
Abstract
Cerebrovascular accidents (CVA) remain one of the major causes of disabilities and mortality worldwide. In the young, carotid artery dissection (CAD) accounts for close to one-quarter of ischaemic strokes, occurring either spontaneously or due to a traumatic mechanism such as strangulation. We hereby, report a case of a young adult with large-vessel occlusion due to post-strangulation internal CAD. This case highlights the importance of raising awareness of the possibility of CAD in the presence of any focal neurologic deficit due to strangulation.
Introduction
A cerebrovascular accident (CVA) is defined as the abrupt onset of a neurologic deficit that is attributable to a focal vascular cause. 1 Approximately 1%–2% of all ischaemic strokes are caused by carotid artery dissection (CAD) in all ages but account for up to 25% of ischaemic strokes in young individuals. 2 The brain vasculature is mainly supplied by paired internal carotid and vertebral arteries with the extracranial segment of the former being more superficial and hence vulnerable to both penetrating and blunt traumatic injuries such as strangulation. The process of strangulation involves the use of an external gripping force on the neck, impeding oxygen and blood supply to the brain and resulting in an altered or total loss of consciousness.3, 4 This can range from the use of bare hands to ligature from a cord, usually in cases of violence. 3 The mechanism of death in cases of strangulation is multifactorial, depending on some factors such as the way the force is applied to the neck: the area, the force magnitude, the duration and the region where the force was applied. 3 There are several reports on the onset of neurologic features following strangulation, amongst which ischaemic stroke has been found in some post-mortem cases.5, 6 We report a case of acute ischaemic stroke as a result of carotid arterial dissection and aneurysm caused by attempted strangulation. To the best of our knowledge, this is the first case report of a stroke resulting from blunt trauma due to strangulation.
Case Presentation
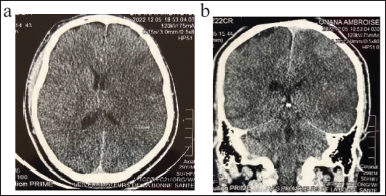
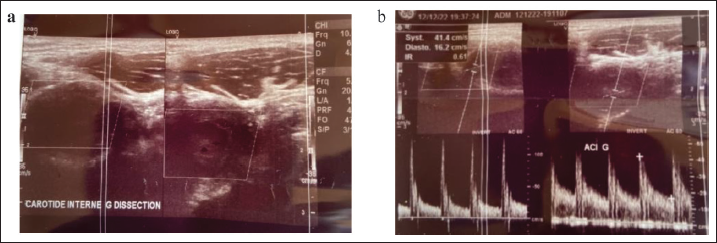
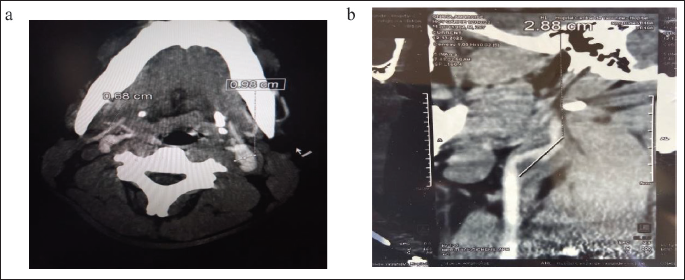
This is a case of a 26-year-old right-handed male with an unremarkable past history and no vascular risk factors, who was brought to the emergency room following a strangulation attempt during a fight. He presented with a sudden-onset right body weakness associated with an inability to speak. Upon admission about 24 hours later, his vital signs were as follows: blood pressure 116/78 mmHg, pulse at 76 bpm, respiratory rate at 18 cycles/minute and oxygen saturation at 98%. On neurologic examination, he was conscious with a Glasgow Coma Scale (GCS) at 15/15. He had a right upper-motor-neuron facial palsy, right-side upper-motor-neuron weakness with grade 0 muscle strength, right hypoesthesia, mixed aphasia, right homonymous lateral hemianopia and right visual and sensory hemineglect giving an estimated National Institute of Health Stroke Severity (NIHSS) score of 17/42. A non-enhanced brain computed tomography (CT) scan revealed a left complete (M1) middle cerebral artery infarct (Figure 1). A carotid Doppler of neck vessels revealed a reduced and almost-occluded proximal portion of the left internal carotid artery (ICA) with a bulge consistent with a resultant aneurysm (Figure 2). CT angiography of neck vessels confirmed a left ICA dissection with a heterogeneous hypodense blood clot and a resultant adjacent aneurysm measuring 28.8 mm by 9.8 mm (Figure 3). A 24-hour Holter-ECG recording showed a sinus regular rhythm with a heart rate of 73 bpm without any abnormalities. Transthoracic cardiac ultrasound presented no intracardiac clots, no valvular changes, no myocardial changes and no cardiac congenital abnormalities such as patent foramen ovale or atrial septal defect. A 24-hour ambulatory Blood Pressure Measurement (ABPM) revealed an average blood pressure of 114/72 mmHg. Other investigations such as complete blood count, serum electrolytes, kidney and liver function tests were within normal limits. Infectious assays such as HIV, Hepatitis B and C serology, TPHA/VDRL assays were all negative. Clotting profile and serum protein electrophoresis were normal. Advanced investigations in our patient were not done due to financial constraints.
Left Internal Carotid Artery Ischaemic Stroke (a) Axial View and (b) Coronal View.
Left Carotid Doppler Ultrasound Studies Revealing the Carotid Dissection an Intimal Free Flap (a) and Significantly Decreased Blood Flow (b).
CT Angiography of Neck Vessels Showing a Left Internal Carotid Dissection and Aneurysm With (a) Cross-sectional and (b) Longitudinal Measurements.
During his hospitalisation, he was placed on Rivaroxaban 15 mg bid. Neurorehabilitation with both the speech therapist and physiotherapist began during hospitalisation and the patient was closely followed up by a multidisciplinary team including neurologists, cardiologists and the neurorehabilitation team (physiotherapists, speech therapists, and neuropsychologists). He was discharged 10 days later after consulting the vascular surgeon where, the indication for vascular surgery was no longer possible.
The evolution two months later was characterised by an improvement of right hemiplegia to a hemiparesis of 3/5, mild improvement of right upper-motor-neuron facial palsy, right hypoesthesia, persistent global aphasia, giving an estimated NIHSS score at 10/42 with a modified Rankin scale (mRS) at 03/5 and a Barthel Index at 60%. At six months post-stroke, he could walk with grade 4—spastic hemiparesis, mild speech improvement and hypoesthesia giving an estimated NIHSS of 07, mRS of 03/5 and Barthel index at 70%.
Discussion
One of the major aetiologies of acute ischaemic stroke in young adults is carotid dissection. 7 Approximately 1%–2% of all ischaemic strokes are caused by CAD, accounting for close to one-quarter of ischaemic strokes in young individuals. 2 Carotid dissection could be spontaneous, or in some cases, occur after a cervical trauma such as strangulation. This case report portrays a large territory ischaemic stroke following a strangulation. In our case, strangulation occurred after a conflict between the victim and another individual leading to loss of consciousness. Studies report that brain injury may occur in survivors of manual strangulation in an acute or late onset. Among the potential aetiologies, cervical CAD with or without thrombosis is the most described mechanism.4, 8 Our patient presented with a dense focal neurologic deficit consistent with a large territory occlusion and an overall estimated NIHSS score of 17/42. Ischaemic stroke due to CAD is considered as a large-vessel occlusive stroke with moderate to severe neurologic deficits. 9 Given that the ICA accounts for approximately two-thirds of the brain’s blood supply, 7 prompt recognition and diagnosis could limit the potential case-fatality rate related to CAD. Thus, a high clinical suspicion should immediately prompt imaging of the neck blood vessels in order to improve outcome.
Neuroimaging is an indispensable investigation in the diagnosis of stroke. 8 Emergency brain computed tomography scan (CT scan) remains the initial and appropriate neuroimaging primordially for the exclusion of cerebral haemorrhage. Then the CT angiography for exploration for any occluded vessel. In our case study, an early non-enhanced brain scan revealed what seemed to be a left complete (M1) middle cerebral artery infarct. In the investigation for a potential thrombo-embolic aetiology, an emergency carotid Doppler of neck vessels revealed reduced and almost-occluded left ICA with a bulge consistent with a resultant aneurysm. CT angiography revealed a left internal (CAD) with a heterogeneous hypodense blood clot and a resultant adjacent aneurysm measuring 28.8 mm by 9.8 mm.
The management of cerebral infarct following internal CAD according to European Stroke Organisation (ESO) 2021 guidelines involves IV thrombolysis and endovascular thrombectomy be considered after ruling out standard contra-indications, checking for any patent circle of Willis and assessing the risk/benefit ratio based on the location of the dissection and bleeding risk. 10 Our case study presented at the emergency service, 24 hours after onset. Moreover, the neuroimaging done already revealed cerebral infarct ruling out the possibility of salvaging any brain tissue. In effect, a study by Mapoure et al. in Cameroon reported that the mean consultation time delay at the emergency after stroke onset was estimated at 47.36 ± 18.48 hours. 11 This could be as result of the low health-seeking attitudes of patients and caregivers with regards to stroke in our resource-limited setting. 12 Large territory ischaemic strokes are associated with debilitating neurologic deficits negatively creating an impact on the functional status of the victim. 13 In our case, he had a moderate/severe NIHSS of 17 accounting for the dense focal neurologic deficit. Studies have reported stroke with dense neurologic deficits to be associated with increased disability and mortality. After acute stroke management, our case still had a poor functional outcome with poor mRS and Barthel index rendering him almost dependent.
Conclusion
Although there are reports of spontaneous (non-trauma-related) stroke, this case report describes a post-strangulation carotid dissection with concurrent aneurysm, leading to compromised cerebral blood flow and hence stroke. This report highlights the need for a high index of suspicion of CAD following a sudden focal neurologic deficit in cases of blunt trauma to the neck, especially after attempted strangulation. This case report adds to the existing literature on nervous system injury due to strangulation.
Footnotes
Acknowledgement
We would like to thank the patient for granting us the permission to publish this case report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
NA.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
A signed informed consent was obtained from the participant prior to publication and every image published was provided after patient’s written permission. Patient details on each image was deleted for the purpose of confidentiality.