
Abstract
Background
As the communal cause of irreversible vision loss in seniors, glaucoma affects more than 67 million people worldwide. Those who suffer from glaucoma have traditionally demonstrated a higher rate of developing stroke. Numerous studies have investigated the relationship between glaucoma and increased stroke risks, but they differ wildly in conclusive findings. To better elucidate the overall findings of the collective studies, a systematic review with the objective of determining the relationship between glaucoma and an increased risk of stroke.
Methods
A systematic database search including MEDLINE, EMBASE, and Cochrane Library as well as unpublished literature was done. Distiller SR, a systematic review software was utilized. After two levels of screening, “Title and Abstract” and “Full text” screening, risk of bias assessment and extraction of the data from the included articles were conducted. STATA 14.0 was used to conduct the meta-analysis. The hazard ratio (HR) was the primary outcome measure.
Results
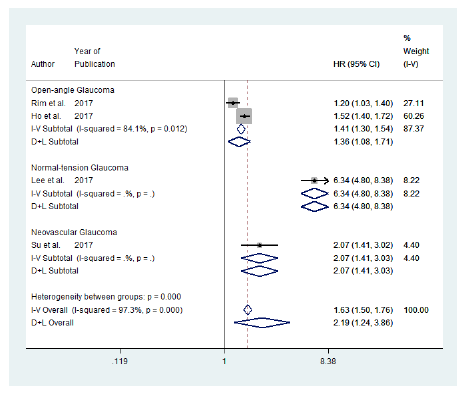
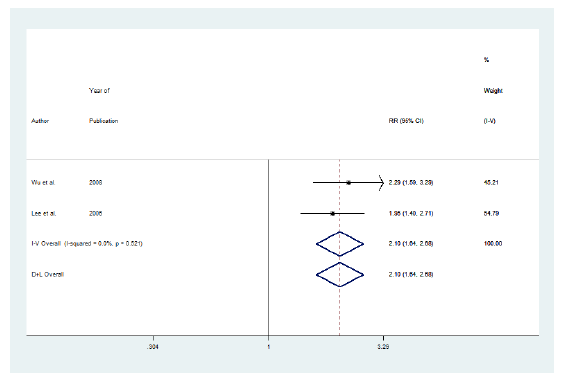
Nine studies (376,650 subjects) were included in the analysis. Results indicated a significant hazard of stroke in patients with open-angle glaucoma (HR = 1.36, 95% confidence interval [CI]: [1.08, 1.71]), normal-tension glaucoma (HR = 6.34, 95% CI: [4.8, 8.38]), and neovascular glaucoma (HR = 2.07; CI: [1.41, 3.03]). Studies examining risks of stroke development showed a significant increase in the relative risks (RR) of developing stroke for those with glaucoma (RR = 2.10, CI: [1.64, 2.68]).
Conclusions
The hazard of developing stroke could be greater for patients with glaucoma. However, randomized controlled trials with longer-term follow-ups need to be conducted in the future in order to make strong conclusions.
Introduction
Glaucoma is a degenerative eye disease that may lead to damage of the optic nerve, loss of vision, and blindness. Additionally, in the world, glaucoma is the second leading cause of vision loss affecting more than 400,000 Canadians 1 and 67 million people worldwide. 1 The global prevalence of glaucoma steadily increased to 80 million people worldwide by 2020 and continues to increase. 2 Direct costs related to glaucoma care for the approximately 2 million US citizens undergoing treatment are estimated to be $2.9 billion. 3 Indirect costs, those which account for productivity loss due to days missed from work, are more difficult to calculate but represent a growing burden on society due to the extreme prevalence of glaucoma. Direct costs arising from glaucoma increase as the severity of the disease increases as it warrants greater medical attention; as approximately half of all patients affected by glaucoma are unaware of their affliction, 4 should they seek out care in the later stages of their treatment—the financial burden on society would increase explosively. The magnitude of this potential financial burden entirely overshadows the existing direct costs, and its realization would put an enormous strain on an already strained public healthcare system.
Although no cure exists for glaucoma, its progression can be delayed with medications. Medication plans vary from patient to patient, but most therapies rely on using a combination of oral and topical medications. The average direct cost may vary from $623 USD per year for early-stage glaucoma patients to $2,511 USD 5 per year for end-stage glaucoma patients. 5 As glaucoma is a chronic disease, treatment is lifelong. This invariably means that any new cases of glaucoma that arise will always pose a consistent financial burden on the public health care system. Since glaucoma is expected to increase in the number of people afflicted, seeking new preventative measures and uncovering information related to the disease is of paramount importance in order to maximize the efficacy of current healthcare and curb the socioeconomic burden caused by this inevitable inflation.
Numerous risk factors are associated with glaucoma. Although no conclusive results exist, there has long been a suspected link between developing glaucoma and suffering from an increased risk of cardiovascular disease. 6 Some studies7–10 have demonstrated that the development of cardiovascular disease in a patient can accelerate the progression of their pre-existing glaucoma implying a level of interaction between the two diseases and possibly a more significant physiological relationship. Patients with glaucoma have also demonstrated an increased susceptibility to suffering a stroke within a five-year follow-up period after their initial diagnosis. 11 Although numerous studies have investigated a possible relationship between glaucoma and increased stroke risk, they vary in their focus, sample size, methodology, and conclusiveness. As such, a definitive relationship or lack of relationship between the two conditions has yet to be established.
The purpose of the current systematic review of existing literature is to better elucidate the overall findings of the collective studies that have been performed with the overall objective being to evaluate the existence of a relationship between glaucoma and an increased risk of stroke.
Methods
Literature Search Strategy
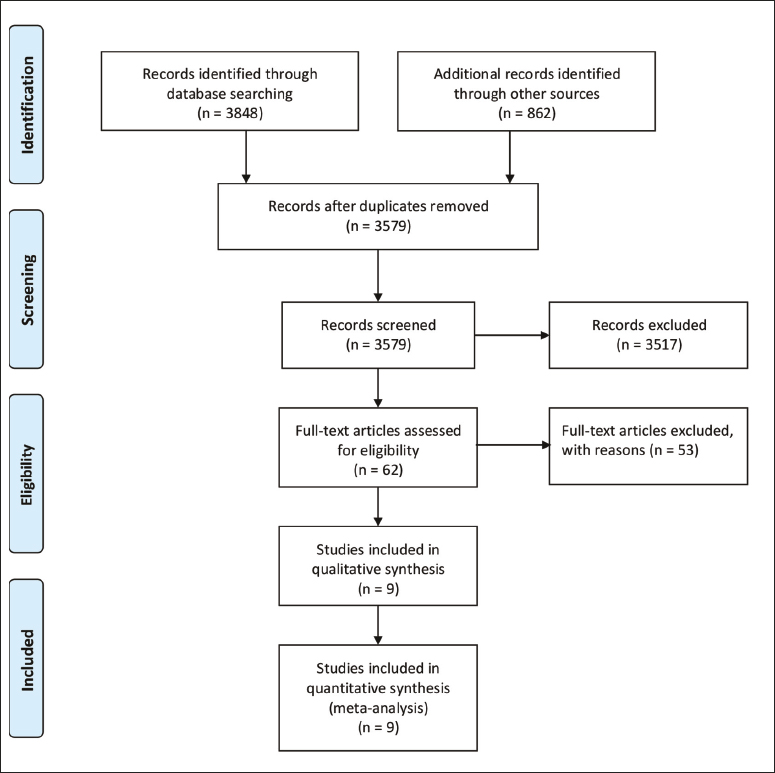
MEDLINE In-Process & Other Non-Indexed Citations, MEDLINE Daily and MEDLINE (Ovid), EMBASE (Ovid), and the Cochrane Library (Wiley) were searched thoroughly and systematically. Additionally, auto alerts were set for the relevant monthly new literature. Further, monthly updates were performed on other databases including HEED, PubMed, and Cochrane Library databases. This research study included relevant articles published till June 30, 2023. Search strategies were constructed with the help of a librarian or an information specialist, utilizing database-specific subject headings and keywords for “glaucoma,” “open-angle glaucoma,” “neovascular glaucoma,” and “ocular hypertension,” “stroke,” “cerebral infarction,” and “cerebrovascular disorders.” Database-specific search strategies were designed. The supplementary material (S1) contains the details of searches conducted on MEDLINE, EMBASE, Cochrane, and Web of Science. Preferred Items for Systematic Reviews and Meta-Analyses guidelines, represented in Figure 1, were used. 12 Ethics approval from the Research Ethics Board (WREM) at the University of Western Ontario is not applicable since no animal or human participants were recruited for the study. Further, patient consent was not applicable since all data is gathered from published sources.
PRISMA Flow Diagram
The grey literature search included ProQuest Dissertations and Theses, the Canadian Health Research Collection (Ebrary), Web of Science, as well as any available meeting abstracts of the European Society of Ophthalmology, Canadian Ophthalmology Society, Association for Research in Vision and Ophthalmology, and American Academy of Ophthalmology. Further, web-based information was searched using Google and other Internet search engines. Further, appropriate experts and agencies were contacted, and hand-searching the bibliographies of all the included studies was carried out.
Inclusion and Exclusion Criteria
Randomized control trials, economic studies, clinical trials, comparative studies, multi-center studies, observational studies, cohort studies, meta-analyses, systematic reviews, and case series were included. Second, studies on human participants were included. Third, studies evaluating mild to moderate glaucoma patients were included in the review. Fourth, studies on adults 18 years old and above were included. Conversely, opinion articles, surveys, editorials, pilot studies, and case reports were excluded. A sample size of at least 20 patients was essential in order to exclude poor-quality articles. Articles omitting complications as well as post-operative outcomes were excluded. English language articles were included. Further, no limitations were placed by the length of the follow-up or location of the study.
All the identified articles through the published and unpublished literature were imported to Distiller SR, (Evidence Partners, Ottawa, Canada). Imported articles were scanned for duplicates manually. After the removal of the duplicate records, the remaining articles were screened at two levels. The screening was conducted by two reviewers independently. The first level of screening was called the “Titles and abstracts screening,” and the second level of screening was called the “full text screening.” For details of the two levels of screening, refer to the supplementary material (S2). Two reviewers (MR and AS) independently screened the studies at each level. At the end of each level of screening, agreements, and disagreements were calculated using Cohen’s kappa (κ) coefficient. Disagreements were resolved by consensus and if consensus was not reached then a third reviewer (MSMM) intervened.
Quality Assessment
The modified Downs and Black checklist 13 was used by the reviewers to perform the quality assessment. From the included nine articles, eight articles were determined to be of fair quality7–11, 14–16 while one was considered to be of poor quality. 6 Additionally, none of the lesser-quality articles were excluded given the limited data availability.
Data Extraction
A data extraction sheet was designed in Excel and approved by the senior investigator. First author’s last name, publication year, design and location of the study, follow-up times (in years), total number of participants, total participants enrolled and completed, participants demographic characteristics, percentage of female patients, type of glaucoma studied, stroke occurrence, adjusted hazard ratio (HR), odds ratio (OR), and relative risks (RR) were extracted.
Statistical Analysis
STATA v. 14.0 (STATA Corporation, College Station, TX, USA) was used to conduct the meta-analysis. The primary outcomes included the adjusted HR, OR, and RR. For categorical data, HR, OR, and RR were calculated as the treatment effect or effect size. Further, based on the presence of heterogeneity, the effect size for each study was then aggregated using the fixed or random-effect model to estimate the summary effect.
To test heterogeneity,
Results
Search Results
The database search identified 3,848 records and 862 records were obtained from the grey literature search. After removing duplicates, a total of 3,579 records remained. Distiller SR was used to remove duplicates. The remaining records were manually screened to remove duplicates that were not removed by Distiller SR. After screening, 62 included articles were screened for full text. Nine studies (376,650 subjects) were included for analysis. Kappa statistics for each level of screening were 0.52 and 0.66, respectively.
Study Characteristics
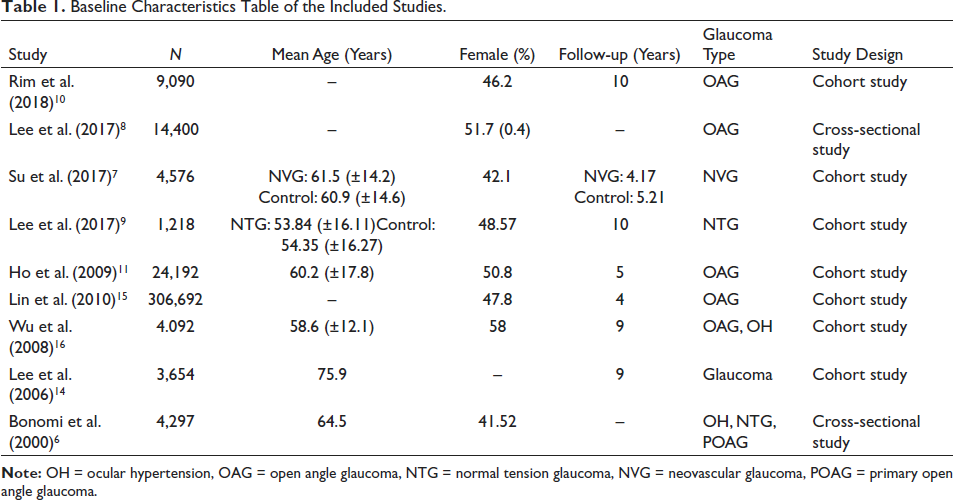
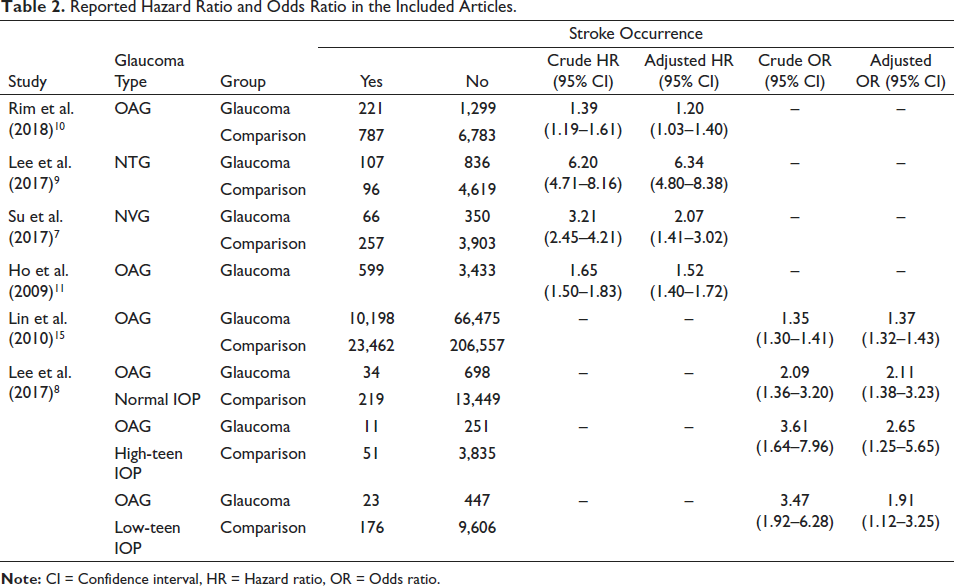
Table 1 lists the sample size, mean age, follow-up in years, study design, and type of glaucoma studied of the included articles. Two articles6, 8 were cross-sectional studies and seven articles7, 9–11, 14–16 were cohort studies. Table 2 lists the stroke occurrence, crude and adjusted HR and 95% confidence interval (CI), and crude and adjusted OR and 95% CI. Table 3 lists the RR of stroke and 95% CI.
Baseline Characteristics Table of the Included Studies.
Reported Hazard Ratio and Odds Ratio in the Included Articles.
Reported Relative Risks in the Included Articles.

Publication Bias
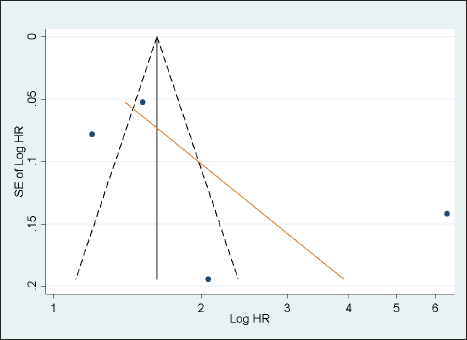
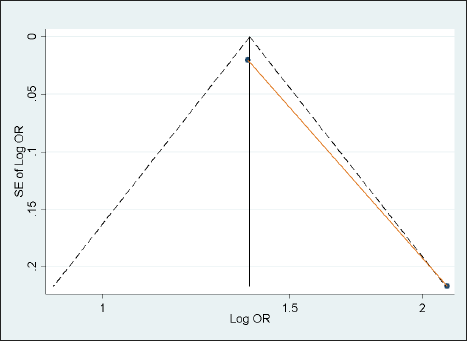
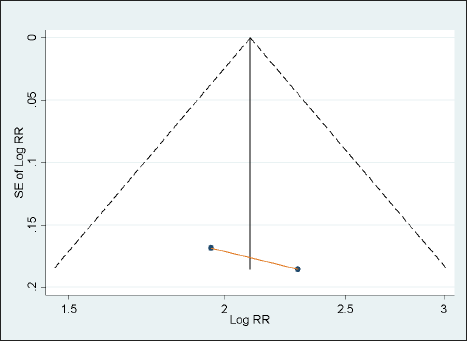
Figures 2.1–2.3 represent funnel plots for HR, OR, and RR of stroke occurrence, respectively, including the fitted regression line from the standard regression (Egger) test for small-study effects. Figure 2.1 shows studies scattered from the top left of the plot to the bottom right of the plot. In Figure 2.2, studies are scattered around the central line of the plot. In Figure 2.3, studies are scattered at the bottom. Further, a few studies at the bottom of the three funnel plots indicate the unpublished small studies with non-significant study results. Additionally, weak evidence for the presence of small-study effects was provided by Egger’s test.
Funnel Plot for Studies Examining Adjusted Hazard Ratio (HR)
Funnel Plot for Studies Examining Adjusted Odds Ratio (OR)
Funnel Plot for Studies Examining Adjusted Relative Risks (RR)
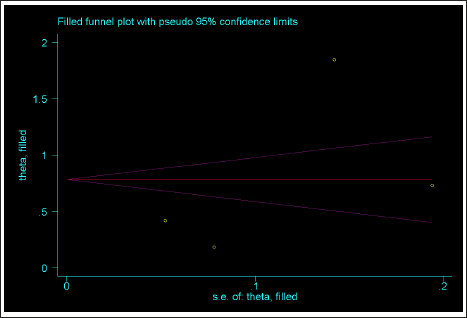
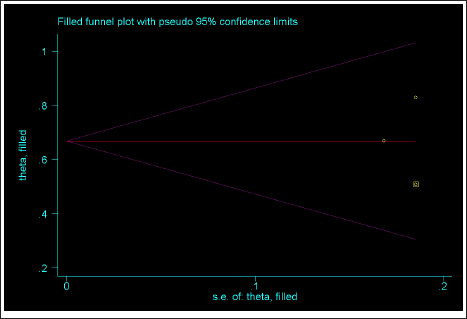
To account for publication bias, a non-parametric Trim and Fill method was used. Figures 2.4–2.6 represent the funnel plots developed using the Trim and Fill method. In Figure 2.4, no “missing” studies were added to the dataset and therefore, the variance between studies and evidence of heterogeneity remained unchanged (p = .0). In Figure 2.5, one missing study was added to the dataset, moving the random-effect summary estimate to OR = 0.315; CI: [−0.37, 0.66]). The new estimate was slightly lower and was non-significant. In Figure 2.6, one missing study was added to the dataset, which resulted in the new estimate of RR = 0.668; CI: [0.465, 0.66]). The new random-effect summary estimate remains statistically significant. This suggests that the correction for publication bias did not change the overall interpretation of the dataset.
Funnel Plot Using Trim and Fill Method for Studies Examining Adjusted Hazard Ratio (HR)
Funnel Plot Using Trim and Fill Method for Studies Examining Adjusted Odds Ratio (OR)
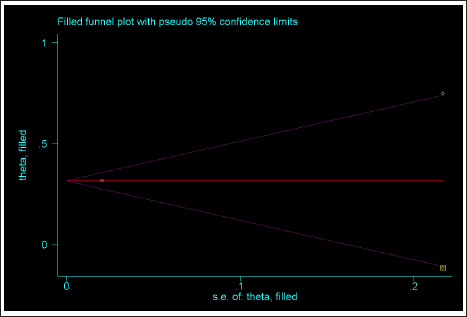
Funnel Plot Using Trim and Fill Method for Studies Examining Adjusted Relative Risks (RR)
Main Outcomes
The hazard, odds, and RR of stroke in glaucoma patients were the main outcomes to be analyzed.
Effect on HR
The HR by type of glaucoma has been summarized in Figure 3. There is a significant increase in the hazard of stroke in glaucoma patients. Significantly (
Forest Plot for Adjusted Hazard Ratio (HR) by Type of Glaucoma
Effect on OR
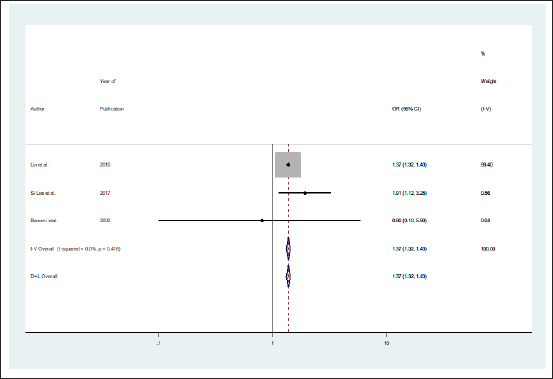
The odds of stroke in glaucoma patients are summarized in Figure 4. A non-significant (p = .416) heterogeneity was observed between the three articles examining the odds of a having stroke in glaucoma patients. Figure 6 suggests that the odds of developing a stroke were 1.37 times greater for those with glaucoma (OR = 1.37, CI: [1.32, 1.43]). Therefore, results indicate higher odds of developing stroke in glaucoma patients. However, ORs need to be interpreted conservatively since the unexplained variance in the model can impact ORs.17
Forest Plot for Adjusted Odds Ratio (OR)
Effect on RR
Figure 5 illustrates a forest plot of RR of stroke in glaucoma patients. Studies examining risks of stroke development showed a significant increase in the RR of developing stroke for those with glaucoma (RR = 2.10, CI: [1.64, 2.68]) with a non-significant (
Forest Plot for Adjusted Relative Risks (RR)
Discussion
A systematic review was performed to examine the hazards, odds, and risks of developing stroke in patients with glaucoma. The principal outcome measure was HR, OR, and RR of stroke in patients with glaucoma. Nine studies (376,650 subjects) were included for synthesis. The characteristics of the included studies were summarized.
The hazard of developing stroke could be greater for those with open-angle glaucoma, normal-tension glaucoma, and neovascular glaucoma. The hazard of developing stroke could be greater for those with glaucoma in general. Additionally, patients with glaucoma are twice at risk for developing stroke compared to controls. A substantial strength of this analysis stems from the fact that all the included studies had coherent results of a significant increase in the hazard of stroke occurrence in those with glaucoma.
Significant heterogeneity was seen among studies examining stroke incidence in glaucoma patients. Therefore, random-effect models using the DerSimonian and Laird method were computed. Further, good quality articles are required in the future to fully understand this relationship. Numerous reasons could exist for the substantial heterogeneity between the studies including different study populations adjusted for comorbidities, different patient demographics, inclusion/exclusion criteria, study location, design, and year the study was conducted. The results of this quantitative synthesis of the currently available literature suggest that more studies need to be reported to better understand the association between glaucoma and the rate of stroke occurrence.
Like every other study conducted, limitations to this study do exist. First, in this research, the modified Downs and Black checklist 13 was employed to check the quality of the articles that were included in the analysis. The modified Downs and Black checklist unveiled a significant variation in quality scoring with high-, medium-, and poor-quality studies having been reported. Nevertheless, given the limited relevant articles available after the thorough search of the literature, all were included, irrespective of their quality. This is a recognized, but necessary, limitation due to the few clinical studies currently available. Second, ORs could get impacted by the unexplained variance in the model and therefore, need to be interpreted conservatively. 17 Third, the inherent biases in the included studies could influence the results the meta-analysis of observational articles, which could get influenced by Ref. [ 18 ]. For example, numerous factors in the articles such as patient population, disease severity, setting, study designs, baseline patient characteristics, and location of the study been performed, could influence the estimates in the original studies.
In conclusion, the hazard of developing stroke could be higher for those with open-angle glaucoma, normal-tension glaucoma, and neovascular glaucoma.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethics approval from the Research Ethics Board (WREM) at the University of Western Ontario is not applicable since no animal or human participants were recruited for the study. Further, patient consent was not applicable since all data is gathered from published sources.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.