
Abstract
The dialysis machine acts as an artificial kidney, a lifesaver for patients whose both kidneys have failed. But the dialysis process is physically painful and economically stressful, especially for poor patients. Even for the government the cost of providing dialysis services to poor patients is exorbitant. This is a case of the setting of the dialysis centres by the Andhra Pradesh Government in partnership with the private service provider on a public-private partnerships basis. There was a dilemma whether to do this project wholly through government budgets or forming a partnership with a private party to implement the project. The project emerged as a successful and imitable example of a public–private partnership for the rest of the country and other developing countries. Apart from being a financially sound and bankable project, efficient project management, efficient contract and risk management, vigilant monitoring by the government, sound payment mechanism and mutually beneficial partnership are the driving factors for the success of this pioneering healthcare PPP project in India.
Year: 2008, Location: Srikakulam in Andhra Pradesh
Sixty-nine-year-old Kanka Rao from Srikakulam in Andhra Pradesh was suffering from chronic kidney failure End-Stage Renal Disease (ESRD). His both kidneys were unable to filter the metabolic toxins and surplus water from the blood for secretion through the urine. As both the kidneys failed to filter the blood, an excessive amount of protein was excreted through the urine; as a result, his body was lacking this protein. In addition, edemas (retained water) were formed in his legs and lungs damaging those organs.
The inadequate removal of toxins started to upset the heartbeats leading to an infection in the heart sac. The nephrologist suggested the remedy of a kidney transplant. Mr Rao tried this option for three years but could not get any kidney donor. The only option left was to go on regular, life-saving, dialysis treatment at a dialysis centre to prevent the damage to further organs. Of course, the dialysis exercise was painful, with each session requiring four hours for the dialysis apart from the waiting and traveling time.
Apart from this physical pain, Kanka Rao, who retired from the education department after serving for more than 36 years, was struggling with the daily challenge of bearing the exorbitant expenses of availing dialysis services. All of his lifesavings were diminishing fast to get dialysis sessions that were costing ₹35,000 per month including travel expenses to the dialysis centre 100 km away from his home. Rao said ‘I needed three dialysis sessions every week. The cost of dialysis itself was too high but the cost of traveling compounds the financial burden, thus making it impossible for a retired person like me’.
Year: 2009, Location: Andhra Pradesh State Government Headquarter
A meeting was arranged on 23 January 2009, at the headquarters of the state government of Andhra Pradesh. The meeting was chaired by Mr Prabhakar Rao, the minister of health. The other participants in the meeting included Mr Niraj Kapoor—Chief Secretary, Mr Ashutosh Apte—Secretary, Health ministry, Mr Harish Sen-Secretary, finance ministry, Prof. Nitin Rao—Technology & Project Management expert, Dr Rupesh Shah—Nephrologist and Mr Vikas Sharma—Legal Advisor.
Excerpt of the Meeting
After the Meeting
Andhra Pradesh State Government appointed a committee comprised nephrologists, legal experts, financial experts and senior government bureaucrats. The committee suggested adopting the public-private partnership (PPP) model which was evolving in the Indian infrastructure sector mainly in the transport and power sector. This project was going to be the first-ever PPP project in the healthcare sector in India.
Procurement Process
The Procurement Committee was established to ensure consistent and correct application of procurement practices. The health secretary of the state was appointed as head of the procurement committee comprising legal, finance, medical and technical experts. In four months, the committee designed and drafted the complete bidding process and prepared the PPP contract terms. The significant terms of the concession are presented in Exhibit 1.
Selection Process
The procurement committee spearheaded the selection process of the applicant/s for operation and management of the services on PPP basis, based on the eligibility criteria (Exhibit 2).The selection criteria were as described:
The service provider must be registered with appropriate statutory authority of the state/central government or under the Companies Act. The service provider shall have a minimum of 5 years of experience in providing health care activities. The service provider shall have a minimum experience of 3 years of running a dialysis centre. The annual turnover of the organization shall be ₹60 million in the last 2 financial years. No litigation shall be pending and no penal measures were taken against the applicant under applicable acts and laws.
Through the selection process, applicants were shortlisted based on the points scored by the applicants on each of the criteria as described in Exhibit 2. The physical inspection of the facilities of the applicants with the prior intimation was undertaken by the procurement committee for gathering information for a short listing of applicants for further processing of selection. The minimum qualifying marks were 60% for the selection in the next round. After short-listing of applicants, the final selection of the service provider from the short-listed bidders was done based on the minimum charges quoted per dialysis session. The procurement committee called the service providers shortlisted in a bidding process to seek clarifications on issues and information or documents.
After a rigorous competitive bidding process, involving technical and financial rounds, and a subsequent round of discussions, Kidney Care (India) Pvt Ltd, 1 a subsidiary of Kidney Care AG, one of the world’s leading healthcare suppliers headquartered in Germany, was awarded the work of setting and operating the dialysis centre in 10 tertiary state-run hospitals on a Build, Operate and Transfer (BOT) basis for seven years linked with the state-run Rajiv Arogyasri health insurance scheme.
Project Implementation
The project was launched in 2010. The Government of Andhra Pradesh provided basic medical treatment to patients living below the poverty line (BPL), free of cost, covered under the Rajiv Arogyasri Insurance Scheme. The Government paid the Kidney Care an agreed price for each performed dialysis. A total of 10 haemodialysis centres hosting 100 haemodialysis machines were established and run by Kidney Care in 10 medical colleges and hospitals in Kakinada, Kurnool, Vishakhapatnam, Srikakulam, Anantapur, Vijayawada districts and NIMS Hyderabad. Kidney Care set up the centres with an investment of ₹20 crores. The Government of Andhra Pradesh paid ₹1,200 per dialysis out of which ₹1,050 was paid to Kidney Care and ₹150 was paid to the respective hospital/medical college.
The district hospitals provided space, electricity, water, nephrologists and supporting staff hired from within the hospitals, making the project cost-efficient. The centre followed the standard protocols for dialysis sessions and maintenance of the facility which was evident from the practice of using distilled RO (reverse osmosis) water for treatment purposes, a practice that may not be as rigorously followed at other centres. The dialysis centres employed efficient bio-medical waste management practices at par with the global standards. Two separate machines were reserved for patients with the risk of infections such as HIV at each dialysis centre. This initiative was the first of its kind PPP model for providing low-cost services to kidney patients in India. According to the incidence rate of ESRD in Andhra Pradesh, there were more than 10,000 patients suffering from kidney-related ailments. These centres come as a great relief to many of these patients to be precise 1,000 patients.
The Monitoring Mechanism
The competent authority of the hospital on behalf of the government, monitored the day-to-day operational activities of the services is undertaken by the service provider. The performance review was conducted by the government authority on a quarterly basis. The senior government officials regularly hosted the performance review meetings. The service partner was required to submit monthly reports in a prescribed format to the concerned officials.
The software approved by the government was installed by the service provider to disseminate information through LAN to the superintendent of the concerned hospital on daily basis on multiple parameters related to the operation, management and performance of the dialysis centre and details of the free services extended to the eligible patients. The government at the state level approved the software packages to be installed by the service provider as well as providing the necessary support to the hospital authorities for monitoring the performance of the services at the concerned hospitals.
The Economic Aspects of the Project
The total cost concept termed Total Cost of Ownership (TCO) was employed to perform a post facto financial analysis of the project to check the adequacy of financial returns for the private partner and value for the money for the government using a financial model as shown in Exhibit 3. It was decided that the ten machines per dialysis centre at contracted rates of ₹1,080 per dialysis session was the most ideal choice to opt for and was in the range which the government was anticipating the rate to be. The cost of the dialysis service ₹1,080 was the amount reimbursed by the government to the service provider, the amount which the service provider collected from the patients and deposited in a designated bank account, and the government reimbursed the service provider separately every month in proportion to the service provided.
The financial analysis demonstrates the commercial viability for the private partner at the contracted price of the dialysis service. The per-session dialysis rate of ₹1,080 was calculated assuming reusing the dialyzer three times for the same patient. If this could be increased, the cost of service delivery could have been brought down even more and the bid variable could be brought down even lower. The finance for this project was arranged under Rajiv Arogyashri Insurance Scheme, the financial grant available from various governmental development projects as well as the departmental fund for procurement, and the dialysis cost recovered from the above poverty line patients.
Statutory and Legal Framework
The dialysis was governed by all the prevalent biomedical, statutory and legal laws/orders governing a similar centre. All the dialysis centres obtained the following certificates:
Building Permit from Works Officer No objection certificate from Fire Officer
The Statutory Acts
Indian Medical Council Act and Code of Medical Ethics, 2002
Drugs and Cosmetics Act, 1940 and Rules 1945.
The license under Bio-medical Management and Handling Rules, 1994
Right to Information Act, 2005
Consumer Protection Act, 1986
The service partner was responsible for the operation and management of the dialysis services under the legal agreement for seven years renewable thereafter based on comprehensive performance appraisal and mutual consent of both the partners. The regular review of performance was undertaken on a quarterly basis. The agreement incorporated the causes for the termination of the agreement.
Safety Measures
The dialysis machines and various processes were operated under the strict trained manpower supervision. The following safety measures were taken into account:
Dialysis machines and associated equipment were located and designed as per the manufacturer’s specific layout guidelines. New machines were purchased instead of a refurbished one. Machines were under an annual maintenance contract for regular maintenance. All possible fire safety measures were adopted. Proper biomedical waste collection, storage and disposal norms were developed, and adhered to.
Environmental Impacts
The dialysis procedure did not produce any harmful radiations or noise, but body fluid wastes were generated during the procedure, which were collected, stored and disposed of safely by the service provider.
Stringent biomedical waste disposal processes were developed and implemented by the partner.
Social Impacts
The improved availability of the tertiary medical treatment and low cost of the service reduced the cost of dialysis service at the private dialysis centres.
Increased awareness about hypertension and diabetes cases in the community.
The patients were benefited by the private sectors quality and efficiency at the government prices, reducing the economic cost of availing the dialysis services.
Enhanced patient satisfaction and diminished strain.
Employment generation for the trained manpower required for operating the centre.
Streamlined operations and efficient work culture of the private partner positively impacted the government healthcare functioning.
Economic Impact
The government was able to discharge its duty of providing good quality dialysis facilities to its citizens at affordable cost thus achieving value for money for its investment while the private partner Kidney Care has gained access to more patients, sold its dialysis machines, and achieved an attractive IRR of 44% (Exhibit 3) on its investment in this project. So, it is an economically WIN–WIN situation for both the partners and emerged as a successful and imitable example of public–private partnership for the rest of the country and other developing countries. A strong payment mechanism linked to the Rajiv Arogyashri insurance scheme and the price of ₹1,080 was correctly chosen. The contract formation, implementation and enforcement were very efficient and a strong partnership was observed between both the parties.
Year: 2016, Location: Andhra Pradesh
More than the disease or even threat to my life, I was petrified of the expenses and financial burden on my family because of me. My husband, who hardly earns ₹10,000 per month, was very worried. Looking at the expenses at the private hospitals, I wished to skip some dialysis sessions to save money. But with the affordable dialysis treatment at the Kidney Care centre, I have regained some mental strength.
Earlier, Rukmini had to spend nearly ₹30,000 on the recommended twelve dialysis sessions each month and this cost has now been halved. Rama Reddy, her husband, says, ‘I am a landless person without any regular income. The Kidney Care centre has come as a big help to my family’.
Year: 2022, Location: Andhra Pradesh
After completion of this project, encouraged by the positive outcome of the PPP model, the renewed contract was awarded through competitive bidding in 2017 to Nephroplus, a service provider with 140 dialysis centres spread over 80 cities across 17 states in India. Under the new PPP contract, per dialysis charge was decided as ₹965 per treatment, the lowest ever by any service provider in the world. The dialysis centres increased to 27 from 10 out of which 12 in Srikakulam with a high incidence of kidney failure in Uddanam Palasa, Kavigiri and Sompeta areas region of Srikakulam. The earlier Rajiv Arogyasri scheme is now reframed as NTR ArogyaSri, and its card-holders are eligible for free treatment. Andhra Pradesh was the first state in the country to offer a pension of ₹2,500 to patients suffering from kidney ailments. The government has a target to render the treatment to 10,000 patients. In Andhra Pradesh before this project, 25% of patients were receiving dialysis. With this initiative, it has gone up to 50–60%.
Appendix A
Exhibit 1. The Roles and Responsibilities of the Partners Set by the Concession Agreement.
The procurement committee recommended the following Roles and Responsibilities of both the parties, the government and the private service provider, and clauses of contract termination from both the sides.
Roles and Responsibilities of the Hospital Authority.
To provide the space/building for operating the dialysis centre at the premises of the hospital.
Provide medical treatment for emergencies during dialysis.
Ensuring a supply of water and electricity and facilitating the laboratory, diagnostic and ambulatory support.
The water supply will also be provided free of cost.
Necessary NOC from the competent authority of the concerned hospital will be provided to the private partner for procurement of a separate electric meters. The government shall arrange at its cost, the installation of the electrical connection and augmentation if required up to the doorstep of the operating rooms for the facilities.
The government shall institute a monitoring mechanism to bring in operational efficiencies and undertake performance reviews of these facilities.
The government shall facilitate access like jugular/femoral catheterization and AV Fistula at a Government facility.
The required investigations, other supportive and emergency services, treatment of complications, medicines and services for complications shall be provided by the Government.
Roles and Responsibilities of the Private Partner/Service Provider.
The partner shall supply, install, maintain and operate the dialysis centre in the hospital.
The partner shall provide a multi para monitor.
The partner shall supply, install and maintain the RO water plant in the centre.
The partner shall supply, install and maintain Dialysis Chairs, cots, and the mattresses in the centre.
The partner shall change the existing civil and electrical infrastructure to establish dialysis centre.
The partner shall provide Isolation Units for seropositive patients.
The partner shall provide and maintain all ancillary equipment such as the Weighing scale, BP apparatus, Stethoscopes, pH meter and power backup to ensure uninterrupted dialysis sessions.
The partner shall arrange for proper Biomedical Waste (BMW) collection as per respective State Pollution Control Board norms.
The partner shall maintain an appropriate database of patient records.
Recruitment and training of the workforce.
Reporting as per the expected norms of the terms of reference.
Maintaining the dialysis equipment in working condition 90% of the time.
Maintenance of the machines and signing Comprehensive Maintenance Contract with the vendors of the machines after the warranty period.
Complying with the fire safety requirements.
Ensuring the services would be operational round the clock.
Clauses for Termination of Agreement.
Failure to start the dialysis services in the hospital within one month of signing the contract.
Collecting charges from the patients against the set policy on patient charges.
Failure to comply with the statutory requirements, Clinical Establishment Acts, Rules, and other rules and regulations.
Criminal activity by key persons in the service provider organization in terms of the operation and management of the dialysis services.
Employing an unqualified and untrained workforce for providing the dialysis services.
Use of the allocated space by the service provider for any other purpose other than the approved ones.
Failure to deposit concession fee for a given quarter by the due date as per terms of the contract.
Failure to undertake a comprehensive maintenance contract with the machine suppliers.
Upon the occurrence of any of the defaults, the authority shall follow the procedures of issuing Notice/Show Cause before deciding on termination of the agreement. The decision of the procurement committee shall be final and binding on the Service provider.
Exhibit 2. The Selection Matrix for the Service Provider.

Exhibit 3. Post Facto Financial Analysis of the Project Using a Financial Model.
Dialysis sessions per patient—three per week
Number of cycles per machine per day—three
Operating efficiency of the dialysis machine—95% (95% of the time the machine is up and running during working hours)
The government provided built space to the partner for setting up the system
Ten dialysis machines per centre were installed
The power consumption per machine per month (including power utilization for administrative purposes) was 150 units. Per month fixed cost for 55 kW three-phase LT power connection was ₹1,800 and per unit power consumption cost was ₹ 7.00
The average per month diesel consumption is 75 L and the average per litre fuel cost was ₹70
The average water usage in the toilet per patient including the staff was 20 L and the average drinking water usage per patient including the staff was 5 L. Per litre unit cost of water including 20% of sanitary charge was ₹75 per litre.
The centre demarcated one machine out of five for seropositive cases.
The service provider facilitated one nephrologist for every district to consult the patients at the district hospital
The requirements for setting up of a dialysis centre.
Space for dialysis unit—2,500 square feet to 3,000 square feet built-up space for installing ten dialysis machines
Dialysis machines
RO plant
Cot, mattresses, and dialysis chairs
Para monitors, ancillary equipment and crash cart
Consumables
Services/items provided by the government.
Administrative responsibilities, required space, adequate raw water, required electrical power required for running the project.
Required investigations, other supportive and emergency services, treatment of complications, medicines and services for complications.
Services/items provided by the partner.
The partner executed the work of modifying the existing civil and electrical infrastructure to facilitate and establish a dialysis centre.
The partner should operate the dialysis centre in the district hospitals.
The partner was responsible for the maintenance of the machine to enable an uninterrupted service.
The partner operated and maintained the RO water plant in the centre.
The partner provided, installed and maintained cots, mattresses and dialysis chair as per the WHO guidelines/Indian Society of Nephrology guidelines.
The partner provided, installed and maintained Para monitors of approved specification as per following ratio: 2 Para monitors for 10 machines.
The partner provided for Isolation Units for HBs Ag and HCV patients as per following ratio: 2 in 10 machines.
The service provider supplied and maintained all the required ancillary equipment such as a weighing scale, blood pressure machine, stethoscopes.
The partner arranged the backup power for the machines to ensure the uninterrupted dialysis.
The partner provided facilities for the disposable, equipment and patient belongings as per the standard requirements of dialysis.
The partner arranged for proper biomedical wastes collection as per Andhra Pradesh State Pollution Control Board norms and provided all the necessary infrastructure supports that are required. The disposal of the biomedical waste was arranged by the private partner.
Financial information.
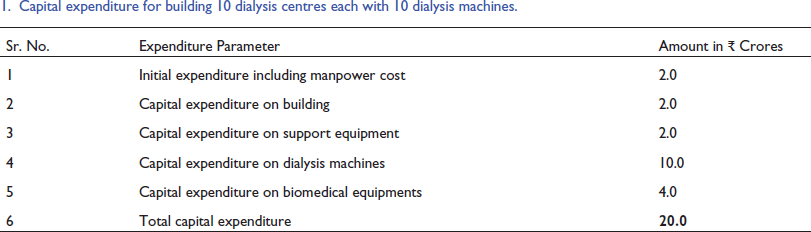
Capital expenditure for building 10 dialysis centres each with 10 dialysis machines.
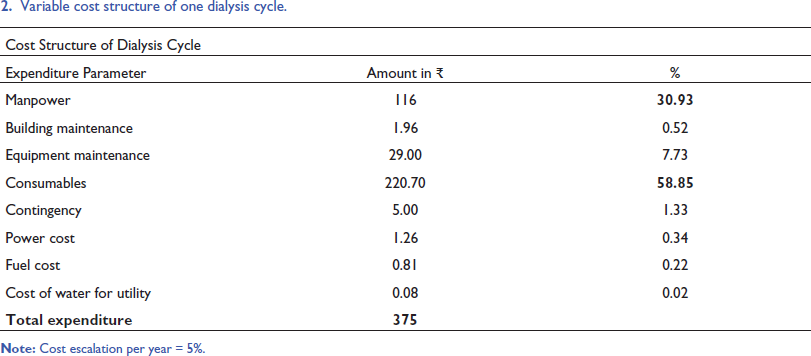
Variable cost structure of one dialysis cycle.
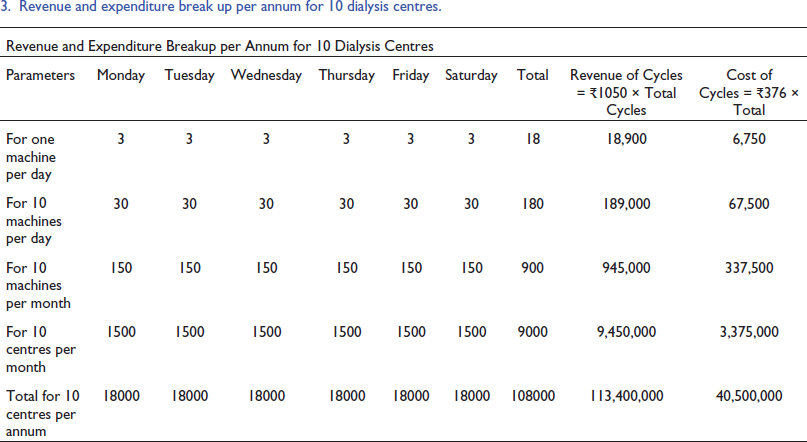
Revenue and expenditure break up per annum for 10 dialysis centres.
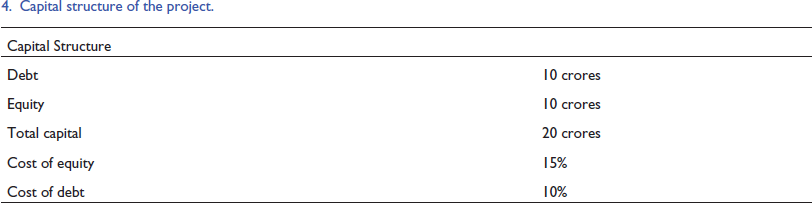
Capital structure of the project.
Income and expenditure statement of the project.
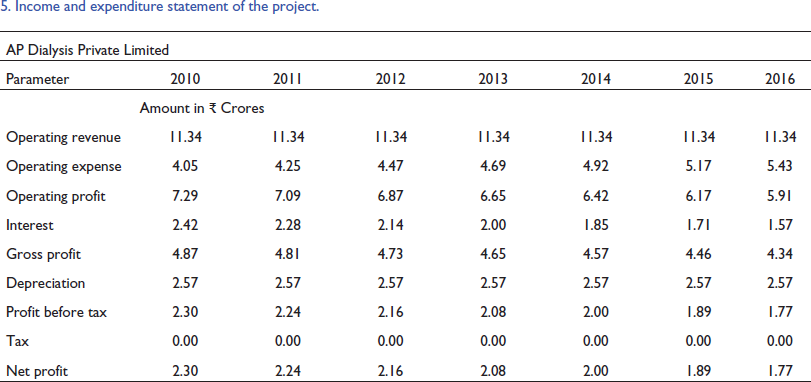
Exhibit 4. Pictures of Dialysis Centres.
The inside scene of dialysis centre.

The dialysis machine.

Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.