
Abstract
Background
Cardioembolic strokes are a common cause of mortality and morbidity because they are usually big and multiple. Despite extensive advances in the determination and management of modifiable risk factors of these strokes, a significant proportion are attributed to non-modifiable factors. We wanted to test the hypothesis that cardioembolic strokes and no other subtypes of ischemic stroke are associated with inclement weather in Kashmir Valley where winter seasons have harsh weather.
Results
A total of 540 ischemic stroke patients were included in the study of which cardioembolic strokes were most common. Cardioembolic strokes were more common in the winter season and associated with lower minimum and maximum temperatures.
Conclusion
Evaluation and management of cardioembolic strokes during winter months may demand more attention, particularly in elderly individuals and those with risk factors for atrial fibrillation.
Introduction
Stroke is the second leading cause of death and a major cause of disability worldwide. 1 Ischemic stroke makes up around 80% of the cases although this proportion is lower in developing Asian countries. Although there are many aetiologies for ischemic stroke such as large artery atherosclerosis (LAA), and small vessel disease, embolism from the heart remains a significant cause of ischemic stroke. 2 Cardiac embolism is significant because it is a preventable cause of cerebral ischemia and its incidence increases with age; thus, its prevalence will increase as communities age. The most important risk factor for cardio-embolism is atrial fibrillation which increases the risk of ischemic stroke by three- to five-fold. 3 Similarly, acute myocardial infarction particularly when associated with the formation of a left ventricular aneurysm is a source of embolism. Patent foramen ovale (PFO) is associated with paradoxical embolism, particularly in young people with embolic stroke of unknown source (ESUS). 4 Other risk factors for cardio-embolism include rheumatic heart disease, heart failure, infective endocarditis, left ventricular dysfunction, prosthetic valves, and so on. 5
Among many non-traditional risk factors, weather has recently been recognized as a risk factor for acute stroke. 6 Day-to-day as well as season-wise variations in weather and its variables may affect the stroke risk. Lower temperature has been found in many studies to increase the risk of stroke. 7 The valley of Kashmir, where this study was conducted, has a moderate climate with unpredictable weather conditions. The hottest month is July (mean minimum temperature 16°C and mean maximum temperature 32°C), and the coldest month is December and January (mean minimum temperature −15°C and mean maximum temperature 0°C) with moderate to heavy snowfall. 8 Over years of neurological practice, the authors observed that, in winter months, cardioembolic strokes particularly related to atrial fibrillation show an increased incidence and the infarcts are usually bigger with higher associated mortality. In this study, we tested the hypothesis that, as compared with other aetiologies of ischemic stroke, cardioembolic strokes are more common in winter.
Methods
All patients admitted to our department with a diagnosis of acute ischemic stroke over a period of 25 months (January 2020 to January 2022) were registered for the study and information required as per the proforma (attached as Supplementary file) was obtained. Patients were further classified into different subtypes as per TOAST (Trial of Org 10172 Acute Stroke Treatment) classification. 9
Weather Parameters
Indian Meteorological Department provided the data regarding various meteorological factors studied in this project.
10
The following meteorological factors obtained on the day of the stroke were studied:
Minimum temperature (°C) Maximum temperature (°C) Relative humidity (%) Wind speed (km/s) Atmospheric pressure (hPa)
Statistical Methods
Data were coded and recorded in the MS Excel spreadsheet program. Statistical analysis was done using SPSS v23 (IBM Corp.). Data were presented in a graphical manner wherever appropriate for data visualization using histograms/Box-and-Whisker plots/column charts for continuous data and bar charts/pie charts for categorical data. The independent ‘t-test’ was used to make group comparisons for continuously distributed data when comparing two groups. The Poisson regression model was used to identify potential independent meteorological variables associated with acute ischemic stroke occurrence. p-value < .05 was considered significant.
Results
A total of 540 patients of acute ischemic stroke patients were included in the study. Men comprised 60%, while women comprised 40% of the study group. The majority of the patients were from rural areas (75% rural vs. 25% urban). Notably, 77% had a history of hypertension, but only 46% of these were compliant with antihypertensive medications. A total of 6.7% of patients had a history of underlying atrial fibrillation of which 61% were on anticoagulation. Novel oral anticoagulants were used more often than vitamin K antagonists (NOACs 55% vs. VKAs 45%).
Cardioembolic strokes were the most common subtype of ischemic stroke followed by cryptogenic strokes (Figure 1).
Classification of Ischemic Strokes by TOAST Schema.
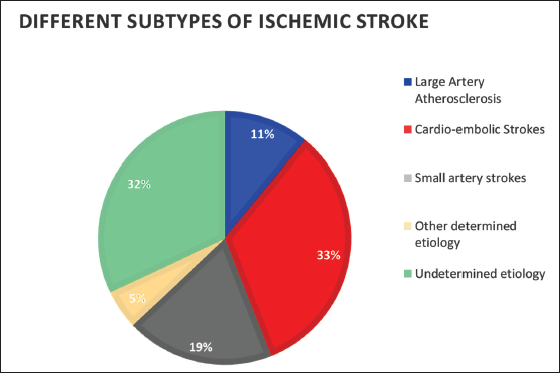
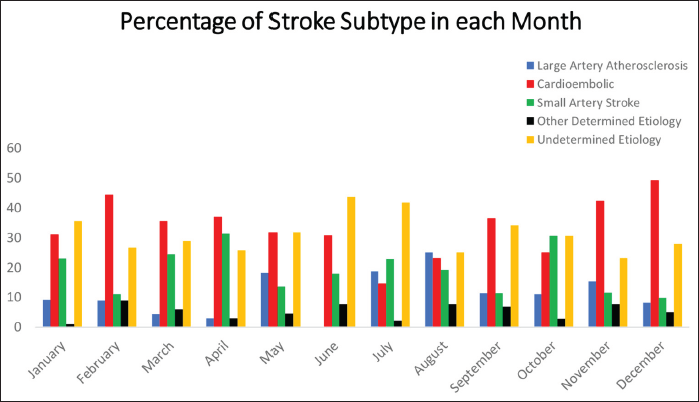
Figure 2 shows the distribution of various ischemic stroke TOAST categories in different months of a year. Cardioembolic strokes were most common in the month of December, while artery-to-artery strokes were most common in August and small artery strokes in April.
Distribution of TOAST Stroke Categories Over Different Months.
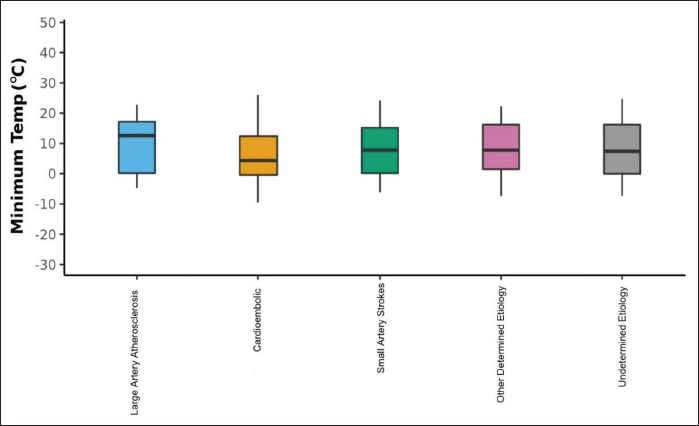
The Box-and-Whisker plot in Figure 3 depicts the distribution of minimum temperature (°C) in the five subtypes of ischemic stroke as per the TOAST schema. The middle horizontal line represents the median minimum temperature (°C), the upper and lower bounds of the box represent the 75th and the 25th centile of minimum temperature (°C), respectively, and the upper and lower extents of the whiskers represent the Tukey limits for minimum temperature (°C) in each of the groups. Cardioembolic strokes were more common than other ischemic stroke subtypes at lower minimum temperatures (p-value = .018)
Relationship Between Minimum Temperature and Ischemic Stroke Subtypes.
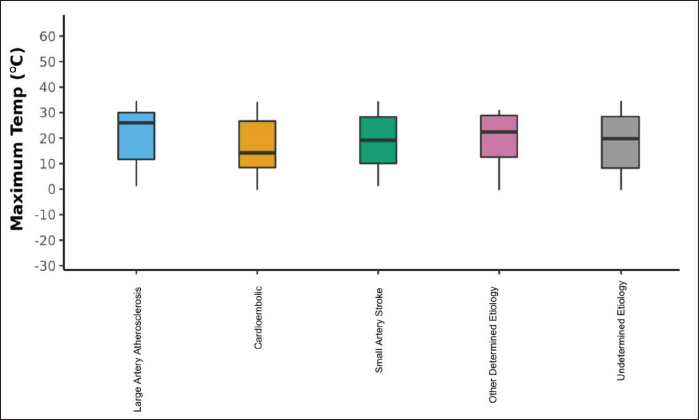
The Box-and-Whisker plot in Figure 4 depicts the distribution of maximum temperature (°C) in the five ischemic stroke groups. The middle horizontal line represents the median maximum temperature (°C), the upper and lower bounds of the box represent the 75th and the 25th centile of maximum temperature (°C), respectively, and the upper and lower extents of the whiskers represent the Tukey limits for maximum temperature (°C) in each of the groups. Artery-to-artery strokes were more common at higher maximum temperatures, whereas cardioembolic strokes were more common at lower mean maximum temperatures.
Relationship Between Maximum Temperature and Ischemic Stroke Subtypes.
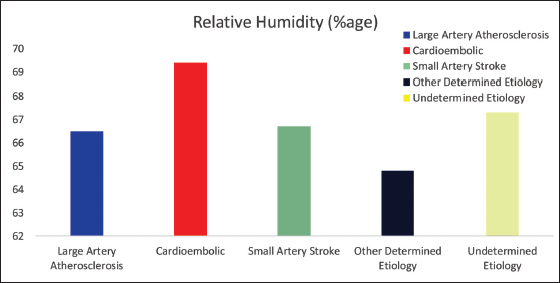
The bar graph in Figure 5 depicts the means of relative humidity (%) in the five different ischemic stroke subgroups, which is not statistically different in different ischemic stroke subtypes.
Relationship Between Humidity and Ischemic Stroke Subtypes.
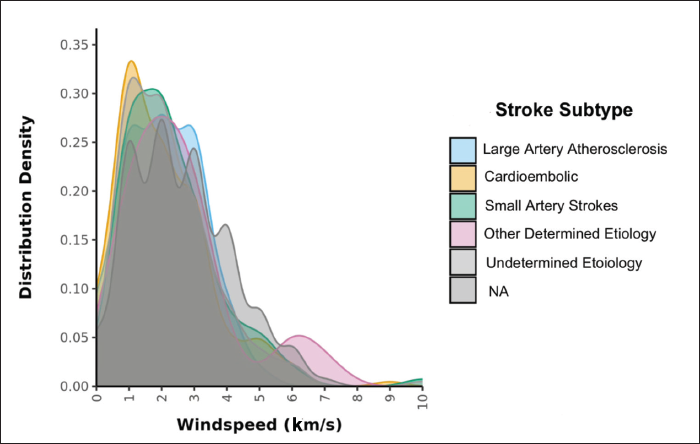
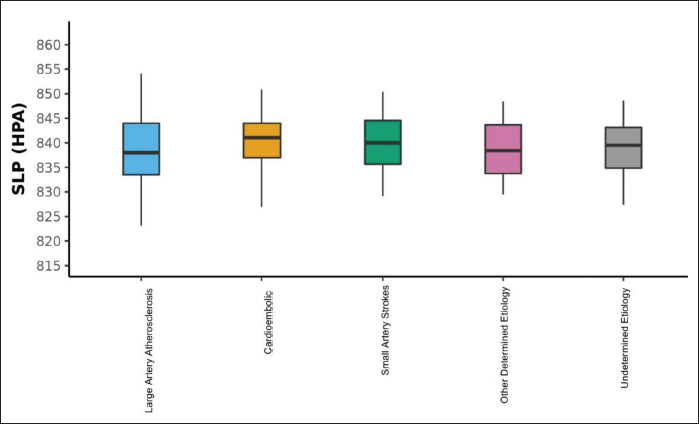
The density plot in Figure 6 depicts the distribution of wind speed (km/s) in the five different subgroups of ischemic stroke, which is not statistically different in these subtypes.The Box-and-Whisker plot in Figure 7 depicts the distribution of atmospheric pressure (HPA) in the five ischemic stroke subgroups. The middle horizontal line represents the median SLP (HPA), the upper and lower bounds of the box represent the 75th and the 25th centile of SLP (HPA), respectively, and the upper and lower extents of the whiskers represent the Tukey limits for SLP (HPA) in each of the groups. There was no statistically significant difference in atmospheric pressure in different ischemic stroke subtypes.
Relationship Between Wind Speed and Ischemic Stroke Subtypes.
Relationship Between Atmospheric Pressure and Ischemic Stroke Subtypes.
Discussion
Cardioembolic strokes form a significant proportion of ischemic strokes, usually associated with bigger infarcts with higher mortality and greater disability. The introduction of novel orally acting anticoagulants (NOACs) in the prevention of cardio-embolism has made treatment simpler and ameliorated the need for frequent monitoring of therapeutic responses like INR (international normalized ratio). Also, novel screening methods such as prolonged recording devices (e.g., loop recorders), blood markers (e.g., pro-BNP), and electrocardiographic and imaging markers have increased the prevalence of cardioembolic strokes.11–14 While many of the risk factors for ischemic strokes may be modifiable and/or potentially modifiable, non-modifiable risk factors pose a special problem. Weather has long been considered a factor that affects stroke risk variously. The seasonal variations of stroke prevalence might affect the management of stroke, particularly secondary prevention. In our study, we found that cardioembolic strokes are more common in winter months, whereas artery-to-artery strokes occur in hot summer months. Lacunar strokes were more common in Spring months. Cardioembolic strokes were associated with lower maximum and minimum temperatures. Thus, although the incidence of ischemic strokes in general increases in winter, the effect of cold weather is more prominent in cardioembolic strokes as compared with other stroke subtypes.15, 16 The mechanism of this increased risk is largely unknown, but cold-induced hypertension, hypercoagulability, and fibrinolysis are some of the proposed mechanisms. Elevated plasma levels of fibrinogen and Factor VII clotting activity during the winter season may induce a pro-coagulant state promoting the formation of blood clots in the left atrium and thus resulting in embolism and strokes.
Atrial fibrillation is the most common arrhythmia encountered in clinical practice. This poly-etiological arrhythmia increases in incidence with advanced age and often predisposes to cardio-embolism particularly strokes increasing the risk of ischemic strokes by four- to five-fold. 17 The strokes are particularly large, often multi-focal and associated with significant morbidity and mortality. 18 The occurrence of paroxysms of atrial fibrillation may be affected by seasonal factors with maximum incidence during winter months and lesser during summer months. A considerable influence of a cold front may exist, explained by the effect of electromagnetic waves occurring in the zone of atmospheric changes, which may penetrate into buildings. 19 Thus, patients with an underlying substrate for the development of atrial fibrillation such as hypertension, ischemic heart disease, hyperthyroidism, and enlarged left atrium may have an increased risk of strokes during the winter season not only from an induced pro-thrombotic state from inclement weather but also due to higher chances of developing atrial fibrillation. Such an observation may create a therapeutic window for screening of atrial fibrillation in such high-risk groups and, if detected, an earlier introduction of anticoagulation to avoid the disastrous effects of ischemic stroke. Also, ischemic strokes are more common during winter months and cool days in patients with underlying atrial fibrillation of any cause. 20 Thus, during winter months, patients with underlying atrial fibrillation should be closely monitored for compliance to anticoagulation, and frequent INRs in those on vitamin K antagonists should be made a routine in clinical practice.
Low humidity is associated with increased blood viscosity which is an established risk factor for ischemic stroke.21–23 However, the association between air humidity and the risk of stroke has been controversial. 24 Elevated atmospheric pressure may promote plaque rupture by exerting pressure on atherosclerotic plaques, thus increasing the risk of ischemic stroke. However, the studies assessing the risk of stroke and these environmental variables have largely been inconclusive.25, 26 We also did not find any significant correlation between stroke risk and weather variables such as atmospheric pressure, air humidity, and wind speed. Although the relation between absolute values of meteorological variables and stroke risk is controversial, changes in weather particularly when rapid have been consistently found associated with an increased risk of stroke. 27 Rapid decreases in ambient temperature and rapid changes in relative humidity and atmospheric pressure, whether negative or positive, increase stroke risk under temperate climate conditions, particularly in patients with underlying cardiac ailments. 28 Although this study supports the notion that cold weather is associated with a higher risk of cardioembolic stroke, certain questions remain unanswered and may stimulate further research. First, should patients, who are at high risk for the development of AF like underlying ischemic heart disease, elderly hypertensive patients, and patients with enlarged left atrium undergo screening for atrial fibrillation and if detected, anticoagulated? Second, should patients on vitamin K antagonists for atrial fibrillation be maintained on higher INR during winter months? Finally, should patients with underlying atrial fibrillation and/or other cardiac ailments be advised to shift to warmer areas during winter months?
Conclusion
Cardioembolic strokes are often large and multifocal, thus associated with greater morbidity and mortality. Despite large advances in the determination of modifiable risk factors for stroke, significant non-modifiable risk factors exist. In regions with inclement weather, cardioembolic strokes remain a significant healthcare concern in the winter season and may require augmentation in the management of underlying predisposing conditions like atrial fibrillation.
Availability of Data and Material
Available with the corresponding author.
Consent for publication
All authors have approved the manuscript for publication.
Footnotes
Acknowledgments
We acknowledged patients for giving us consent to be a part of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Ethics Committee (IEC) of Sheri Kashmir Institute of Medical Sciences (SKIMS) Srinagar on 6 November 2019.
Funding
We Received a grant from Sheri Kashmir Institute of Medical Sciences, J & K, India 190011.