
Abstract
Background
Mild cognitive impairment can be considered as the preclinical stage of Alzheimer's disease. With the addition of COVID-19 disease to the cognitive decline that occurs with aging, it may cause dementia with severe cognitive losses such as Alzheimer's disease in some people. Physical activity and brain-occupying practices can significantly improve the risk factors for cognitive disorders and Alzheimer's disease.
Objective
The aim of study was to examine the effect of green walking and intelligence game on the cognitive skills of individuals aged 50–70 years with COVID-19.
Methods
The randomized controlled study was completed with 40 individuals, 20 in the experimental and 20 in the control group. Individuals in the experimental group green walking for 30 min three days a week for one month in two groups of 10 people, accompanied by the researcher. In addition, these individuals played intelligence games (brain games-memory thinking and brain exercise) via their smartphones for 15 min every day for a month.
Results
The cognitive skills and cognitive dimensions of “attention, concentration, memory, language and orientation” of the individuals in the experimental group were significantly increased compared to the control group individuals (p < 0.05).
Conclusions
It was found that green walk and intelligence game practice increased the cognitive skills of individuals aged 50–70 years who had outpatient COVID-19.
Introduction
In January 2020, the seventh human coronavirus, severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), was discovered in Wuhan, Hubei province, China and spread globally around the world. This virus has caused thousands of deaths caused by coronavirus disease (COVID-19). As a result, the World Health Organization (WHO) declared this disease a pandemic on 12 March 2020. 1
COVID-19 affects many organs and systems, including the respiratory system. One of the systems it damages is the central nervous system (CNS). SARS-CoV-2 enters the CNS by crossing the blood brain barrier of the olfactory nerve or the vascular endothelium. After the virus enters the central nervous system (CNS), it gradually spreads along neurotransmission or hematogenous pathways, leading to infiltration and proliferation within the CNS and causing systemic inflammation. In this situation, it causes cognitive decline, particularly in the areas of working memory, executive functions, and attention. 2
Cognitive skills are defined as general mental capacity, including problem-solving, planning, reasoning, abstract thinking, quick learning, and learning from experiences to grasp complex thoughts. Changes occur in neurotransmitter systems with age. These changes begin in the third decade of life and manifest as neuronal losses resulting in decreased cognitive performance. 3 Age-related changes in the structural and functional integrity of the prefrontal and basal ganglia structures have been reported to be associated with a range of cognitive deficits, such as decreased memory and reduced information processing speed due to inhibition. 4 Older adults are more vulnerable to persistent cognitive impairments due to their high prevalence of comorbidities, which increases their risk of contracting COVID-19 and developing complications. 5 According to Alonso-Lana and colleagues, a published retrospective study found that 24% of 50 COVID-19 patients admitted to the neurology unit experienced short-term memory loss, and more than one-third of patients exhibited inattention and disorientation upon discharge from the intensive care unit. 6 The cognitive outcomes of 1077 patients who agreed to a follow-up visit 2–7 months after hospital discharge due to COVID-19 were evaluated, and 92.8% of patients were found to have at least one persistent symptom. Among the top 10 most frequently reported symptoms were short-term memory loss and slowed thinking. Additionally, 17% of patients were reported to have cognitive impairment. 7
Green walking is one of the nature sports that involves physical activity and supports cognitive development. In healthy adults, regular physical exercise has been found to enhance memory and attention, prevent inhibition, and increase processing speed. It is recommended that healthy older adults engage in aerobic activity (such as brisk walking) for 20–30 min, 3–5 days per week. 8 Walking improves cognitive decline both in healthy aging and in pathological conditions associated with aging. 9
Intelligence games are recognized as brain-training and brain-enhancing games as they are one of the factors that support cognitive development. By exercising the brain (brain gymnastics), they make the brain work harder. It is stated that brain training games have the effect of improving cognitive functions or preventing regression. 10 Many intervention studies of brain training games have reported improved performance on cognitive tasks such as speed and accuracy, visual-motor coordination, attention, memory, working memory and global cognitive function.11,12 Studies conducted with healthy adults and the older person show that cognitive training programs are effective on memory, general cognition, and executive functions.13,14
Older adults are more susceptible to COVID-19 infection and experience more severe symptoms of the disease than other members of the community. To mitigate the negative cognitive impacts of COVID-19, memory exercises 15 and aerobic exercises have been recommended for older adults to maintain and enhance cognitive functions. 16 Nurses need to monitor physical exercise and cognitive training practices for older adults to find new approaches and interventions to improve cognitive functions negatively affected by COVID-19. Consequently, this study aims to examine the impact of green walking and intelligence games on the cognitive skills of individuals aged 50–70 who have had COVID-19.
Methods and materials
Place and time of the research
The data of the study were collected from the electronic records of Tercan State Hospital between January-May 2022.
Ethical and legal aspects of the research
Institutional authorization dated 24/06/2021 and numbered E-15872173-771 was obtained from Erzincan Provincial Health Directorate for Tercan State Hospital and ethics committee approval dated 21/10/2021 and numbered 24237859-780 was obtained from Karadeniz Technical University Faculty of Medicine Clinical Research Ethics Committee. Individuals were included in the study after giving written and verbal consent to the Minimum Informed Consent Form. Permission to use the scale was obtained from Prof. Dr Banu Tavat, who conducted the validity and reliability study of the Montreal Cognitive Assessment Scale.
Population and sample of the study
The study population of the study consisted of patients diagnosed with laboratory-confirmed COVID-19 by polymerase chain reaction (PCR) at Tercan State Hospital.Power analysis was used to determine the sample of the study. The sample size was calculated using the G*Power program with the error amount α = 0.05 and the power of test as 0.80 (80%) and the effect size as 1.08, taking an intelligence game study as a reference due to the lack of previous studies on the subject. 17 As a result of the statistical analysis, it was found that a total of 30 individuals, 15 in the experimental group (green walking and intelligence group) and 15 in the control group, should be included in the study. 18 Considering that if the sample size increases, the standard error will decrease and the study power will increase, each group was increased by 34% (five people) and a total of 40 individuals, 20 individuals for each group, were included in the study.
The “block randomization” method was used to randomize individuals. In this method, the number of groups and their probabilities must be equal in each block. When there are two groups (A and B), the size of the blocks should be two, four, six, eight; when there are three groups (A, B and C), three, six, nine, twelve should be preferred. In our study, octoblocking was preferred due to the fact that there were two groups, the number of subjects in the block between six and 12 was considered ideal, and it was divisible by the number of samples. In determining the experimental and control groups, the coin toss method was used to determine the experimental group A and the control group B. Since there would be four A and four B in each block in octuple blocking, the number of all possible blocks was calculated to be 70 blocks as a result of the combination C (8,4). Since it would be sufficient to randomly select five blocks for 40 people, five numbers between 1 and 70 were generated using the Excel program and the numbers 12, 37, 25, 46, and 7 were obtained. Individuals were randomized according to the ABAABABABB, ABBBAABA, BBAABABAAB, BABABABABA, and ABABBBAA blocks corresponding to these numbers. The first eight individuals included in the study were randomized according to the distribution in block 12, and the next eight individuals were randomized according to block 37. The randomization of the entire sample was completed in this way, ensuring an equal and homogeneous distribution. The CONSORT flow diagram of the study is given in Figure 1.
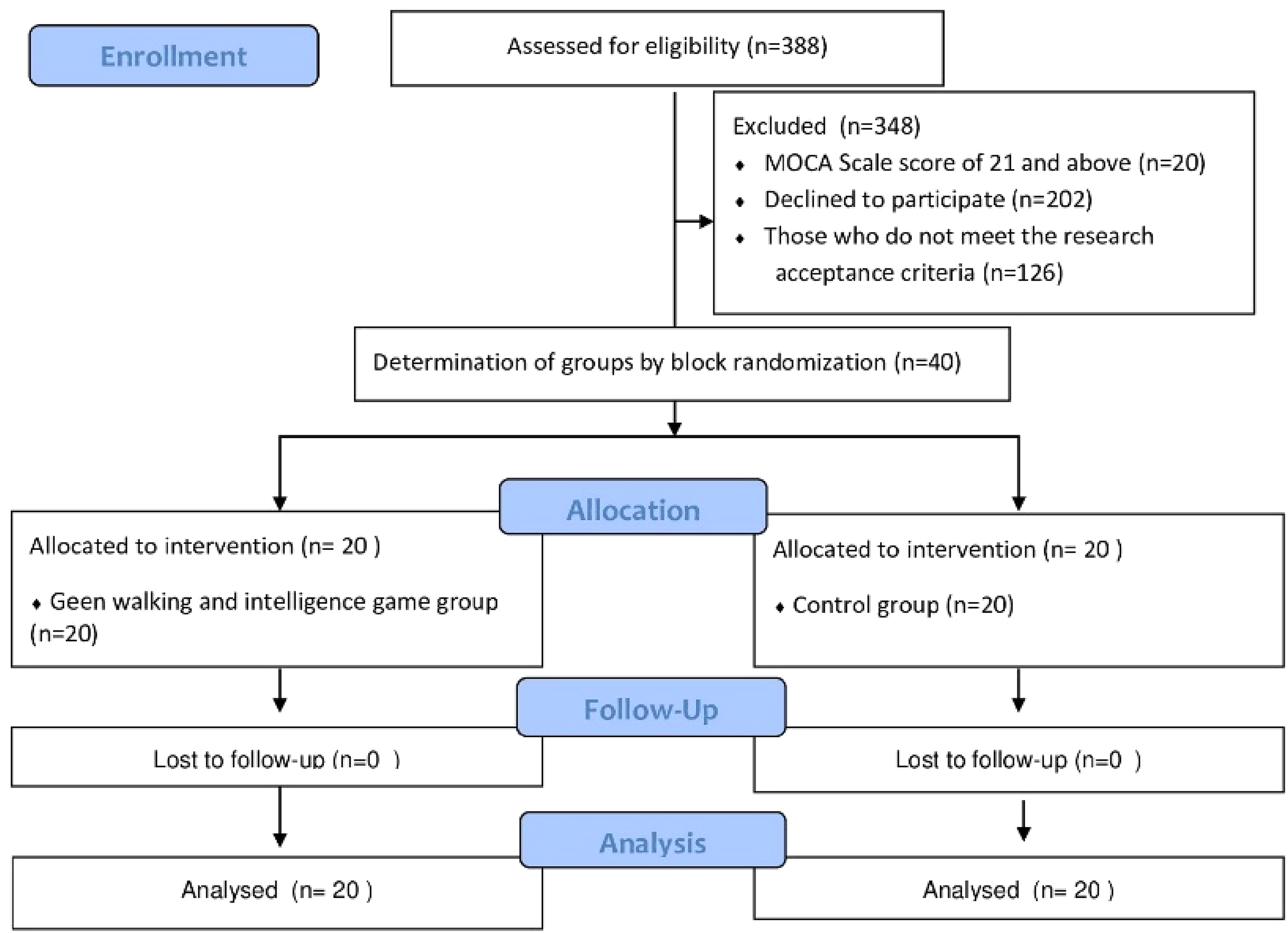
CONSORT flow diagram of research.
Criteria for research acceptance
Having electronic records and contact (address, telephone) information of individuals diagnosed with COVID-19 at Tercan Hospital and whose COVID-19 test became negative within one year by being placed in home quarantine with outpatient treatment, 19 being at least primary school graduate, residing in Tercan. Individuals were between the ages of 50–70, scoring 20 and below on the Montreal Cognitive Assessment Scale, 20 being able to perform self-care activities independently, 21 having a good general condition, having a smartphone or having a smartphone in the household, having a physician's approval stating that there is no harm in green walking for 30 min three days a week for one month for the individuals in the experimental group, and agreeing to participate in the study.
Criteria for research not acceptance
Positive COVID-19 (PCR) test result, visual and hearing impairment, balance problems, using a cane or walker, being bedridden or wheelchair dependent, being diagnosed with Parkinson's disease, dementia, Alzheimer's disease, cancer, having a history of central nervous system disease that may cause cognitive dysfunction, being on antipsychotics, antidepressants, mood stabilizers, antiepileptics, benzodiazepines and medications that may interfere with evaluation having undergone any surgery that prevents walking, having a condition that prevents walking. 22
Criteria for exclusion
Hospitalization for any reason, change of residence, emigration, death, infection requiring isolation, deterioration of general condition, inclusion in another aerobic exercise program, unwillingness to continue the study.
Data collection tools
Data were collected with the Individual Information Form, Montreal Cognitive Assessment (MoCA) Scale, Montreal Cognitive Assessment Application Instruction, and Experimental Group Follow-up Form. As intervention, Green Walking Information Brochure, Intelligence Game Information Brochure, Green Walking, Intelligence Game application, Telephone Interviews, and Home Visits were applied.
Individual information form
This form was developed by the researcher by reviewing the literature. 23 The form consisted of two parts. The first part included seven questions to determine the identifying information of the individuals (age, gender, marital status, job, education level, income perception level, and cohabitants); the second part included a total of 11 questions, including four questions to determine COVID-19 characteristics (presence of chronic disease, presence of COVID-19 symptoms, COVID-19 symptoms and COVID-19 treatment status).
Montreal cognitive assessment scale
The scale was developed in 2005 by Nasreddine and colleagues to differentiate between normal individuals and those with mild cognitive problems. 24 It is particularly effective for use in the early stages of cognitive issues. The adaptation and predictive validity studies of the scale for Turkish culture were conducted by Selekler and colleagues (2010), and its usability in clinical practice was found to be appropriate. 20 The scale assesses different cognitive dimensions, including attention and concentration, executive and abstract functions, memory, language, visuo constructional skills, and orientation. The scale scores range from a minimum of ‘0 points’ to a maximum of ‘30 points.’ While a threshold value of 21 points is considered, a score of 20 or below indicates cognitive dysfunction. The Cronbach's alpha value of the scale was found to be 0.851, and for this study, the Cronbach's alpha value was 0.703.
Montreal cognitive assessment practice guidelines
This instruction provides information to the researcher about how to administer and score the MoCA scale. The scale includes the scoring of 11 questions in total, including visual construction skills (cube), tracking, visual construction skills (clock), memory, naming, attention, verbal fluency, sentence repetition, delayed recall, abstract thinking and orientation. 25
Green walking
The American Geriatrics Society recommends that healthy older person/adults engage in aerobic activity, including brisk walking for 20–30 min, 3–5 days a week. 8
Green walking information brochure
The green walking information brochure was created by the researcher by reviewing the relevant literature.26,27 The brochure included written and visual information that individuals should pay attention to while green walking.
Intelligence game (brain games-memory thinking and brain exercise)
Intelligence Game is a brain training app available for download on IOS and Google play. Easy to access and use, this game can be played offline and is in Turkish. Developed by Content Arcade Games, 28 this game is organized under seven main game categories and 27 sub-topics: “bender, focus, think fast, retention, brain IQ, logic and reflex”.
With reference to the literature where similar games were played, it was observed that games were played every day for a month with a total playing time of 15 min and three games were selected from among the games.29,30 Therefore, the following three games were selected as the games to be played in our study.
Sort disk towers game in the bender category
There are three hard disks and five rings, pink, blue, green, yellow and orange. In the game, which progresses in levels starting from 1, an example of which color rings will be placed on which disks is given at the top of the screen. The player is asked to create the same shape to complete the level. The level is completed by placing the rings from the disks with upward and diagonal hand moves (Figure 2). 28
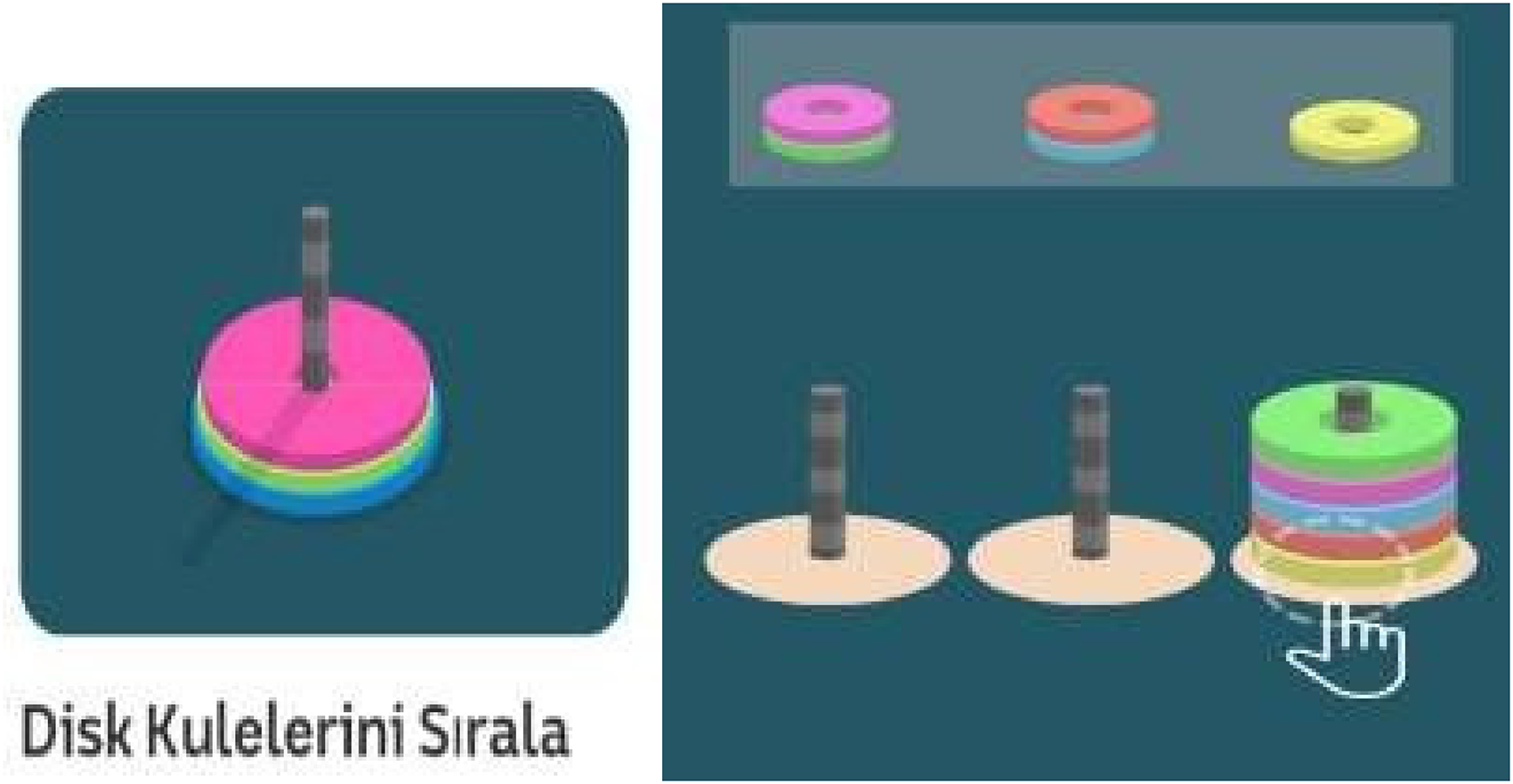
Sort disk towers game. 31
Quick thinking game from the reflexes category
In this game, there are 4 × 4 white circles. During the game, pink circles with a white center and pink edges appear inside the white circles in a mixed manner. The pink ring appears in another white circle in a mixed manner. The player is asked to touch whichever pink circle the ring appears on. Points are awarded for each correctly touched circle (Figure 3). 28
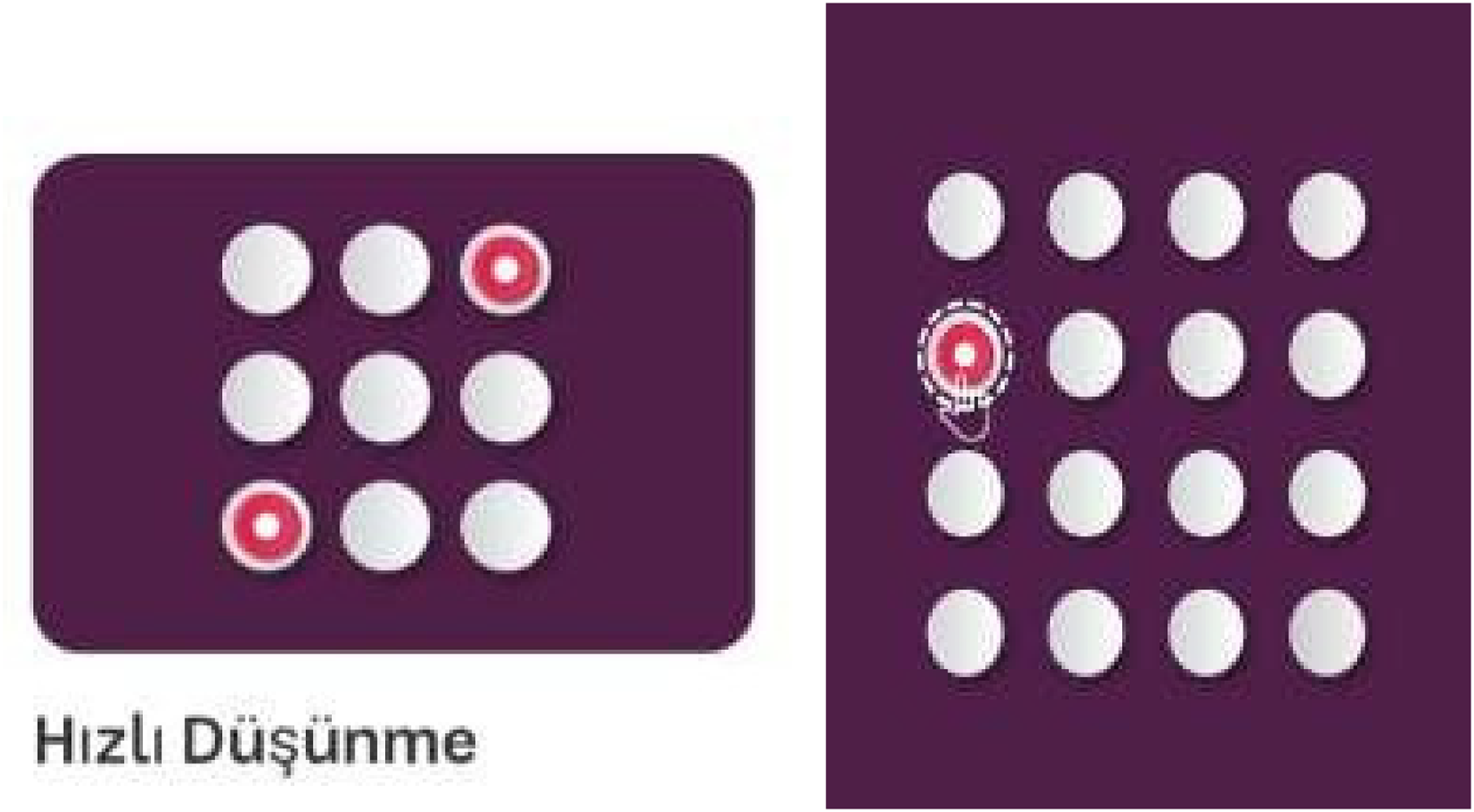
Quick thinking game. 31
Feed the fish game from focus category
At the bottom of the screen, orange bait is formed and this bait must reach the fish swimming in the water. The level is completed by scoring points when the moving fish are touched directly above them. Since the fish is swimming, if the place where the player touches the fish is not exactly in line with the fish, feeding with the bait is not successful. 28
Intelligence game information brochure
This brochure was created by the researcher.29,30 The brochure included information on “the name and language of the game, which age group it is suitable for, how to install the game on the phone, how to play the game, which games to choose, how long and how many days, hours and how to play the games”.
Experimental group follow-up form
This form was developed by the researcher. In the form, each individual in the experimental group was monitored in terms of green walking and playing intelligence games.
Data collection method
Experimental group
First, the researcher reached the individuals by phone. The first interview was conducted with a home visit. Individuals were administered the Individual Information Form and the MoCA scale as a pre-test by the researcher using the face-to-face interview method according to the MoCA Application Instruction. Then, this group of individuals was informed about green walking and given the Green Walking Information Brochure. Then, intelligence games application was downloaded to the smartphones of the individuals/family members by the researcher. The individuals played the first intelligence games game in the presence of the researcher. The individuals in the experimental group green walking for 30 min three days a week for a month with the researcher. In addition, these individuals played intelligence games game every day for a month. The individuals’ green walking and intelligence game practices were monitored by the researcher through telephone interviews using the Experimental Group Follow-up Form. As a result, each individual in this group green walking a total of 12 times and played 30 intelligence games during the study. Then, the MoCA scale was administered to these individuals as a post- test using the face-to-face interview method during the second home visit according to the MoCA Application Instruction.
Control group
First, the researcher reached these individuals by telephone. The first interview was conducted with the researcher's first home visit. The researcher administered the Individual Information Form and the MoCA scale as a pre-test to the individuals by using the face-to-face interview method according to the MoCA Application Instruction. No intervention was made to the individuals in this group. One month later, the MoCA scale was administered to these individuals as a post-test using the face-to-face interview method during the second home visit.
Green walking
For the green walking, the area located in the center of Tercan, easy to access, with a stream passing by and trees around it was determined as the walking path and the walking path was 2.5 km long in total. For individuals who had COVID-19, a green walking trail with a low degree of difficulty without slopes was selected. 31 Upon the requests of the individuals, the green walking group of 20 individuals was divided into two groups of 10 individuals each. The individuals in the first group of 10 green walking with the researcher on Mondays, Wednesdays, and Fridays; the individuals in the second group of 10 green walking for 30 min on Tuesdays, Thursdays, and Saturdays between 14:00–14:30, the time interval of their choice, for one month (April-May). The 30-min green walking was recorded in the Experimental Group Follow-up Form.
Intelligence game (brain games-memory thinking and brain exercise)
The Intelligence Game (Brain Games-Memory Thinking and Brain Exercise) application was downloaded and installed on the smart phones of the individuals in the Experimental group or their relatives (spouse, child, relative living with them) by the researcher by providing internet connection. The researcher provided information on how to play the intelligence game by using the Intelligence Game Information Brochure and this brochure was given to the individuals. They played the games in the morning in the time period 2 h after breakfast 32 for 30 days and 15 min, once a day, simultaneously with green walking for a month.
Implementation of the experimental group follow-up form
The green walking status of the individuals in the experimental group was recorded 12 times, three times a week, on the Experimental Group Follow-up Form by the researcher on the day of the green walking. In addition, the intelligence playing status of this group of individuals was recorded by the researcher in the Experimental Group Follow-up Form by making 30 phone calls, one phone call per day for each individual for one month.
Evaluation of data
The data obtained from the study were analyzed with the licensed SPSS 22.0 (IBM SPSS Statistics 22 software) package program. The conformity of the data to normal distribution was examined by Shapiro Wilk test. When parametric test assumptions were met, Independent Sample t test was used for intergroup analysis and Paired Sample t test was used for intragroup analysis. The eta square (η2) was used to evaluate the magnitude of the difference between the groups.
Results
No significant difference was found between the experimental and control groups in terms of age, gender, marital status, job, education level, income perception level and people living (p > 0.05) (Table 1).
Descriptive information of individuals (n = 40).
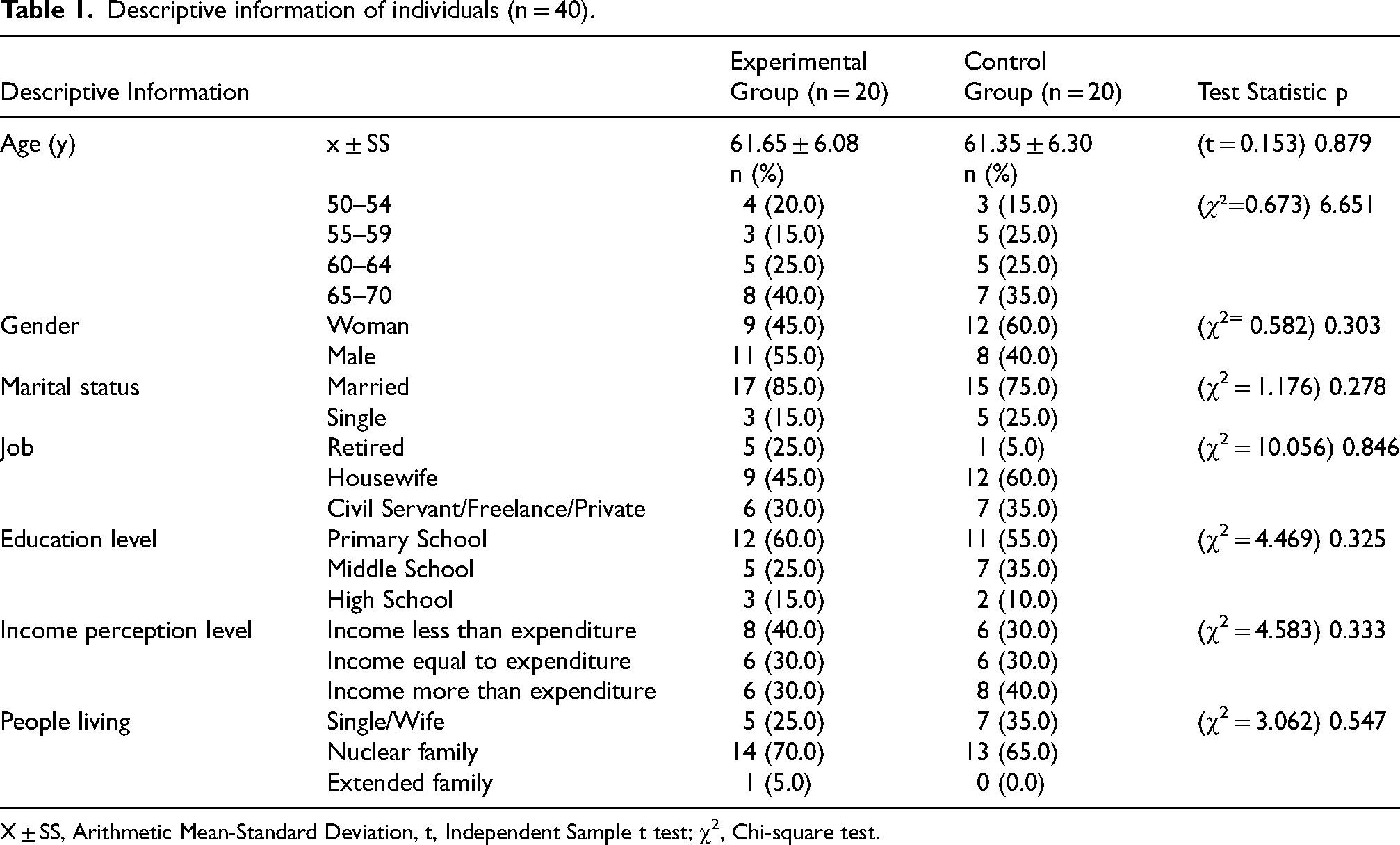
X ± SS, Arithmetic Mean-Standard Deviation, t, Independent Sample t test; χ2, Chi-square test.
Table 2 shows the characteristics of COVID-19. While there were no significant differences between the groups with regarding to the presence of chronic diseases, the presence of COVID-19 symptoms, back pain, fever, loss of smell/taste, cough, weakness, chills, headache, nasal congestion, nausea, vomiting symptoms and receipt of COVID-19 treatment (p > 0. 05), whereas significant differences were found for symptoms of chills (χ2 = 4.000; 0.046), shortness of breath (χ2 = 5.630; p = 0.018) and runny nose (χ2 = 20.000; p = 0.000) (Table 2).
Individual characteristics related to COVID-19 (n = 40).
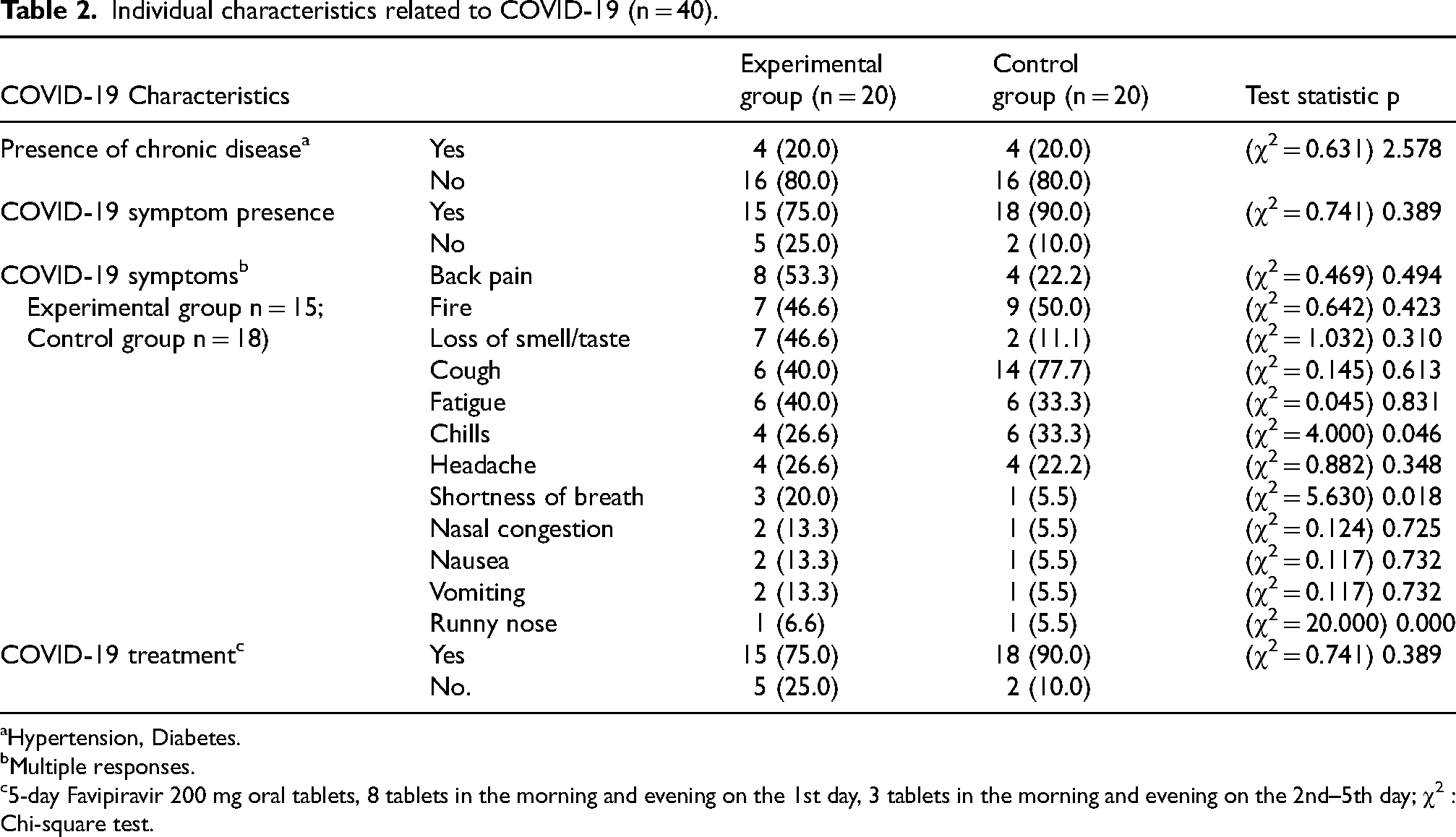
Hypertension, Diabetes.
Multiple responses.
5-day Favipiravir 200 mg oral tablets, 8 tablets in the morning and evening on the 1st day, 3 tablets in the morning and evening on the 2nd–5th day; χ2 : Chi-square test.
While there was no significant difference between the two groups in terms of mean MoCA scores in the pre-test (p > 0.05); in the post-test, it was determined that the experimental group had significantly higher mean scores than the control group (t = 7.016; p = 0.000). In intragroup examinations, while there was a statistically significant increase in the mean MoCA scores of the individuals in the experimental group (t = −12.076; p = 0.000); no significant difference was found in the mean MoCA scores of the individuals in the control group (p > 0.05). When the effect size eta-square calculation was examined, it was determined that the numerical value was 0.695 and that the green walking and intelligence game application had a great effect on the increase in the mean MoCA score (Table 3).
Comparison of pretest-posttest Montreal cognitive assessment scale mean scores.
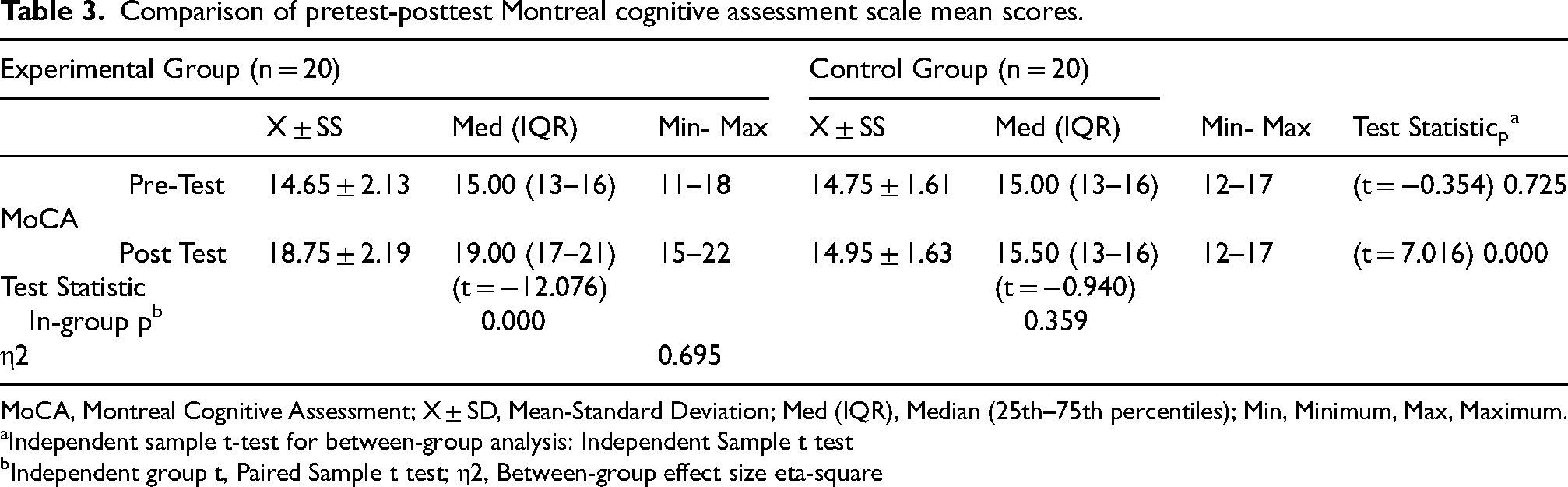
MoCA, Montreal Cognitive Assessment; X ± SD, Mean-Standard Deviation; Med (IQR), Median (25th–75th percentiles); Min, Minimum, Max, Maximum.
Independent sample t-test for between-group analysis: Independent Sample t test
Independent group t, Paired Sample t test; η2, Between-group effect size eta-square
Table 3 shows the pretest and posttest MoCA scale cognitive dimensions mean scores of the experimental and control group individuals. While no statistically significant difference was found between the two groups in terms of “attention concentration” mean scores in the pretest (p > 0.05), it was found in the posttest (t = 2.131; p = 0.040). In intragroup examinations, a significant increase was found in the mean scores of the individuals in the experimental group (t = - 2.651; p = 0.016), but not in the control group (p > 0.05). In terms of “executive and abstract functions” mean scores no statistically significant difference was found between the two groups in the pretest and posttest (p > 0.05). In intragroup examinations, a significant increase was found in the mean scores of the individuals in the experimental and control groups (t = −3.684; p = 0.002), but not in the control group (p > 0.05).
While no statistically significant difference was found between the two groups in terms of “Memory” mean scores in the pretest (p > 0.05), it was found in the posttest (t = 2.230; p = 0.032). In intragroup examinations, a significant increase was found in the experimental group (t = −4.682; p = 0.000), but not in the control group (p > 0.05).
While there was no statistically significant difference between the two groups in terms of “language” mean scores in the pretest (p > 0.05), a significant difference was found in the posttest (t = 7.151; p = 0.000). In intragroup examinations, a significant increase was found in the experimental group (t = −3.327; p = 0.004), but not in the control group (p > 0.05).
There was no statistically significant difference between the two groups in terms of pre- test and post-test “visual structuring” mean scores (p > 0.05). In intragroup examinations, a significant increase was found in the mean scores of the individuals in the experimental group (t = −5.940; p = 0.000), but not in the individuals in the control group (p > 0.05).
While there was no statistically significant difference between the two groups in terms of pretest “orientation” mean scores (p > 0.05), a significant difference was found in the posttest (t = 4.329; p = 0.000). In intragroup examinations, a significant increase was found in the experimental group (t = −4.660; p = 0.000), but not in the control group (p > 0.05). The Eta-square numerical value of the “attention concentration” (η2 = 0.111), “executive and abstract functions” (η2 = 0.068), “memory” (η2 = 0.116), and “visual structuring” (η2 = 0.078), and it was determined that the effect of green walking and intelligence games application on the increase in the mean score of MoCA cognitive dimension was moderate. It was determined that the eta-square numerical value of “language” (η2 = 0.662) and “orientation” (η2 = 0.359), the effect value was large and the effect of the green walking and intelligence games application on the increase in the mean score of the MoCA cognitive dimension was large (Table 4).
Comparison of pretest-posttest Montreal cognitive assessment scale cognitive dimensions mean scores (n = 40).
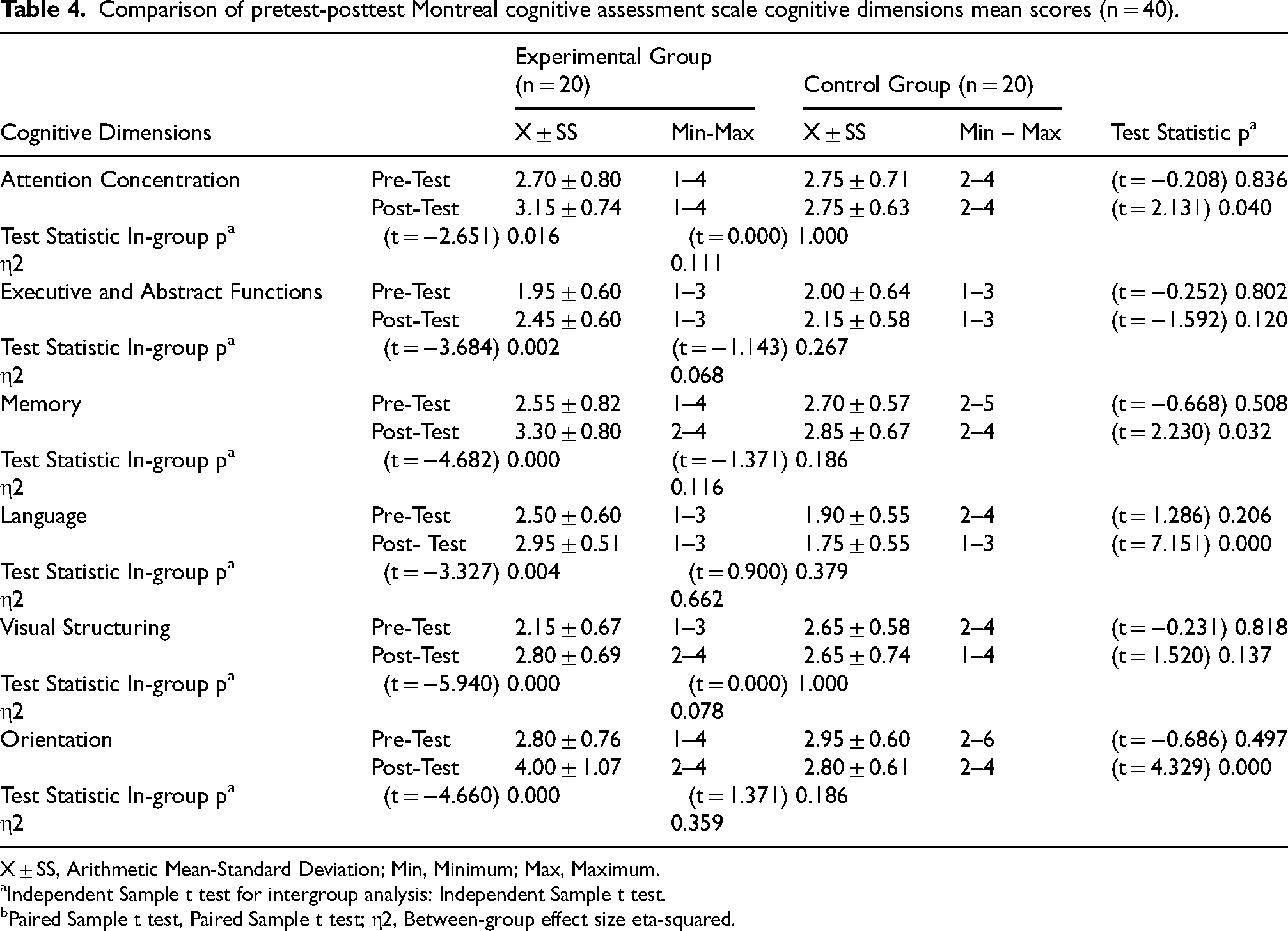
X ± SS, Arithmetic Mean-Standard Deviation; Min, Minimum; Max, Maximum.
Independent Sample t test for intergroup analysis: Independent Sample t test.
Paired Sample t test, Paired Sample t test; η2, Between-group effect size eta-squared.
Discussion
In our study, green walking and intelligence games had an increasing effect on the cognitive skills of individuals aged 50–70 years who had outpatient COVID-19. In the COVID-19 pandemic, memory exercises 15 and aerobic exercises have been recommended for older adults with mild cognitive impairment to maintain and improve cognitive functions. 16 In many studies, it has been found that the combined use of physical exercise and cognitive training practices improves general cognitive functions33,34 in older adults in parallel with our study results. It has been reported that cognitive involvement is caused by neuronal loss and regional atrophy in the gray area of the temporal and frontal cortex and functional brain imaging studies indicate that walking has a positive effect on the prefrontal cortex and increases cognitive functions by inducing cellular and molecular processes that increase learning, memory, and brain plasticity. 35 Intelligence games, on the other hand, lead to activation in the prefrontal lobe, thus improving cognitive abilities by gaining the ability to think and problem-solve in the face of difficulty with the novelty of playing more than one game. 36
Attention and concentration is cognitive skill that requires focusing mental processes such as comprehension and perception only on the needed stimuli to the exclusion of other stimuli and focusing on the subject for a certain period of time, and it decreases after the age of 50. 21 Shenjie et al. stated that intelligence games improve the ability to sustain attention for a longer period of time. 37 In this direction, the reason for the increase in the cognitive dimension of attention concentration in our study was thought to be that the individuals in the experimental group focused their attention on the game they played without being affected by internal and external stimuli in the games they played within the scope of intelligence games, and that they focused on nature by excluding other stimuli around them with green walking.
Executive and abstract functions include time management, prioritization, understanding complex and abstract functions, using new strategies, and abstraction skills by associating relationships between concepts beyond the known. 38 COVID-19 infection has the effect of decreasing executive and abstract functions. 39 However, intelligence games are reported to contribute positively to the improvement of executive functions as they require planning the next step of the game, observing clues to reach the goal and developing strategies simultaneously. 40 In our study, the game “sort disc towers” played by individuals within the scope of intelligence games requires planning the next moves while sorting colored discs, choosing among different alternatives and thinking about the unknown in order to reach a logical conclusion. At the same time, green walking involves planning and deciding on the steps of each stage from the beginning to the end of the walking. In this context, it was thought that the implementation of green walking and intelligence games increased the cognitive skills of “executive and abstract functions” of individuals.
Shrinkage of white and gray matter in the brain, changes in the lateral prefrontal cortex, hippocampus, cerebellum and caudate nucleus, and decreased cholinergic and dopaminergic activity negatively affect attention and memory processes. 41 In this context, COVID-19 infection negatively affects the memory functions of patients. However, memory is an important cognitive domain that is affected in the early stages of mild cognitive impairment. 42 In our study, green walking and intelligence games increased the cognitive skills of memory in individuals aged 50–70 years with outpatient COVID-19.
With aging, skills such as speaking, verbal expression, producing meaningful words and/or sentences are preserved, but language skills such as finding category-appropriate words (verbal fluency), word finding and/or naming deteriorate. 43 DeDe et al. (2004) state that being in nature contributes to the reduction of physical and mental stress and therefore helps to improve language skills by increasing attention and learning. 44 Within the scope of this information, in our study, it was thought that green walking and intelligence game practice had positive effects on increasing the language cognitive dimension of individuals with COVID- 19.
Compared to exposure to urban landscapes, exposure to nature landscapes has a positive effect on visual structuring. 38 Visual configuration is the ability to form visual images, to organize two- and three-dimensional object parts effectively in the mind, to mentally manipulate, rotate, flip or invert the stimulus. As a result of the MoCA scale applied by Dressing et al. in patients to determine the cognitive profiles of outpatients with long-term neurocognitive symptoms after COVID-19, they found a deficiency in the visual configuration of only one patient. 45 It was thought that the increase in the “visual structuring” cognitive dimension of the experimental group within the group was due to the ability to use their mental organization skills effectively in the games played within the scope of the intelligence game and the visual information encountered during the nature walk was transferred to the mind and retained.
Orientation, which is related to direction determination and the maintenance of a sense of direction, regulates the spatial relations of the individual with the environment. 46 Grub et al. (2008) reported an increase in orientations including environmental signs, route information, place and time orientation and awareness of geographical orientation with regular walks. 47 It is thought that a sense of direction, concept of place and spatial awareness are formed with green walking. Therefore, in our study, green walking was thought to increase the orientation cognitive dimension of individuals who survived COVID-19 outpatient. In addition, it was interpreted that the intelligence game application increased the design and shaping skills of the environment in the orientation cognitive dimension.
Conclusion
As a result, it was determined that green walking and intelligence game application increased the cognitive skills of individuals between the ages of 50 and 70 who had outpatient COVID-19. In conclusion, it was found that nature walks and brain teasers increased the cognitive skills of individuals aged 50–70 years who received outpatient COVID-19 treatment. When diseases caused by cognitive losses are added to the aging process, the cognitive decline that occurs in this process accelerates even more. Nature walks and brain teasers are recommended both to reduce this decline and to adopt a healthy lifestyle. It is also recommended to be included as a new approach and intervention in nursing practices.
Limitations of the study
The limitation of the study is that the research was conducted only with individuals living in Tercan District and Tercan State Hospital. In addition, the use of the MoCA scale both in the acceptance criteria of the study and in the evaluation of individuals’ cognitive skills constitutes another limitation.
Footnotes
Acknowledgments
The authors would like to thank all participants to our research. This work is the doctoral thesis of the corresponding author and thesis advisor.
Author contributions
Zahide Akeren (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Resources; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing); Sevilay Hintistan (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Resources; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing)
Data availability
The data is provided if the author requests it from the author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.