
Abstract
Background
Non-small cell lung cancer (NSCLC) remains a major contributor to cancer-related deaths, with chemotherapy offering limited survival gains. Motesanib, a multi-targeted angiogenesis inhibitor, was studied in combination with carboplatin and paclitaxel (C/P) for NSCLC therapy. Nonetheless, inconsistent efficacy outcomes and notable side effects resulted in its withdrawal. This meta-analysis investigates the tolerability of motesanib + C/P versus placebo or bevacizumab in NSCLC patients.
Objectives
To determine the safety profile of motesanib + C/P in NSCLC, with a focus on adverse events (AEs) associated with treatment.
Methods
Relevant studies were sought by conducting searches in databases such as PubMed, Cochrane, Scopus, Google Scholar, and clinicaltrials.gov. Four randomized controlled trials (RCTs) were carried out with a total of 1,945 participants. Cochrane tools were used to assess bias, and statistical evaluation was conducted using RevMan 5.3.
Results
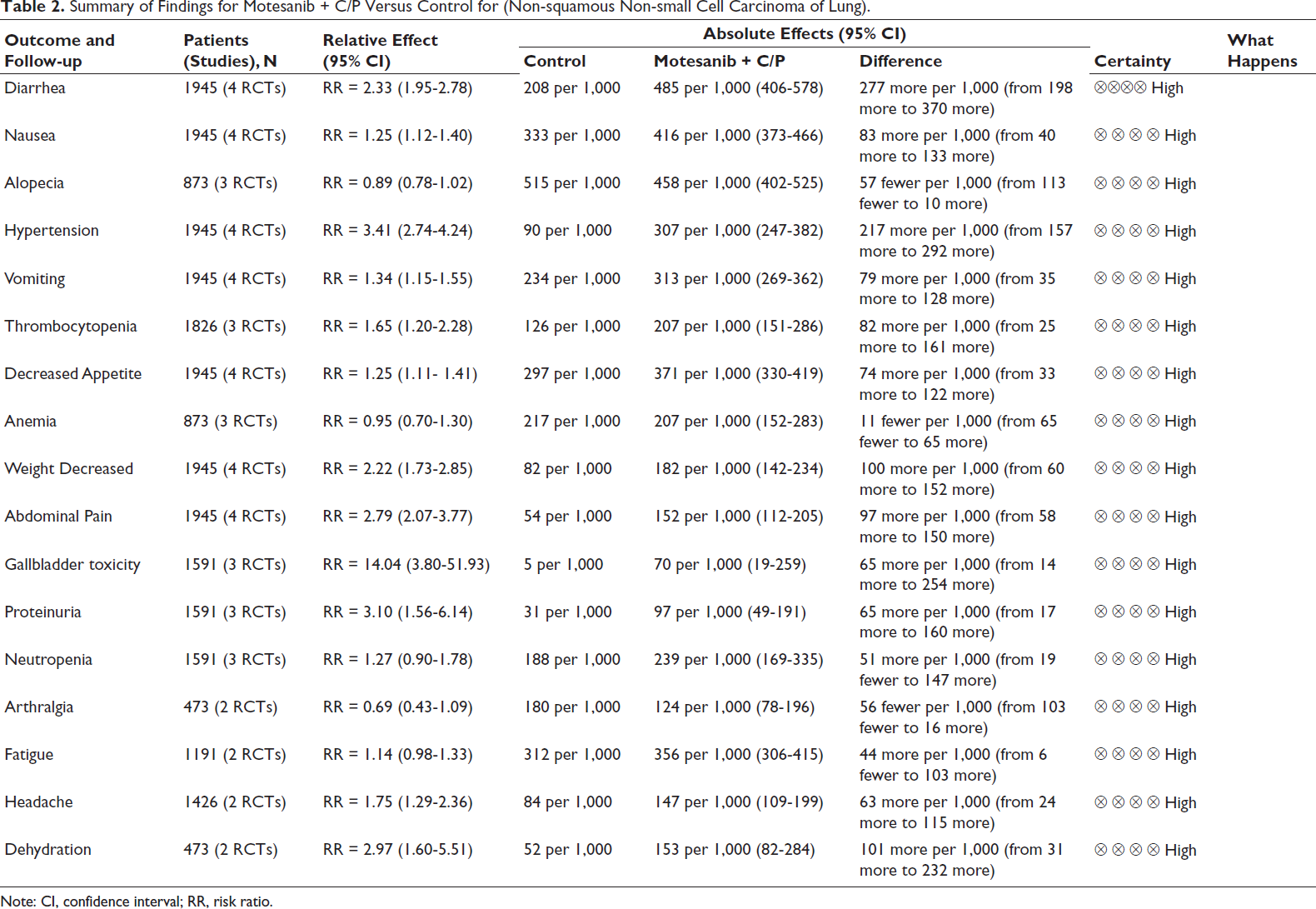
Motesanib did not significantly improve OS or PFS compared to placebo. However, it showed a higher likelihood of hypertension (RR = 3.41, 95% CI [2.74-4.24]), gallbladder toxicity (RR = 14.04, 95% CI [3.80-51.93]), diarrhea (RR = 2.33, 95% CI [1.95-2.78]), vomiting (RR = 1.34, 95% CI [1.15-1.55]), weight loss (RR = 2.22, 95% CI [1.73-2.85]), dehydration (RR = 2.97, 95% CI [1.60-5.51]), as well as proteinuria (RR = 3.10, 95% CI [1.56-6.14]).
Conclusions
Motesanib does not provide a survival advantage over standard treatments and poses significant safety concerns, particularly regarding cardiovascular and gastrointestinal toxicity. These findings emphasize the need for cautious clinical use and further research into safer angiogenesis inhibitors for NSCLC. The findings are based on a limited number of RCTs (four studies), which should be considered when interpreting the results.
Introduction
NSCC, particularly adenocarcinoma, generally has a better prognosis than squamous cell carcinoma. Studies indicate that patients with Stage IA NSCC have improved overall survival (OS) rates compared to those with squamous cell carcinoma. 1 Moreover, NSCC exhibits diverse molecular alterations, which are critical for personalized treatment strategies. For instance, the identification of specific mutations can guide targeted therapy decisions. 2
However, despite the lack of efficacy in non-small cell lung cancer (NSCLC), motesanib has shown promise in other cancers. For example, in cisplatin-resistant bladder cancer cells, motesanib exhibits synergistic antitumor effects when combined with cisplatin, inducing apoptosis and cell cycle arrest. 3 Although the development of resistance to motesanib is a potential limitation to its clinical use. In some tumor models, resistance may arise due to compensatory signaling pathways or mutations in target kinases. However, preclinical studies suggest that combining motesanib with other targeted therapies, such as COX-2 inhibitors, may overcome resistance and enhance antitumor effects. 4
In patients with Stage IIIA non-squamous NSCLC, the combination of neoadjuvant bevacizumab and platinum-based chemotherapy significantly improved disease-free survival (DFS), though it did not increase the rates of pathological complete response (pCR). 5 The combination of bevacizumab with chemoradiotherapy enhances levels of VEGF, bFGF, and Let-7, leading to improved therapeutic outcomes in patients with NSCLC. 6 In addition, the development of bevacizumab-loaded nano dispersions for targeted drug delivery in NSCLC has shown potential, with efficient drug release and safety profiles, suggesting a promising approach for enhancing therapeutic efficacy. 7
NSCLC remains a significant contributor to cancer-related mortality, with minimal survival advantages obtained from conventional chemotherapy. Motesanib, an angiogenesis inhibitor, has been assessed in conjunction with carboplatin and paclitaxel (C/P). However, inconsistent findings concerning its efficacy and safety, coupled with notable adverse effects, have resulted in its discontinuation. This meta-analysis evaluates the efficacy and safety of motesanib in comparison to placebo or bevacizumab (B), concentrating on endpoints including OS, progression-free survival (PFS), objective response rate (ORR), adverse events (AEs), and treatment-related toxicities.
Despite its discontinuation, motesanib underwent extensive clinical trials, revealing significant adverse effects. Understanding these toxicities is crucial for evaluating kinase inhibitors’ safety profiles and guiding future drug development. This meta-analysis synthesizes available data to highlight key safety concerns that contributed to motesanib’s clinical failure.
Patients and Methods
Sources of Data and Methodology for Search
An exhaustive search was conducted across the PubMed, Cochrane Library, Scopus, Google Scholar, and ClinicalTrials.gov databases from their inception until March 2025. The search strategy included keywords and Medical Subject Headings (MeSH) terms, such as:
(“Non-Small Cell Lung Cancer” OR “NSCLC” OR “Carcinoma, Non-Small-Cell Lung” [MeSH] OR “Non-Small Cell Lung Cancer” OR NSCLC) AND (motesanib OR “motesanib” OR “Indazoles” [MeSH]) AND (Carboplatin OR “Carboplatin”[MeSH]) AND (Paclitaxel OR “Paclitaxel” [MeSH]) AND (“Placebo” OR “Placebos” [MeSH] OR Bevacizumab OR “Bevacizumab” [MeSH]) AND (“Overall Survival” OR “Progression-Free Survival” OR “Objective Response Rate” OR “Adverse Events” OR “Survival Rate” [MeSH] OR “Disease-Free Survival” [MeSH] OR “Treatment Outcome” [MeSH] OR “Adverse Effects” [MeSH]). Searches in PubMed utilized both MeSH terms and free-text words.
The study selection followed the PICO framework: patients (P) included those diagnosed with NSCLC; interventions (I) involved the administration of motesanib in combination with C/P (motesanib + C/P); controls (C) were patients receiving a placebo or no additional treatment; and outcomes (O) focused on the AEs associated with motesanib + C/P therapy. In this meta-analysis, only articles that were published in English were taken into account.
Selection Criteria
The analysis employed specific inclusion criteria: (a) randomized controlled trials (RCTs) assessing the efficacy of motesanib in conjunction with C/P (motesanib + C/P) against a placebo; (b) studies involving patients with a diagnosis of NSCLC; (c) trials that included participants without significant comorbidities; (d) for crossover studies, only data from the initial randomization phase were utilized to prevent carryover effects; and (e) RCTs that explicitly reported adverse outcomes pertinent to this meta-analysis.
The exclusion criteria included: (a) clinical trials that did not specifically target NSCLC patients or involved participants with substantial comorbidities; (b) studies that did not assess motesanib + C/P as the exclusive intervention; and (c) trials that enrolled fewer than nine patients in each treatment arm. Moreover, observational studies, such as case-control studies, retrospective or prospective cohorts, and cross-sectional analyses, along with peer-reviewed articles, commentaries, editorials, letters to the editor, and case reports, were excluded.
Selection Process
The titles and abstracts of all identified studies were thoroughly evaluated by two independent authors to ensure that they satisfied the inclusion criteria. Full-text versions of potentially eligible articles were then assessed independently by the same two reviewers. Key details extracted included the main characteristics of each trial, the therapeutic interventions used, and the reported outcomes.
Outcome Measures
To evaluate the safety of the intervention, the incidence of adverse effects was assessed and compared between the intervention and placebo groups. AEs recorded included diarrhea, nausea, vomiting, decreased appetite, weight loss, gallbladder toxicity, neutropenia, headache, and fatigue. Data extraction was performed 4 weeks after the intervention.
Data Extraction
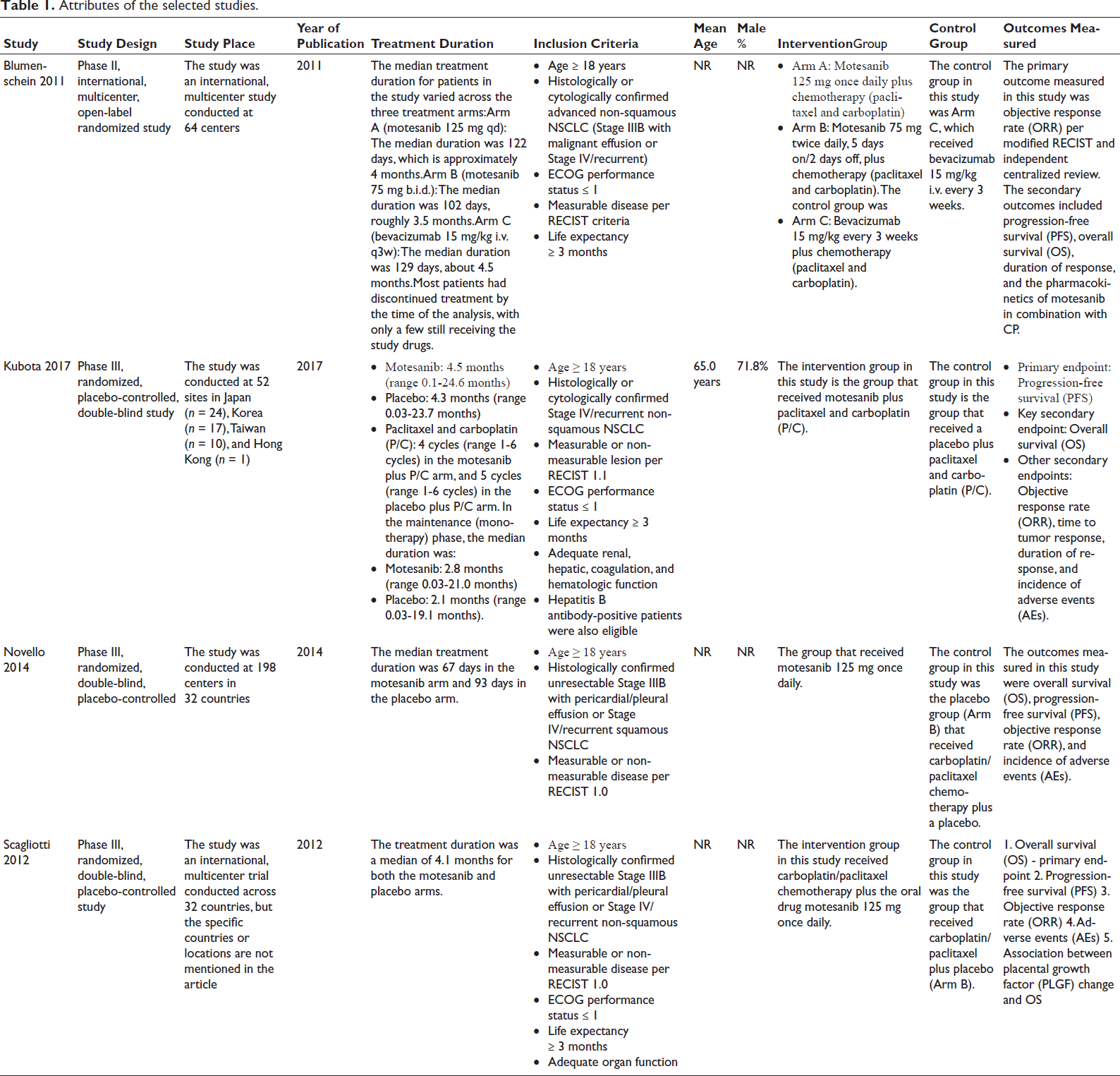
Data were independently extracted by two authors using standardized extraction forms. Information on the outcomes, as previously described, was collected from relevant graphs and tables. Patient demographics and characteristics, such as mean age and sex, from the included studies were summarized in tabular form (Table 1).
Attributes of the selected studies.
Quality Assessment
The methodological quality of the included trials was independently assessed by two authors using Version 2 of the Cochrane risk of bias instrument for randomized trials (RoB 2). 8 Potential selection, attrition, allocation, and reporting biases were the primary focus of the evaluation. Any discrepancies between examiners were resolved through discussion or, if necessary, by consulting with a third reviewer.
Statistical Analysis
The meta-analysis was conducted using the protocols specified in the Cochrane Handbook for Systematic Reviews of Interventions. 9 The reporting adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria, with the checklist included at the conclusion of the publication. 10
All statistical analyses were conducted utilizing RevMan 5.3 software (Cochrane Management System). 11 Standardized mean differences (SMD) or mean differences (MD) with 95% confidence intervals (CI) were computed for continuous outcomes.
A P value below .05 was deemed statistically significant unless stated differently. Intention-to-treat populations were included whenever applicable. The I2 statistic was employed to evaluate heterogeneity among the studies. 9
Results
Literature Review
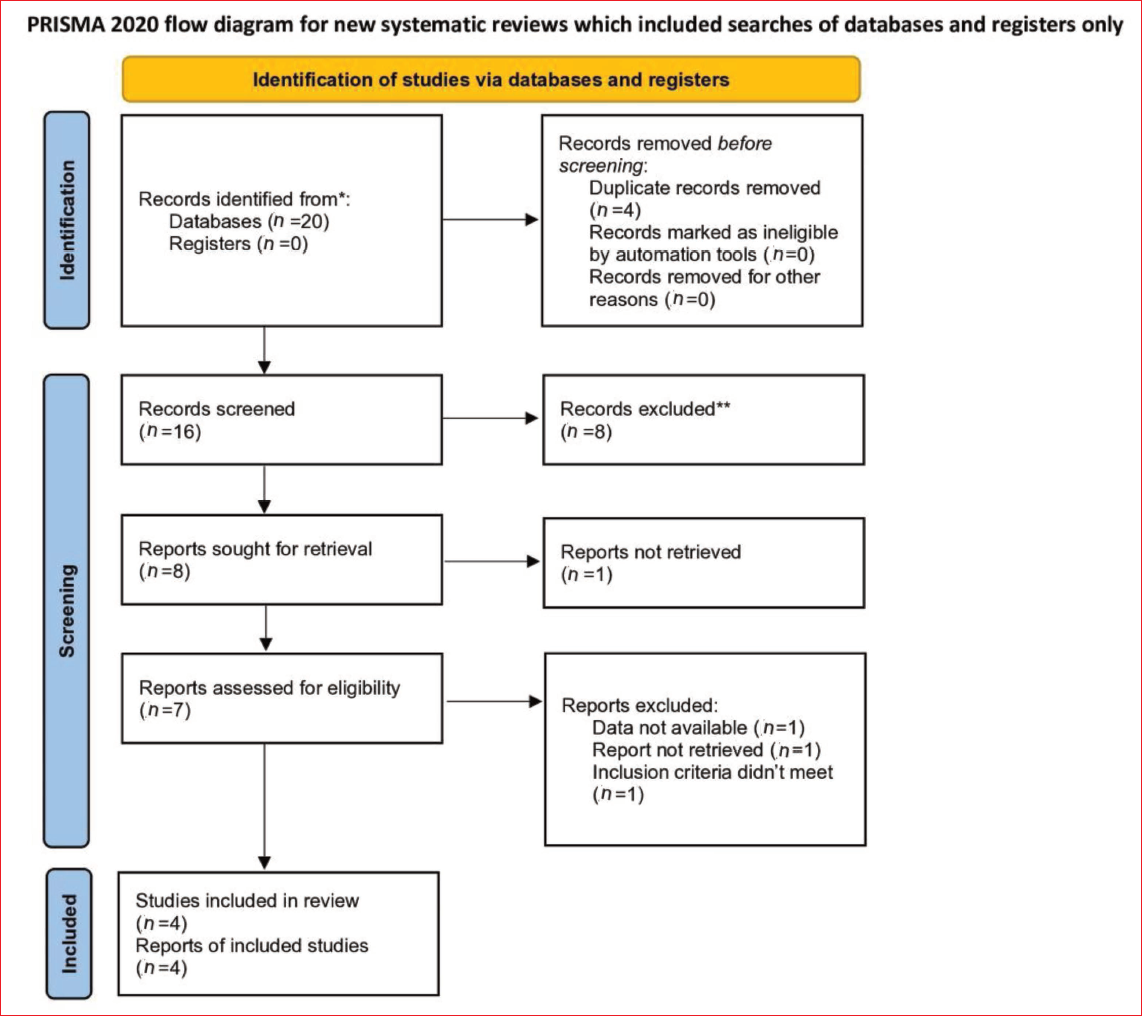
A thorough examination of electronic databases, encompassing all information until March 2025, initially identified 20 articles. After removing four duplicate entries, 16 records remained. Title and abstract screening resulted in the exclusion of eight articles. The whole texts of the remaining eight articles were obtained for thorough assessment. One study was excluded due to the inability to obtain the necessary data. Of the seven reports assessed for eligibility, three were excluded because of unavailable data, inability to retrieve reports, or failure to meet the inclusion criteria. Ultimately, four RCTs were chosen for inclusion. The selection procedure is depicted in the PRISMA flow diagram (Figure 1).
PRISMA 2020 Flow Diagram for the Systematic Review. This PRISMA (Preferred Reporting Items for Systematic Review and Meta-analyses) Flow Diagram Illustrates the Process of Identifying, Screening, and Including Studies for the Systematic Review and Meta-analyses. The Diagram Consists of Four Main Phases: Identification, Screening, Eligibility, and Inclusion. The Number of Studies Involved in Each Phase Are Shown in the Figure.
Attributes of Recognized Studies
The attributes of the four studies considered are encapsulated in Table 1. All studies were published between 2011 and 2017.
Quality Assessment
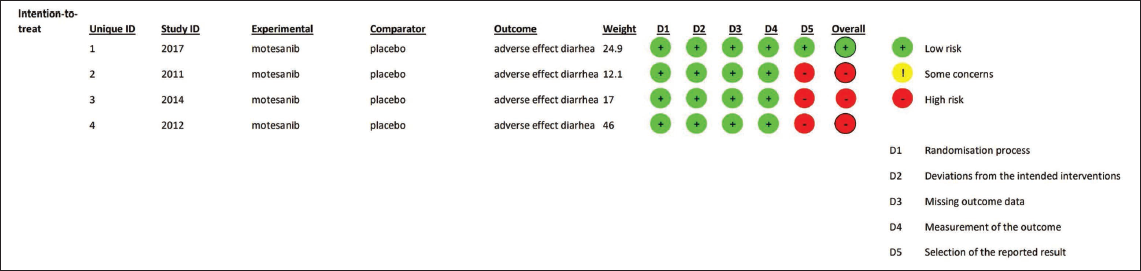
The comprehensive quality of the incorporated studies was assessed utilizing the Cochrane Risk of Bias Tool. The studies often show a minimal risk of bias. Figure 2 presents a comprehensive summary of the assessment outcomes.
Risk of Bias Summary for Included Studies. This Figure Represents the Risk of Bias Assessment for Included Studies. The Risk of Bias Was Evaluated by the Cochrane Risk of Bias 2.0 Tool, and the Results Are Summarized in the Figure. The Detailed Assessment for Each Domain Is Visually Represented Using Colored Circles Indicating the Level of Risk. Green: Low Risk. Yellow: Some Concerns. Red: High Risk. D1: Randomization Process, D2: Deviations from the Intended Interventions. D3: Missing Outcome Data, D4: Measurement of the Outcome. D5: Selection of the Reported Result.
Results of Synthesis
Four RCTs, encompassing a total of 1,945 patients with recurrent or Stage III/IV non-squamous non-small cell lung carcinoma, were included in the synthesis to assess the safety profile of motesanib in combination with C/P regarding OS and PFS. In all studies, participants received a consistent dose of 125 mg motesanib alongside C/P. Treatment duration was monitored at specified intervals, with evaluations conducted every 6 weeks across the studies. Overall, the findings were statistically insignificant, with motesanib associated with a higher incidence of adverse effects compared to placebo. Importantly, no heterogeneity was observed among the studies (I2 = 0%), reflecting high consistency in the outcomes.
For secondary outcomes, a meta-analysis was performed to evaluate the intervention’s effects on multiple body systems, including the nervous, digestive, and vascular systems. Data from all four trials were incorporated, focusing on AEs during treatment and variations in OS/PFS. The secondary analysis also demonstrated minimal heterogeneity (I2 = 0%) and statistically insignificant results, indicating that motesanib had no substantial impact on the occurrence of AEs.
Certainty of Evidence
The reliability of evidence was evaluated utilizing the GRADEpro guideline formulation tool (software). 12 Adverse effects such as diarrhea, nausea, hypertension, vomiting, thrombocytopenia, decreased appetite, anemia, and weight loss were rated as having high certainty, based on narrow confidence intervals, consistency across studies, and strong clinical relevance. Similarly, evidence related to abdominal pain, gallbladder toxicity, proteinuria, neutropenia, fatigue, headache, and dehydration was also classified as high certainty, supported by precise effect estimates and rigorous methodological quality. A comprehensive summary of the certainty ratings for each event is available in Table 2.
Summary of Findings for Motesanib + C/P Versus Control for (Non-squamous Non-small Cell Carcinoma of Lung).
Safety Profile
Abdominal Pain
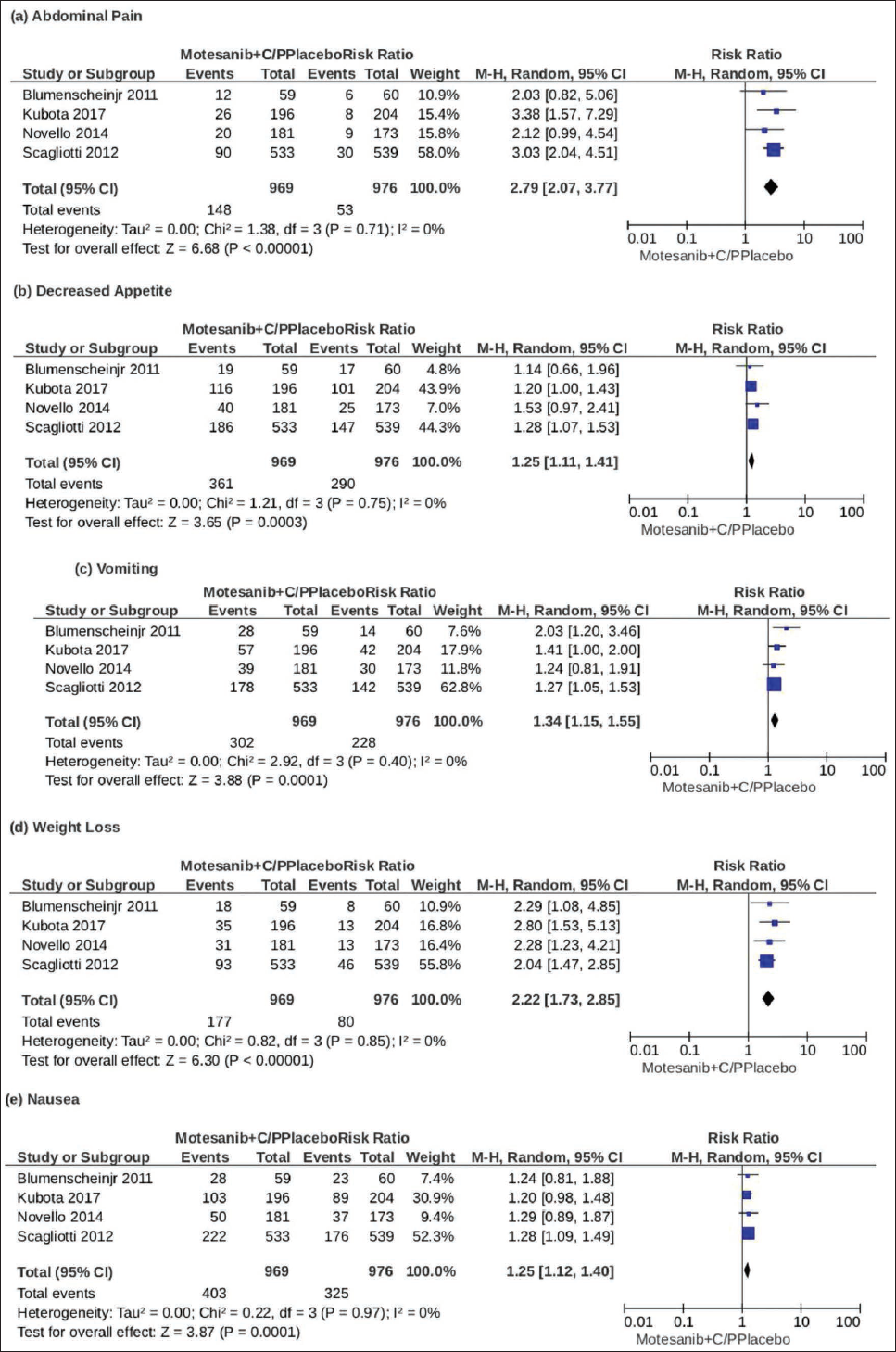
To assess the impact of motesanib on abdominal pain among the included participants, data from four studies comprising 1,945 individuals were thoroughly analyzed. The results, presented in Figure 3, demonstrated a significant association (RR = 2.79, 95% CI [2.07, 3.77], P ≤ .00001, I2 = 0%), with the certainty of evidence rated as high.
Forest Plots Comparing Motesanib to Placebo. (a) Forest Plot Showing the Event/Total Occurrences for Abdominal Pain Across Four Studies. (b) Forest Plot Showing Event/Total Occurrences of Decreased Appetite Across Four Studies Between Motesanib and Placebo. (c) Forest Plot Showing Occurrences of Vomiting Between Placebo and Motesanib Across Four Studies. (d) Forest Plot Showing Events of Weight Loss Between Usage of Motesanib Versus Placebo Across Four Studies. (e) Forest Plot Showing Events of Nausea Across Four Studies. (f) Forest Plot Showing Events of Hypertension Across Four Studies. (g) Forest Plot Showing Events of Diarrhea Across Four Studies. (h) Forest Plot Showing Comparison Between Occurrences of Anemia Across Three Studies. (i) Forest Plot Showing Comparison Between Occurrences of Thrombocytopenia Across Three Studies. (j) Forest Plot Showing Comparison Between Occurrences of Alopecia Across Three Studies. (k) Forest Plot Showing Comparison Between Occurrences of Proteinuria Across Three Studies. (l) Forest Plot Showing a Comparison Between Occurrences of Neutropenia Across Three Studies. (m) Forest Plot Showing Comparison Between Occurrences of Gallbladder Toxicity Across Three Studies. (n) Forest Plot Showing Comparison Between Events of Arthralgia Across Two Studies. (o) Forest Plot Showing Comparison Between Events of Headache Across Two Studies. (p) Forest Plot Showing a Comparison Between Events of Fatigue Across Two Studies. (q) Forest Plot Showing Comparison Between Events of Dehydration Across Two Studies. IV, Random: Inverse Variance Method, Random Effects Model. CI: Confidence Interval. The Horizontal Line Represents Confidence Intervals for Individual Studies, with a Diamond Shape Representing the Overall Effect Size; the I2 Value Indicates Heterogeneity.
Decreased Appetite
Data from four studies involving 1,945 participants were thoroughly analyzed to evaluate the effects of motesanib on appetite levels. A reduction in appetite was observed, with the results presented above (RR = 1.25, 95% CI [1.11, 1.41], P = .0003, I2 = 0%), and the certainty of evidence assessed as high.
Vomiting
Data from four studies comprising 1,945 participants were analyzed to assess the incidence of vomiting. The findings, as shown above, reported a significant association (RR = 1.34, 95% CI [1.15, 1.55], P = .0001, I2 = 0%), with the certainty of evidence rated as high.
Weight Loss
Data from four studies involving 1,945 participants were thoroughly analyzed to assess changes in body weight among individuals receiving motesanib. The analysis yielded the following results (RR = 2.22, 95% CI [1.73, 2.85], P < .00001, I2 = 0%), with the certainty of evidence rated as high.
Nausea
Data from four studies comprising 1,945 participants were analyzed to evaluate the incidence of nausea associated with motesanib use. The findings, illustrated in the figure above, reported a significant association (RR = 1.25, 95% CI [1.12, 1.40], P = .0001, I2 = 0%), with the certainty of evidence assessed as high.
Hypertension
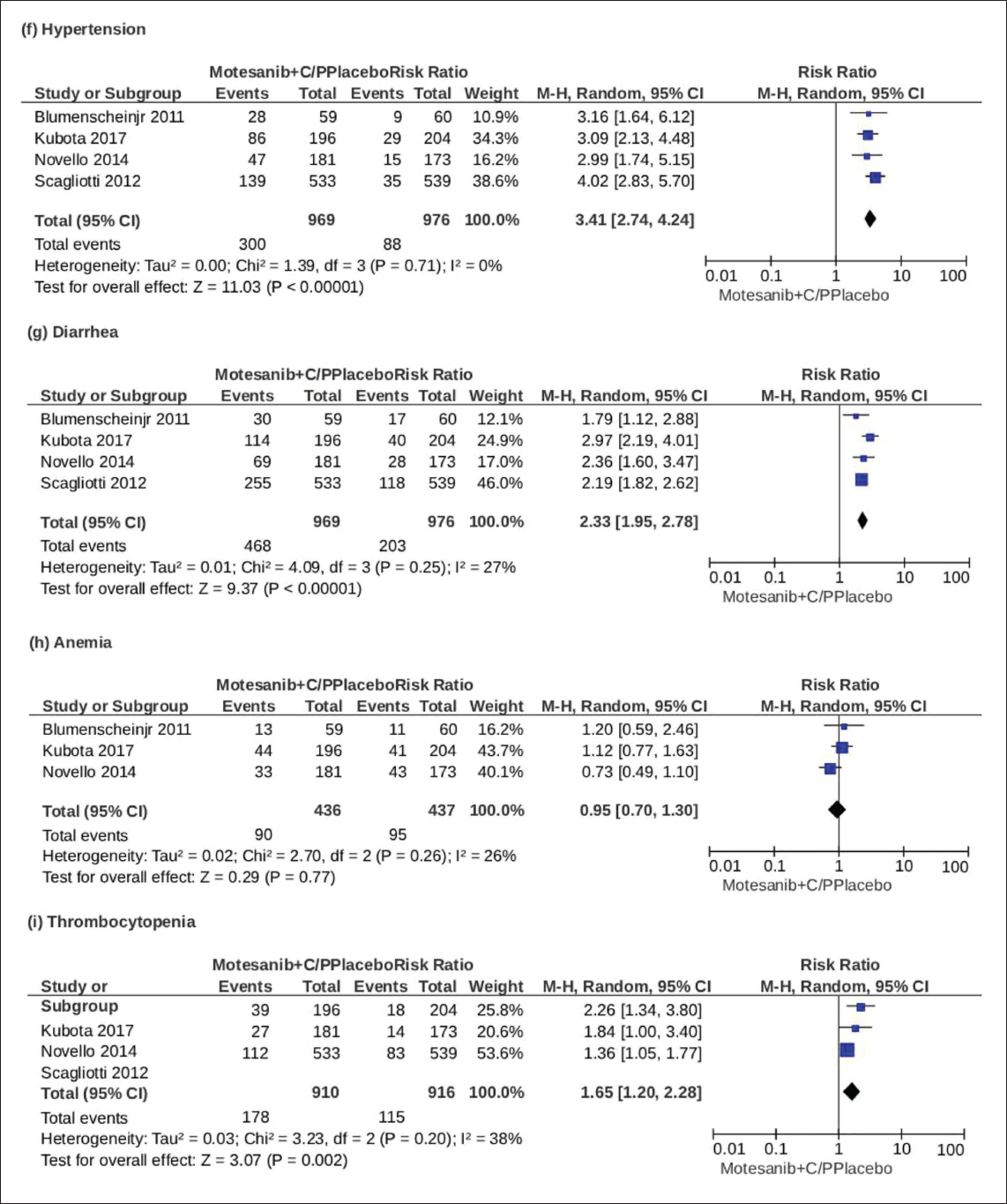
Data from four studies involving 1,945 subjects were analyzed to assess the incidence of hypertension associated with motesanib use. The results, presented in the figure above, indicated a significant association (RR = 3.41, 95% CI [2.74, 4.24], P < .00001, I2 = 0%), with the certainty of evidence rated as high.
Diarrhea
Data from four studies involving 1,945 participants were analyzed to assess the incidence of diarrhea associated with motesanib use. The findings, illustrated in the diagram above, demonstrated a significant association (RR = 2.33, 95% CI [1.95, 2.78], P < .00001, I2 = 27%), with the certainty of evidence rated as high.
Anemia
Data from three studies involving 873 participants were analyzed to evaluate changes in red blood cell (RBC) counts. Patients treated with motesanib exhibited a reduction in RBC levels (anemia); however, the results were not statistically significant (RR = 0.95, 95% CI [0.70, 1.30], P = .77, I2 = 26%), with the certainty of evidence rated as high.
Thrombocytopenia
Data from three studies involving 1,826 participants were analyzed to assess the incidence of thrombocytopenia associated with motesanib use. The analysis yielded the following results (RR = 1.65, 95% CI [1.20, 2.28], P = .002, I2 = 38%), with the certainty of evidence rated as high.
Alopecia
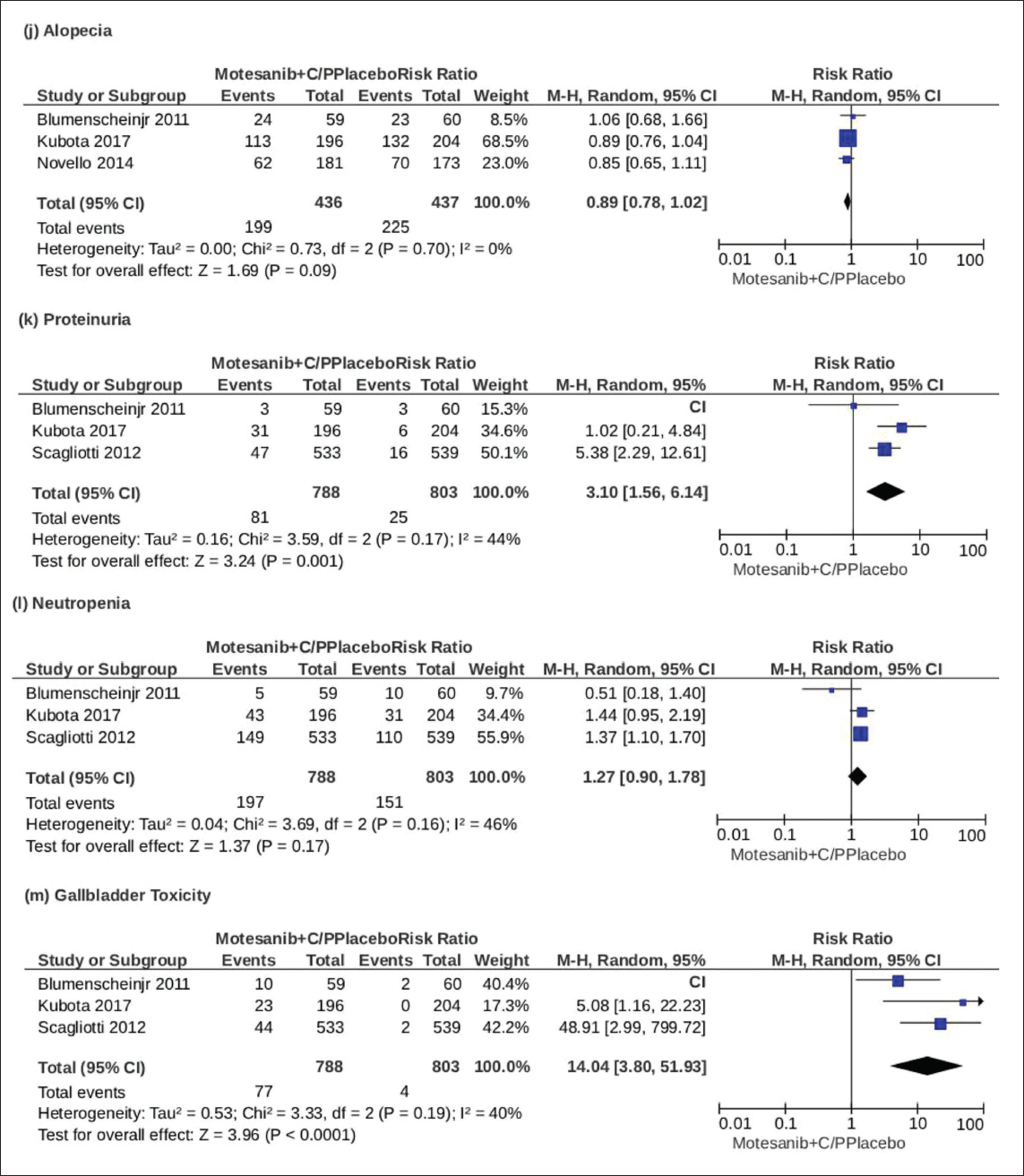
Data from three trials comprising 873 people were evaluated to assess the prevalence of baldness. The results, as presented, indicated no statistically significant association (RR = 0.89, 95% CI [0.78, 1.02], P = .09, I2 = 0%), with the certainty of evidence rated as high.
Proteinuria
Data from three studies involving 1,591 participants were thoroughly analyzed to assess the incidence of proteinuria. The analysis produced the following results (RR = 3.10, 95% CI [1.56, 6.14], P = .001, I2 = 44%), with the certainty of evidence rated as high.
Neutropenia
Data from three studies involving 1,591 participants were analyzed to evaluate the incidence of neutropenia. The results, illustrated in the graph above, indicated no statistically significant association (RR = 1.27, 95% CI [0.90, 1.78], P = .17, I2 = 46%), with the certainty of evidence rated as high.
Gall Bladder Toxicity
Data from three studies involving 1,591 participants were analyzed to evaluate the effects of motesanib on the gallbladder. The analysis revealed a significant association (RR = 14.04, 95% CI [3.80, 51.93], P < .0001, I2 = 40%), with the certainty of evidence rated as high.
Arthralgia
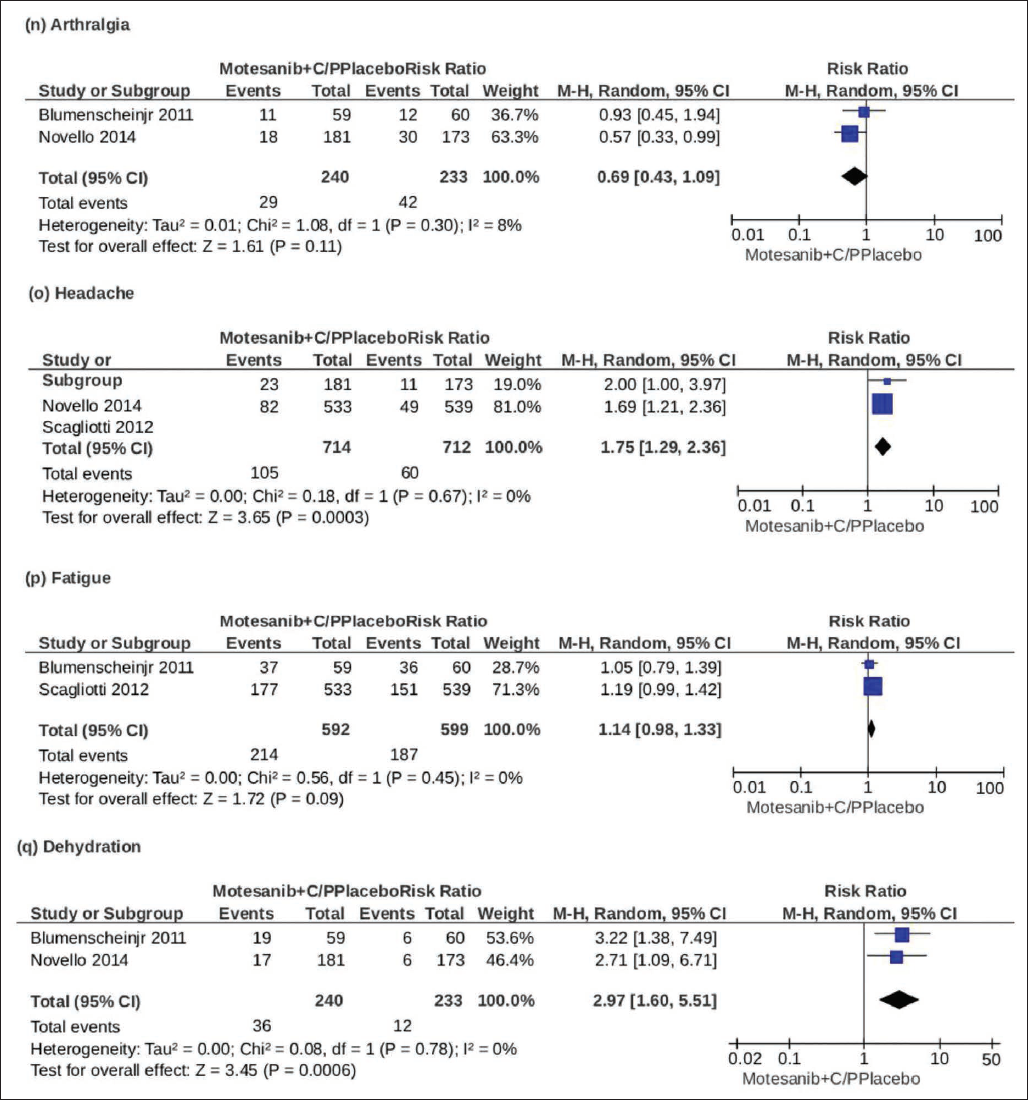
Data from two studies with 473 participants were examined to compare the effects of motesanib and bevacizumab on arthralgia. The results, illustrated in the figure above, showed no statistically significant difference (RR = 0.69, 95% CI [0.43, 1.09], P = .11, I2 = 8%), with the certainty of evidence rated as high.
Headache
Analysis of data from two trials with 1,426 individuals produced the following results: (RR = 1.75, 95% CI [1.29, 2.36], P = .0003, I2 = 0%), with the certainty of evidence assessed as high.
Fatigue
Data from two studies comprising 1,191 participants were retrieved and analyzed to evaluate the effect of motesanib on fatigue levels. The analysis yielded the following results (RR = 1.14, 95% CI [0.98, 1.33], P = .09, I2 = 0%), with the certainty of evidence rated as high.
Dehydration
Data from two studies, including 473 subjects, were meticulously analyzed and the following results were attained as shown in the diagram above (RR = 2.97, 95% CI [1.60, 5.51], P = .0006, I2 = 0% [High certainty]).
Discussion
This meta-analysis thoroughly assessed the safety profile of motesanib, drawing from 17 adverse outcomes across multiple studies with a cumulative sample size of over 1,900 participants (Figure 3). The results indicate that motesanib is linked to a statistically significant rise in the occurrence of several side effects, particularly abdominal pain, hypertension, and gall bladder toxicity, all demonstrating high relative risks and minimal heterogeneity. These results underscore the consistent and reproducible pattern of motesanib-induced toxicity, especially in the gastrointestinal and cardiovascular domains.
Gastrointestinal AEs—such as nausea, vomiting, decreased appetite, diarrhea, and weight loss—were commonly reported, aligning with the drug’s known mechanism targeting vascular endothelial growth factor receptors, which can impair mucosal integrity and gut motility. Although some events, like alopecia and anemia did not reach statistical significance, their inclusion adds depth to the safety profile and warrants further long-term investigation.
Proteinuria and thrombocytopenia also emerged as notable findings, suggesting renal and hematologic monitoring should be standard in clinical practice. Interestingly, while fatigue and arthralgia were reported, the results suggest a more modest or inconsistent impact, possibly influenced by patient heterogeneity or study design.
Overall, this analysis reinforces the need for personalized treatment strategies when using motesanib, balancing its therapeutic benefits against its side effect burden. Future research should aim to stratify risks by patient subgroups and explore combination regimens that may mitigate these toxicities.
Most outcomes in our meta-analysis showed an I2 value of 0%, suggesting a high level of agreement among the included studies. This unusually low variability may be attributed to several factors. The studies shared similar designs and patient populations, and the dosing regimens of motesanib were largely consistent, which likely contributed to uniform results. Additionally, the small number of studies may limit the assessment of variability, and formal tests for publication bias, such as Egger’s regression, were not conducted. These factors should be considered when interpreting the pooled findings, even though the results appear highly consistent.
Limitations
This meta-analysis possesses numerous limitations that should be acknowledged when evaluating the findings. First, although only RCTs were included to ensure high-quality evidence, the limited number of studies (n = 4) and varying sample sizes may affect the statistical power, especially for less common AEs.
Second, we relied on aggregate study data rather than individual patient-level data, which restricts the ability to conduct more granular subgroup analyses based on age, sex, genetic profiles, or comorbid conditions. Third, potential publication bias cannot be entirely ruled out, as only published English-language studies were considered, and negative results may be underreported. Moreover, variations in motesanib dosage, administration duration, and concomitant therapies across studies may have introduced unaccounted heterogeneity. Finally, some AEs reported with non-significant P values (e.g., fatigue, alopecia) may still be clinically relevant but lacked adequate power to achieve statistical significance.
Conclusion
This comprehensive review and meta-analysis establishes that motesanib, in conjunction with C/P for non-squamous NSCLC, does not provide a survival advantage and is linked to a markedly elevated risk of side events, particularly involving gastrointestinal, cardiovascular, and hepatobiliary systems. While motesanib demonstrated some antitumor potential in preclinical and other cancer models, its toxicity profile in NSCLC patients raises substantial concerns regarding its safety and tolerability. Clinicians should exercise caution when considering angiogenesis inhibitors and prioritize agents with more favorable efficacy-safety ratios. Future research should explore alternative regimens, risk mitigation strategies, and biomarkers to identify patients who may benefit from such therapies while minimizing harm.
Footnotes
Abbreviations
NSCLC = Non-small cell lung cancer
C/P = Carboplatin and paclitaxel
OS = Overall survival
PFS = Progression-free survival
ORR = Objective response rate
AEs = Adverse events
RCTs = Randomized controlled trials
VEGFR = Vascular endothelial growth factor receptor
RR = Risk ratio
CI = Confidence interval
PRISMA = Preferred reporting items for systematic reviews and meta-analyses
RoB = Risk of biass
Authors’ Contribution
The study’s conceptualization and design were executed by ASC and HSZ. HA and MAMQ performed the literature review. MSH and MA conducted the screening of titles and abstracts, while MAM executed the full-text screening. HZ oversaw data entry. SUO and ASC performed the data analysis and produced the funnel diagrams. All authors contributed equally to the composition and revision of the article and endorsed the final version for submission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
NA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
NA.
Proclamation of Artificial Intelligence (AI) and AI-enhanced Technologies
Artificial intelligence tools were utilized during the preparation of this manuscript to assist with language refinement and content organization. All outputs generated by the AI were carefully reviewed, edited, and verified by the authors. The authors take full responsibility for the integrity, accuracy, and originality of the final content.