
Abstract
Background
Therapeutic options are limited for unresectable isolated recurrent cervical lymph node (LN). There are different methods of salvaging the recurrent nodes such as surgery, reirradiation by fractionated external beam radiation therapy, stereotactic body radiotherapy, and interstitial brachytherapy. However, interstitial brachytherapy method is very less commonly used. We highlighted a treated case of oropharyngeal cancer with isolated recurrent neck node treated with interstitial brachytherapy under ultrasound guidance.
Methods and materials
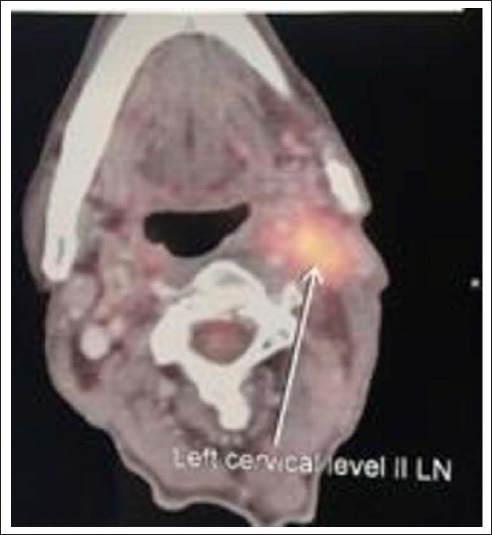
One 60-year-old male patient diagnosed with case of squamous cell carcinoma vallecula with left level II LN, cT2N1M0, was given 70 Gy in conventional fractionation to the gross primary and node and 59 Gy and 56 Gy to the intermediate and low-risk volumes, respectively. Post chemoradiation, we achieved complete metabolic and morphological response of the primary and neck node as well. However, he developed a recurrent fluorodeoxyglucose avid level II LN of size 3×2 cm after 7 months which was fixed. Positron emission tomography (PET) scan showed a PET avid recurrent node abutting the great vessels in the left side.
We treated by computed tomography (CT)-based high-dose-rate interstitial brachytherapy using Ir-192. High-risk clinical target volume was defined as 1.5 cm margin around the gross tumor volume, trying to achieve 100% volume with 95% dose prescribing 35 Gy/10 fractions @ 350cGy/# to HRCTV using Oncentra treatment planning system.
Result
He developed complete metabolic response after 3 month of nodal brachytherapy confirmed by PET CT and remained disease free for 30 months till the last follow-up.
Conclusion
Ultrasonography-guided interstitial nodal brachytherapy is a valid option and feasible in previously irradiated patients with isolated recurrent neck node of head and neck cancers. However, more number of patients needed to be done by similar fashion for adequate data generation and proper conclusion.
Introduction
Isolated cervical lymph node (LN) recurrences occur in approximately 10% of head and neck cancer (HNC) patients following radical treatment.1–3 Despite significant improvements in the treatment of HNC, neck LN recurrences remain a clinical challenge after primary radiotherapy. Therapeutic options are limited for unresectable isolated recurrent cervical LN.4-7 Surgical salvage is the preferable approach for recurrent HNC.8, 9 Only 30% of patients with isolated cervical recurrences are suitable candidates for this approach. 10 Another potential approach interstitial brachytherapy method is very less commonly used. Radical reirradiation by external beam radiation therapy (EBRT) is often not feasible because of significant morbidity on account of previous radiation. 11 Hence, a majority of these patients are treated with supportive care and palliative chemotherapy with poor response and outcome. 12
Brachytherapy plays an important role in obtaining good local control associated with acceptable complication rates in recurrent HNC.1, 3, 4, 6, 7, 11, 13-18 However, a paucity of outcome data exists regarding the treatment of isolated recurrent neck disease with interstitial brachytherapy. In addition, most reports are presenting results utilizing low-dose-rate (LDR) techniques.1, 3, 4, 19 With High-dose-rate brachytherapy (HDR-BRT), dosimetrically equivalent or superior outcomes compared to LDR brachytherapy and EBRT for gynecological tumors and other locations have been achieved.20, 21 However, the same data in head and neck malignancies and the use of interstitial brachytherapy is minimal.
In this article, we demonstrated our first experience of use of HDR-BRT in management of isolated neck nodal recurrence in a treated case of oropharynx.
Methods and Materials
In February 2018, one 60-year-old male patient diagnosed with case of squamous cell carcinoma of vallecula with left level II LN, cT2N1M0, was given 70 Gy in conventional fractionation to the gross primary and node and 59 Gy and 56 Gy to the intermediate and low-risk volumes, respectively. Three months post chemoradiation, we achieved complete metabolic and morphological response of the primary and gross node. After 7 months, he developed an isolated left side level II neck node which was positron emission tomography (PET) avid (Figure 1), abutting the carotids, confirmed by fine needle aspiration cytology. Due to fixity of nodal mass, surgery could not be done and planned for brachytherapy. Primary tumor and initial treatment characteristics are shown in Table 1.
Axial PET CT-image showing a left-sided isolated level IIA recurrent lymph node.
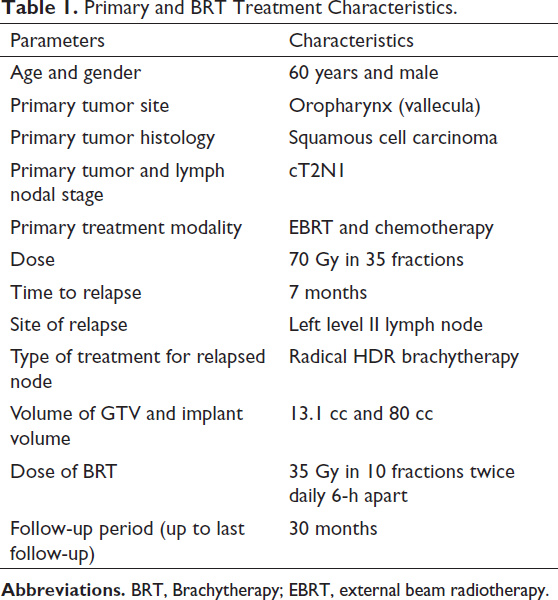
Primary and BRT Treatment Characteristics.
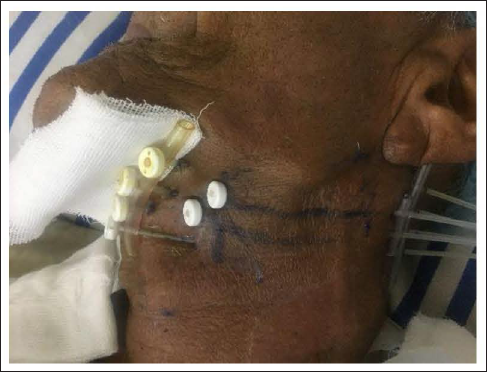
Before brachytherapy, we performed a contrast enhanced computed tomography (CT) scan of head and neck and also contoured the carotid vessels and gross LN to know orientation of exact topography of the LN with respect to the vessels. Similarly, a prebrachytherapy, ultrasound ultrasonography (USG) of neck was performed to correlate the depth of deepest plane of the LN and to correlate with the vessels. A nasogastric tube was placed for feeding at the beginning of the procedure. The implant procedure was performed under general anesthesia with neck in semi-extended position and the exact site of LN marked by ink with 1 cm margin around with exact pathway of needle placement was traced on the surface of skin (Figure 2). The maximum insertion depth, direction, and position of the implanted catheters were estimated by interactive CT scanning done before. With the use of potable ultrasound, straight stainless-steel needles were introduced through the tissue of the LN avoiding puncture of the vessels. Depending upon the predefined depth, a 2-plane implant was performed for adequate coverage of the total LN with margin. Plastic catheters were threaded through each needle and then the needle was removed, leaving the catheter in place. We were able to introduce 6 catheters. The plastic catheters were placed as near parallel as possible at 10-mm interval. The catheters were held to the skin exit points with plastic buttons. With adequate care, CT simulation was done followed by contouring of the gross recurrent LN. Then, brachytherapy plan was developed with adequate coverage with appropriate dwell position of the sources by Oncentra treatment planning system (TPS).
Exact site of implant with ink marks.
Tumor demarcation and corresponding target volume (CTV = GTV + 1.5 cm) delineation were performed using the Oncentra TPS. For 3D dose optimization, active source dwell positions were selected along the catheters to ensure placement inside the CTV and to assure a location at 5.0 to 10.0 mm below the CTV surface. The dosimetric dose distribution is shown in Figure 3. Treatment was performed over consecutive days with an interfractional interval of at least 6 h. He was planned to give 35 Gy/10 fractions @ 350cGy/# to the gross LN by Ir192 HDR with Oncentra TPS. We tried to achieve 95% volume to cover >95% dose. The patient has completed all the planned fractions without any interruption or gap.
Axial CT-image showing a Left-sided submandibular lymph node recurrence with 2D-isodose distribution after CT-based treatment planning for a plane lying centrally to the target extension. The colour gradation represents: brown = 150% isodose, red = 100% isodose, blue = 90% isodose, and green = 80%. The target volume is denoted as red delineated PTV and the interstitial catheters identifiable as dark dots inside it.

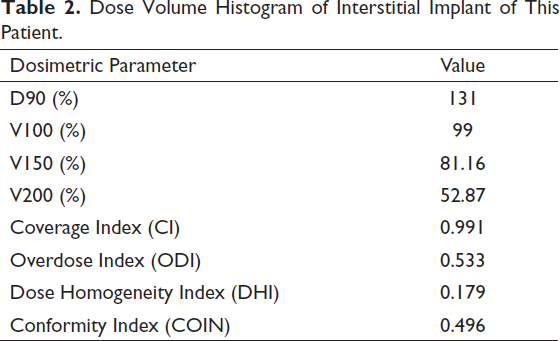
The dose heterogeneity was specified by V100, V150, and V200 (Table 2). Toxicity was graded according to the Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer grading system. 22
Dose Volume Histogram of Interstitial Implant of This Patient.
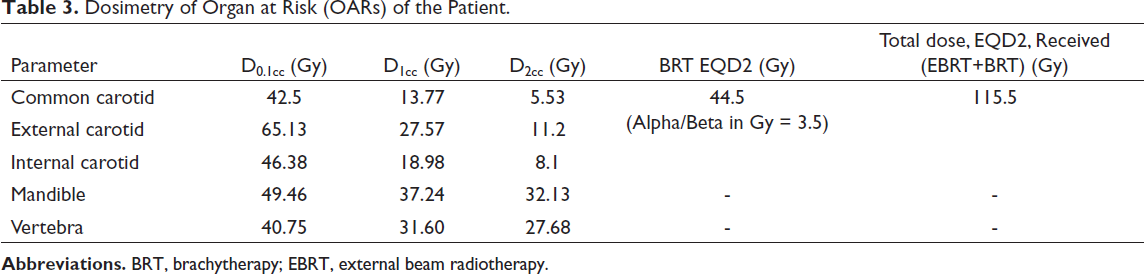
The dosimetry of common carotid, external carotid, and internal carotid artery is depicted in Table 3. The maximum dose to 0.1 cm3 (D0.1cc), 1 cm3 (D1cc), and 2 cm3 (D2cc) of the carotid and the mean carotid dose from HDR brachytherapy were recorded and total dose (EQD2) was calculated.
Dosimetry of Organ at Risk (OARs) of the Patient.
Results
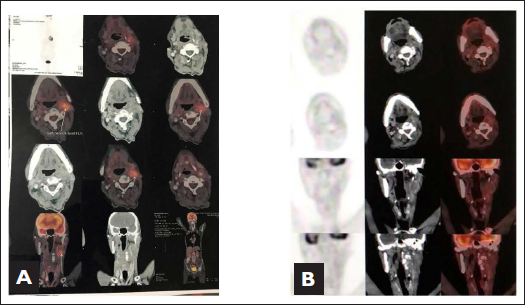
He developed complete clinical, morphological, and metabolic response after 3 month of nodal brachytherapy confirmed by PET CT (Figure 4A, B) and doing absolutely well with regular follow-up every 3 months. His last follow-up was till December of 2020 and then follow-up was lost. On telephonic conversation with relatives, we found that he lost follow-up due to outbreaks of COVID-19 and succumbed in the month of May 2021. The exact cause of death was unknown. However, he was apparently alright without any disease till his last follow-up. He remained complete disease free for 24 months till the last follow-up.
Acute and Late skin reactions after 2 weeks and 6 months of brachytherapy
He developed acute grade 4 skin toxicity (Figure 5A) at the re-irradiated area and healed completely at 2 months of post irradiation. He developed hypopigmentation that remained permanently with grade 2 skin fibrosis. There was no grade 2 or more late skin toxicity (Figure 5B). No incidence of delayed wound healing or carotid blowout or infection was found.
Axial PETCT before and after brachytherapy showing response evaluation.

Discussion
Therapeutic options are limited for isolated neck nodal recurrence and high-level evidence is rare. While surgical resection is the widely preferred salvage attempt for isolated neck disease, only about 20% to 30% of patients seem to be suitable for this approach, leading to overall 5-year survival of 20% to 30%.5, 23-26 Surgical salvage following definitive chemoradiotherapy may be successful in selective salvageable patients in isolated neck node recurrences. EBRT can lead to severe local toxicities in view of reirradiation to the primary. 27 When reirradiation is the only remaining salvage option, BRT has demonstrated effectiveness in the management of locally recurrent head- and neck lesions which develop within previously irradiated volumes.16, 17, 28-32 However, clinical data on the role of BRT in isolated cervical lymphadenopathy from HNC are rare and most authors’ reports result with LDR- and not HDR-techniques.
HDR-BRT, however, can deliver a high dose directly to the target volume, and provides the advantage of rapid dose fall-off, thereby allowing for sparing of normal tissue.11, 18, 33 Even with the advent of technologies and the use of intensity-modulated radiotherapy growing, the toxicity levels with brachytherapy have found to be better compared to the newer treatment advents due to the advantage provided by brachytherapy. Results of retrospective literature show that HDR interstitial brachytherapy has shown acceptable local control and overall survival rates along with tolerable toxicities and morbidity in recurrent HNCs. 34 However, in the series of cases, all the recurrences in the primary sites are either in the oral cavity or oropharynx. None of the cases was implanted in the neck node or excluded from the study.
Largest retrospective study treated 74 patients of inoperable neck node recurrent patients who were treated with radical radiotherapy with or without chemotherapy by interstitial Ir-192 interstitial HDR brachytherapy of medial salvage dose of 30 Gy (12-36 Gy) twice daily from 2000 to 2007. 23 The Local control rate was approximately 67% in 1, 2, and 3 years. The 1-, 2-, and 3-year disease free survival (DFI) was 42%, 37%, and 19%, respectively. Our patient was also treated by similar fashion with a salvage dose of 35 Gy twice daily doses of 6-h apart for 5 days. There was acute grade 4 reaction post radiation but there were no late grade 3 or 4 complications till the last follow-up of DFI more than 2 years.
While focusing upon toxicity, in addition to survival, severe complication rates of up to 36%, including 7% grade V toxicity, have been reported that showed the rate of severe complication rate is 13% including pharyngeal cutaneous fistula without grade V toxicity in his retrospective series. 23
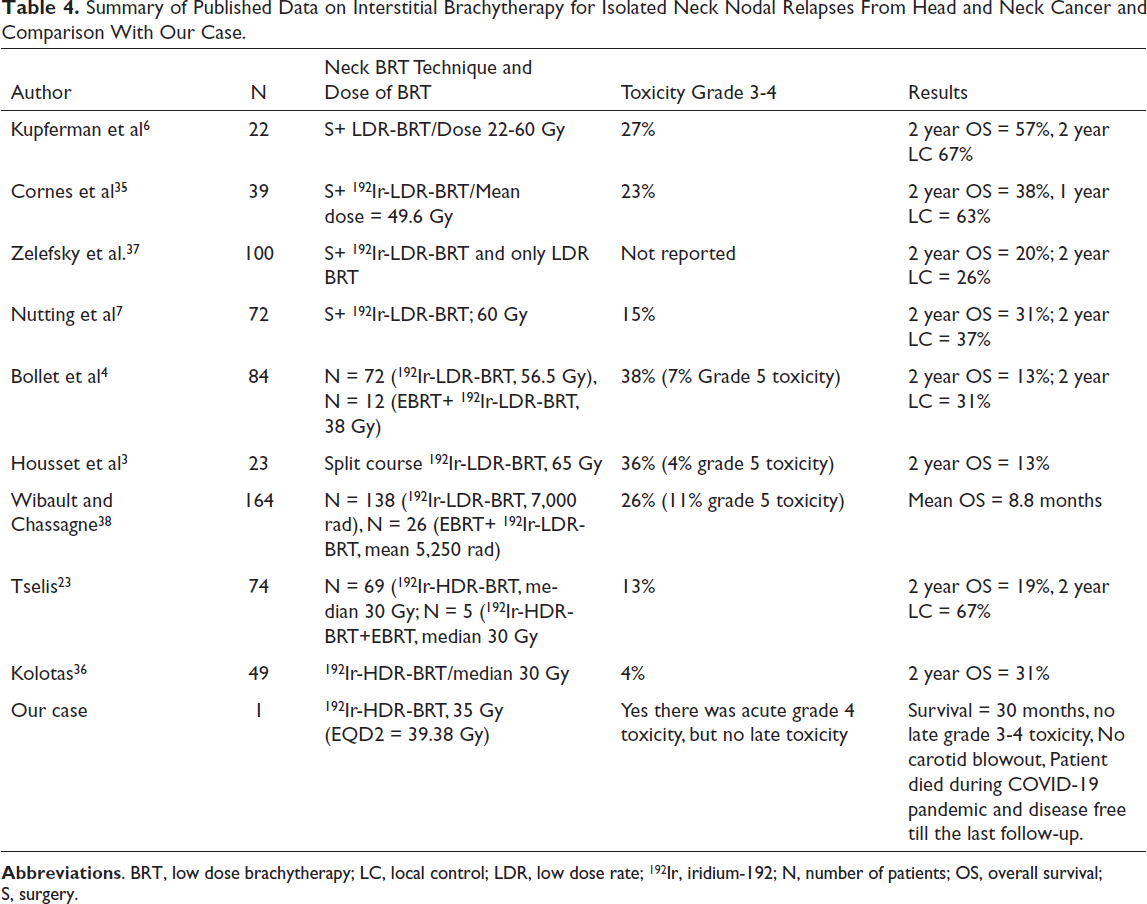
There are few limitations in this study. First, this is only 1 single case showing good survival which is not enough to conclude and second, there may be some dosimetric discordance of achieving ideal brachytherapy plan. To our knowledge, there were only 2 studies showing results of 192Ir-HDR-BRT of recurrent neck nodes (Table 4). Although this was a case report, it showed that HDR interstitial brachytherapy demonstrated a better local control probability with an acceptable toxicity.
Summary of Published Data on Interstitial Brachytherapy for Isolated Neck Nodal Relapses From Head and Neck Cancer and Comparison With Our Case.
Conclusions
Reirradiation of recurrent HNC is a therapeutic challenge. USG-guided interstitial nodal brachytherapy is a valid option and feasible and provides efficacious treatment in previously irradiated patients with isolated recurrent neck node of HNCs. However, more number of patients are needed to be done for adequate data generation and proper conclusion.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
For publication, the relatives of the patient have been informed and consent has been taken for the same.