
Abstract
Objective
The purpose of this review is to comprehend the treatment outcome of different PNS cancer histologies and their survival.
Materials and Procedures
A review of our institutional database from January 2010 to December 2022 included 122 sinonasal cancer patients. After exclusions, 84 patients whose data sets were complete underwent analysis. Overall survival (OS), loco-regional failure-free survival (LRFS), and distant metastases-free survival (DMFS) were the measured endpoints.
Results
With a median follow-up time of 26 months, there was no correlation detected between histological type and OS, LRFS, or DMFS. It was discovered that the type of treatment technique was substantially related to LRFS. Surgery plus adjuvant radiation and/or chemotherapy had a minor tendency to be significant in terms of OS, with a median OS of 56 months (95% CI: 38.6–73.3).
Conclusions
It showed that the use of different treatment modalities had an impact on LRFS, while the type of histology did not correlate with the effectiveness of the treatment.
Key Messages
PNS malignancies consist of a diverse group of histologies. Decisions regarding treatment options vary according to institution protocols and rely mostly on historical data with low evidence. Survival and failure patterns depend more on treatment techniques than histology of the disease.
Introduction
Cancers of the nasal cavity (NC) and paranasal sinuses have a low worldwide incidence approximating 1 in 100,000 per year. 1 Sinonasal malignancy overall forms a rare subset of head and neck cancer accounting for 5% of total head and neck cases. Cancers of the maxillary sinus (MS) are twice as common as those of the NC and cancers of the other paranasal sinuses are even rarer. They have been seen to develop after the age of 40 years except in cases of esthesioneuroblastoma histology which shows bimodal age distribution and occurs twice as commonly in men than in women.2, 3 The risk factors are unique relative to other primary sites in the aerodigestive tract and include occupational exposure in chrome and gas manufacturing, radium dial exposure, the production of mustard gas, nickel refining, and, of particular relevance to MS cancers, prior exposure to Thorotrast.4, 5 Squamous cell carcinomas of the NC are more frequently associated with nickel workers and smokers.6, 7 The rarest of these rare PNS tumors is the Sino nasal undifferentiated carcinoma (SNUC) which makes up 3%–5% of PNS carcinomas. This variety is rather a diagnosis of exclusion. 8 Owing to their uncommon incidence, heterogenous histologies, and paucity of data, PNS malignancies prove to be a challenge for treating surgeons, radiation oncologists, and medical oncologists alike. High surgical morbidity as a result of extensive resections deems these primaries sub-optimal results in the long term. The lack of consensus on treatment guidelines adds to the uncertainty in the extent and use of surgical and radiation modalities, further compromising results and complication rates. There is a dire need for prospective studies for these primaries in order to better comprehend the patterns of failure, the role of combined modality treatments, possible role of molecular techniques in identifying subsets with better prognosis. At present, due to the dearth of such evidence, therapeutic decisions are being made based on retrospective studies and individual institutional experiences.
Materials and Methods
The institutional database was reviewed for patients with PNS tumors from January 2010 to December 2022. A consecutive 122 patients were found to match the search criteria. Of the 122 patients, 38 were excluded from the present analysis for one or more of the following reasons: history of prior or concurrent malignancy, failure to complete radiotherapy (RT), and metastatic disease at presentation. The remaining 84 patients were included in the study to assess the impact of locoregional treatment on the endpoint. The specific endpoints examined included distant metastases-free survival (DMFS), Loco regional failure-free survival (LRFS), and overall survival (OS). The Kaplan-Meier product-limit method was used to estimate the local control and survival probabilities. The Cox proportional hazards method was used to assess the statistical significance in multivariate analysis.
Results
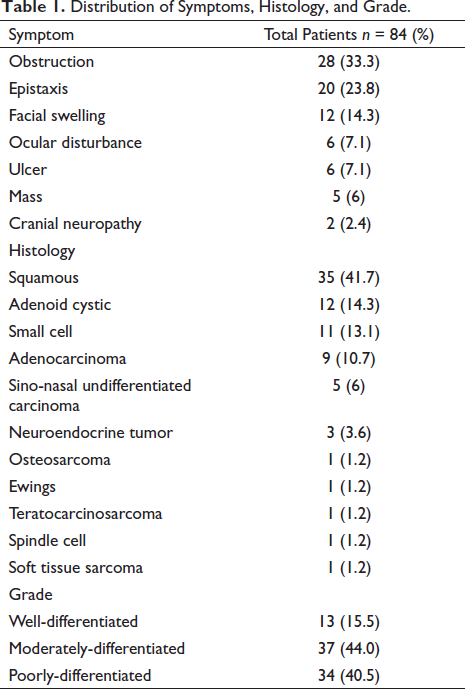
Of the 84 patients, 54 were men (64.3%) and 30 were women (35.7%). Sixty-three (75%) of 84 patients had a history of prior or current tobacco use at diagnosis. Detailed information on occupational exposures was unavailable for our patients. The primary tumor site, often difficult to determine because of the advanced presentation of PNS tumors, was assigned to the predominant region of tumor bulk at diagnosis. Most tumors originated in the NC (41.7%), followed by MS (35.7%), and ethmoid sinus (ES) (17, 20.2%). The least common site in the cohort was Sphenoid sinus (SS) (2, 2.4%) The presenting symptoms shown in Table 1, were the presence of a mass, sinusitis, epistaxis, nasal obstruction, cranial neuropathy, pain, and facial edema. A total of 11 varieties of histology were seen in the study group as confirmed on histology. Most patients (41.7%) had squamous cell carcinoma. The second most common variety was adenoid cystic carcinoma (14.3%). The rest of the histologies are shown in Table 1. The grade of tumor was found to be moderately differentiated in most (44%) followed by poorly differentiated (40.5%) and well-differentiated tumors were least common (15.5%).
Distribution of Symptoms, Histology, and Grade.
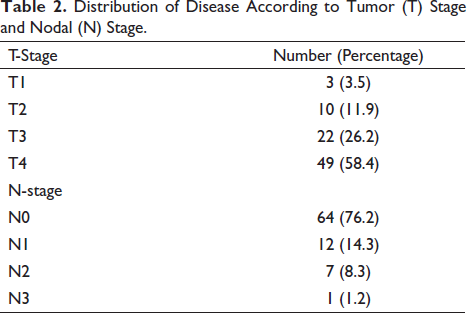
Tumors were staged according to the 2010 American Joint Committee on Cancer staging system for paranasal sinus tumors and NC tumors. Using these criteria, three patients had Stage T1 disease, and 10, 22, and 49 patients had Stage T2, T3, and T4 lesions. Sixty-four patients (76.2%) presented with clinically uninvolved cervical lymph nodes, and 12,7 and one patients had N1, N2, and N3 nodal staging respectively, shown in Table 2.
Distribution of Disease According to Tumor (T) Stage and Nodal (N) Stage.
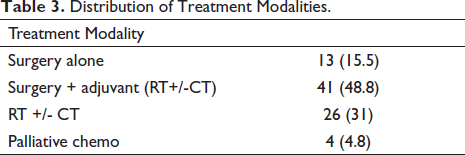
The distribution of treatment modalities is shown in Table 3. Thirteen patients (15.5%) were treated with surgery alone as the treatment modality. Twenty-one patients (25%) received surgery with adjuvant radiation. Twenty patients (23.8%) were treated with a combination of surgery and concurrent chemo-radiotherapy (CCRT). Radiation alone was used in three patients (3.6%). Definitive chemo-radiotherapy was used in 25 patients (29.8%). The number of chemotherapy cycles ranged from two to four (mean three). The agents used included cisplatin, fluorouracil, and doxorubicin. All patients underwent RT using a 6-MV photon on LINAC. The median dose delivered when radiation was included in the treatment modality was 66 Gy.
Distribution of Treatment Modalities.
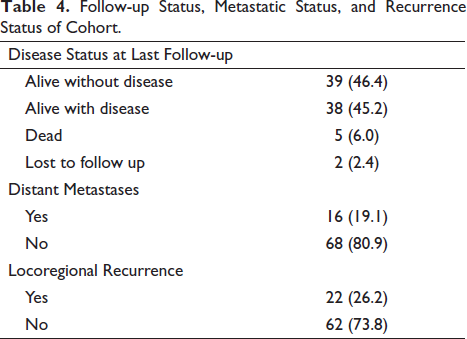
Follow-up Status, Metastatic Status, and Recurrence Status of Cohort.
Univariate analysis was performed using the log–rank statistic to identify prognostic factors for DMFS, LRFS, and OS. The variables examined for potential significance included patient age; gender; primary site; primary stage; nodal stage; histologic type; tumor grade, and treatment modality (or combination) used. Statistically significant prognostic factors for LRFS included the treatment modality used (p = .002), however, among all the prognostic factors studied, no association was found in relation to DMFS and OS.
The median follow-up of the entire cohort was 26 (1–27) months.
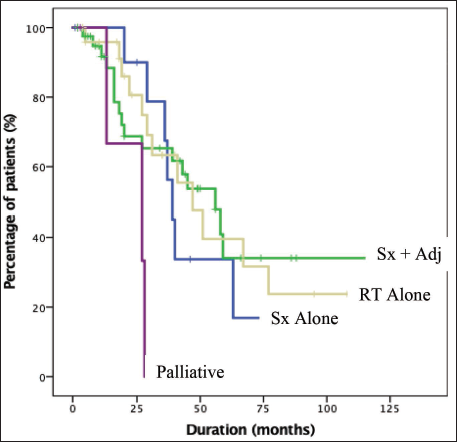
The type of histology or grade of differentiation did not significantly correlate with OS (p = .287, p = .748, respectively). The type of treatment modalities used showed a slight trend towards significance for OS (p = .078) (Figure 1), where the median OS for surgery alone was 39 (95% CI: 33.2–44.7) months, for surgery in combination with adjuvant treatment (RT or CCRT) was 56 (95% CI: 38.6–73.3) months, for RT alone was 47 (95% CI: 31–62.8) months.
Kaplan Meir Curve Depicting Overall Survival (OS) as a Function of Treatment Modality.
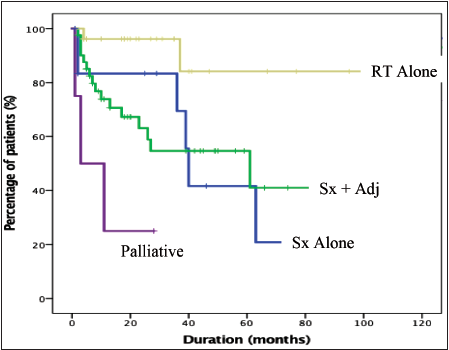
Twenty-two patients (26.2%) had locoregional failures. No significant difference was found based on the grade of differentiation of the tumor (p = .069). Median survival duration was reached only for well-differentiated tumors, which was 27 (95% CI: 24.5–29.4) months. The type of histology did not correlate with LRFS (p = .292). The type of treatment modality had a significant effect on LRFS with p = .002 (Figure 2). Median survival for surgery alone was 40 (95% CI: 37.5–42.5) months, and surgery in combination with adjuvant treatment (radiation with or without chemotherapy) was 61(8.4–113.5) months. Median survival for radiation alone treatment was not reached.
Kaplan Meir Curve Depicting Locoregional Failure Free Survival (LRFS) as a Function of Treatment Modality.
Sixteen patients (19%) had distant failures. The most common site of failure was the lung in 56% of patients, followed by the kidney (25%), non-regional LN (12.5%), and brain (6.25%). On comparing the effect of treatment modalities on DMFS, no significant difference was found (p = .807). Types of histology also made no significant difference to DMFS (p = .927); similarly, grade of differentiation had no significant association with DMFS (p = .209). Median survival duration was not reached for DMFS.
Discussion
Paranasal sinus malignancies continue to pose a significant challenge in identifying the best action plan. Without level 1 evidence favoring a standard treatment modality, the decision regarding the preferred treatment protocol must be based on a retrospective series. This lack of a unified approach can be attributed mainly to the rarity of these subsites as a primary and wide spectrum of heterogeneity in their histology. Other factors include the involvement of nearby critical structures like the base of the skull, and orbit which portend surgical challenges on their own. This study elucidates a single institution’s experience treating PNS malignancies over a decade.
The epidemiological variables of patients in the study were comparable with existing literature. In our study, males were more commonly affected than females (56% vs. 44%), most patients gave a history of current or past tobacco use either in the form of smoking or chewable (75%) and the most common sites involved were NC and MS like other studies had shown. Most patients presented in OPD with locally advanced stages. This could be attributed to the fact that the presenting symptoms often mimic benign or infective etiologies wherein eventual involvement of critical optic or neural structures prompts medical attention.
In a study by Harbo et al., the most common presenting complaints were swelling (59%), pain (34%), nasal obstruction (22%), and visual disturbances (11%). 9 The distribution of presenting complaints was similar in our study, comprising pain, swelling, obstructive features, epistaxis, ulcer, ocular changes, and cranial neuropathy.
The major challenge of primary diagnostic evaluation is to accurately assess the extent of involvement. It is imperative to perform a thorough history and physical examination with special emphasis on cranial nerve examination, and nasal and mucosal examination. For subsites difficult to examine, upper aerodigestive endoscopies must be performed to confirm primary and aid biopsy proof. Imaging modalities preferred to comprise contrast-enhanced CT scans and MRI. CT scans provide the obvious advantage of a better picture in terms of bony involvement and MRI for intracranial and orbital extension. 10 For metastatic workup, chest skiagrams are sufficient as there is infrequent involvement of distant sites, and the role of routine PET scans is not considered essential. 11
Prognostic factors affecting disease-free survival, local control, and OS in PNS carcinoma were studied by Dulguerov and found that T stage, histology, location, and treatment modality used were all independent prognostic factors for survival. The five-year actuarial survival was 91% for T1, 64% for T2, 72% for T3 and 49% for T4. In terms of histology, five-year carcinoma-specific actuarial survival was 78% for adenocarcinoma and 60% for undifferentiated varieties. 12 Ganly et al. in an international collaborative study on craniofacial resection for malignant PNS tumors found similar outcomes in terms of OS for both squamous and adenocarcinoma, however, better disease-specific survival was found in favor of adenocarcinoma. 13 Our study however failed to show histology or T stage as a viable prognostic factor.
Several studies have shown that neck metastases at presentation were associated with poor prognosis and indicated tumor extension outside the sinonasal cavity.14–16
Surgery as a single modality of treatment has generally been associated with poor outcomes in terms of OS. Amendola et al. in a study of 39 patients treated with curative intent with surgery or radical RT found no statistical difference in OS at five years after treatment with a survival rate of 31% and 35% for surgery alone and RT alone, respectively. 17 Other studies have shown improved results with combined modality treatment, especially for MS tumors. In a study on 61 patients by St Piere and Baker, 16% of patients underwent surgery alone, 53% underwent definitive radiation and 31% received combined modality therapy (CMT). There was a trend for improved survival among patients who received a combination of both surgery and adjuvant radiation. 18 Paulino et al. studied MS tumors where 23% of patients were treated with definitive radiation alone and 77% with both surgeries followed by adjuvant radiation. Local control and disease-specific survival rates were both significantly improved in the combined modality arm at five years. OS was 0% for RT alone compared to 52% for CMT. 19 Jiang et al. showed although non-significant, improvement in locoregional control with CMT. 20 In our study, LRFS was significantly influenced by the treatment modality. The median survival for surgery in combination with adjuvant treatment (radiation with or without chemotherapy) was 61 months, for surgery alone was 40 months, and for RT alone was not reached.
Timing of radiation has been investigated in several studies, most of which emphasized that radiation in post-operative settings had better outcomes than preoperative. Ganly et al. reported Preop RT in patients requiring craniofacial resection had a negative impact on recurrence-free survival with a 1.6 times increase in relative risk of recurrence as compared to no preoperative RT, this result could be due to difficulty in assessment of the extent of surgical resection required to obtain clear margins in previously irradiated patients. 13
An important aspect of the treatment of PNS malignancies is the uncertainty surrounding the adequate management of nodes. Nodal failure rates in the absence of elective treatment have been shown to be in the range of 9% to as high as 33% in a few studies. 21 Jiang et al. evaluated the patterns of lymph node recurrence among 73 patients with MS tumors. 22 They identified histology as the most important prognostic factor, with squamous cell and undifferentiated tumors having a maximum predilection for nodal relapse at 33% and 50%, respectively. Our study also showed no statistical association between nodal relapse and histology. Paulino in their study on MS tumors found 26% of patients with nodal recurrence and suggested prophylactic treatment of ipsilateral neck for patients at high risk of relapse 1 . In maxillary tumors, in a series by MD Anderson Cancer Centre, the incidence of nodal spread was found to correlate with the histologic type (17%, with squamous cell or poorly differentiated carcinomas, vs. 4% for patients with adenocarcinoma, adenoid cystic carcinoma, or mucoepidermoid carcinoma). The rate of nodal relapse in patients who did not receive elective neck treatment also showed association with histologic type (38%, with squamous cell or poorly differentiated carcinomas, vs. 8% patients with adenocarcinoma, adenoid cystic carcinoma, or mucoepidermoid carcinoma). 23
At our institution, prophylactic nodal irradiation was not routinely delivered in all post-operative cases. Only in cases of positive lymph node involvement in dissected specimens, was nodal irradiation considered in an adjuvant setting. In settings of definitive chemo-radiation, patients with involved nodes at presentation were given elective nodal irradiation in case of MS tumors, especially with squamous cell histology. The high locoregional failure rate in the current study (26.2%) indicates the scope for improvement in locoregional treatment modalities. Apart from a few retrospective case series, few studies in recurrent settings have been done. Therefore, data on patterns of failure and their improvement remains unnavigated. Hoeppe et al. in a retrospective study suggested that the primary treatment field remains the predominant site of treatment failure in paranasal sinus and NC tumors. 24
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
No ethical approval or informed consent was required.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.