
Abstract
Brain metastasis is seen in 10% to 20% of all adult cancer patients. One of the main modalities of treatment is stereotactic radiosurgery (SRS). Here, we describe the step by step procedure for stereotactic planning of brain metastasis by using a clinical scenario. The management of brain metastasis starts with the clinical evaluation of the patient followed by imaging and SRS treatment in the present case. The paper highlights the sequential process of radiation planning for SRS—starting from simulation, planning, evaluation of plan, and treatment.
Introduction
The incidence of brain metastasis is 10 times more than the primary brain tumors. MRI of brain is the best imaging modality for diagnosis of brain metastasis. The treatment options for brain metastasis include surgery, whole brain radiotherapy, stereotactic radiation in the form of stereotactic radiosurgery (SRS) or stereotactic radiotherapy, or best supportive care depending on the general condition of patient or number of brain metastasis. 1 In this paper, the various steps of radiation planning for SRS have been illustrated in an easy way for the beginners who are planning for SRS in a case of brain metastasis.
Case History
A 70-year female, with a history of triple negative breast cancer (TNBC) post modified radical mastectomy post chemotherapy and radiotherapy after 6 months of follow up, presented with the chief complaints of headache and giddiness for 1 month.
Imaging
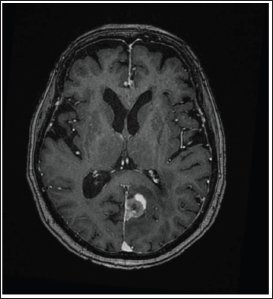
Contrast Enhanced Magnetic resonance imaging (CE-MRI) of the brain revealed a well-defined lesion measuring 2.2 cm × 2.2 cm in the left occipital lobe with ring enhancement and minimal edema, no mass effect or midline shift (Figure 1). The Positron Emission Tomography Computed Tomography (PET-CT) scan showed increased uptake in brain with multiple lung nodules. The above features were suggestive of left occipital lobe brain metastasis in a treated case of triple negative carcinoma breast.
MRI Images of Patient With Single Lesion at the Left Occipital Region With Ring Enhancement and Minimal Edema.
Brain Metastasis Prognostic Index
All patients with brain metastasis should undergo disease specific Graded Prognostic Assessment (GPA). 2 This GPA takes into account various factors such as primary tumor type, molecular profile of tumor, and number of brain metastasis. It helps the physician as well as the patient to choose the appropriate treatment.
In the current case, details of patient such as age of patient at the time of diagnosis of brain metastasis, Karnofsky Performance Status of the patient, number of brain metastasis, tumor type, and molecular subtype were used to calculate the GPA to be 1.5 with median survival of 7.7 months.
Treatment Decision by the Tumor Board
The patient details were put in the tumor board for decision regarding the line to treatment. After group discussion with neurosurgeon, radiation oncologist, and medical oncologist, board decided to plan for stereotactic radiosurgery followed by chemotherapy.
Treatment Decision by the Radiation Tumor Board
TNBC being an aggressive histology, a TNBC patient with brain metastasis would benefit from whole brain radiation with simultaneous integrated boost to the solitary lesion. But basing on the advanced age of the patient, ie 70 years, and in order to prevent development of radiation induced neurological toxicity and deterioration of quality of life, the radiation tumor board opined for SRS. In the present case, there was a single brain metastasis of diameter 2.2 cm, the radiation tumor board decided for single fraction SRS with 18 Gy marginal dose as per RTOG 9005. 3
RT Planning
Here we describe the steps of treatment of brain metastasis from simulation to plan execution
Step 1: CT Simulation
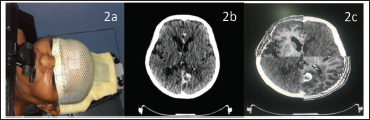
During simulation, patient was set up in the supine position with neutral neck position and immobilization was done using FRAXION thermoplastic mask and stereotactic frame with mouth bite (Figure 2a). Fiducials were placed on the thermoplastic mask after proper alignment with the lasers. Intravenous contrast was given at a dose of 1 mL per kg body weight. Then, CT scan was taken from the vertex to neck with CT slice thickness of 1 mm as is depicted in Table 1 (Figure 2b). After simulation, the DICOM CT, images were sent to our Oncentra server which was then imported for delineation of target and organ at risk (OAR).
Immobilization of the Patient Using the Stereotactic Thermoplastic Mask and Frame During CT Simulation in (2a), the Planning CT Scan in (2b), and Fusion of MRI of the Patient With Planning CT Scan in (2c).
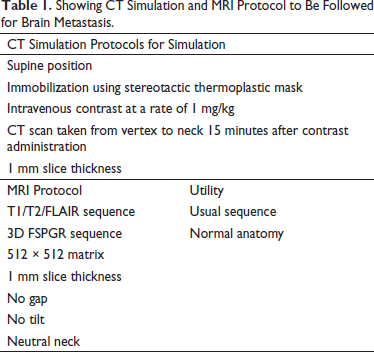
Showing CT Simulation and MRI Protocol to Be Followed for Brain Metastasis.
Step 2: MRI Protocol
MRI of brain of the patient was done using 512 × 512 matrix in the neutral neck position similar to that of CT scan during simulation with no gap, no tilt, and 1 mm slice thickness as depicted in Table 1. The MRI should include the usual T1, T2, FLAIR sequences. In addition, the 3D FSPGR was used to view the normal anatomy. 4 If dedicated MR simulator is available, MR simulation can be done using this MRI protocol and the simulation process being same as the CT simulation mentioned above.
Step 3: Image Fusion
This acquired MRI sequences were fused with the planning CT scan by contouring the eyes, lens, basilar artery, sinuses, and calcification and matching was done using the auto-fusion technique to help in target and OAR delineation (Figure 2c).
Step 4: Target Delineation
The gross tumor seen on the CT images that was fused with the MRI images to consider the exact extension of tumor was delineated as Gross Tumor Volume (GTV) (Figures 3a,b). There is no necessity of Clinical Target Volume margin in case of SRS brain metastasis. The Planning Target Volume (PTV) was drawn taking 1 mm around the GTV (Figure 3c). Smoothing of the contour was done from the adjacent bone. Multi-planar evaluation, ie evaluation of both the GTV and PTV, were done in all the three planes—axial, coronal, and sagittal.
The Delineation of GTV (Pink) in Planning CT Is Shown in 3a, Delineation of GTV (Pink) in MRI Is Shown in 3b and PTV (Cyan) Is Generated by Taking 1 mm Margin Around GTV Shown in 3c.
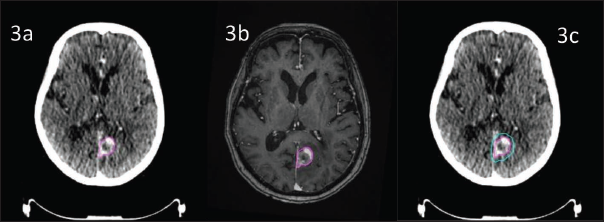
In the present case, the GTV volume was 4.65 cc and the PTV volume was 5.75 cc.
Step 5: Organs at Risk (OAR) Delineation
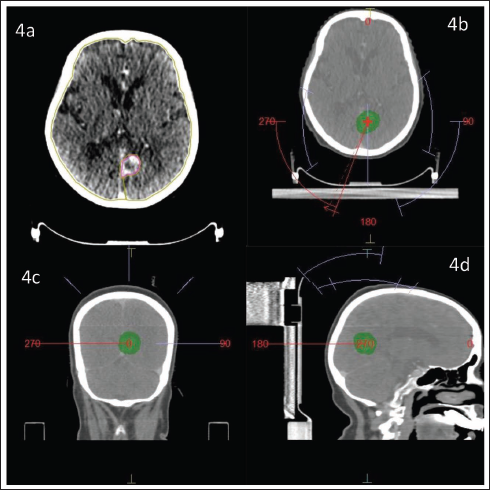
The OARs for delineation included both the cochlea, brainstem, hippocampus, optic chiasma, and optic apparatus. The cochlea was contoured in the bone window setting while other OARs, ie brainstem, hippocampus, optic chiasma, and optic apparatus, were contoured using the MRI that was fused with the planning CT. Also Brain-GTV was also drawn as an OAR (Figure 4a).
Showing the Brain-GTV in 4a and Beam Arrangement in Axial (4b), Cronal (4c), and Sagittal View (4d).
Step 6: RT Technique
Radiation planning can be done using any of the RT techniques such as Intensity Modulated Radiotherapy (IMRT), Volumetric Modulated Arc Therapy (VMAT), Dynamic Conformal Arc Therapy (DCARC), or 3-Dimensional Conformal Radiotherapy (3DCRT) according to convenience of radiation physicist and physician.
In the present case planning was done using the VMAT technique.
Step 7: Plan Evaluation
After the completion of planning by the physicist, the evaluation for the treatment plan was done using the following indices.
PTV Coverage Index
Following planning, the coverage of the PTV need to be seen. The prescription isodose level was such that not 100% of the prescribed dose covered 100% of the PTV. Often 95% of the prescription dose covered 95% or higher percentage of the PTV, otherwise 100% of the prescription dose covered 95% or higher percentage of the PTV. 5
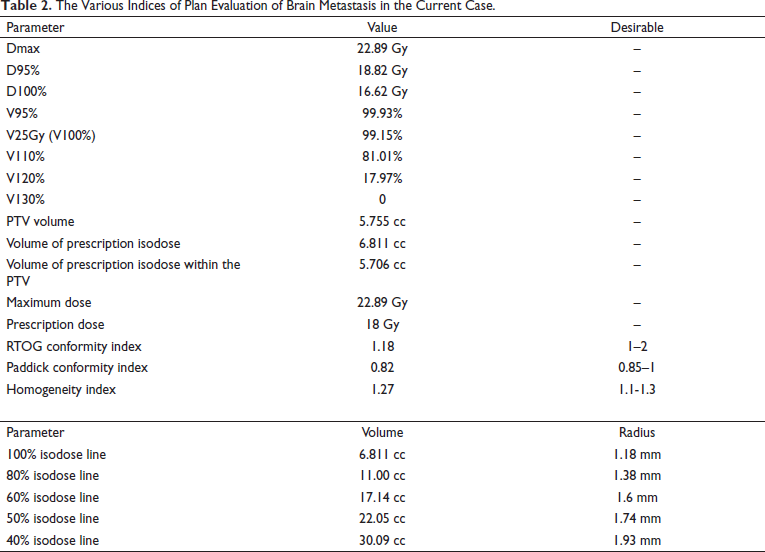
In the present case, 95% of the prescription dose covered 99.9% of the PTV and 100% of the prescription dose covered 99.15% of the PTV which satisfied the above-mentioned parameter for the PTV coverage as depicted in the Table 2.
The Various Indices of Plan Evaluation of Brain Metastasis in the Current Case.
Intracranial Organ at Risk (OAR) Index
Keeping in mind the desirable dose constraints to the OAR we need to check the dose to individual OARs. 6
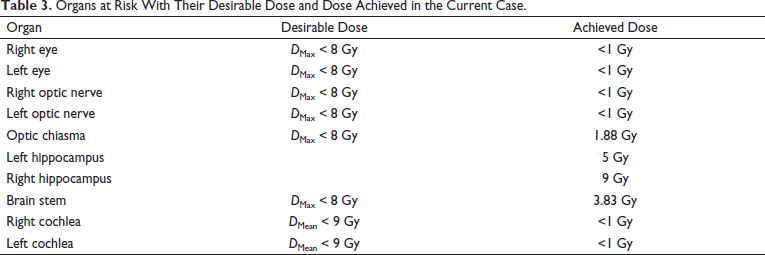
The dose desirable and dose achieved for all the OARs in the present case is depicted in Table 3.
Organs at Risk With Their Desirable Dose and Dose Achieved in the Current Case.
Whole Brain-GTV Dose
Korytko et al have stated that while treating Non-AVM tumors with Gamma Knife, in order to reduce the risk of symptomatic radiation induced necrosis of brain, the dose to 12 Gy volume of Brain-GTV should be limited to <10 cc. 7 This data can be extrapolated while treating patients with single fraction SRS.
In the current case, the 12 Gy volume of Brain-GTV was 10.765 cc.
CIRTOG = Volume of prescription isodose / PTV volume
In this case of VS, the RTOG conformity index was 1.18 (Table 2).
CIPaddick = (Volume of prescription isodose in the area of interest ie PTV) 2 / PTV volume × Volume of prescription isodose
Here in the current case, the Paddick conformity index was 0.82 (Table 2).
Homogeneity Index
It was calculated using the formula:
Homogeneity index = Maximum dose / Prescription dose
In this case the homogeneity index was 1.27 (Table 2).
Dose Fall Off
The dose fall off observation is very much needed in the plan evaluation under the heading of gradient index. For this we need to calculate the difference between various isodose lines. In order to calculate the difference between the isodose lines we need to calculate the equivalent radius.
Equivalent Radius Calculation
To evaluate the dose gradient, we have to find out the difference between radius of various isodose lines. But none of the isodoses are spherical. So, we use the following formula to calculate the equivalent radius.
First: Find out the specified isodose volume
Second: Calculate the radius of the isodose volume by using the formula:
V = 4/3 ύ r 3
r = (3V/4 ύ)*1/3
The calculation of volume and radius of various isodose lines in the present case is shown in Table 2.
Gradient Index
The formula for calculating gradient index is as follows.
Gradient index = Equivalent radius of 50% isodose – Equivalent radius of prescription isodose. Ideally the gradient index should be between 0.3 mm and 0.9 mm.
In the current case, the gradient index was 1.74 mm – 1.18 mm = 0.56 mm which was close to ideal gradient index.
Gradient index can also be calculated as the ratio of the volume enclosed by half of the prescription isodose divided by the prescription isodose volume. The ideal value is < 3. 5
In the present case, the gradient index was calculated by 9 Gy volume / 18 Gy volume, ie 22.2/6.8 = 3.2.
Distance Between Various Isodose Lines
The ideal difference between 80% and 60% isodose lines should be < 2 mm. 9
In the current case it was 0.22 mm.
The ideal difference between 80% and 40% isodose lines should be < 8 mm.
In present case, it was 0.55 mm.
Beam Arrangement
The arrangement of the beams (Figures 4b-d) was done such that there is adequate coverage of the target while giving less dose to the OARs. It should be noted that the beams should not pass through the ipsilateral eye.
Step 8: Quality Assurance (QA)
Mechanical isocenter check was done using the Winston Lutz test and the point dose verification was done keeping the tolerance as 1 mm. 10
Step 9: Dry Run
Treatment verification consists of setup reproduction, isocenter verification, and clinically verifying each treatment field—check beam clearance, check any interlock—MLC interlock and potential monitor unit problems. Then clearly mark the immobilization devices after successful dry run.
Step 10: Premedication Protocol
Prior to start of treatment premedication was delivered in the form of tablets as described further—all starting the day before start of RT treatment:
Tablet Dexamethasone 8 mg—thrice daily Tablet Ondansetron 8 mg—thrice daily Tablet pantoprazole 40 mg—once daily If the patient is diabetic, proper diabetic care needs to be done.
Step 11: Set up Verification and Treatment Delivery
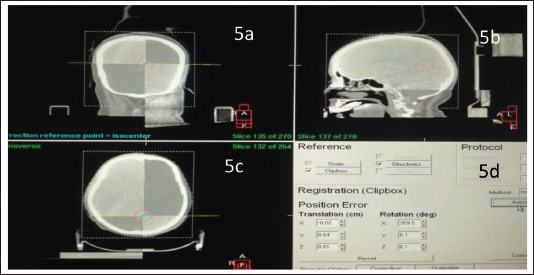
It includes cone beam CT correction (Figures 5a-c) and hexapod corrections (Figure 5d). After all the corrections been done treatment was delivered.
Depicting the Treatment Verification by CBCT Correction of the Patient During the Treatment in Coronal (5a), Sagittal View and (5b), Axial (5c), and the Hexapod Correction of the Same Patient During the Treatment in 5d.
Step 12: Post Medication
It is an optional protocol that usually includes anti emetics, proton pump inhibitors, and tapering the dose of steroid over a week.
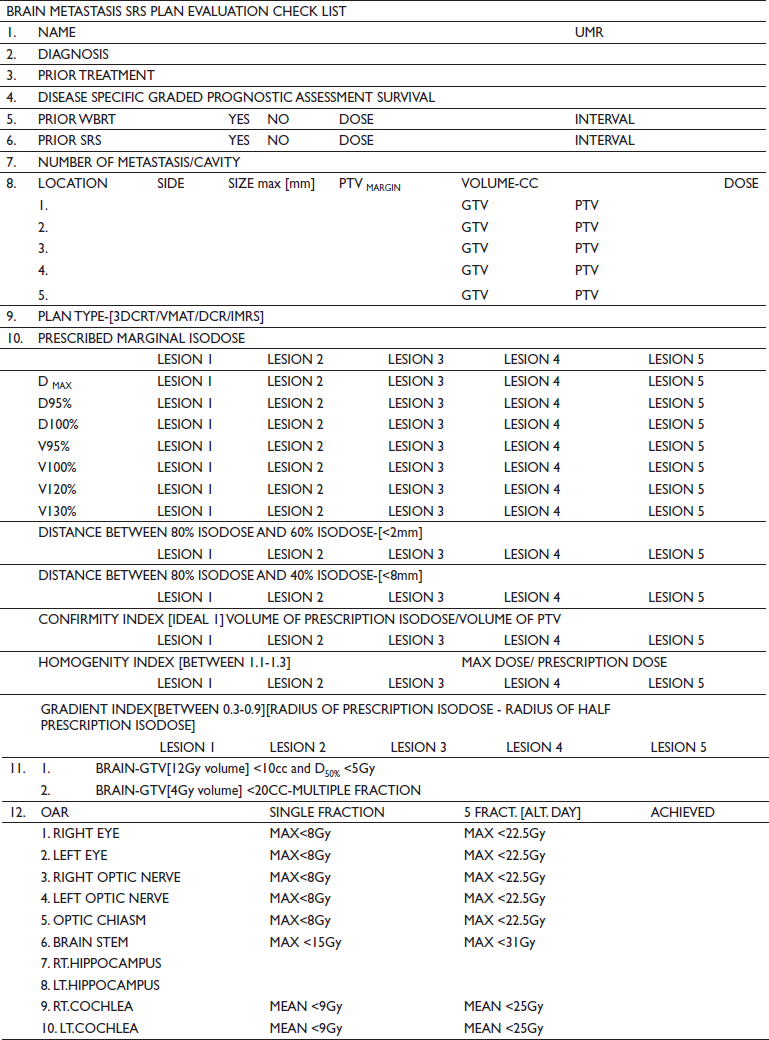
We also provide the Brain Metastasis SRS Plan Evaluation sheet as a supplementary file that will help in proper and accurate plan evaluation for every SRS case of brain metastasis.
Conclusion
This paper conceptualizes and acts as an easy guide for the beginners for the stereotactic radiation planning for brain metastasis.
Appendix
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.