
Abstract
Background:
Endoscopic ultrasound–guided cystogastrostomy has become the first-line treatment for symptomatic peripancreatic fluid collections. The aim of this study is to analyze the efficacy and safety of cystogastrostomy via a meta-analysis of the literature.
Methods:
We performed a systematic search of PubMed and Medline databases for studies published from January 2005 to May 2018. We included randomized controlled trials along with retrospective and prospective observational studies reporting endoscopic ultrasound–guided cystogastrostomy stent placement for peripancreatic fluid collections. The primary outcome for our meta-analysis was complete peripancreatic fluid collection resolution on imaging. Our secondary outcomes included comparative efficacy and safety of the procedure for pseudocysts and walled-off pancreatic necrosis using metal and plastic stents.
Results:
Seventeen articles involving 1708 patients met our inclusion criteria for meta-analysis. Based upon the random effects model, the pooled technical success rate of cystogastrostomy was 88% (95% confidence interval = 83–92 with I2 = 85%). There was no difference in the technical success rate between pancreatic pseudocysts and walled-off pancreatic necrosis (91% and 86%, respectively p = nonsignificant). The adverse event rates for metal and plastic stents were equivalent (14% and 18%, respectively, p = nonsignificant).
Conclusion:
Endoscopic ultrasound–guided cystogastrostomy stents are effective in the treatment of pancreatic pseudocysts and walled-off pancreatic necrosis. We found no difference in technical success or adverse event rates of drainage based on peripancreatic fluid collection type or stent used.
Introduction
Hospital admissions due to acute pancreatitis have increased over 20% worldwide and over 50% in the United States during the past 20 years. 1 , 2 Peripancreatic fluid collections (PFCs) are common complication of acute and chronic pancreatitis. According to the 2012 revised Atlanta classification, PFCs are categorized into four subtypes: (1) acute peripancreatic fluid collections (APFC); (2) pancreatic pseudocysts (PP), which typically develop after 4 weeks of acute pancreatic injury; (3) acute necrotic collections (ANCs), which occur during the early phase of necrotizing pancreatitis prior to demarcation; and (4) walled-off pancreatic necrosis (WOPN). 3 Although WOPN also takes 4 weeks to develop, unlike the purely liquid PPs, it contains solid material. PPs are the most common of the chronic PFCs and arise in 5–16% of acute pancreatitis cases, 20–40% of chronic pancreatitis cases, and in 30–40% of alcohol-induced chronic pancreatitis. 4 , 5
While APFCs and ANCs tend to resolve on their own without requiring treatment, a significant portion of PPs and WOPN do not resolve spontaneously and can lead to sepsis and hemorrhage. 6 PP and WOPN drainage has historically been via surgery, which is efficacious yet risky, as evidenced by significant adverse events (AEs) occurring in up to 30% of cases. 7 Endoscopic ultrasound (EUS)–guided cystogastrostomy, which is performed via creation of a fistulous tract through either the stomach or duodenum and the cavity of the PFC, has largely supplanted surgery for treatment of symptomatic PFCs due to comparable efficacy without the high risk of complications.8–11 In addition, EUS-guided cystogastrostomy has been shown to reduce the total mean cost of PFC treatment by more than 50% and provide shorter hospital stay when compared with surgical cystogastrostomy. 10
Although many studies have examined the efficacy of cystogastrostomy for PFC treatment, there have been few comprehensive analyses comparing the safety and efficacy of the procedure for PPs and WOPN. 12 The aim of this study is to assess the technical efficacy and safety of EUS-guided cystogastrostomy for both types of PFCs when done with plastic or metal stents.
Methods
Search strategy and eligibility criteria
Two authors (B.R. and D.J.) conducted an independent search of Medline and PubMed databases for articles from January 2005 to May 2018. The search terms used were ‘pancreatic pseudocyst’ OR ‘pancreatic fluid collection’ OR ‘walled-off necrosis’ AND ‘endosonography’ OR ‘cystogastrostomy’ OR ‘cystogastrostomy outcome’ OR ‘cystogastrostomy trial’. Articles were considered eligible if EUS-guided cystogastrostomy was performed to drain a PFC without prior surgical manipulation. We included prospective and retrospective cohort studies along with randomized controlled trials. Articles were excluded if they lacked full-text publication, were not in English, were done on non-human subjects, lacked clear definition of technical success, included only clinical symptom improvement as the primary outcome, or involved fewer than five patients. If there was a disagreement between the two authors regarding an article category, a third author (M.A.) would mediate and make the final decision. Articles were selected for analysis in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 13 Because this study involved only de-identified data that were already published, it was approved and received exempt status from the institutional review board (IRB) committee of New York-Presbyterian Brooklyn Methodist Hospital (IRB 1227161-1). As a result, our study did not require informed consent.
Data extraction and target outcome
Data extraction was uniform for all studies. We collected the total number of patients, sex, age, type of PFC (WOPN or PP), type of stent used, AE rate, clinical success, and surveillance period. Our target outcome was overall technical success of cystogastrostomy defined as complete radiographic resolution of PFC. Secondary outcomes were comparisons of efficacy and safety between PP and WOPN as well as between metal and plastic stents. Safety was assessed by AEs reported. The AEs included stent migration, bleeding, and infection, among others. We identified 17 studies suitable for analysis (Figure 1).

PRISMA diagram.
Data analysis
Forest plots containing fixed and random effect models were generated for each outcome of interest. Outcomes were presented via pooled means and 95% confidence intervals (CI). A p-value > 0.05 would be considered nonsignificant (NS). A meta-regression model for overall success and AE rates of metal and plastic stents was conducted. Odds ratios (ORs) with p-value were generated for secondary outcomes involving metal and plastic stents. Heterogeneity between studies was tested via I2 statistic of Higgins. 14 An I2 ⩾ 50% with a p-value < 0.1 was considered significant and required interpretation from the random effects model. Funnel plots were used to assess for publication bias and Eggers regression test was used to evaluate publication bias quantitatively. 15 All data analyses were conducted on R Core Team (2018), Version 3.4.2 (Vienna, Austria).
Results
Study selection
We identified 160 articles via PubMed/Medline. We excluded 91 of these based on title or abstract, another 31 due to inadequate data for analysis, and 21 more for miscellaneous reasons ranging from unclear or contrasting outcomes to missing data required for analysis. We ultimately found 17 articles involving 1708 patients who met our inclusions for analysis (Figure 1).16–32 If a study involved patients being treated with metal stents and others with plastic stents, then we separated the groups in our analysis, hence some being listed twice (Table 1). We excluded a total of 59 patients who had been treated with plastic stents through metal stents from our final analysis.
Overview of included studies.

PFC: peripancreatic fluid collection; PP: pancreatic pseudocyst; WOPN: walled-off pancreatic necrosis.
Most articles defined technical success as complete radiographic resolution of the PFC after cystogastrostomy (Table 1). To maintain uniformity across studies, articles with contrasting or unclear outcomes were excluded from analysis.
Efficacy and safety
Based upon the random effects model, the pooled technical success rate of cystogastrostomy was 88% [95% confidence interval (CI) = 83–92% with I2 = 85%] as seen in Figure 2. There was no statistically significant difference in the technical success rate of PP or WOPN (91% versus 86%, respectively, p = NS) as shown in Figures 3 and 4. We also found no difference in PP drainage efficacy between metal stents or plastic stents (91% for both; Figure 5) or in that for WOPN drainage by stent type (89% versus 83%, respectively, p = NS; Figure 6). There was no difference in overall AE rates between metal and plastic stents (14% versus 18%, respectively, p = NS; Figures 7 and 8).

Pooled overall efficacy for cystogastrostomy in PPs and WOPN.

Pooled efficacy for cystogastrostomy in PPs.

Pooled efficacy for cystogastrostomy in WOPN.
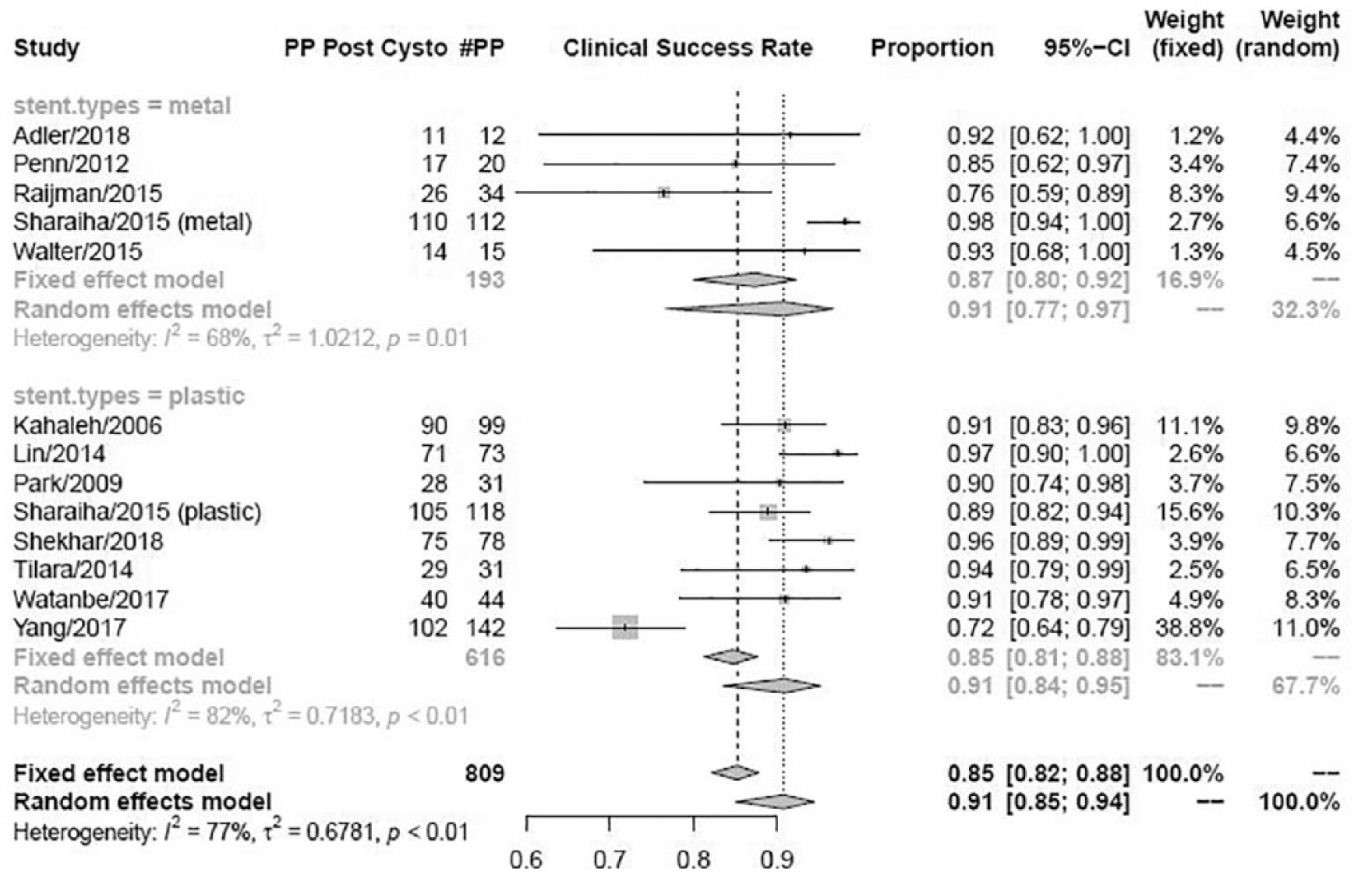
Cystogastrostomy efficacy for PP by stent type.

Cystogastrostomy efficacy for WOPN by stent type.
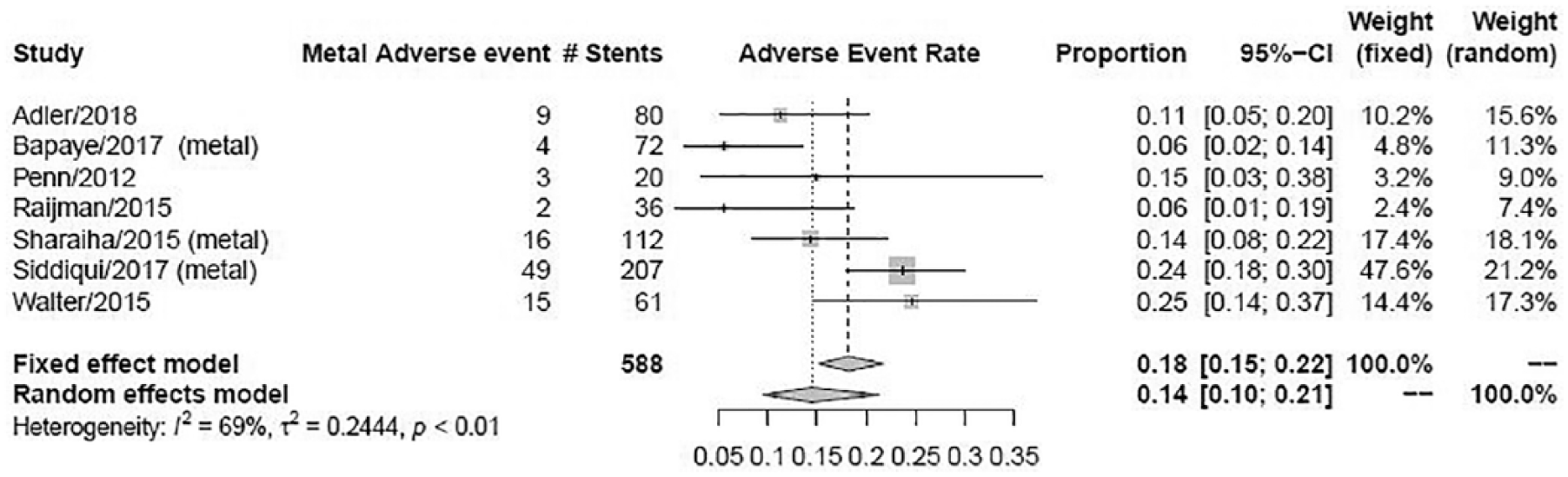
Pooled adverse events for metal stents.

Pooled adverse events for plastic stents.
Heterogeneity and publication bias
There was significant heterogeneity among the studies collected as evidenced by the I2 values > 50% in our Forest plots and in Figure 9. We attributed this to the large number of retrospective studies, the small number of prospective studies, and variability in outcomes such as length of time to imaging resolution. As such, our data interpretation was done via random effect models. We also found evidence of publication bias as shown on our funnel plot (Figure 10).

Heterogeneity plot.
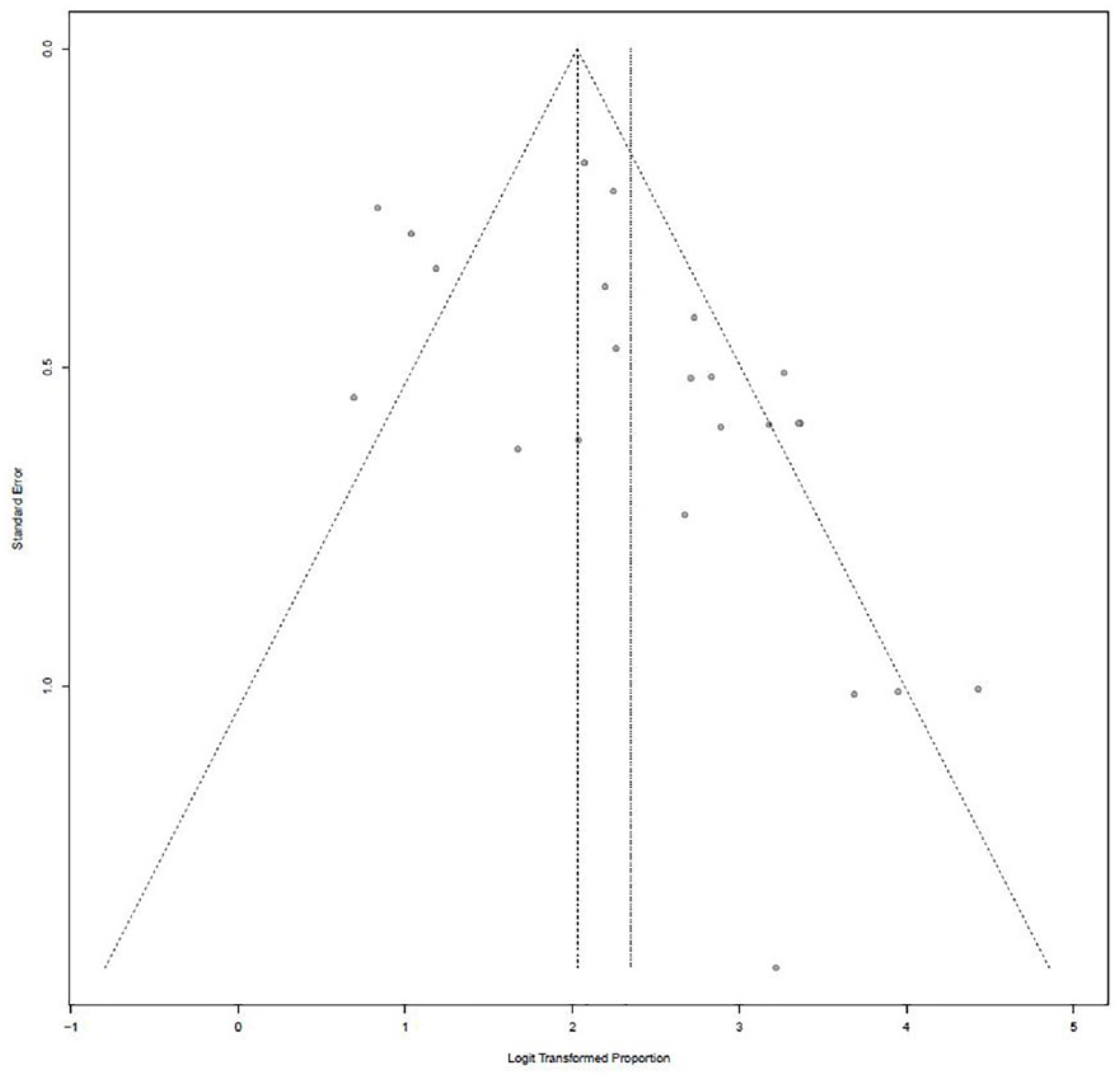
Funnel plot for publication bias.
Discussion
EUS-guided cystogastrostomy has become the standard therapy for symptomatic PFCs and our meta-analysis reinforces the documented efficacy of this treatment. We found the cumulative technical success of EUS-guided cystogastrostomy for PPs and WOPN to be 88%. This is consistent with findings in the literature which typically show success rates ranging from 75–95%. 26 , 33 Although others have noted decreased efficacy for WOPN compared with PP, 33 we found no significant difference in outcomes between these PFC types. We anticipate that continued technological advances in equipment and imaging will further enhance efficacy of EUS-guided drainage irrespective of PFC subtype.
We found no significant difference in efficacy between metal and plastic stents. The newer lumen-apposing self-expandable metallic stent (LASEMS) has gained widespread acclaim given ease of use and improved efficacy with PFC drainage. In a recent literary review involving 298 cases, Patil and colleagues 34 report that LASEMS has a 96% clinical success rate, which they defined as resolution of symptoms, and a 97% technical success rate, defined as complete radiographic resolution of PFC. In their single center retrospective study, Fasullo and colleagues 35 found that LASEMS reduced interval resolution of PFC after stent placement by nearly half when compared with plastic stents, but they did not find any difference in AE rates. The authors concluded that LASEMS was preferable to plastic stent but that prospective studies would be needed to confirm their findings.
A recent meta-analysis comparing efficacy and safety of PFC with lumen-apposing metal stents (LAMS) and plastic stents among 11 studies (N = 688) found no difference in technical success between LAMS and plastic stents, although fewer AEs were noted compared with plastic stents. 36 We found comparable efficacy between both stent types, but did not identify a clear safety advantage to LAMS. Our findings are similar to Bang and colleagues 37 who found no difference in AE between stent types and in contrast to Saunders and colleagues 12 who found that metal stents had fewer AEs than plastic ones. Varadarajulu and colleagues 38 found that complications of cystogastrostomy include perforation, stent migration, bleeding, and infection. Although complications were relatively rare, they resulted in emergency surgery, repeat endoscopy, prolonged hospitalization, and even death. As such, the reduction in post-stent placement AE reduces overall morbidity, hospital stay, and treatment cost. 18 Although we favor LASEMS in our own practice, we acknowledge that plastic stents are effective and safe alternatives.
Limitations
The limitations of this study are largely related to incorporation of observational studies, which lends itself to heterogeneity and selection bias. Although we could mitigate heterogeneity via use of random effects models, we could not eliminate it entirely from our analyses. We did not differentiate between the types of metal or plastic stents, nor did we include the 59 patients from the listed studies who had gotten plastic stents through metal ones. We did not distinguish between articles that used single or multiple stents. Patients who had multiple stents or specific types of metal or plastic stents may have had different outcomes, but these patients were not consistently analyzed separately within the included studies. The paucity of multi-arm prospective trials in this topic increases risk of selection and publication bias. We attempted to address this by identifying studies with clear technical target outcomes, but we concede that the biases may remain. Finally, the experience of the endoscopists placing the stents was not assessed given lack of reporting in the manuscripts.
Strengths
This study was able to effectively analyze technical outcomes of PFC drainage by both patient factors (PFC subtype) and procedure variables (stent subtype). Few studies have provided comparative data and even fewer have reported outcomes in a comprehensive meta-analysis format.
Conclusion
The shortcomings notwithstanding, our study is one of the most comprehensive meta-analyses on this topic to date and it adds to the substantial body of evidence highlighting the efficacy and safety of EUS-guided cystogastrostomy for PP and WOPN. Our study likewise supports the use of metal and plastic stents given the similar safety and efficacy profile. Additional multi-arm prospective trials are needed to compare the safety and efficacy of novel metal and plastic stents among PFCs given the relatively sparse data. We look forward to further studies into this important topic.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.