
Abstract
Keywords
Introduction
Mild cognitive impairment (MCI) represents a crucial point in the spectrum of cognitive health, signifying a departure from normal aging and potentially foreshadowing the onset of dementias such as Alzheimer's disease (AD). With an estimated one third of those over 65 affected by MCI, the condition poses a considerable public health challenge. 1 Precise and early identification of MCI is essential, as it holds the promise of timely interventions that may decelerate its progression.
The subtle nature of MCI symptoms and its overlap with normal cognitive aging complicate its diagnosis. Clinicians and researchers rely on a range of cognitive assessment tools, each with its own strengths and limitations, to distinguish MCI from typical aging. Central to the efficacy of these instruments, like the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), are their psychometric properties, such as sensitivity, specificity, and reliability.
This review aims to conduct a systematic evaluation of these scales, incorporating the COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) scoring system—a framework that rates the quality of tools based on measurement properties including internal consistency, structural validity, and reliability. 2 By examining these properties across various MCI scales, the review seeks to determine which instruments provide the most accurate diagnostic capabilities for MCI in different patient populations and care settings. The findings have the potential to significantly impact clinical practice, improving the accuracy of MCI diagnostics and, ultimately, patient care strategies.
Methods
Design
This systematic review adopts the refined COSMIN approach, a methodology tailored for systematic evaluations of Patient-Reported Outcome Measures.3–5 Our methodology adheres to the updated guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and conforms to AMSTAR (A MeaSurement Tool to Assess systematic Reviews) criteria, which assess the methodological rigor of systematic review.6,7 This approach ensures a comprehensive, standardized, and transparent review process, allowing for an objective and reliable evaluation of the included studies.
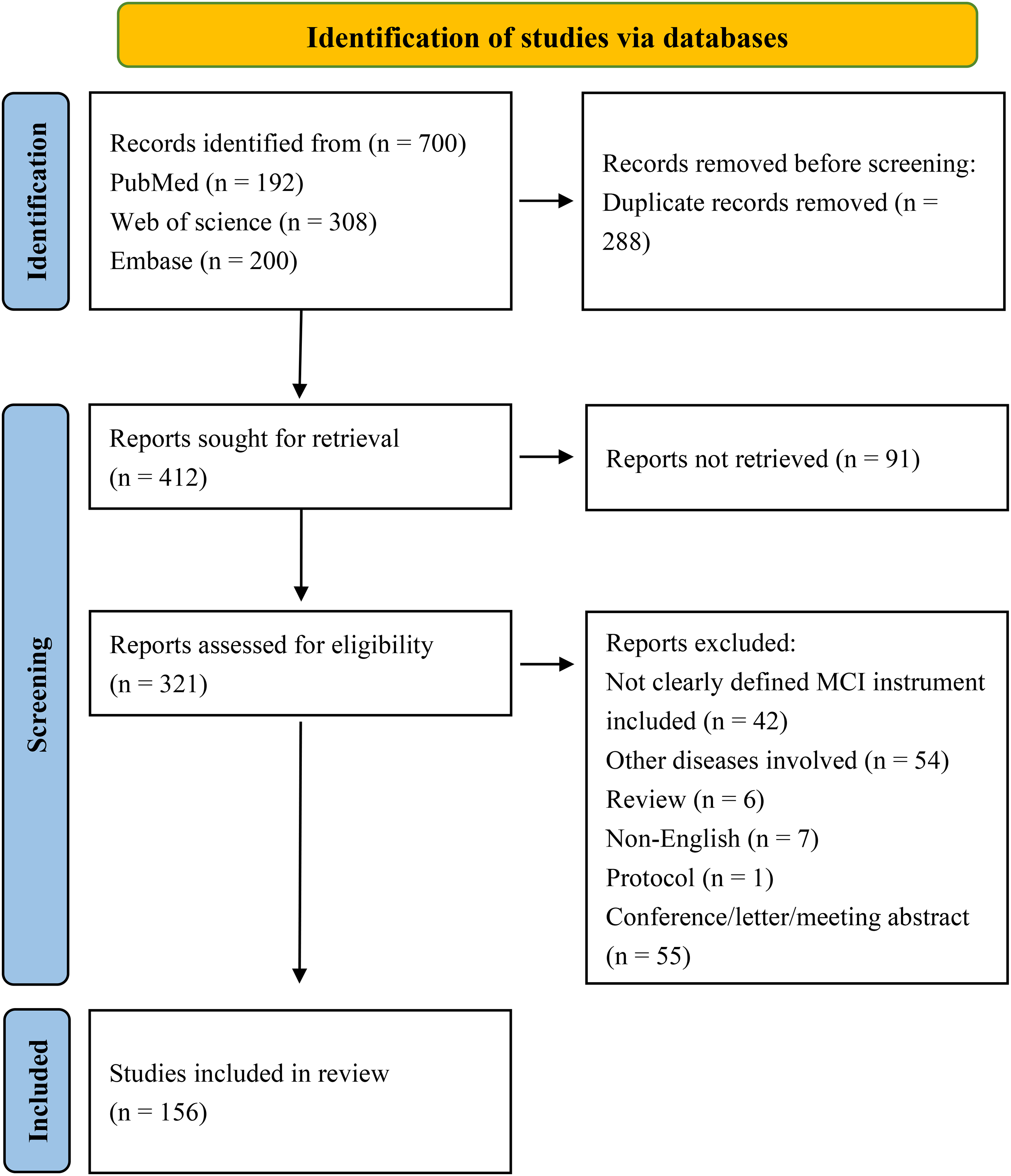
Study flow chart.
Search strategy
Our search strategy (Figure 1) systematically identified studies relevant to the assessment of MCI using various scales, with a particular focus on the COSMIN scores for these tools. Comprehensive searches were conducted across databases, including PubMed, Web of Science, and Embase, from their inception until December 2023. We used a combination of keywords and MeSH terms tailored to the constructs of interest. Keywords included “Mild Cognitive Impairment,” “MCI screening,” “COSMIN,” “neuropsychological tests,” “internal consistency,” “reliability,” “validity,” “sensitivity,” and “specificity.” Boolean operators such as “AND” and “OR” were used to broaden or narrow the searches as necessary. For example, our search strings included combinations like (“MCI” OR “cognitive impairment, mild”) AND “assessment scales” AND “COSMIN scoring” OR “psychometric properties.” All identified records underwent a rigorous screening process, and the search strategy was supplemented by reviewing the references of key articles. The specifics of the search strings, including the full array of search terms and the logic of their combination, are detailed in Figure 1 and Tables 1–7.
Measurement properties of performance-based measures: validity.
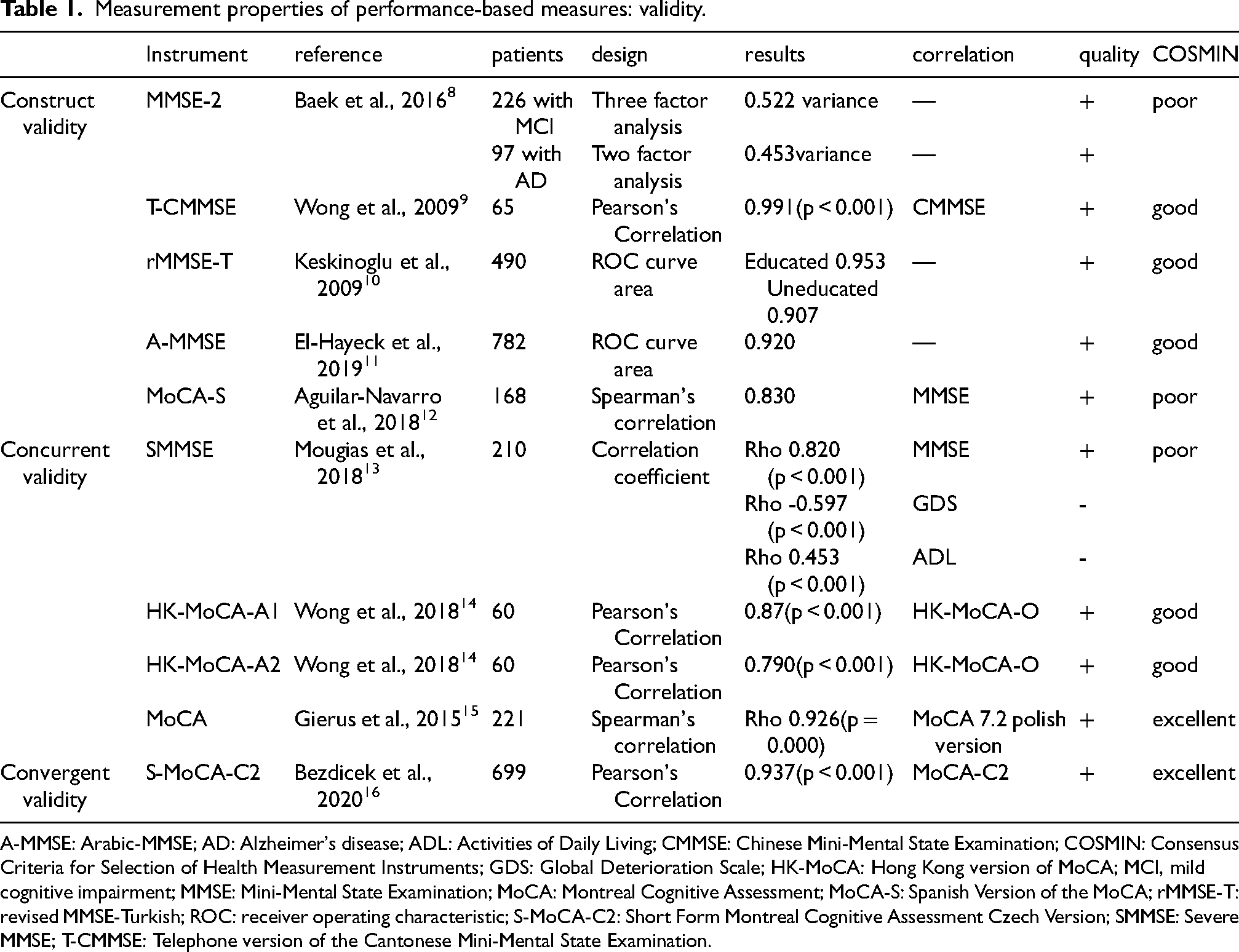
A-MMSE: Arabic-MMSE; AD: Alzheimer's disease; ADL: Activities of Daily Living; CMMSE: Chinese Mini-Mental State Examination; COSMIN: Consensus Criteria for Selection of Health Measurement Instruments; GDS: Global Deterioration Scale; HK-MoCA: Hong Kong version of MoCA; MCI, mild cognitive impairment; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; MoCA-S: Spanish Version of the MoCA; rMMSE-T: revised MMSE-Turkish; ROC: receiver operating characteristic; S-MoCA-C2: Short Form Montreal Cognitive Assessment Czech Version; SMMSE: Severe MMSE; T-CMMSE: Telephone version of the Cantonese Mini-Mental State Examination.
Measurement properties of performance-based measures: reliability.
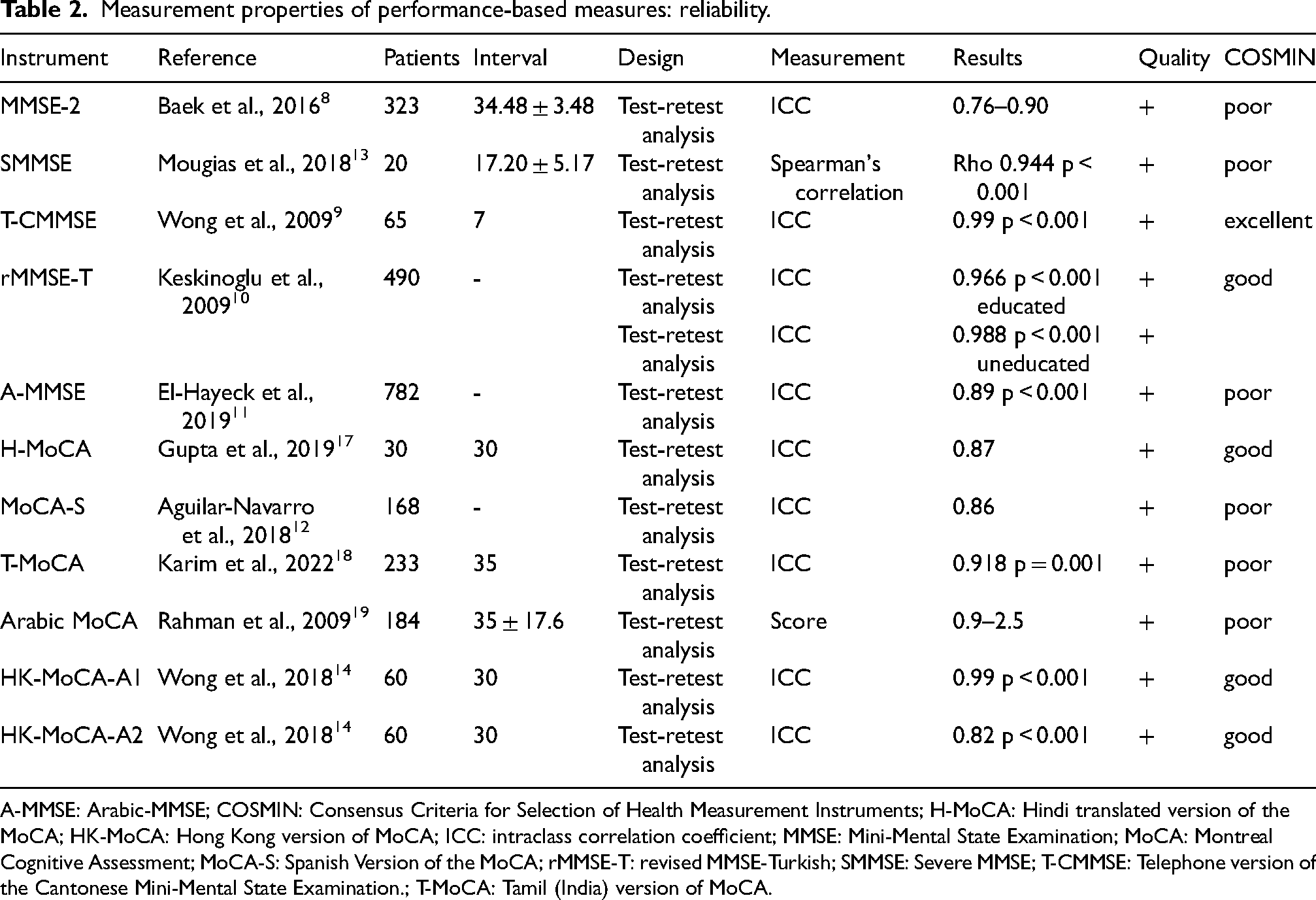
A-MMSE: Arabic-MMSE; COSMIN: Consensus Criteria for Selection of Health Measurement Instruments; H-MoCA: Hindi translated version of the MoCA; HK-MoCA: Hong Kong version of MoCA; ICC: intraclass correlation coefficient; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; MoCA-S: Spanish Version of the MoCA; rMMSE-T: revised MMSE-Turkish; SMMSE: Severe MMSE; T-CMMSE: Telephone version of the Cantonese Mini-Mental State Examination.; T-MoCA: Tamil (India) version of MoCA.
Measurement properties of performance-based measures: internal consistency.
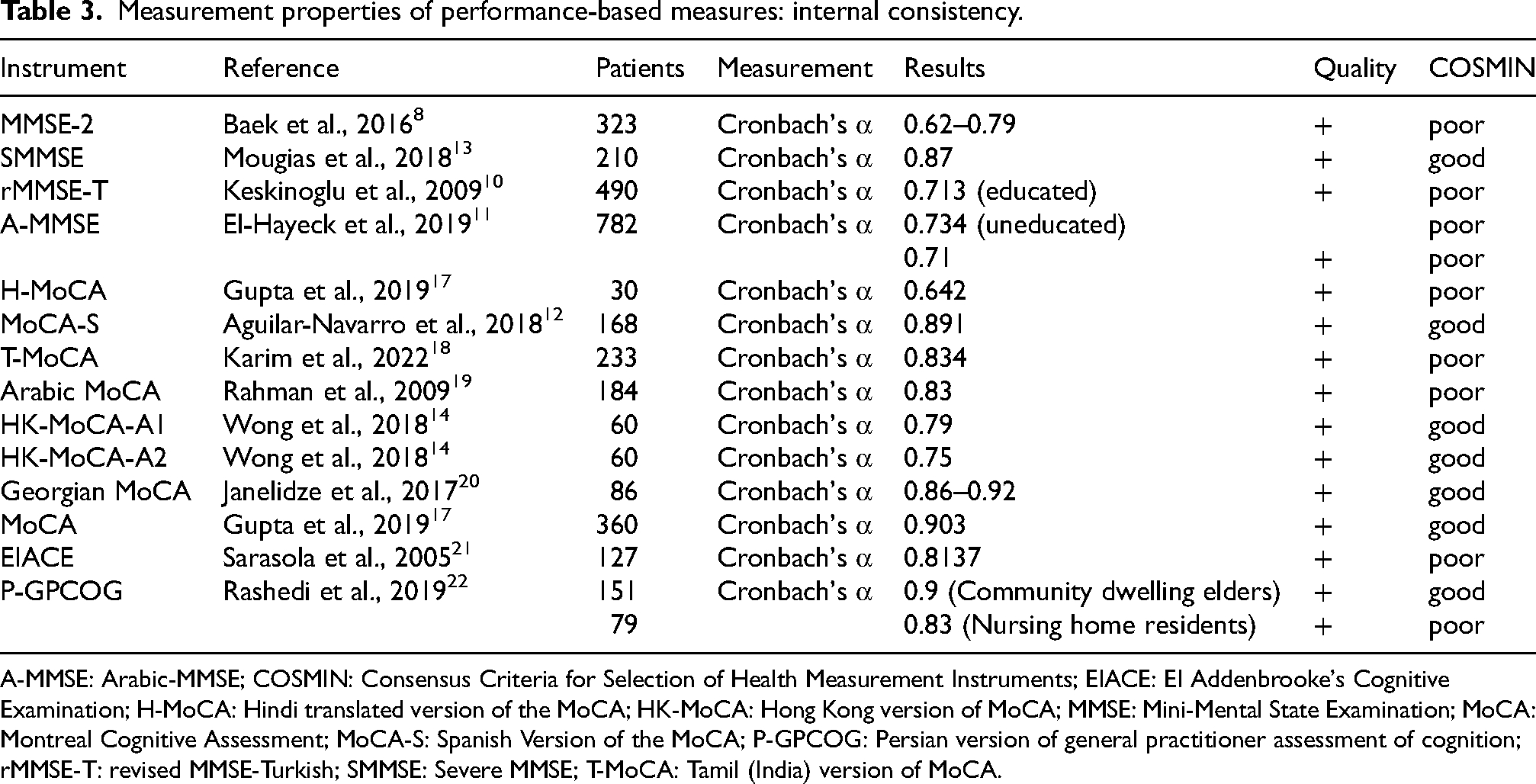
A-MMSE: Arabic-MMSE; COSMIN: Consensus Criteria for Selection of Health Measurement Instruments; EIACE: EI Addenbrooke's Cognitive Examination; H-MoCA: Hindi translated version of the MoCA; HK-MoCA: Hong Kong version of MoCA; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; MoCA-S: Spanish Version of the MoCA; P-GPCOG: Persian version of general practitioner assessment of cognition; rMMSE-T: revised MMSE-Turkish; SMMSE: Severe MMSE; T-MoCA: Tamil (India) version of MoCA.
Measurement properties of performance-based measures: sensitivity and specificity.
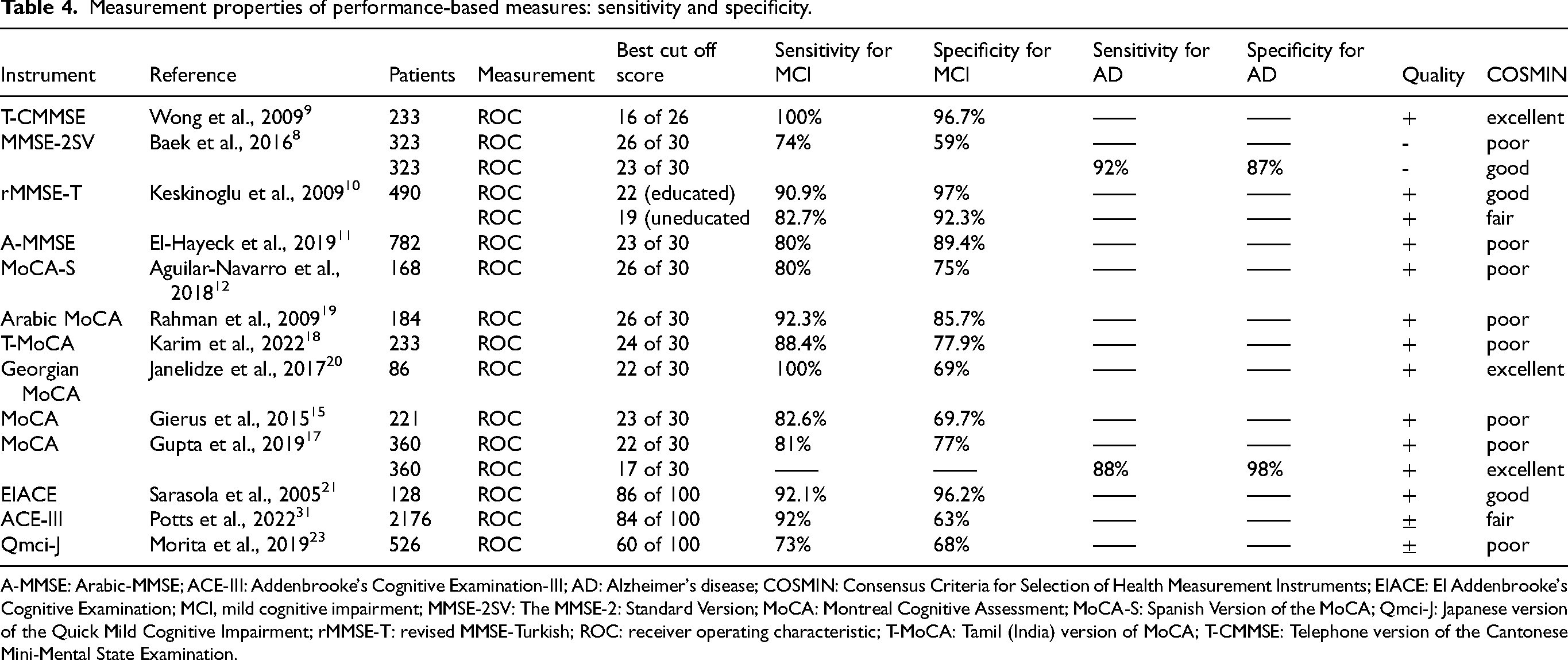
A-MMSE: Arabic-MMSE; ACE-III: Addenbrooke's Cognitive Examination-III; AD: Alzheimer's disease; COSMIN: Consensus Criteria for Selection of Health Measurement Instruments; EIACE: EI Addenbrooke's Cognitive Examination; MCI, mild cognitive impairment; MMSE-2SV: The MMSE-2: Standard Version; MoCA: Montreal Cognitive Assessment; MoCA-S: Spanish Version of the MoCA; Qmci-J: Japanese version of the Quick Mild Cognitive Impairment; rMMSE-T: revised MMSE-Turkish; ROC: receiver operating characteristic; T-MoCA: Tamil (India) version of MoCA; T-CMMSE: Telephone version of the Cantonese Mini-Mental State Examination.
Summary of measurement properties.
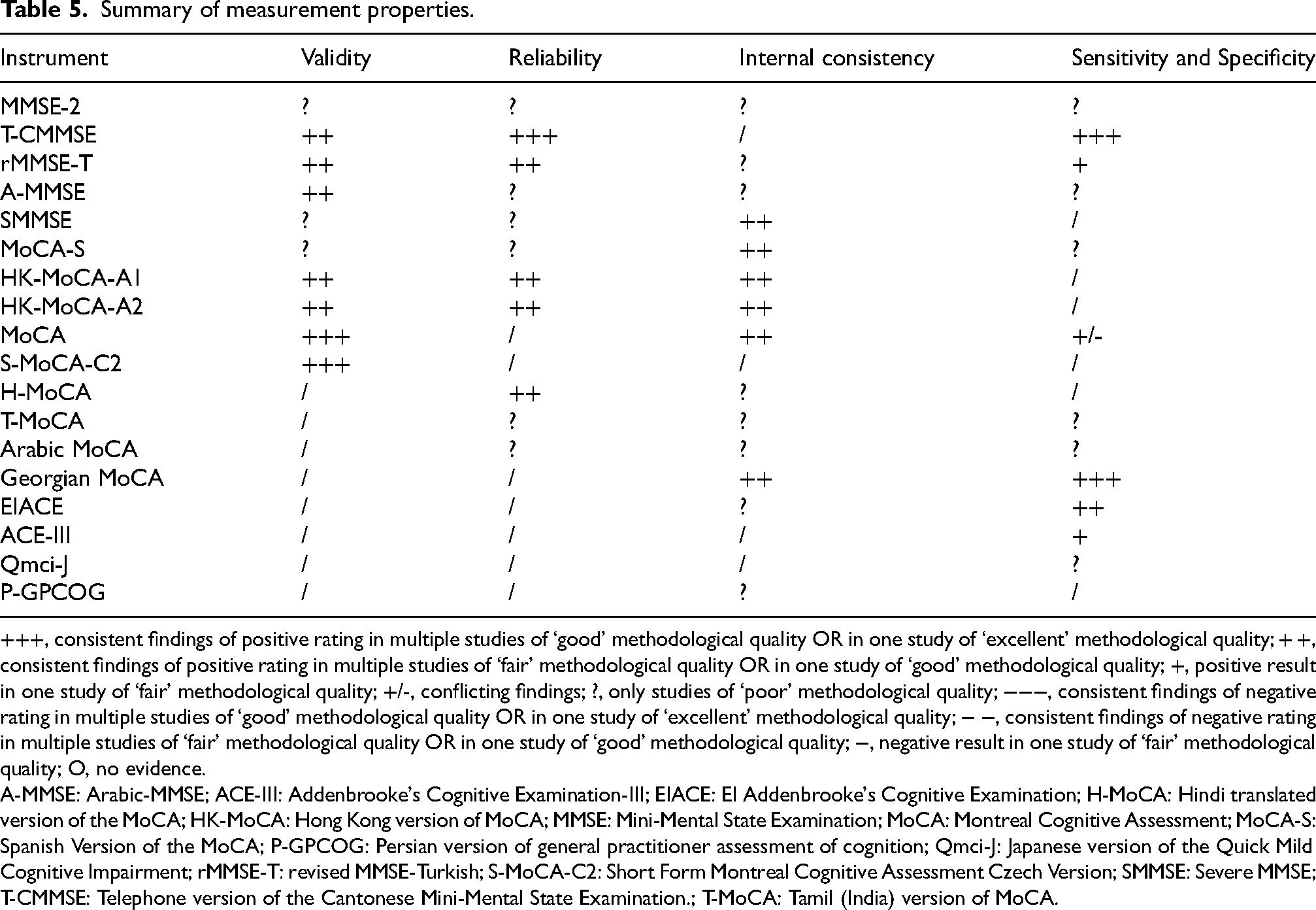
+++, consistent findings of positive rating in multiple studies of ‘good’ methodological quality OR in one study of ‘excellent’ methodological quality; + +, consistent findings of positive rating in multiple studies of ‘fair’ methodological quality OR in one study of ‘good’ methodological quality; +, positive result in one study of ‘fair’ methodological quality; +/-, conflicting findings; ?, only studies of ‘poor’ methodological quality; −−−, consistent findings of negative rating in multiple studies of ‘good’ methodological quality OR in one study of ‘excellent’ methodological quality; − −, consistent findings of negative rating in multiple studies of ‘fair’ methodological quality OR in one study of ‘good’ methodological quality; −, negative result in one study of ‘fair’ methodological quality; O, no evidence.
A-MMSE: Arabic-MMSE; ACE-III: Addenbrooke's Cognitive Examination-III; EIACE: EI Addenbrooke's Cognitive Examination; H-MoCA: Hindi translated version of the MoCA; HK-MoCA: Hong Kong version of MoCA; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; MoCA-S: Spanish Version of the MoCA; P-GPCOG: Persian version of general practitioner assessment of cognition; Qmci-J: Japanese version of the Quick Mild Cognitive Impairment; rMMSE-T: revised MMSE-Turkish; S-MoCA-C2: Short Form Montreal Cognitive Assessment Czech Version; SMMSE: Severe MMSE; T-CMMSE: Telephone version of the Cantonese Mini-Mental State Examination.; T-MoCA: Tamil (India) version of MoCA.
Articles included in the review with COSMIN methodological evaluation scores.
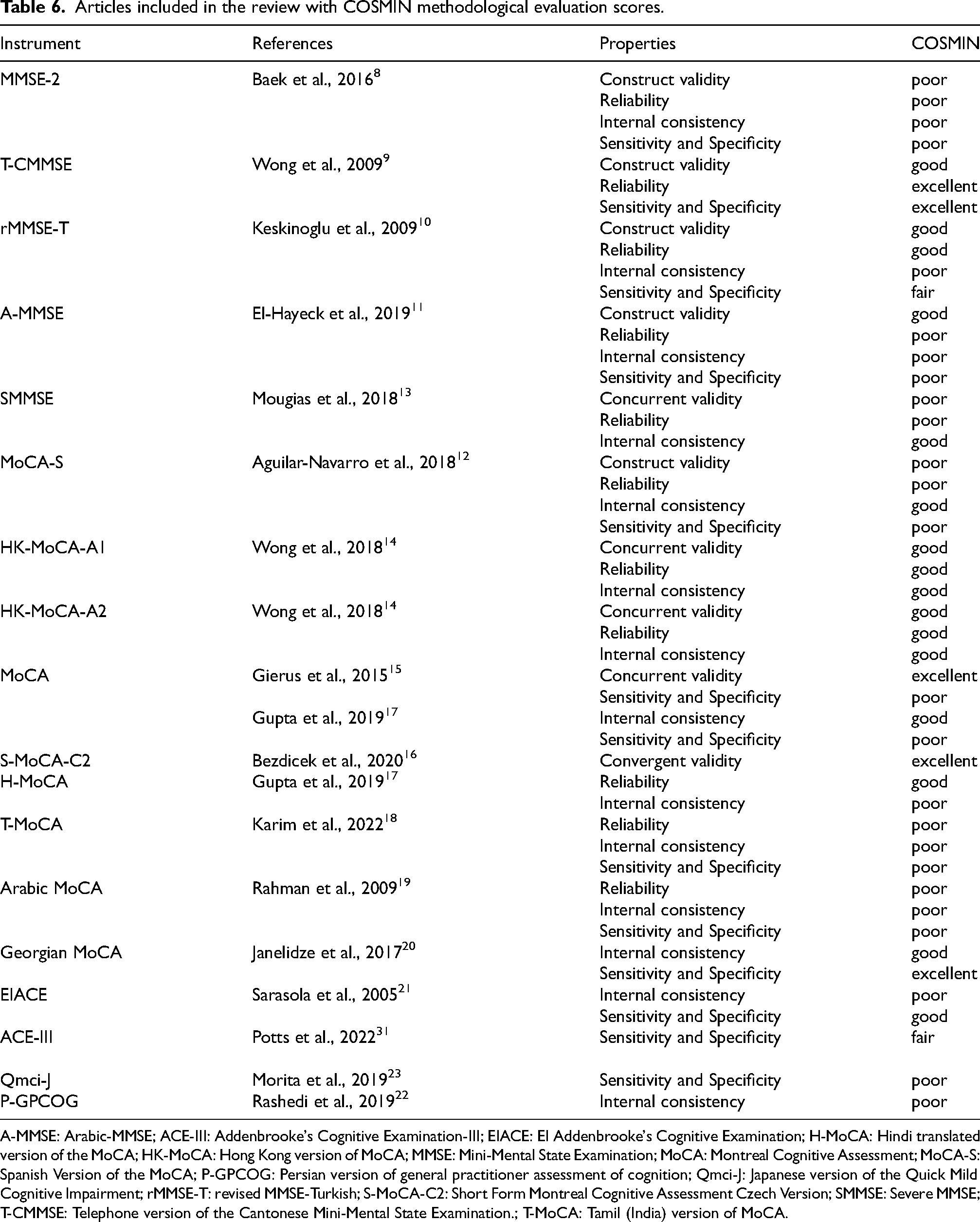
A-MMSE: Arabic-MMSE; ACE-III: Addenbrooke's Cognitive Examination-III; EIACE: EI Addenbrooke's Cognitive Examination; H-MoCA: Hindi translated version of the MoCA; HK-MoCA: Hong Kong version of MoCA; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; MoCA-S: Spanish Version of the MoCA; P-GPCOG: Persian version of general practitioner assessment of cognition; Qmci-J: Japanese version of the Quick Mild Cognitive Impairment; rMMSE-T: revised MMSE-Turkish; S-MoCA-C2: Short Form Montreal Cognitive Assessment Czech Version; SMMSE: Severe MMSE; T-CMMSE: Telephone version of the Cantonese Mini-Mental State Examination.; T-MoCA: Tamil (India) version of MoCA.
Details of the included instruments.
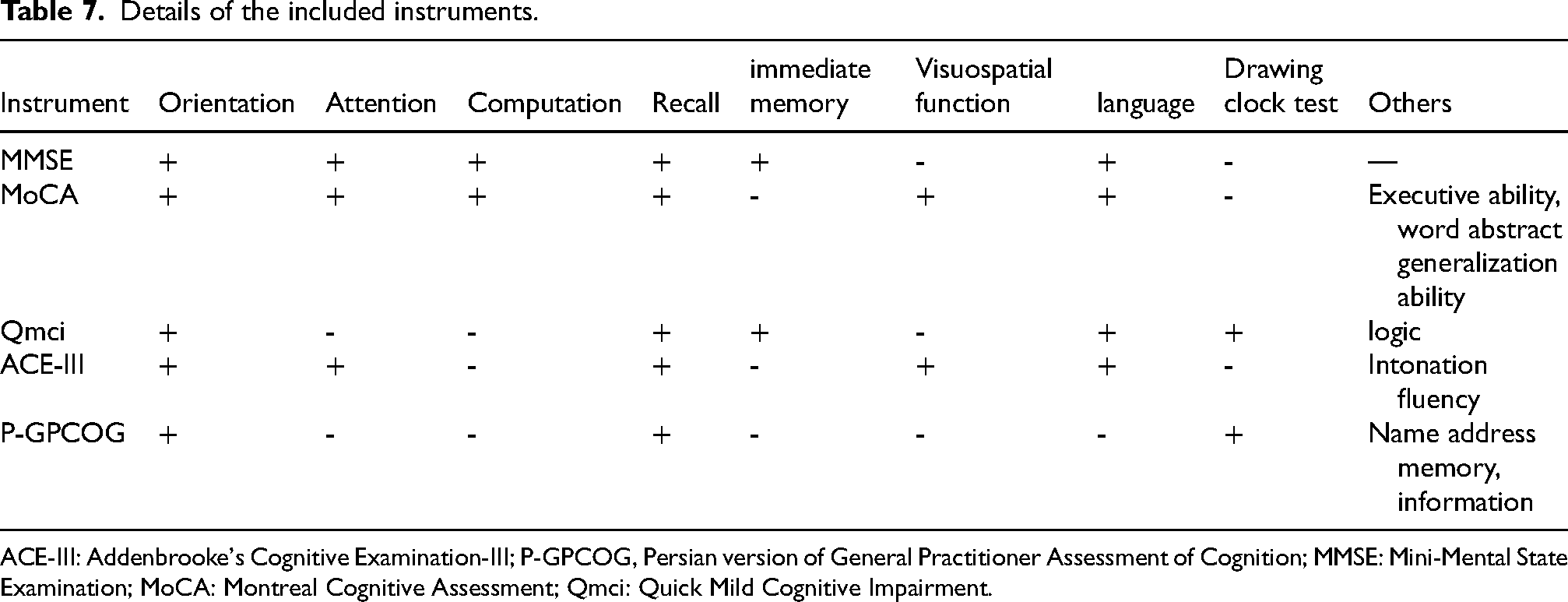
ACE-III: Addenbrooke's Cognitive Examination-III; P-GPCOG, Persian version of General Practitioner Assessment of Cognition; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; Qmci: Quick Mild Cognitive Impairment.
Eligibility criteria
A screening process based on titles and abstracts was first conducted to exclude irrelevant studies. Subsequently, articles that potentially met the inclusion criteria were independently evaluated by two reviewers through a comprehensive full-text examination. Conflicts regarding the eligibility of studies were resolved through discussion and consultation with a third reviewer with significant expertise. Inclusion criteria encompassed quantitative studies, including both randomized controlled trials and observational studies, published as full-text original articles. Exclusions were made for brief communications such as letters, editorials, and conference abstracts, focusing the review on comprehensive scholarly reports.
Participants
Patients who received a confirmed diagnosis of MCI or AD by clinical assessment, neuropsychological testing, magnetic resonance imaging or positron emission tomography scans, blood tests, and/or psychiatric evaluation.
Language
The search for studies was confined to those documented in either English or Spanish.
Setting
A manual search was conducted to identify relevant studies beyond electronic databases. The initial screening of studies was jointly performed by two investigators based on the study titles and abstracts. This step was followed by an independent, detailed review of the full texts by a separate pair of researchers. A collaborative approach was used to resolve any disagreements. In cases of multiple reports originating from a single study, characterized by overlapping authorship, methodology, and patient cohorts, priority was given to the initial report. Subsequent reports were only considered if they provided additional insights or outcomes.
Data extraction
Data from included studies were extracted and compiled into a structured template, including variables such as sample size, mean age of participants, gender, study setting, country, language, and details of subscales, including the number of items and scale parameters. Additionally, we used the Excel template recommended by COSMIN, available on their official website, to record our evaluations and to assist in determining the methodological quality ratings for each domain of interest.
Handling missing data
In instances where data were incomplete or combined with data from patients with other diseases, we contacted the original authors directly, requesting the specific data related to MCI or AD cohorts. This step ensured the accuracy and comprehensiveness of our dataset for analysis.
Evaluation of the measurement property result studies
The evaluation of the studies’ measurement properties was conducted using the COSMIN methodology, which covers a wide range of measurement properties, including but not limited to internal consistency, reliability, measurement error, various aspects of validity (content, construct, cross-cultural, and criterion), responsiveness, and interpretability. Each property within a study was carefully assessed and assigned a quality rating - ‘excellent’, ‘good’, ‘fair’, or ‘poor’. The depth of COSMIN analysis varied per study, depending on the extent of measurement properties examined, resulting in different assessments across the reviewed literature.
Evaluation of the methodological quality of the studies
The methodological rigor of the studies was rated using the COSMIN framework, which defines four levels – poor, fair, good, and excellent. 24 This evaluation process was carried out by two independent researchers, with each measurement property being assigned an overall grade based on its lowest individual score. A third expert reviewer was consulted to mediate and resolve any analytic discrepancies that arose between the initial assessors, thereby ensuring a thorough and objective evaluation of each study's methodological integrity.
Best evidence synthesis: Levels of evidence
Our analysis integrated three distinct dimensions to evaluate the robustness of each measurement property in the assessed questionnaires. First, we employed the COSMIN checklist to determine the methodological quality (detailed in Table 6). Second, we assessed the outcomes of the measurement properties. Finally, we applied the criteria set forth by Terwee et al. 25 (detailed in Tables 1–7). This comprehensive approach allowed for a thorough evaluation of the measurement properties.
In cases where clinical and methodological homogeneity existed among the studies, we employed quantitative synthesis to summarize the outcome measures. Conversely, when substantial heterogeneity was present across the studies, we applied qualitative summary techniques. This dual approach facilitated a nuanced and in-depth understanding of the measurement properties within the scope of our review, enabling us to account for both the commonalities and the differences among the included studies.
By integrating these three dimensions—methodological quality, assessment of measurement property outcomes, and the application of standardized criteria—our analysis provided a robust and comprehensive evaluation of the questionnaires. This methodology not only allowed for a systematic appraisal of the measurement properties but also ensured that the findings were grounded in a well-established framework, enhancing the reliability and validity of our conclusions.
Results
Measurement properties
Internal consistency
The internal consistency of various MCI assessment scales was examined using the COSMIN checklist to evaluate their methodological quality and reliability of each instrument was assessed with Cronbach's alpha, ensuring consistent measurement of cognitive constructs.
Several cognitive assessment tools demonstrated satisfactory to excellent internal consistency, as evidenced by their Cronbach's alpha values and COSMIN scores. The MMSE-2, which involved 323 participants, demonstrated a Cronbach's alpha between 0.62 and 0.79. 8 This range indicates satisfactory internal consistency, as evidenced by a positive COSMIN score. Similarly, the Severe MMSE (SMMSE) sampled 210 individuals and reported a Cronbach's alpha of 0.87, suggesting high internal consistency, supported by a positive COSMIN score. 13
The revised MMSE-Turkish (rMMSE-T), administered to 490 patients, yielded Cronbach's alpha values of 0.713 for educated subjects and 0.734 for uneducated ones, both with positive COSMIN scores. 10 The Arabic-MMSE (A-MMSE), applied to 782 patients, yielded a Cronbach's alpha of 0.71, confirming consistent performance with a positive COSMIN rating. 11 The Hindi translated version of the MoCA (H-MoCA), administered to 30 individuals, resulted in a Cronbach's alpha of 0.642, indicating moderate internal consistency but a poor COSMIN score, suggesting the need for further validation. 17 In contrast, the Spanish Version of the MoCA (MoCA-S), involving 168 subjects, demonstrated high internal consistency (Cronbach's alpha = 0.891) but a poor COSMIN score. 12 The Tamil (India) version of MoCA (T-MoCA) reported a Cronbach's alpha of 0.834 from 233 participants, along with a positive COSMIN score. 18
Furthermore, the Arabic MoCA and the Hong Kong version of MoCA (HK-MoCA-A1) demonstrated good internal consistency. The Arabic MoCA (184 participants) and HK-MoCA-A1 (60 individuals) exhibited good internal consistency, with Cronbach's alpha values of 0.83 and 0.79, respectively, and positive COSMIN scores.14,19 The HK-MoCA-A2 (60 patients) and Georgian MoCA (86 participants) showed Cronbach's alpha values of 0.75 and 0.86–0.92, respectively. 20 The MoCA, with a larger sample of 360 patients, displayed excellent internal consistency (Cronbach's alpha = 0.903) and a positive COSMIN score. 26 Finally, the El Addenbrooke's Cognitive Examination (EIACE; 127 subjects) and Persian version of general practitioner assessment of cognition (P-GPCOG; assessed in 151 community-dwelling elders and 79 nursing home residents) demonstrated high internal consistency, with Cronbach's alpha values of 0.8137, 0.9, and 0.83, respectively, and positive COSMIN ratings.21,22
Reliability
Several cognitive assessment tools were evaluated for their test-retest reliability to ensure consistency of results over time.
The MMSE-2, involving 323 participants, showed an impressive intraclass correlation coefficient (ICC) between 0.76 and 0.90, indicating high reliability. The SMMSE, with 20 subjects, demonstrated a strong Spearman's correlation coefficient (rho) of 0.944 (p < 0.001), reflecting consistent performance in repeated assessments.
The Telephone version of the Cantonese Mini-Mental State Examination (T-CMMSE), including 65 participants, achieved an outstanding ICC of 0.99 (p < 0.001), indicating excellent test-retest reliability and supported by an ‘excellent’ COSMIN score. 9 This finding was further supported by an ‘excellent’ COSMIN score. The rMMSE-T, assessing 490 individuals, revealed an ICC of 0.966 (p < 0.001) for educated participants and 0.988 (p < 0.001) for uneducated participants, both indicating very high reliability.
The A-MMSE was evaluated with 782 patients and reported an ICC of 0.89 (p < 0.001), ensuring its reliability in a large and diverse sample. The H-MoCA, involving 30 subjects, showed an lCC of 0.87 (p < 0.001), which is considered ‘good’ according to COSMIN criteria.
The MoCA-S, which included 168 participants, had an lCC of 0.86. The T-MoCA, with 233 subjects, reported an ICC of 0.918 (p = 0.001), both suggesting strong reliability. The Arabic MoCA, assessed with 184 individuals, utilized a scoring system and showed results ranging from 0.9 to 2.5, affirming its reliability over time.
The HK-MoCA-A1, with 60 participants, demonstrated an excellent ICC of 0.99 (p < 0.001), rated ‘good’ by COSMIN standards. The subsequent version, HK-MoCA-A2, with the same number of participants, also reported a ‘good’ ICC of 0.82 (p < 0.001).
These assessments collectively confirm the robustness and reliability of the scales for assessing cognitive impairment. Most instruments exhibited high internal consistency and received positive COSMIN ratings, underscoring their suitability for repeated use in clinical and research settings.
Validity
Various cognitive assessment tools for MCI and AD were evaluated for their construct, concurrent, and convergent validity. The MMSE-2, involving 323 participants, demonstrated satisfactory construct validity with variances of 0.522 and 0.453 in three-factor and two-factor analyses, respectively. These results, set against measures of cognitive function, indicate satisfactory construct validity. The T-CMMSE, assessed among 65 individuals, showed an impressive Pearson's correlation of 0.991 (p < 0.001) with the standard MMSE, suggesting excellent construct validity. Similarly, the rMMSE-T, administered to 490 individuals, exhibited excellent construct validity with receiver operating characteristic (ROC) curve areas of 0.953 for the educated group and 0.907 for the uneducated group. The A-MMSE was administered to 782 patients and showed a robust ROC curve area, indicative of strong construct validity.
Concurrent validity was examined using the SMMSE with 210 patients, demonstrating a Spearman's correlation coefficient of 0.820 (p < 0.001) against the MMSE. 27 It also showed correlations of −0.597 (p < 0.001) with the Global Deterioration Scale (GDS) and 0.453 (p < 0.001) with the Activities of Daily Living (ADL) scale, confirming its effectiveness in reflecting concurrent cognitive and functional statuses. HK-MoCA-A1 and HK-MoCA-A2, with 60 subjects each, yielded Pearson's correlations of 0.87 and 0.79 (p < 0.001) against the HK-MoCA-O, respectively, substantiating their concurrent validity. The MoCA, with 221 participants, showed a strong Spearman's correlation of 0.926 (p < 0.001) with the MoCA 7.2 Polish version, highlighting its concurrent validity. Moreover, the MoCA-S, involving 168 subjects, exhibited a Spearman's correlation of 0.830 with the MMSE, further supporting its concurrent validity.
Convergent validity was assessed with the Short Form MoCA Czech Version (S-MoCA-C2), involving 699 individuals, revealing a Pearson's correlation of 0.937 (p < 0.001) with the MoCA-C2, indicating high convergent validity.
Sensitivity and specificity
A comprehensive evaluative review of MCI assessment scales examined a range of instruments for their diagnostic sensitivity and specificity. The T-CMMSE with 233 patients showed a sensitivity and specificity for MCI of 100% and 96.7%, respectively, at the optimal cut-off score of 16 out of 26. The MMSE-2: Standard Version (MMSE-2SV), involving 323 individuals, demonstrated a sensitivity of 74% for MCI and 92% for AD, with specificity at 59% for MCI and 87% for AD, at a cut-off score of 26 out of 30.
The rMMSE-T, administered to 490 subjects, reported sensitivities of 90.9% for educated and 82.7% for uneducated individuals, and specificities of 97% and 92.3% for MCI, respectively, at the cut-offs of 22 and 19. The A-MMSE, with a large cohort of 782 patients, showed 80% sensitivity and 89.4% specificity for MCI at a cut-off of 23 out of 30. The MoCA-S, assessed among 168 participants, exhibited 80% sensitivity and 75% specificity for MCI at a cut-off score of 26 out of 30. The Arabic version of the MoCA, with 184 subjects, had a sensitivity of 92.3% and specificity of 85.7% for MCI at the cut-off of 26 out of 30.
The T-MoCA, involving 233 participants, presented an 88.4% sensitivity and 77.9% specificity for MCI at a cut-off of 24 out of 30. The Georgian MoCA, with 86 individuals, reported 100% sensitivity and 69% specificity for MCI at a cut-off of 22 out of 30.
Two separate studies evaluated the standard MoCA. The first, involving 221 patients, showed a sensitivity of 82.6% and specificity of 69.7% for MCI at a cut-off of 23 out of 30, while the second, with 360 participants, demonstrated 81% sensitivity and 77% specificity for MCI at a cut-off of 22 out of 30. For AD, the second study displayed remarkable sensitivity (88%) and specificity (98%) at a cut-off of 17 out of 30.
Additionally, the EIACE, assessed with 128 subjects, revealed a sensitivity of 92.1% and specificity of 96.2% for MCI at a cut-off of 86 out of 100. The Addenbrooke's Cognitive Examination-III (ACE-III), with a substantial sample of 2176 individuals, showed a sensitivity of 92% and specificity of 63% for MCI at a cut-off of 84 out of 100. The Japanese version of the Quick Mild Cognitive Impairment (Qmci-J), evaluated among 526 subjects, reported a sensitivity of 73% and specificity of 68% for MCI at a cut-off of 60 out of 100. 23
The COSMIN ratings varied across instruments, with several scales rated as ‘excellent’ or ‘good’, signifying robust methodological quality. These findings underscore the importance of selecting scales with proven sensitivity and specificity for both MCI and AD, ensuring precise and reliable cognitive impairment assessments in clinical practice.
Methodological evaluation of measurement properties
The COSMIN criteria were used to evaluate the methodological quality of cognitive assessment tools, revealing a spectrum of methodological robustness. The MMSE-2, T-CMMSE, and SMMSE displayed methodological shortcomings, receiving predominantly ‘poor’ ratings. In contrast, the A-MMSE demonstrated more favorable outcomes, with ratings ranging from ‘good’ to ‘fair.’ The MoCA-S, Georgian MoCA, HK-MoCA-A1 and A2 exhibited ‘good’ ratings across several measurement properties, indicating their sound methodological construct. The rMMSE-T and S-MoCA-C2 were distinguished by their ‘good’ methodological quality. Variability was observed in the H-MoCA, T-MoCA, and Arabic MoCA, which presented a dichotomy of ‘good’ and ‘poor’ ratings, suggesting the need for cautious application. The standard MoCA, through separate validations, consistently showed ‘good’ to ‘excellent’ ratings. Conversely, the EIACE, P-GPCOG, and Qmci-J exhibited a juxtaposition of ‘good’ ratings in some respects, yet ‘poor’ in others. The ACE in Spanish and ACE-III, while not uniformly robust, showed promise in certain domains with ‘good’ ratings, underscoring their selective utility. This comprehensive analysis underscores the imperative for judicious selection of cognitive assessment instruments, ensuring alignment with clinical and research imperatives for accurate cognitive evaluation.
Best evidence synthesis: Overall levels of evidence
The methodological caliber of cognitive assessment instruments, appraised via COSMIN standards, exhibits a spectrum of efficacy. The MMSE-2, T-CMMSE, A-MMSE, SMMSE, and MoCA-S are characterized by a range of methodological qualities, varying from poor to fair, indicating the need for cautious interpretation of their results. In contrast, the rMMSE-T, HK-MoCA-A1 and A2 are noted for their reliability, with consistently good ratings across multiple measurement properties, making them more suitable for repeated assessments.
The standard MoCA stands out with its ‘excellent’ validity ratings, underscoring its methodological integrity and suitability for accurate cognitive evaluations. Similarly, the Georgian MoCA is distinguished by its superior sensitivity and specificity, making it a valuable tool for identifying cognitive impairment in clinical settings.
However, the Arabic MoCA, EIACE, ACE in Spanish, ACE-III, Qmci-J, and P-GPCOG necessitate judicious use due to their varied methodological ratings, ranging from poor to good across different measurement properties. This variability highlights the importance of carefully considering the specific strengths and limitations of each tool before application.
The S-MoCA-C2's ‘excellent’ validity enhances its methodological profile, suggesting its potential for accurate cognitive assessments. In contrast, the H-MoCA and T-MoCA results remain indeterminate, with a mix of good and poor ratings, indicating the need for further validation studies to establish their methodological robustness.
This synthesis accentuates the importance of discerning the appropriate cognitive assessment tool, contingent upon the COSMIN ratings, to ensure precise evaluation of cognitive impairment. By carefully considering the methodological quality of each instrument, clinicians and researchers can select the most appropriate tool for their specific needs, optimizing the accuracy and reliability of cognitive assessments in diverse populations.
Discussion
Studies have revealed significant variations in the prevalence of MCI and its progression to AD. For instance, a study conducted on subjects with MCI revealed that 53% had prodromal AD according to International Working Group-1 criteria. The three-year progression rate to AD-type dementia in this group was 50%, compared to 21% for subjects without prodromal AD. 28 This information highlights the importance of accurate diagnosis and timely intervention. Additionally, the prevalence of MCI varies based on demographic and geographical factors. A study in elderly Chinese populations found the overall prevalence of MCI to be 20.8%, with a higher incidence in rural (23.4%) compared to urban areas (16.8%), 29 suggesting that factors such as lifestyle and access to healthcare could play a role in the incidence and identification of MCI. These findings highlight the need for cognitive assessment tools that are sensitive and adaptable to different populations and stages of cognitive decline, as well as the necessity for tools that can accurately differentiate between MCI and early stages of AD.
In the area of neurocognitive disorders, particularly MCI and AD, precise cognitive assessment is the cornerstone of diagnosis. The complex clinical presentation of MCI, which often overlaps with the spectrum of normal cognitive aging, necessitates tools that are both sensitive and specific. This section explores the pivotal role of standardized cognitive assessment instruments, such as the MMSE-2, T-CMMSE, and MoCA. These tools are examined for their psychometric robustness, including their sensitivity, specificity, and overall reliability. 30 The variation in methodological quality of these instruments, as evidenced by the COSMIN scoring system, underscores the imperativeness of selecting the most appropriate tool tailored to the clinical context. An in-depth discussion of these tools’ psychometric properties and their application in diagnosing MCI and AD not only illuminate the complexities inherent in such assessments but also address the need for continuous refinement of these diagnostic instruments. This analysis is crucial in underscoring the role of accurate cognitive assessment as a linchpin in the timely and accurate diagnosis of MCI and AD, ultimately paving the way for targeted therapeutic interventions.
In the complex arena of cognitive assessment for MCI and AD, the HK-MoCA-A1 and HK-MoCA-A2 have emerged as significant instruments. Exhibiting high internal consistency (Cronbach's alpha: HK-MoCA-A1 – 0.79, HK-MoCA-A2 – 0.75) alongside commendable test-retest reliability, these tools are validated as robust instruments for cognitive screening within the Hong Kong demographic. When compared to other prevalent instruments, the MMSE-2, despite its widespread application, presents limitations in its sensitivity, notably in the early detection of cognitive decline. However, its straightforward administration protocol makes it an optimal instrument for general cognitive screening across a spectrum of settings. In contrast, the T-CMMSE distinguishes itself with its superior reliability, especially in telephonic assessments, thus offering a pragmatic solution for patient populations that are remote or otherwise inaccessible. Furthermore, the MoCA is characterized by its enhanced sensitivity in identifying MCI, rendering it a preferred tool for early-stage diagnosis. Its various iterations, inclusive of the HK-MoCA-A1 and A2, are tailored to address diverse cultural and linguistic nuances, thereby broadening its international applicability. In considering the appropriateness of these tools for distinct demographic groups, the HK-MoCA-A1 and A2 are particularly apt for Cantonese-speaking cohorts, ensuring a culturally and linguistically congruent assessment. The MMSE-2, while less sensitive but user-friendly, is apt for initial screenings spanning a wide range of populations, from community settings to primary care environments. The telephonic adaptation of the T-CMMSE avails itself as a unique asset for populations encumbered by limited access to in-person healthcare services. In conclusion, the selection of a cognitive assessment instrument should be meticulously informed by the specificities of the patient demographic, including but not limited to linguistic, cultural, and healthcare access factors. The findings of this study advocate for a bespoke approach in instrument selection, aiming to optimize the efficacy and accuracy of cognitive assessments for MCI and AD. This revised section provides a more scientifically nuanced and polished overview of the various cognitive assessment tools, emphasizing their suitability for different patient groups and diagnostic contexts.
In the critical appraisal of cognitive assessment tools for MCI and AD, the COSMIN criteria serve as a pivotal framework for methodological evaluation. This framework stratifies the tools into four methodological echelons: poor, fair, good, and excellent, thereby offering a comprehensive perspective on their psychometric properties. For example, the MMSE-2, a widely employed instrument, manifests considerable methodological limitations, as evidenced by its predominant allocation in the ‘poor’ category across diverse measurement dimensions such as construct validity, reliability, internal consistency, and sensitivity and specificity. In contrast, the T-CMMSE garners ‘good’ to ‘excellent’ methodological accolades, particularly notable in the realms of reliability and construct validity, signifying its exemplary methodological integrity. Further, the HK-MoCA-A1 and A2 exhibit commendable methodological merit, predominantly achieving ‘good’ ratings in multiple measurement properties. Notably, the HK-MoCA-A1 demonstrates a remarkable ICC of 0.99 in test-retest reliability analyses. The standard MoCA, through its independent validations, consistently secures ‘good’ to ‘excellent’ methodological standings, affirming its robustness and reliability. Conversely, instruments such as the EIACE, ACE-III, and P-GPCOG showcase a dichotomy in their methodological ratings, oscillating between ‘good’ and ‘poor’. This dichotomous trend underlines the necessity for cautious application and interpretation in varied clinical and research contexts. Thus, the application of the COSMIN framework in this study underscores the critical need for discerning selection of cognitive assessment instruments. This study emphasizes the critical importance of methodological rigor in ensuring accurate cognitive evaluation, particularly in the context of MCI and AD. The evident variability in methodological quality, as demonstrated through the systematic analysis of various cognitive assessment tools, underscores the necessity for ongoing evaluation and refinement of these instruments. By continually assessing and improving the psychometric properties and methodological robustness of these tools, researchers and clinicians can enhance their applicability and effectiveness across a wide range of patient populations and clinical settings.
Furthermore, the evaluation of cognitive assessment tools for MCI and AD revealed a diverse range of methodological robustness across the assessed instruments. The MMSE-2 and SMMSE predominantly received ‘poor’ ratings, indicating significant methodological limitations. On the contrary, the T-CMMSE and the rMMSE-T demonstrated superior performance, with the T-CMMSE achieving an outstanding ICC of 0.99, indicative of excellent test-retest reliability, and the rMMSE-T revealing high reliability with ICCs of 0.966 and 0.988 for educated and uneducated participants respectively. In contrast, the Automated MMSE showed more moderate outcomes, with ratings ranging from ‘good’ to ‘fair,’ suggesting its relatively lesser methodological robustness compared to the T-CMMSE and rMMSE-T. The MoCA and its adaptations, such as the Georgian MoCA, HK-MoCA-A1 and A2, were distinguished by ‘good’ to ‘excellent’ ratings, reflecting their robust methodological constructs. The MoCA, in particular, was noted for its ‘excellent’ validity, highlighting its methodological integrity and appropriateness for cognitive evaluation. The Georgian MoCA was identified for its outstanding sensitivity and specificity, rendering it a preferred instrument for precise cognitive impairment assessment. However, tools including the Arabic MoCA, EIACE, ACE-III, Qmci-J, and P-GPCOG demonstrated mixed methodological ratings, necessitating careful consideration in their application. The S-MoCA-C2, with its ‘excellent’ validity, enhances its profile in methodological terms, while the results for the H-MoCA and T-MoCA remain inconclusive, suggesting the need for cautious use.
Based on these findings, the following recommendations are proposed:
Initial Screening: For initial cognitive screenings, the MMSE-2 is recommended due to its user-friendly administration, despite its lower sensitivity in detecting early-stage cognitive decline. Its straightforward protocol makes it an ideal choice for primary care settings and community-based assessments. Comprehensive Cognitive Evaluations: When a more detailed cognitive assessment is required, the MoCA and its variants, particularly the Georgian MoCA, are advised. These tools demonstrate superior methodological qualities, including heightened sensitivity and specificity, making them well-suited for in-depth evaluations of cognitive function. Culturally and Linguistically Diverse Populations: For patient populations with specific cultural and linguistic needs, such as Cantonese-speaking individuals, the HK-MoCA-A1 and A2 are recommended. These adaptations ensure that cognitive assessments are conducted in a manner that is compatible with the patient's background, enhancing the accuracy and relevance of the results. Remote or Underserved Populations: In cases where patients have limited access to in-person healthcare services, the T-CMMSE is recommended. This tool has demonstrated strong performance in telephonic assessments, making it an ideal choice for remote cognitive evaluations or for reaching underserved populations. Research Settings: For research applications, instruments that have received ‘good’ to ‘excellent’ COSMIN ratings are preferred. Tools such as the MoCA, Georgian MoCA, and S-MoCA-C2 have shown robust methodological quality, ensuring that study findings are reliable and valid. Researchers should prioritize the use of these instruments to maintain high standards of scientific rigor.
In conducting this systematic review, several methodological limitations need to be addressed, highlighting the importance of careful interpretation of the results. A significant constraint is the linguistic scope of the review, limited to literature in English and Spanish. This exclusion of studies in other languages may introduce selection bias, potentially omitting crucial research and affecting the breadth of the analysis. Additionally, the study employed a combination of strategic manual searches and electronic database queries. While this approach aimed to enhance the study's scope, it introduced subjective judgments during the initial selection and detailed examination of texts. Although a collaborative approach was used to reconcile scholarly disagreements, the risk of interpretive bias in selecting and analyzing studies persists. In instances of incomplete or combined data sets, direct contact was made with original authors to obtain specific data relevant to MCI or AD cohorts. While this proactive step was intended to improve data accuracy and completeness, it may be subject to response bias depending on the original authors’ willingness and ability to provide data.
The analytical framework of the study included both quantitative and qualitative synthesis of outcomes, applying quantitative synthesis in cases of clinical and methodological consistency and qualitative summaries in cases of notable heterogeneity. While this comprehensive approach facilitated a nuanced understanding of the measurement properties, it also introduced limitations in the uniform interpretation and integration of heterogeneous data sets, potentially impacting the overall methodological soundness of the conclusions drawn. In summary, this study provides valuable insights into the methodological quality of cognitive assessment tools for MCI and AD, but the outlined limitations necessitate cautious extrapolation of the results and underscore the need for further methodologically sound research in this area.
Additionally, none of the assessment instruments consistently excelled across all measurement properties, indicating variable quality. To recapitulate, it is crucial to emphasize the necessity for continued and methodologically robust research in the field of cognitive assessment tools for MCI and AD diagnosis. Our study highlights a spectrum of methodological qualities across various cognitive assessment instruments, ranging from moderate to excellent. This variability underscores the critical need for future research to focus on refining these tools to enhance their sensitivity, specificity, reliability, and applicability in diverse clinical and research settings. Potential research avenues should aim to address the limitations identified in this study, such as exploring cognitive assessment tools in languages beyond English and Spanish to incorporate a broader range of cultural and linguistic contexts. Additionally, further investigation is needed to understand the efficacy of these tools in different stages of cognitive impairment and across various demographic groups, including age, education level, and cultural backgrounds. There is also a pressing need for longitudinal studies to assess the long-term reliability and validity of these cognitive assessment tools in predicting the progression of MCI to AD. Such studies would provide invaluable insights into the predictive power of these tools, thereby enhancing their clinical utility. Furthermore, integrating technological advancements like digital assessments and machine learning could improve the accuracy and efficiency of cognitive evaluations. Developing sophisticated tools that integrate seamlessly into clinical practices to deliver precise diagnostics is a critical research direction. Ultimately, this review sets the stage for future efforts aimed at creating refined, reliable, and universally applicable cognitive assessment tools that facilitate the early and accurate diagnosis of MCI and AD, leading to better patient outcomes.
Conclusion
This study sheds light on the varied effectiveness of cognitive assessment tools for diagnosing MCI and AD, underscoring the critical need for selecting tools that align with specific diagnostic and monitoring requirements. We find that the MMSE-2, although widely used, shows moderate sensitivity, particularly in detecting early-stage cognitive impairments. In contrast, the culturally adaptive T-CMMSE proves more effective in linguistically and culturally diverse groups. The HK-MoCA-A1 and A2 are specifically effective for the Hong Kong population, highlighting the significance of cultural relevance. The MoCA stands out for its ability to detect early cognitive decline across various demographics, demonstrating its versatility.
However, the study is limited by its demographic scope and the range of tools assessed. Future research should aim for greater inclusivity and broader evaluation of tools to enhance the generalizability of the findings. Our results support a tailored approach to selecting cognitive assessment tools, tailored to the specific profiles and needs of individual patients, thus improving diagnostic accuracy and the effectiveness of treatments in managing MCI and AD. This research represents a significant advance in furthering the understanding of cognitive assessment in neurodegenerative disorders, guiding us towards improved patient care and outcomes in addressing these intricate conditions.
Footnotes
Author contributions
Xia Peng (Methodology; Writing – original draft); Chen Run Li (Investigation; Writing – original draft); Ting Liang (Methodology); Shifen Xu (Resources; Writing – review & editing); Yan Cao (Resources; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by Special plan for research on aging and maternal and child health of Shanghai Municipal Health Commission (2020YJZX0123), and Traditional Chinese Medicine Science and Technology Development Project of Shanghai Medical Innovation & Development Foundation (WL-YSBZ-2022003K).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data will be made available on request.