
Abstract
Background/Objectives
Benign prostate hyperplasia and prostate cancer are prostate disorders that have continued to pose major concerns among adult men. Prostate-specific antigen (PSA) determination is inadequate to differentiate these conditions, as it is raised in both conditions. Also, most often, high levels are seen in cases already established with clinical signs or symptoms of prostate complications. Serum calcium, which can exist in the ionized and non-ionized form, has been postulated to increase the risk of prostate cancer. There is an urgent need for further evaluation of ionized calcium as a prospective biomarker for prostate disorders; hence, this study aims to evaluate the potential use of ionized calcium as a marker of benign prostate hyperplasia and prostate cancer.
Methods
A total of 138 consenting male subjects, 50 years and above, diagnosed with prostate cancer (70 subjects) or benign prostatic hyperplasia (BPH) (68 subjects), attending the urology clinic, and another 69 non-prostate diseased subjects of the same age group from the general clinic as negative controls, were recruited randomly from Lagos University Teaching Hospital, Idi-Araba for this prospective cross-sectional study. After calculating the sample size based on a previous local prevalence rate of 7.9%, a total of 5 mL of venous blood was collected from all participants and dispensed into appropriate specimen containers. Serum and plasma were obtained using standard techniques; thereafter, ionized and total calcium, as well as free and bound PSA, were determined using standard methods. The data generated were subjected to statistical analysis using SPSS version 28, with a P < .05 considered significant.
Results
The mean serum concentration of total PSA, free PSA, serum ionized calcium and total calcium levels among adult males with benign prostate hyperplasia and prostate cancer were significantly higher than those of the control group. A positive correlation was found between total calcium and total PSA (P < .05). Additionally, ionized calcium showed a strong and positive correlation with both total and free PSA (P < .000). Also, ionized calcium demonstrated a sensitivity of 62.5% compared to the current gold standard for PSA, which is 71.1%, and a better negative predictive value of 47.1% compared to total PSA’s 32.4%.
Conclusion
Ionized calcium, therefore, is a potential biomarker for early detection of prostate cancer and could serve as a better predictor for future prostate cancer. It is recommended that ionized calcium be added to the screening tests for all men aged 50 years to monitor for early development of prostate disorders, particularly prostate cancer.
Introduction
The prostate gland, a primary sex organ among males, is about the size of a walnut and lies just below the bladder, from where it adds fluid to the semen. It consists of connective tissues and glandular tissues, which help push semen through the urethra. 1 A tumor in the prostate may interfere with proper control of the bladder and normal sexual functions. Often, the first symptom of prostate cancer is difficulty in urinating. 2 However, because a more familiar, non-cancerous condition of the prostate, benign prostatic hyperplasia (BPH), also causes the same problem, difficulty in urination, it is not necessarily due to cancer, but is much more likely from BPH. Prostate-specific antigen (PSA) determination is inadequate to differentiate these conditions, as it is raised in men with cancer but also in many men with benign conditions. 3 Cancerous cells within the prostate itself are generally not deadly on their own. As the tumor grows, it can directly invade adjoining structures like seminal vesicles, rectum and pelvic wall, and as the tumor grows and becomes cancerous, some of the cells break off and spread through the lymph or the blood, to either the bones, lymph nodes, lungs, seminal vesicles and the pelvic region; a process known as metastasis that can ultimately result in morbidity and potential prostate cancer-specific mortality. 4
Prostate cancer is the most commonly diagnosed malignancy among adult males in Western countries. Although prostate cancer is often very slow-growing, it can be aggressive, especially in younger men. 5 Given its slow-growing nature, many men with the disease die of other causes rather than from the cancer itself. Furthermore, African American men are generally diagnosed with more advanced stages of prostate cancer at an earlier age. 6 Consequently, since in most cases, the disease can be treated effectively and even eradicated when the disease is detected at a very early stage, much effort is being placed on detecting prostate cancer in an early, curable stage to decrease the rate of mortality from this disease. PSA, currently used for prostate cancer diagnosis, is a specific biomarker based on the release of PSA from damaged prostate epithelial cells by prostate cancer or BPH, rendering PSA ineffective in the prognosis and prevention of prostate cancer.
Calcium, which is required for vascular contraction and vasodilation, muscle function, nerve transmission, intracellular signaling, and hormonal secretion, has been postulated to increase the risk of prostate cancer, especially with high intakes of total, dietary, or dairy calcium. 7
Since, less than 1% of total body calcium is needed to support these critical metabolic functions its concentration is tightly regulated and does not fluctuate with changes in dietary intakes; the body uses bone tissue as a reservoir for and source of calcium to maintain constant concentrations of calcium in blood, muscle, and intercellular fluids hence calcium can be in the form of ionized “working” form of calcium, or unionized is the “storage” and “transport” form, playing different but crucial roles in maintaining overall calcium homeostasis.7, 8 Men who have ionized serum calcium levels in the highest third are three times more likely to die of prostate cancer than those with the least amount of ionized serum calcium. 9 The urgent need for further evaluation of ionized calcium as a prospective biomarker for prostate cancer has been advocated since it is necessary to start early monitoring for the development of prostate cancer with a biomarker of disease specificity when there are no clinical signs or symptoms of prostate complications. The ionized serum calcium level measurement may serve as a better biomarker of prostate gland cancer, as a doubling of the risk for prostate cancer was shown among men whose serum calcium level was recorded in the highest third (above the 75th percentile value) of the total serum calcium; 10 hence, this study aims to evaluate the potential use of ionized calcium as a marker of benign prostate hyperplasia and prostate cancer.
The specific objectives:
To determine the serum total PSA, free PSA and serum ionized calcium level among adult males with benign prostate hyperplasia and prostate cancer. To determine the correlation between total and ionized serum calcium and total and free serum PSA of the patients. Compare the predictive values, specificity, sensitivity, and efficiency of calcium with that of PSA.
Ethical Approval
Lagos University Teaching Hospital, Idi-Araba’s ethics committee approved this study after a detailed explanation of the research was provided in our application with No: REF.NO.ADM/DCST/221. Informed consent was obtained from the participating patients and subjects after they were thoroughly informed about the research.
Human Subjects
A total of 138 consenting male subjects, 50 years and above, who have been diagnosed with prostate enlargement or prostate cancer with PSA above 4ng/ml and attended the urology clinic in the Lagos University Teaching Hospital, Idi-Araba, were randomly recruited for this prospective cross-sectional study. Of these, 70 male subjects were diagnosed with prostate cancer. In comparison, 68 patients with BPH and another 69 non-prostate diseased subjects within the same age group above were recruited from the general clinic and matched as negative controls.
Sample Size Determination
The Armitage et al. technique was used to calculate the sample size based on a previous local prevalence rate of 7.9% among men 50 years and older, with significance at 5% level.11, 12
Exclusion Criteria
All male subjects below 50 years of age.
Intake of oxalate and oral phytate, which reduces calcium absorption.
Chronic renal failure resulting in tubular loss of calcium and non-formation of active vitamin D.
Hyperthyroidism/thyrotoxicosis.
All subjects who had their prostate gland examination before sample collection through Direct Rectal Examination (DRE) were excluded.
Inclusion Criteria
All male subjects 50 years and above diagnosed with prostate cancer or BPH.
Sample Collection
A 5 mL venous blood sample was collected from subjects and controls and dispensed into specimen containers to determine ionized and total calcium, as well as free and bound PSA. Samples were allowed to retract and spun at 3,000 rpm for 5 minutes. The supernatant plasma was separated and stored at −20°C for batch analysis.
Procedures, Reagents and Equipment for Laboratory Determinations
Total calcium was determined using an autoanalyzer with the Randox reagent, based on the Arsenazo III reaction, while ionized calcium was analyzed with an ion-selective electrode (ISE). Similarly, Free and total PSA were determined using the ELISA method with kits and reagents from Fortress Products. All the equipment used, which includes an Auto analyzer, an ELISA Machine, a washer, a centrifuge, a pipette, and a water bath, was standardized according to the manufacturer’s instructions. All data generated were subjected to statistical analysis using SPSS version 28, with a P < .05 considered significant.
Results
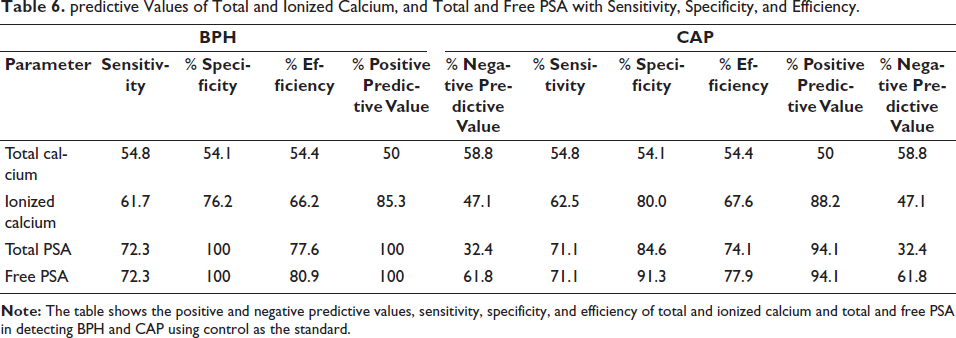
The mean serum concentration of total PSA, free PSA, serum ionized calcium and total calcium level among adult male with benign prostate hyperplasia and prostate cancer were significantly higher than that of the control group as shown in Table 1 with the concentrations not showing any significance different (P > .05), irrespective of the various age groups compared as seen in Tables 2 and 3. There was a positive correlation between total calcium and total PSA (P < .05) (Table 4). A weaker correlation was observed between total calcium and free PSA (P < .05), whereas ionized calcium showed a strong and positive correlation with both total and free PSA (P < .0001) (Table 5). Additionally, ionized calcium demonstrated a sensitivity of 62.5% compared to the current gold standard of PSA, at 71.1%, and a better negative predictive value of 47.1% compared to total PSA’s 32.4%, as shown in Table 6.
Analysis of Total and Ionized Calcium, and Total and Free PSA in CAP, BPH, and Control Subjects.
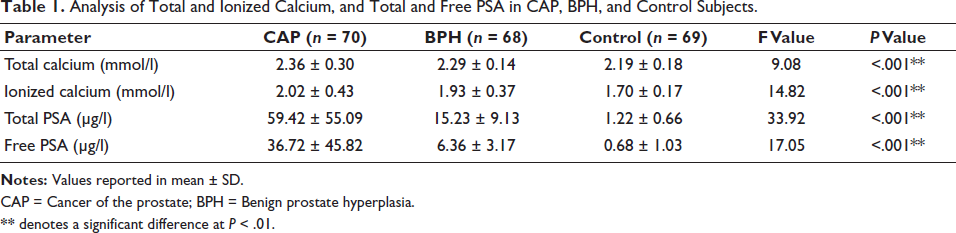
CAP = Cancer of the prostate; BPH = Benign prostate hyperplasia.
** denotes a significant difference at P < .01.
Levels of PSA, tCal, and iCal in Different Age Groups in BPH.
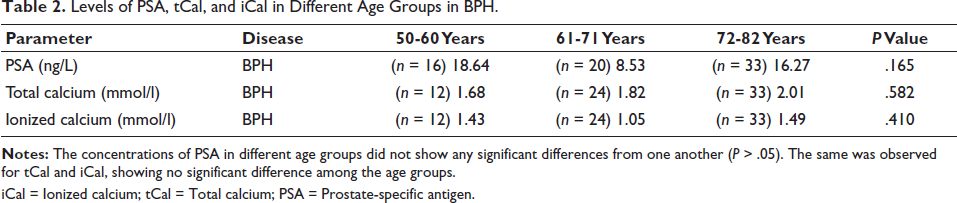
iCal = Ionized calcium; tCal = Total calcium; PSA = Prostate-specific antigen.
Levels of PSA, tCal, and iCal in Different Age Groups in CAP.
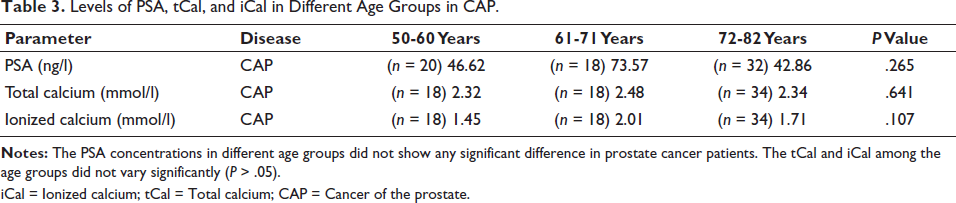
iCal = Ionized calcium; tCal = Total calcium; CAP = Cancer of the prostate.
Correlation of Total Calcium and Ionized Calcium with Total and Free PSA in CAP.
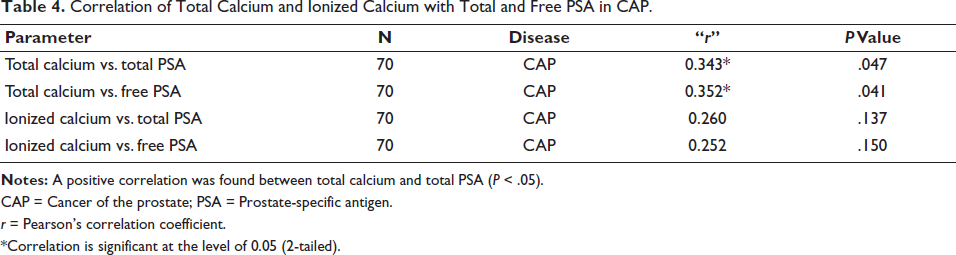
CAP = Cancer of the prostate; PSA = Prostate-specific antigen.
r = Pearson’s correlation coefficient.
*Correlation is significant at the level of 0.05 (2-tailed).
Correlation of Total Calcium and Ionized Calcium with Total PSA and Free PSA in BPH.
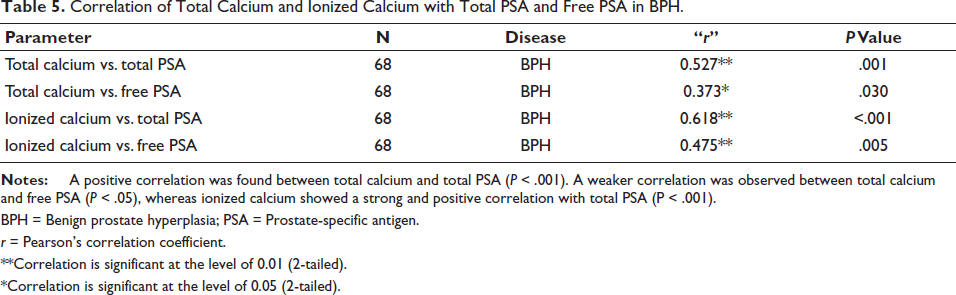
BPH = Benign prostate hyperplasia; PSA = Prostate-specific antigen.
r = Pearson’s correlation coefficient.
**Correlation is significant at the level of 0.01 (2-tailed).
*Correlation is significant at the level of 0.05 (2-tailed).
predictive Values of Total and Ionized Calcium, and Total and Free PSA with Sensitivity, Specificity, and Efficiency.
Discussion
This study, which set out to evaluate serum calcium and PSA assays among BPH and CAP, two common conditions that can affect the prostate gland with similar symptoms in men, is very apt, as there is reported evidence of an increase in the prevalence of these conditions among men in Nigeria, 13 making the need to evaluate more potential biomarkers a priority.
The higher levels of serum total PSA and free PSA of the study population that were statistically significant when compared with the controls (P < .01) in CAP and BPH, agreed with other workers14–17 where the population with prostate cancer had a significant increase in the mean serum level of total PSA compared with the controls (P < .0001). Abnormal leakage of PSA into the circulation, which further influences its expression in the malignant epithelium following a distorted prostatic glandular architecture, has been attributed to this increase. 18 Our findings also revealed significantly higher PSA values, with a three-fold increase in CAP compared to BPH. The rise in PSA is more consistent in BPH than in CAP, where total PSA levels vary widely. Although some patients with CAP have low PSA levels within the range of BPH, others experience a three-fold increase, leading to large standard deviations due to the skewness of PSA values in CAP patients. Other studies 19 showed a similar finding where prostate cancer was diagnosed in 15.2% of men with a PSA level at or below 4.0 ng/ml. Similarly, both total and ionized calcium values were higher in CAP and BPH than in the control (P < .05), with no significant difference in values between CAP and BPH. This was corroborated by previous investigations, 9 who showed that men with ionized calcium levels in the highest third are three times more likely to die of prostate cancer than those with the least amount of ionized calcium. Men with ionized serum calcium levels above the 75th percentile of the normal value are at risk of future development of prostate cancer. This study found the 75th percentile value of ionized calcium in the study population to be 1.7963 mmol/L. This is a critical risk value for the future development of prostate cancer in the studied population. Calcium controls molecular factors and signaling pathways involved in the development of prostate cancer and its progression. 7 The differences in calcium signaling between normal cells and those of amplitude, localization of the signal within cells, or kinetic differences of the signal itself characterize CAP cells. These differences in calcium signaling impact cellular processes such as survival, growth, differentiation, and others, responsible for the development of prostatic carcinoma. 20 It is the changes in plasma membrane and endoplasmic reticulum channels and GAP junctions that are mainly responsible for the disturbances of calcium intracellular concentrations in CAP cells. 21
In CAP, the ionized calcium level is elevated. This value is higher than that of ionized calcium in BPH, suggesting that ionized calcium levels are increased in the serum of patients with confirmed prostate cancer. This can be of diagnostic value before clinical manifestations of prostate damage occur, making ionized calcium an ideal parameter for early monitoring of prostate changes. These findings support the hypothesis that serum calcium is a prospective biomarker of fatal prostate cancer. 9 Specifically, a study in Rivers State, Nigeria, 22 suggested a link between high calcium intake and an elevated prostate cancer risk. Other studies have proven that in prostate cancer, the levels of PTH are higher than the levels in matched controls.
A PTH increase and thus a parallel calcium rise are in some way connected to or induced by prostate cancer. 23
It is worth noting that the concentrations of PSA, total calcium, and ionized calcium did not show variations across different age groups in BPH. The same was observed for tcal and ical, showing no significant difference among the age groups in CAP. This was due to the non-separation of patients under treatment from new cases, who still had high values of PSA, tcal, and ical, which is a major limitation of the study.
Furthermore, both total serum and ionized calcium levels showed a positive relationship with total and free PSA in BPH, with total serum calcium levels increasing alongside total PSA. This increase in total calcium was primarily due to ionized calcium, which, as previously shown, correlated well with total PSA. In patients with elevated PSA, ionized calcium was also high, hence the total calcium. This finding supported the findings of other previous studies9, 10 who compared men in the top tertile with those in the bottom tertile of serum Ca, and reported that Ca in the upper tertile, and not hypercalcemia, was the factor determining an increased risk of death.
Additionally, the sensitivity of ionized calcium observed in this study was 62.5%, compared with the current gold standard of PSA at 71.1%. However, ionized calcium has a better negative predictive value of 47.1% compared to total PSA’s 32.4%. It shows a gradual rise, years before damage is done to the prostate gland, giving time for detection. Though the PSA sensitivity is high, it is organ-specific and rises sharply when the organ is already damaged.
On the one hand, ionized calcium is disease-specific and rises years before the damage is eventually done to the prostate. Hence, the combination of ionized serum calcium for early detection of predisposed individuals and serum PSA for symptomatic prostate cancer patients is advised for the diagnosis of prostate cancer.
Conclusion
In prostate cancer, total serum calcium and ionized calcium levels increased in tandem with total PSA and free PSA levels. A positive correlation was found between serum calcium and serum PSA. While serum calcium levels increased early enough to prevent damage to the prostate, serum PSA levels increased when damage had already occurred to the prostate. The use of ionized calcium in the monitoring of prostate cancer may serve as a potential biomarker for early detection. The ionized calcium is a far more useful indicator for detecting CAP and BPH, as a positive test result is over 1.7 times more likely to indicate the actual presence of the disease compared to a positive total calcium result. The high specificity also means fewer unnecessary follow-up procedures are triggered by false-positive results. Under these conditions, PSA is highly sensitive and specific, but with little benefit for prevention or advancing the five-year survival rate. Ionized calcium, therefore, is the best biomarker for prostate cancer and serves as a better predictor of future prostate cancer, as the ionized serum level remains stable over a long period and is genetically controlled.
Recommendations
It is recommended that all men aged 50 years should be screened for prostate cancer using ionized calcium to monitor for early development of this disease. Values greater than 1.79 mmol/l alert patients to the risk of future development of prostate cancer. The combination of PSA and ionized calcium is recommended in advanced symptomatic disease of the prostate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.