefits obtained from the treatment. To exclude clinical contraindications to bariatric treatments, nutritional and psychological/psychiatric counseling are always performed as first-level investigations, whereas a cardiologist and/or pneumologist evaluation is offered to selected patients.5,102 Of note, polysomnography should be routinely done in patients with a high-risk of sleep apnea.102 As psychological disorders may negatively affect postoperative bariatric outcomes,104,105 a careful selection of patients should be performed to exclude patients with poorly controlled or major psychiatric disorders (i.e. drug or alcohol abuse, nonstabilized psychotic disorders, severe depression, personality, and eating disorders, unless specifically advised by a psychiatrist experienced in obesity).106–109 Nowadays, in fact, psychiatric conditions should be diagnosed and treated before addressing the patient to any bariatric surgical treatment.5,106,110
If guidelines counseling the right procedure for bariatric surgical treatments are widely available,107 endoscopic procedure still miss of uniform recommendations. During the multidisciplinary reunions, once selected, the patient who might benefit from interventional bariatric treatment, we carefully assess all procedure-related contraindications, which are usually shared by the main endoscopic procedures (i.e. previous GI surgery, GI structural, or functional abnormality, coagulation disorders, GI tract obstruction or bleeding, pregnancy, breastfeeding, severe liver disease, and any contra-indication to endoscopy).27,37,46,51,57,82,86,88,91,111 The type of surgical or endoscopic procedure best fitting the patient is chosen according to personal history, dietary habits, lifestyle, and the clinical evaluation performed. As it concerns BMI, almost every procedure has different indications related to it (see in each device section). Among the most widespread endoscopic procedures available in our Department, we mainly suggest IGBs as a bridge to surgery in selected cases112,113 whereas we would suggest ESG for patients with BMI between 30 and 40, and as a bridge to surgery in super obese patients, or patients unfit surgery. For the treatment of metabolic conditions such as type-2 diabetes, more robust evidence is needed to compare endoscopic and surgical bariatric procedures. We believe that there is still a certain discrepancy in terms of treatment choice for obesity among reference centers and the scientific community is experiencing the absolute need of universal criteria to choose the right bariatric treatment for each patient.
Conclusion
Obesity is a major cause of death, with a rising incidence over time. It is not only linked to overeating, but it can be considered as a complex disease where genetic and environmental factors are tied together. Endoscopic bariatric therapies include a complex network of procedures that may bridge the gap of efficacy and safety in the management of obesity, but further evidence is required. Among the available endoscopic techniques, the procedure best fitting each patient should be tailored following a multidisciplinary approach. Despite promising attempts, specific and proper guidelines are still a key unmet need: it is, therefore, fundamental to establish universal criteria, easy to apply and of undoubted scientific value in order to orientate the choice of the specific bariatric treatment best fitting each patient.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.C. is consultant for Olympus, Cook Medical, and Boston Scientific. I.B. is a research grant holder from Apollo Endosurgery and is consultant for Apollo Endosurgery, Cook Medical, and Boston Scientific. V.B., C.G., and B.O. have nothing to declare.
ORCID iD
Ivo Boškoski
References
1.
YachDStucklerDBrownellKD.Epidemiologic and economic consequences of the global epidemics of obesity and diabetes. Nat Med2006; 12: 62–66.
2.
AcostaAStreettSKrohMD, et al. White Paper AGA: POWER—Practice Guide on Obesity and Weight Management, Education, and Resources. Clin Gastroenterol Hepatol2017; 15: 631–649.e10.
3.
BrayGAKimKKWildingJPH. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes Rev2017; 18: 715–723.
4.
HalesCMCarrollMDFryarCD, et al. Prevalence of obesity among adults and youth: United States, 2015-2016. NCHS Data Brief2017: 1–8.
5.
YumukVTsigosCFriedM, et al. European guidelines for obesity management in adults [published correction appears in Obes Facts. 2016;9(1):64]. Obes Facts2015; 8: 402–424.
6.
LuigTAndersonRSharmaAM, et al. Personalizing obesity assessment and care planning in primary care: patient experience and outcomes in everyday life and health. Clin Obes2018; 8: 411–423.
7.
SullivanSKumarNEdmundowiczSA, et al. ASGE position statement on endoscopic bariatric therapies in clinical practice. Gastrointest Endosc2015; 82: 767–772.
8.
ASGE/ASMBS Task Force on Endoscopic Bariatric Therapy. A pathway to endoscopic bariatric therapies. Surg Obes Relat Dis2011; 7: 672–682.
9.
CurioniCCLourencoPM.Long-term weight loss after diet and exercise: a systematic review. Int J Obes2005; 29: 1168–1174.
10.
GreenwayFL.Physiological adaptations to weight loss and factors favouring weight regain. Int J Obes2015; 39: 1188–1196.
11.
MacleanPSBergouignanACornierMA, et al. Biology’s response to dieting: the impetus for weight regain. Am J Physiol Regul Integr Comp Physiol2011; 301: R581–R600.
12.
FamiliariPBoškoskiIMarcheseM, et al. Endoscopic treatment of obesity. Expert Rev Gastroenterol Hepatol2011; 5: 689–701.
13.
HillCKhashabMAKallooAN, et al. Endoluminal weight loss and metabolic therapies: current and future techniques. Ann N Y Acad Sci2018; 1411: 36–52.
14.
GómezVWoodmanGAbu DayyehBK.Delayed gastric emptying as a proposed mechanism of action during intragastric balloon therapy: results of a prospective study. Obesity2016; 24: 1849–1853.
15.
MionFNapoléonBRomanS, et al. Effects of intragastric balloon on gastric emptying and plasma ghrelin levels in non-morbid obese patients. Obes Surg2005; 15: 510–516.
16.
Mathus-VliegenEMde GrootGH.Fasting and meal-induce CCK and PP secretion following intragastric balloon treatment for obesity. Obes Surg2013; 23: 622–633.
17.
PopovVBOuASchulmanAR, et al. The impact of intragastric balloons on obesity-related co-morbidities: a systematic review and meta-analysis. Am J Gastroenterol2017; 112: 429–439.
18.
CreaNPataGDella CasaD, et al. Improvement of metabolic syndrome following intragastric balloon: 1 year follow-up analysis. Obes Surg2009; 19: 1084–1088.
19.
GencoALópez-NavaGWahlenC, et al. Multi-centre European experience with intragastric balloon in overweight populations: 13 years of experience. Obes Surg2013; 23: 515–521.
20.
SullivanSSwainJWoodmanG, et al. Randomized sham-controlled trial of the 6-month swallowable gas-filled intragastric balloon system for weight loss. Surg Obes Relat Dis2018; 14: 1876–1889.
21.
MachytkaEGaurSChuttaniR, et al. Elipse, the first procedureless gastric balloon for weight loss: a prospective, observational, open-label, multicenter study. Endoscopy2017; 49: 154–160.
22.
RaftopoulosIGiannakouA.The Elipse Balloon, a swallowable gastric balloon for weight loss not requiring sedation, anesthesia or endoscopy: a pilot study with 12-month outcomes. Surg Obes Relat Dis2017; 13: 1174–1182.
CourcoulasAAbu DayyehBKEatonL, et al. Intragastric balloon as an adjunct to lifestyle intervention: a randomized controlled trial. Int J Obes2017; 41: 427–433.
25.
PonceJWoodmanGSwainJ, et al. The REDUCE pivotal trial: a prospective, randomized controlled pivotal trial of a dual intragastric balloon for the treatment of obesity. Surg Obes Relat Dis2015; 11: 874–881.
26.
MachytkaEKlvanaPKornbluthA, et al. Adjustable intragastric balloons: a 12-month pilot trial in endoscopic weight loss management. Obes Surg2011; 21: 1499–1507.
27.
TateCMGeliebterA.Intragastric balloon treatment for obesity: review of recent studies. Adv Ther2017; 34: 1859–1875.
28.
SpyropoulosCKatsakoulisEMeadN, et al. Intragastric balloon for high-risk super-obese patients: a prospective analysis of efficacy. Surg Obes Relat Dis2007; 3: 78–83.
29.
TateCMGeliebterA.Intragastric balloon treatment for obesity: FDA safety updates. Adv Ther2018; 35: 1–4.
30.
StavrouGTsaousiGKotzampassiK.Life-threatening visceral complications after intragastric balloon insertion: is the device, the patient or the doctor to blame?Endosc Int Open2019; 7: E122–E129.
31.
VoelkerR.Deaths reported after intragastric balloon surgery. JAMA2017; 318: 996.
Abu DayyehBKNoarMDLavinT, et al. Pivotal randomized-controlled trial of the adjustable (SPATZ-3) Intragastric Balloon System For Weight Loss. Gastrointest Endosc2019; 89: AB58–AB59.
35.
JamalMHAlmutairiRElabdR, et al. The safety and efficacy of procedureless gastric balloon: a study examining the effect of elipse intragastric balloon safety, short and medium term effects on weight loss with 1-year follow-up post-removal. Obes Surg2019; 29: 1236–1241.
36.
AlsabahSAl HaddadEEkroufS, et al. The safety and efficacy of the procedureless intragastric balloon. Surg Obes Relat Dis2018; 14: 311–317.
MarinosGEliadesCRaman MuthusamyV, et al. Weight loss and improved quality of life with a nonsurgical endoscopic treatment for obesity: clinical results from a 3- and 6-month study. Surg Obes Relat Dis2014; 10: 929–934.
39.
SauerNRöschTPezoldJ, et al. A new endoscopically implantable device (SatiSphere) for treatment of obesity–efficacy, safety, and metabolic effects on glucose, insulin, and GLP-1 levels. Obes Surg2013; 23: 1727–1733.
AstrupAKristensenMGnessiL, et al. Oral administration of Gelesis100, a novel hydrogel, significantly decreases body weight in overweight and obese subjects. Presented at the Endocrine Society’s 96th annual meeting and expo, Chicago, IL, 21–24June2014, Abstract SUN-0897, https://endo.confex.com/endo/2014endo/webprogram/Paper13676.html
42.
GreenwayFLAronneLJRabenA, et al. A randomized, double-blind, placebo-controlled study of Gelesis100: a novel nonsystemic oral hydrogel for weight loss. Obesity2019; 27: 205–216.
43.
UrbanLEAudetDRonES, et al. Effect of a non-systemic, orally-administered hydrogel, GS100, on metformin pharmacokinetics. Can J Physiol Pharmacol2018; 96: 1127–1131.
AlqahtaniAAl-DarwishAMahmoudAE, et al. Short-term outcomes of endoscopic sleeve gastroplasty in 1000 consecutive patients. Gastrointest Endosc2019; 89: 1132–1138.
46.
Abu DayyehBKAcostaACamilleriM, et al. Endoscopic sleeve gastroplasty alters gastric physiology and induces loss of body weight in obese individuals. Clin Gastroenterol Hepatol2017; 15: 37–43.e1.
47.
SharaihaRZKediaPKumtaN, et al. Initial experience with endoscopic sleeve gastroplasty: technical success and reproducibility in the bariatric population. Endoscopy2015; 47: 164–166.
48.
SharaihaRZKumtaNASaumoyM, et al. Endoscopic sleeve gastroplasty significantly reduces bodymass index and metabolic complications in obese patients. Clin Gastroenterol Hepatol2017; 15: 504–510.
49.
Lopez-NavaGBautista-CastanoISharaihaRZ, et al. Endoscopic sleeve gastroplasty for obesity: a multicenter study of 248 patients with 24 months follow-up. Obes Surg2017; 27: 2649–2655.
50.
SartorettoASuiZHillC, et al. Endoscopic sleeve gastroplasty (ESG) is a reproducible and effective endoscopic bariatric therapy suitable for widespread clinical adoption: a large, international multicenter study. Obes Surg2018; 28: 1812–1821.
51.
BarrichelloSHourneaux de MouraDTHourneaux de MouraEG, et al. Endoscopic sleeve gastroplasty in the management of overweight and obesity: an international multicenter study. Gastrointest Endosc2019; 90: 770–780.
52.
Graus MoralesJCrespo PérezLMarquesA, et al. Modified endoscopic gastroplasty for the treatment of obesity. Surg Endosc2018; 32: 3936–3942.
53.
Lopez-NavaGGalvãoMPBautista-CastañoI, et al. Endoscopic sleeve gastroplasty for obesity treatment: two years of experience. Arq Bras Cir Dig2017; 30: 18–20.
54.
HedjoudjeADayyehBACheskinLJ, et al. Efficacy and safety of endoscopic sleeve gastroplasty: a systematic review and meta-analysis. Clin Gastroenterol Hepatol2020; 18: 1043–1053.e4.
55.
FayadLAdamASchweitzerM, et al. Endoscopic sleeve gastroplasty versus laparoscopic sleeve gastrectomy: a case-matched study. Gastrointest Endosc2019; 89: 782–788.
56.
NovikovAAAfanehCSaumoyM, et al. Endoscopic sleeve gastroplasty, laparoscopic sleeve gastrectomy, and laparoscopic band for weight loss: how do they compare?J Gastrointest Surg2018; 22: 267–273.
57.
EspinosJCTurróRMoragasG, et al. Gastrointestinal physiological changes and their relationship to weight loss following the POSE procedure. Obes Surg2016; 26: 1081–1089.
58.
SullivanSSwainJMWoodmanG, et al. 12 Month randomized sham controlled trial evaluating the safety and efficacy of targeted use of endoscopic suture anchors for primary obesity: the essential study. Gastroenterology2016; 150: S25–S26.
59.
MillerKTurroRGreveJW, et al. MILEPOST multicenter randomized controlled trial: 12-month weight loss and satiety outcomes after poseSM vs. medical therapy. Obes Surg2017; 27: 310–322.
60.
EspinosJCTurroRMataA, et al. Early experience with the incisionless operating platformTM (IOP) for the treatment of obesity: the primary obesity surgery endolumenal (pose) procedure. Obes Surg2013; 23: 1375–1383.
61.
Lopez-NavaGBautista-CastanoIJimenezA, et al. The primary obesity surgery endolumenal (POSE) procedure: one-year patient weight loss and safety outcomes. Surg Obes Relat Dis2015; 11: 861–865.
62.
GysBPlaekePLammeB, et al. Endoscopic gastric plication for morbid obesity: a systematic review and meta-analysis of published data over time. Obes Surg2019; 29: 3021–3029.
63.
KhanZKhanMAHajifathalianK, et al. Efficacy of endoscopic interventions for the management of obesity: a meta-analysis to compare endoscopic sleeve gastroplasty, AspireAssist, and primary obesity surgery endolumenal. Obes Surg2019; 29: 2287–2298.
64.
CohenRVOliveira da CostaMVCharryL, et al. Endoscopic gastroplasty to treat medically uncontrolled obesity needs more quality data: a systematic review. Surg Obes Relat Dis2019; 15: 1219–1224.
65.
HubertyVIbrahimMHiernauxM, et al. Safety and feasibility of an endoluminal-suturing device for endoscopic gastric reduction (with video). Gastrointest Endosc2017; 85: 833–837.
66.
HubertyVMachytkaEBoškoskiI, et al. Endoscopic gastric reduction with an endoluminal suturing device: a multicenter prospective trial with 1-year follow-up. Endoscopy2018; 50: 1156–1162.
67.
VerlaanTPaulusGFMathus-VliegenEM, et al. Endoscopic gastric volume reduction with a novel articulating plication device is safe and effective in the treatment of obesity (with video). Gastrointest Endosc2015; 81: 312–320.
68.
BierthoLLebelSHouldF, et al. Open, prospective study to evaluate the safety and preliminary effectiveness of the ACE™ stapler for the treatment of obesity. Gastrointest Endosc2016; 83: AB144.
69.
RodriguezLReyesEFagaldeP, et al. Pilot clinical study of an endoscopic, removable duodenal-jejunal bypass liner for the treatment of type 2 diabetes. Diabetes Technol Ther2009; 11: 725–732.
70.
TarnoffMRodriguezLEscalonaA, et al. Open label, prospective, randomized controlled trial of an endoscopic duodenal-jejunal bypass sleeve versus low calorie diet for pre-operative weight loss in bariatric surgery. Surg Endosc2009; 23: 650–656.
71.
GersinKSRothsteinRIRosenthalRJ, et al. Open-label, sham-controlled trial of an endoscopic duodenojejunal bypass liner for preoperative weight loss in bariatric surgery candidates. Gastrointest Endosc2010; 71: 976–982.
72.
SchoutenRRijsCSBouvyND, et al. A multicenter, randomized efficacy study of the EndoBarrier gastrointestinal liner for presurgical weight loss prior to bariatric surgery. Ann Surg2010; 251: 236–243.
73.
KoehestaniePde JongeCBerendsFJ, et al. The effect of the endoscopic duodenal-jejunal bypass liner on obesity and type 2 diabetes mellitus, a multicenter randomized controlled trial. Ann Surg2014; 260: 984–992.
74.
Abu DayyehBKKumarNEdmundowiczSA, et al. ASGE Bariatric Endoscopy Task Force systematic review and meta-analysis assessing the ASGE PIVI thresholds for adopting endoscopic bariatric therapies. Gastrointest Endosc2015; 82: 425–438.e5
75.
RohdeUHedbäckNGluudLL, et al. Effect of the EndoBarrier Gastrointestinal Liner on obesity and type 2 diabetes: a systematic review and meta-analysis. Diabetes Obes Metab2016; 18: 300–305.
76.
JirapinyoPHaasAVThompsonCC.Effect of the duodenal-jejunal bypass liner on glycemic control in patients with type 2 diabetes with obesity: a meta-analysis with secondary analysis on weight loss and hormonal changes. Diabetes Care2018; 41: 1106–1115.
77.
PatelSRMasonJHakimN.The duodenal-jejunal bypass sleeve (endobarrier gastrointestinal liner) for weight loss and treatment of type II diabetes. Indian J Surg2012; 74: 275–277.
78.
RubanAAshrafianHTeareJP.The EndoBarrier: Duodenal-Jejunal bypass liner for diabetes and weight loss. Gastroenterol Res Pract2018; 2018: 7823182.
79.
de MouraEGMartinsBCLopesGS, et al. Metabolic improvements in obese type 2 diabetes subjects implanted for 1 year with an endoscopically deployed duodenal-jejunal bypass liner. Diabetes Technol Ther2012; 14: 183–189.
80.
Zechmeister-KossIHuićMFischerS.The duodenal-jejunal bypass liner for the treatment of type 2 diabetes mellitus and/or obesity: a systematic review. Obes Surg2014; 24: 310–323.
81.
BetzelBDrenthJPHSiersemaPD.Adverse events of the duodenal-jejunal bypass liner: a systematic review. Obes Surg2018; 28: 3669–3677.
82.
QuezadaNMuñozRMorelliC, et al. Safety and efficacy of the endoscopic duodenal-jejunal bypass liner prototype in severe or morbidly obese subjects implanted for up to 3 years. Surg Endosc2018; 32: 260–267.
CarranoFMPeevMPSaundersJK, et al. The role of minimally invasive and endoscopic technologies in morbid obesity treatment: review and critical appraisal of the current clinical practice. Obes Surg2020; 30: 736–752.
85.
SandlerBJRumbautRSwainCP, et al. Human experience with an endoluminal, endoscopic, gastrojejunal bypass sleeve. Surg Endosc2011; 25: 3028–3033.
86.
SandlerBJRumbautRSwainCP, et al. One-year human experience with a novel endoluminal, endoscopic gastric bypass sleeve for morbid obesity. Surg Endosc2015; 29: 3298–3303.
87.
RajagopalanHCherringtonADThompsonCC, et al. Endoscopic duodenal mucosal resurfacing for the treatment of Type 2 diabetes: 6-month interim analysis from the first-in-human-proof-of-concept study. Diabetes Care2016; 39: 2254–2261.
88.
van BaarACGHollemanFCrenierL, et al. Endoscopic duodenal mucosal resurfacing for the treatment of type 2 diabetes mellitus: one year results from the first international, open-label, prospective, multicentre study. Gut2020; 69: 295–3303.
MachytkaEBužgaMZoncaP, et al. Partial jejunal diversion using an incisionless magnetic anastomosis system: 1-year interim results in patients with obesity and diabetes. Gastrointest Endosc2017; 86: 904–912.
SullivanS.Aspiration therapy for obesity. Gastrointest Endosc Clin N Am2017; 27: 277–288.
93.
Thompson CCAbuDayyehBKKushnerR, et al. Percutaneous gastrostomy tube device for the treatment of class II and class III obesity: results of a randomized controlled trial. Am J Gastroenterol2017; 112: 447–457.
94.
NyströmMMachytkaENorénE, et al. Aspiration therapy as a tool to treat obesity: 1- to 4-year results in a 201-patient multi-center post-market European registry study. Obes Surg2018; 28: 1860–1868.
95.
ThompsonCCAbu DayyehBKKushnirV, et al. Aspiration therapy for the treatment of obesity: 4-year results of a multicenter randomized controlled trial. Surg Obes Relat Dis2019; 15: 1348–1354.
96.
García-CompeanDMaldonado GarzaH.Intragastric injection of botulinum toxin for the treatment of obesity. Where are we?World J Gastroenterol2008; 14: 1805–1809.
97.
FoschiDLazzaroniMSangalettiO, et al. Effects of intramural administration of botulinum toxin A on gastric emptying and eating capacity in obese patients. Dig Liver Dis2008; 40: 667–672.
98.
BustamanteFBrunaldiVOBernardoWM, et al. Obesity treatment with Botulinum Toxin-A is not effective: a systematic review and meta-analysis. Obes Surg2018; 27: 2716–2723.
99.
de MouraEGHRibeiroIBFrazãoMSV, et al. EUS-guided intragastric injection of Botulinum Toxin A in the preoperative treatment of super-obese patients: a randomized clinical trial. Obes Surg2019; 29: 32–39.
100.
DargentJMionFCostilV, et al. Multicenter randomized study of obesity treatment with minimally invasive injection of hyaluronic acid versus and combined with intragastric balloon. Obes Surg2015; 25: 1842–1847.
101.
YumukVFrühbeckGOppertJM, et al. An EASO position statement on multidisciplinary obesity management in adults. Obes Facts2014; 7: 96–101.
102.
SauerlandSAngrisaniLBelachewM, et al. Obesity surgery: evidence-based guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc2005; 19: 200–221.
103.
FriggAPeterliRZynamonA, et al. Radiologic and endoscopic evaluation for laparoscopic adjustable gastric banding: preoperative and follow-up. Obes Surg2001; 11: 594–599.
104.
HainerVToplakHMitrakouA.Treatment modalities of obesity: what fits whom?Diabetes Care2008; 31(Suppl. 2): S269–S277.
105.
SarwerDBWaddenTAFabricatoreAN.Psychosocial and behavioral aspects of bariatric surgery. Obes Res2005; 13: 639–648.
106.
GrossCMvan ElstLT.Psychological and psychiatric contraindications. In: KarczWKThomuschO (eds) Principles of metabolic surgery. Berlin: Springer, 2012, pp. 153–157.
107.
FriedMYumukVOppertJM, et al. Interdisciplinary European guidelines on metabolic and bariatric surgery. Obes Surg2014; 24: 42–55.
108.
MahonyD.Psychological assessments of bariatric surgery patients. Development, reliability, and exploratory factor analysis of the PsyBari. Obes Surg2011; 21: 1395–1406.
109.
BusettoLDickerDAzranC, et al. Practical recommendations of the Obesity Management Task Force of the European Association for the Study of Obesity for the Post-Bariatric Surgery Medical Management. Obes Facts2017; 10: 597–632.
110.
WaddenTAButrynMLSarwerDB, et al. Comparison of psychosocial status in treatment-seeking women with class III vs. class I-II obesity. Obesity2006; 14(Suppl. 2): 90S–98S.
111.
KotzampassiKGrosomanidisVPapakostasP, et al. 500 intragastric balloons: what happens 5 years thereafter?Obes Surg2012; 22: 896–903.
112.
WeinerRGutberletHBockhornH.Preparation of extremely obese patients for laparoscopic gastric banding by gastric balloon therapy. Obes Surg1999; 9: 261–264.
113.
BallWRazaSSLoyJ, et al. Effectiveness of intra-gastric balloon as a bridge to definitive surgery in the super obese. Obes Surg2019; 29: 1932–1936.