
Abstract
India’s medical service industry is an emerging force in Southeast Asia, which should be recognized. A large portion of the country’s GDP is being earned through this sector. Paradoxically, India’s rural sphere has always been highly deprived of medical facilities even in rudimentary level. This huge imbalance was previously an issue for India to reach to a footing through innovation. India still being a developing country has majority of people living in rural areas where quality healthcare is not only difficult to avail but sometimes even hard to access. In such circumstances, an initiative like Lifeline Express (LLE) has provided the people with access to quality healthcare which has been crucially needed. It is a very simple idea but incredibly complex in terms of execution throughout the whole region. The LLE is a hospital which moves throughout rural India in a form of a fully equipped train. Since 1991, this initiative in India has generated some commendable projects through which it has served many rural Indians. Through this case, it will be comprehensible of how the train and the medical team function and will show the limitations and challenges healthcare in India is facing and how LLE has proved its fantastic ability to fight with the constraints and make healthcare reach the doorsteps of the rural people. Despite the challenges and limitations, it is also been revealed how the journey of LLE has grown from a three-coach train to seven-coach train where patients get treatment of many diseases from the early 1990s to this day.
Introduction
A developing country has to face many obstacles, many challenges while serving the people within it. In the southern part of Asia—the country famous for its cultural variety, sports involvement—India is essentially facing several challenges in maintaining quality life standards all over the country. The people of India do face challenges in terms of economic well-being, safety, and most importantly proper healthcare. To improve the quality of healthcare it is important to meet the health-related targets of the Sustainable Development Goals. The main targets of quality healthcare are safe, effective, patient-oriented, timely and equitable (Deorari & Livesley, 2018). As a developing country, India is unable to ensure quality healthcare throughout the nation. Nevertheless, it is endeavouring relentlessly to become a nation where healthcare services reach to people all around the country.
Rural Healthcare in India
India is currently the world’s seventh largest country in terms of area and the second most populated country. With a population of approximately 1.3 billion, roughly 67% of the general public still resides in rural areas which amount to 871,000,000 people (World Population Review, 2019). There is a colossal difference in the quality of life between the urban and rural residents. Moreover, only 3% of doctors live in rural areas whereas 70% of India’s population lives in rural areas (Munjal, 2017). This is further clarified with official data that clearly states the doctor-to-patient ratio which is 1:11,082 people. The World Health Organization’s (WHO) recommended ratio is 1:1,000; thus exceeding 10 times more than what it should be. The National Health Profile in 2018 displays the states with the poorest doctor-population ratio: Bihar (1:28,391), Uttar Pradesh (1:19,962), Jharkhand (1:18,518), Madhya Pradesh (1:16,996), Chhattisgarh (1:15,916) and Karnataka (1:13,556) (The Financial Express, 2018a, b). One of the contributing factors is the largely differentiated healthcare systems present in these two areas. The urban healthcare system is so well established that India has become ‘one of the fastest growing medical tourism destinations in Asia’ with the projection to accomplish an industry worth USD 9 billion industry by the year 2020 (India Today, 2017). However, 871 million people living in roughly 638,000 villages are now struggling for rudimentary healthcare services. It is alarming to comprehend that 19% of the world’s population without access to water actually reside in the rural areas of India which exacerbate the condition of the people (Pandey & Sengupta, 2018). According to the National Health Profile (NHP) data, India spends an inconsequential amount (only 1.02%) of their GDP on health which depicts that such minimal expenditure is directly linked to the degradation of health care services (Dey, 2018). The public healthcare infrastructure is built on a three-tier system grounded on the population customs. The Seventh Five Year Plan (1985–1990) has given higher importance to Rural Healthcare. It included one sub-centre for a population of 5,000 and one Primary Health Centre as well as one Community Health Centre (CHC) for a population of 100,000. Health institutions such as Primary Health Centres (PHCs), 1 Subcentre, 2 CHCs, 3 Multipurpose Workers Scheme and Village Health Guide have been established in the rural healthcare system. India has a poor record in public health spending a little over 1% of GDP on public healthcare (Biswas, 2018). Consequently, the sector has been confronted with many challenges. Especially in rural areas, the inhabitants are the sufferers of poor healthcare service arrangement. The challenges in rural healthcare are manifold. India is facing the challenges in the form of limited awareness, inefficient physical infrastructure and insufficient human resources to serve the rural people and many more.
Awareness about Health Schemes
Although there have been multiple schemes put into place to support the rural residents, the regulatory body has lacked in publicizing its efforts. Most people in rural areas are not aware of the systems and arrangements set up for their benefit. A more market centred strategy will certainly help to create awareness in the general people. As rural people are already apprehensive about allopathic medications and are more comfortable with Ayurvedic or domestic remedies, the rural demographic requires more convincing compared to the urban population (The Hans India, 2016). If more promotion efforts are undertaken, perhaps the patients would be more inclined to visit the facilities constructed for them. This results in the under-utilization of the existing rural hospitals and amenities which has become a common phenomenon.
Physical Infrastructure
The physical infrastructure of the rural healthcare scenario has been elaborated earlier in this article. However, the problem with the establishments is that 91.5% of the CHCs, 78% of the PHCs and 49.7% of the sub-centres are situated in a derelict, run-down government buildings. In terms of the availability of the hospital beds, the situation is bleak as it only offers 149,690 beds spread across 6,795 hospitals. The basic requirements of the clinics are non-existent, for example, electricity was not present in 4% of PHCs while 7% of them did not have access to regular water supply (NRHM, Budget Briefs, 2014–2015). Additionally, the unsanitary conditions in hospitals are abysmal.
Human Resources and Medical Team
The deficit and insufficiency of medical professionals have immobilized the rural healthcare establishments. With a scant 3% doctors living in rural areas and 35% residing in semi-urban areas, a significant portion of the population suffers due to the unavailability of doctors. Unfortunately, there exist only 1 million doctors to give treatment to a population of 1.3 billion (Sharma, 2017). The difficulty does not end with the absence of medical professionals as the issues runs deeper. This is because four out of five doctors do not have the credentials to practice medicine. Patients also observe the absenteeism of the doctors and other medical staff. Lack of administrative action and unregulated practice by these ‘doctors’ steer towards ineffectual service delivery, resulting in fruitless service provisioning.
Preparedness to Fight NCDs in Rural Areas
Non-communicable diseases in India can be seen to be escalating especially in rural areas impacting the people’s health drastically. This is enormously challenging because NCDs are distressing a younger population where low awareness of the disease subsists and the facilities to combat it are not present. What is more is that medical professionals required to treat the patients do not practice in the rural areas and attempting to pay their hefty fees push them to poverty.
Neonatal Mortality Rate
UNICEF recently published its report on new-born mortality rate exhibiting that India is the 12th worst among the 52 lower-middle-income countries in this criterion. The report classified all the countries conferring to the number of deaths per 1,000 live births. Within 28 days of birth, annually 2,600,000 babies pass away, averaging 7,000 deaths every day. Among those, 640,000 deaths befall in India where the mortality rate is 25.4 deaths per 1,000 live births (Qrius, 2018). An in-depth analysis showed that the deaths can be attributed to premature birth, birth asphyxia, trauma, low weight, low nutrition of the mothers, and so on. Gender discrimination, being a socio-cultural factor, is prevalent in India and is also another reason for infant deaths (Jaysawal, 2015).
The Case: Lifeline Express
The constitution of India regards ‘right to life’ to be fundamental and holds the government responsible for ensuring ‘right to health’ with the means of ensuring proper healthcare to all of the habitants (Gupta & Bhatia, 2017). Consequently, medical solutions like Lifeline Express (LLE) are bound to be established. As mentioned in the beginning, LLE is the world’s first hospital train that travels all over rural India to bring free medical treatment to the neglected poor. The expedition of the venture began in the year 1991. Since its beginning, LLE is devoted to helping the poor in India to provide proper healthcare services. The venture realises the hardship the rural people have to go through to get healthcare services which are deliberated as a basic right to them. This is the 29th year of establishment of the train and till date, it is running strongly to make healthcare solutions available to the disadvantaged public.
Every journey to every rural destination is considered as a project. A project to deliver quality healthcare to those people of India who cannot access healthcare services easily. Each such journey is known as a project. Till 2018, the train has completed 199 projects (Railways News, 2019). The inspiring venture of LLE began with the simple dream to make healthcare services in the parts of the country where inhabitants find it hard to access healthcare.
Inception of LLE
One of the many challenges of healthcare in India is insufficient human resources. Especially in rural areas doctors and medical staff are unwilling to go because of the poor facilities. LLE is rather another solution to this problem. The initiation of LLE was shaped by collaboration between the Impact India Foundation (IIF), Health Ministry of India and the Indian Railways (IR). On 16 July 1991, the project initiated its journey and to date it is serving the people by means of various medical facilities. With the simple vision to make healthcare services available to the farthest corners of the country impact furthered the formation.
A number of 100,000 voluntary services from surgeons and medical personnel from across India and abroad have been helping to execute about 120 projects and served 600,000 Indians (Chatarjee, 2010). Currently, there are 20 permanent paramedic staffs along with many doctors volunteering from nearby medical colleges and hospitals of each project (Siddiqui & Kataria, 2018). The Chief Executive of the LLE reports to the Chief Executive Officer of IIF. The Chief Executive travels by the train, looks after the daily tasks and co-operates with all the collaborations. Apart from the seniors, there are also essential support staffs for maintenance and regular operational activities. Apart from the support staff, nothing is permanent in the train. The doctors’ change and equipment are upgraded (Gaikwad, 2016).
The impact was established in October 1983 as an International Initiative against Avoidable Disablement. It was promoted by the UNDP, UNICEF and WHO in association with the Governments of each participating country. IIF executes the function of a catalyst to carry together the Government, the corporate sector and existing NGOs in mass health programmes of India (Impact India, 2019). The Mumbai-based NGO—Impact India Foundation (IIF) proposed the idea of this project to IR and they signed a Memorandum of Understanding (MoU). According to the MoU signed, IR provided a three-coach train with required resources (such as water, electricity, and so on) to run the train and IIF took care of arranging the medical facilities. Starting 28 years ago, the train had only three coaches. Today it runs with four additional coaches making it seven coaches with advanced medical services (Pal, 2017). The hospital train has treated more than 1.2 million people establishing awareness and teaching the locals about health-related issues (Farret d’Astiès, 2019).
‘Bottom of the Pyramid’ in India: Healthcare Access through Lifeline Express
India is the second-most populous country in the world with 1.353 billion of population. Unlike countries such as China, India has not been able to overcome poverty with its majority of people (84 million poor in India, The New India Express, 2020). However, India did deduce its poverty line rate from 58% to 37% within 2011–2012 to 2017–2018 according to the World Bank. The difference between the rural and urban areas is still large enough for it not to afford and access to the basic healthcare line. As mentioned earlier, geography plays a part too in this when it comes to the accessibility. In terms of a commercial perspective, there has always been a hesitant tendency among the entrepreneurs to undertake gigantic initiatives to bring about any radical changes to uplift the living standards of these underprivileged people. The belief is that uplifting the poor was mostly of the domain of government or was simply too risky and hence, they lacked the insight and cost structures to reach poor consumers. However, the trend shifted towards investing at the bottom through the emergence of communication technological advancement. This measures up a more favourable operational spot for LLE and its services. The ‘bottom of the pyramid’ (Prahalad, 2012) in India in terms of possession of total wealth on average shows that around 770.7 million adults own less than US$10,000 whereas only 760 people own more than a US$100 million (Credit Suisse Global Health Report, 2017). Now, for these people to even have the appropriate access is a matter of strategy. It is a common thing for people in developing countries to usually lack access more than the developed ones. The WHO Constitution (1946) states that ‘…the highest attainable standard of health as a fundamental right of every human being’. That is why access to healthcare should be regarded as a basic societal right (Culyer, 1995). This concept arrives only if the relevant hindrances to avail the service are uplifted. Making the service available is easier than paving the way to access for people living under the poverty line, economically speaking and for people living in the dispersed area, geographically speaking.
Operation of Its Congenial Service
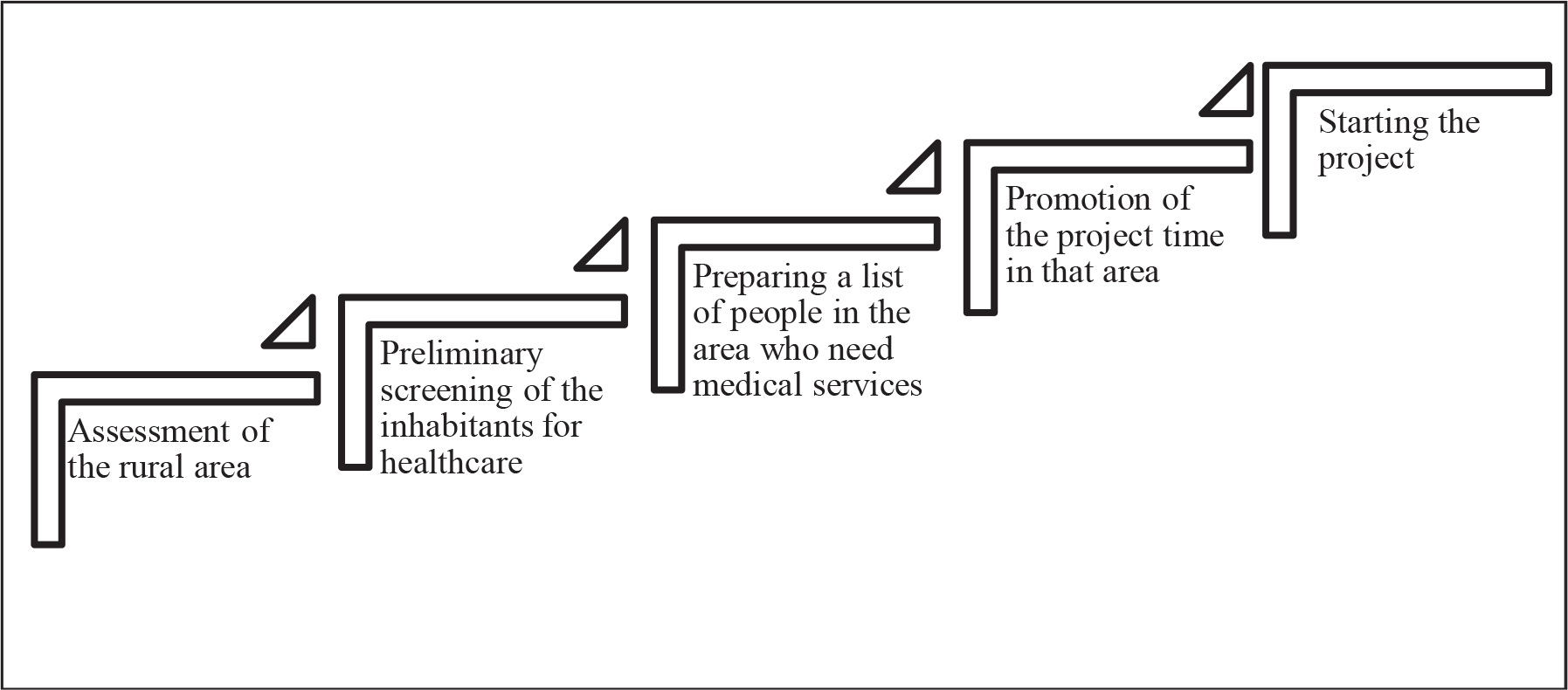
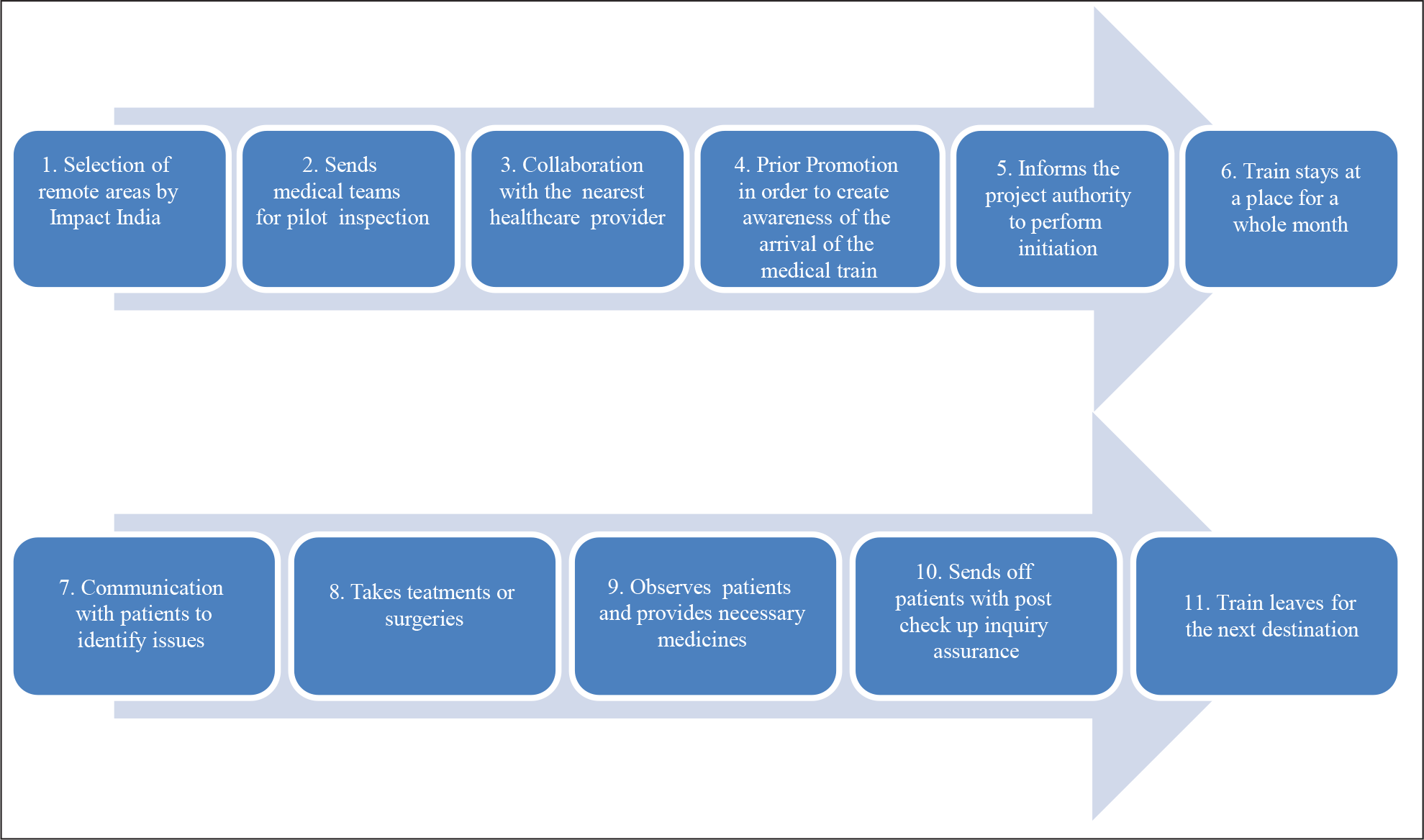
The concept of LLE initiated with a simple inspiration—to serve the unserved, needy segment of the population through reaching out to them. Before the arrival of the train in any particular location—a medical team visits the area to scrutinize health data, available healthcare facilities and vital health indicators. Following the pilot inspection, the team of LLE would collaborate with the local primary health centre or community health centre to prepare a list of people living in that area who need medical services (Pal, 2017). About the location of every project, Impact India has made one condition to be fulfilled—the location has to be remote enough where medical services are not available and accessible (Impact India Foundation, 2019). The medical facilities conducted in the trains include a whole host of services, starting from different kinds of ophthalmological surgeries to dedicated cancer treatments now. The train (as shown in Figure 1) parks for one month at a selected location where patients are treated for orthopaedic, hearing and visual impairments, cleft lips, and more recently for epilepsy, neurological and cardiac disorders, dental and gynaecological problems—most of which are pre-screened in the nearest local hospital. The train has made a health impact both in India, as well as around the world where it has inspired similar initiatives (Indiatimes, 2018; Pal, 2017). The train smoothly camps in different parts of India to conduct medical projects. The projects offer a free consultation, treatment and surgeries in various specialities. The seven-coach train has three operating theatres which are set with advanced medical apparatus (Ra, 2019). The coaches are instilled with air conditioners so that the patient and staff working in it do not suffer. Wi-Fi service is also available for better communication. The coaches have operation theatres, pathology lab, mammography unit, gynaecology examination room, dental unit, X-ray unit, pharmacy, consultation cubicles, numerous patient wards, onboard power generators, a well-equipped pantry (Figure 2) and lodging for medical staff (Pal, 2017). Each project presents an enormous and multifarious exercise in planning, meticulous coordination and action by various bodies. Usually, the following are involved: the sponsor who may be an Indian business entity, foundation, institution, or the State/Central Government; the Government’s Ministry of Health & Family Welfare, Social Welfare, and through them, the various local, State and Central Government agencies working in the rural areas; the IR, for coordinating the movement of the train, parking facilities at sidings along with provision for water, electricity and levelling land at the siding, NGOs to take care of the minute, local details at the site create awareness about LLE as well as mobilize volunteers, medical and para-medical professionals, who provide their services and expertise on a voluntary basis, mass media to help create public awareness and finally, the beneficiaries for whom this entire exercise is targeted (Impact India Foundation, 2009). Figure 3 gives a snapshot of the steps of operation process in every project of LLE.


Availability of the Medical Consultancy and Service
Medical facilities should be in close proximity of its recipients (Peters et al., 2008), with rural areas suffering the most in terms of availability of medical facilities. LLE is indeed a way out to this challenge. Availability is not enough if the value and norm of the provided service are not accepted by the people of the rural areas. For primary healthcare to reach the greatest number of homes, it must be in line with the prevailing local cultural norms (Declaration of Alma-Ata, 1978). In developing countries, some people even try to be in ignorance their prescribed medical attention if there is a slight bit of possibility for modern medicines to bring up any cultural questions or concerns. Some perceive the modern medicines to be contradictory to their belief in medicine. Previously in India, it was not a matter of concern as basic healthcare was provided and people were accepting it since it is, of course, the basic need they require or imminent death as another alternative. Later on, as more complex, the equipment got installed and the more tangled the medicines had become, it became a concern to do a thorough investigation prior to every project to meet the social will of the people. As a result, more people are started making use of these services. Acceptance of surgical processes such as plastic surgery became frequent due to its cultural bias towards facial perfection for a marital purpose. Understanding the societal norms helped shape the service projects swifter.
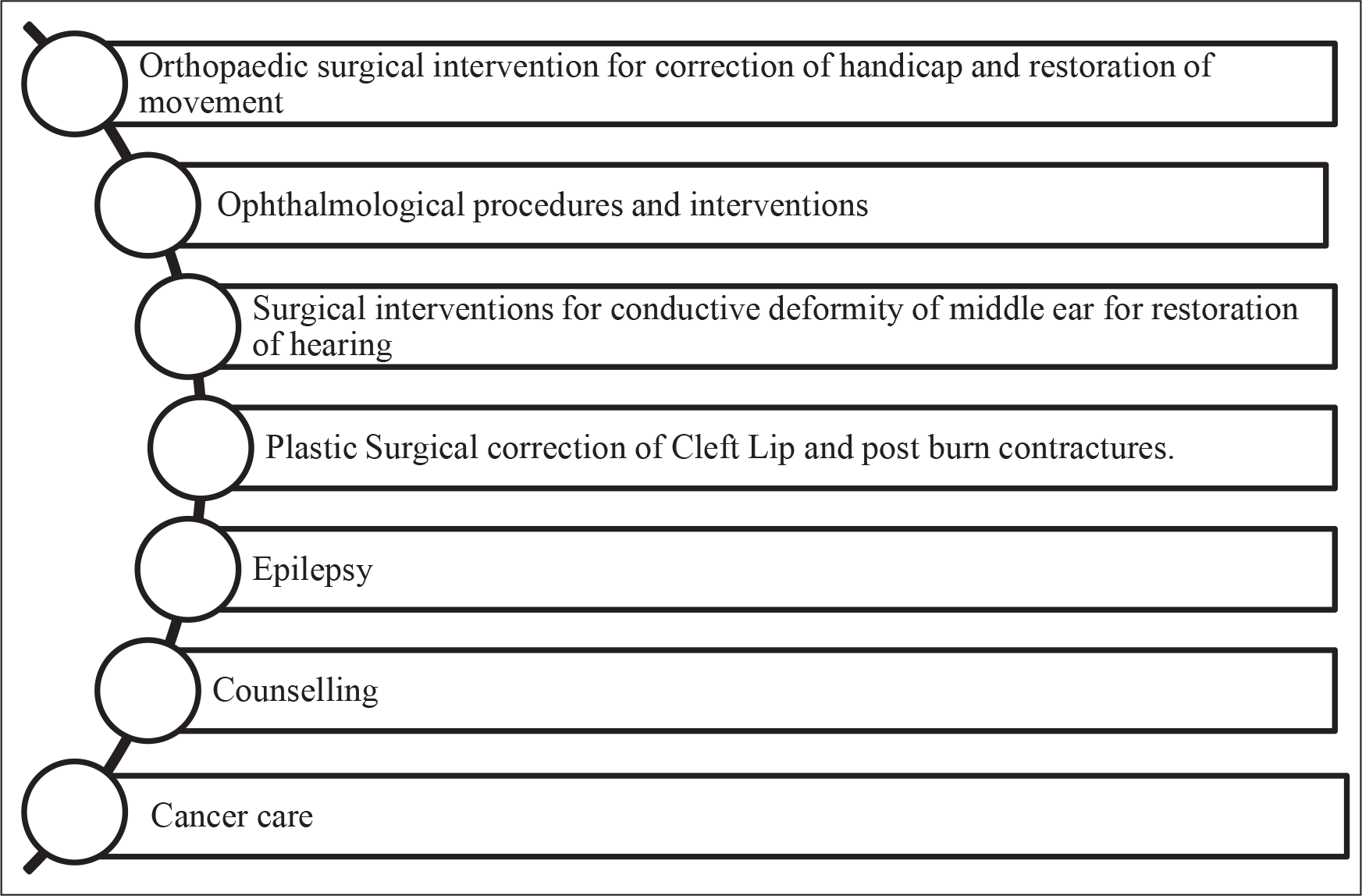
The LLE offers services like repair of sight through cataract operations, correction of clefts through surgery, dental services. Additionally, it teaches surgeons, working in smaller towns to acquire expertise in the finer skills of micro-surgery (The Economic Times, 2014). Starting from those facilities today LLE has endeavoured to give treatments to patients with cancer. In its project, to remote Tripura, the train has treated 900 cancer victims and 900 dental patients in December 2018 (The Financial Express, 2019). It has several medical supplies, pathology lab, mammography unit, orthopaedic surgery, neurological treatment unit, dental facilities, an X-ray machine, pharmacy, consultation cubicles and lodging for medical staff. The surgeons and doctors on board continue to handle a large number of medical conditions including epilepsy, cataract, cancer, cleft lips, polio, plastic surgeries, dental and oral surgeries, burns and disabilities and disorders of the eye, ear, nose and limbs (Nath, 2019). Figure 4 illustrates the list of medical services the train is providing so far.
The LLE has been regarded as ‘A Surgeon’s Dream’ as it provides the medical personnel with the modern functionalities to serve the needy people (Impact India, 2019). The staff compartment of this LLE train consists of 12 berth staff-quarter, kitchen unit, water purifier, gas stove, electric oven and refrigerator (Vikaspedia, 2019). These available resources certainly make the exertion of the staff and volunteers of LLE easy. With the upgrading facilities and an increasing number of available facilities, it can be expected that the performance outcome of the magic Train will be the light of hope for rural India.
Apprehension of Healthcare and Beyond
The rural people who are often deprived of their fundamental medical needs are not even properly aware of important health issues. For example, sufficient knowledge of breastfeeding practice was found in only one-third of the pregnant females in two studies (De et al., 2016; Pandey et al., 2015). The country is in compelling need of proper health education for the rural people.
The model of LLE functions on a public–private partnership (PPP). Each project is sponsored by a private organization. Impact India has only one condition for the private sponsor regarding each project—the location of each project should be in a comparatively isolated region. As a result, those who genuinely need medical care would be able to receive it. A preparation period of 6 months is run before the train arrives. Firstly, a proper study is conducted of the area and then an awareness campaign is built up to reach out the residents of that region so that they know the train is arriving at their region and its itinerary. For example, before the train arrives at its selected destination a medical team visits the area to assess the health requirements, work with vital data and supervise existing facilities. This functioning process helps local doctors and medical staff to acquire adequate knowledge (Chatterjee, 2010; Pal, 2017). LLE also aims to inform the locals about the proper approach to healthcare (Dey, 2018). This act shows how the project believes that prevention is better than cure—that proper learning on health and wellbeing would help the people to maintain fine physical condition and build a healthy future generation. Often local journalists are engaged in the preparation stage to raise awareness; leaflets are distributed through health workers to reach more inhabitants (Chatterjee, 2010). Currently, their ongoing and upcoming projects include the G. V. Meditech Ltd., which is high quality and cost-efficient healthcare to people in Uttar Pradesh from Varanasi, secondly, one of the fastest-growing hospital chains is the CARE hospitals, which provide both primary and tertiary healthcare services, then Amrita Institute of Medical Science (AIMS), Deepalaya—Community Health Program and Health point Service India (HSI), they are responsible for providing lots of other medical fees including clean drinking safe water, medicines, diagnostic tools and consultancy.
Cost Efficiency of Lifeline Service
Private health sectors are excruciatingly hard to afford and to access for rural people. Due to a large number of people with the low average income in most of the developing countries, cash-flow can be, and it is a significant issue in attaining proper healthcare considering how to experience these services are beyond the reach of impoverished families (Anderson & Billou, 2007). Bearing the basic medical cost is near to impossible for these poor people to afford let alone travelling to the nearest private medical institution. It is even costlier if the rural people required any complex form of medical services such as cardiac operations, dental and sight restoration and so on. The relief is that LLE comes free of cost. ‘The train, which is the flagship of Impact India Foundation, in partnership with the Indian Railways, has medically served more than 10,00,000 poor in rural India, restoring sight, movement, hearing and correction of cleft lips with dental and neurological treatment and more, completely free of cost’ (2011–2016, Impact India Foundation). This free of cost initiative, of course, raises a question of the quality provided. ‘However, there is generally a strong correlation between the quality of service received and the price paid for receiving it, and compromising with quality increases the likelihood of unsafe care’. The similar kinds of services such as the Friendship Floating Hospitals in Bangladesh raised the same issue (Ahmed et al., 2015, 2019). However, the LLE, with the help of hundreds of donors, medical personnel, partners and well-wishers around the world, was able to leave no stone unturned in maintaining the quality of the service for both the patients and the on-track learning young surgeons. There are also plastic surgery services which are rendered to people who are unfortunate with facial scars, marks and deformity, which have damaged their social existence. These surgeons are expert and can even do surgeries on older people with utmost expertise of which on contrary, would have been risky and costly.
With the resulting success of LLE, IIF is now planning further to develop strategies to resolve the pressing issues in developing India. They have inaugurated Cancer diagnosis in the train and are teaching the rural population regarding diagnosis, prevention and timely treatment of the disease. Also, the train is dedicated to making the rural population aware of the importance of family planning, enabling birth control (Impact India Foundation, 2018).
Strategic Approach: Mobilization in HealthCare in India
The railway medical service may not be the one-stop solution to the massive population dispersed in remote geographical areas but it has certainly been stimulating the medical service to be mobilized. ‘Being mobile, it could benefit many provinces and there were some important health issues it could address’, stated by Fong (1997), a Hong Kong-based legislator and a healthcare activist when she first heard the notion of a hospital train in India. Mobilization of Healthcare service created a bridge between a massive portion of the population who were previously denied of medical service and the healthcare organization itself. A strategic management move was bound to be deployed since India’s large areas were deprived of medical attention both in rudimentary cases and critical ones. The initiative of LLE, therefore, introduced this strategy and became a trendsetter in the world almost two decades ago. However, due to some major drawbacks of such a project, it could not make any ginormous difference in the medical arena in India’s rural domain.
The operational mobility service model of LLE here shows (see Figure 5) that there are still some management loopholes. This is the reason as to why this project has not yet provided the expected geographic coverage that it was supposed to. The communication procedure sometimes takes weeks to initiate a project to a particular destination. However, prior to LLE, there were no physical methods which were pliable enough to provide any sort of medical service to those distances ever before.
Setbacks and Challenges
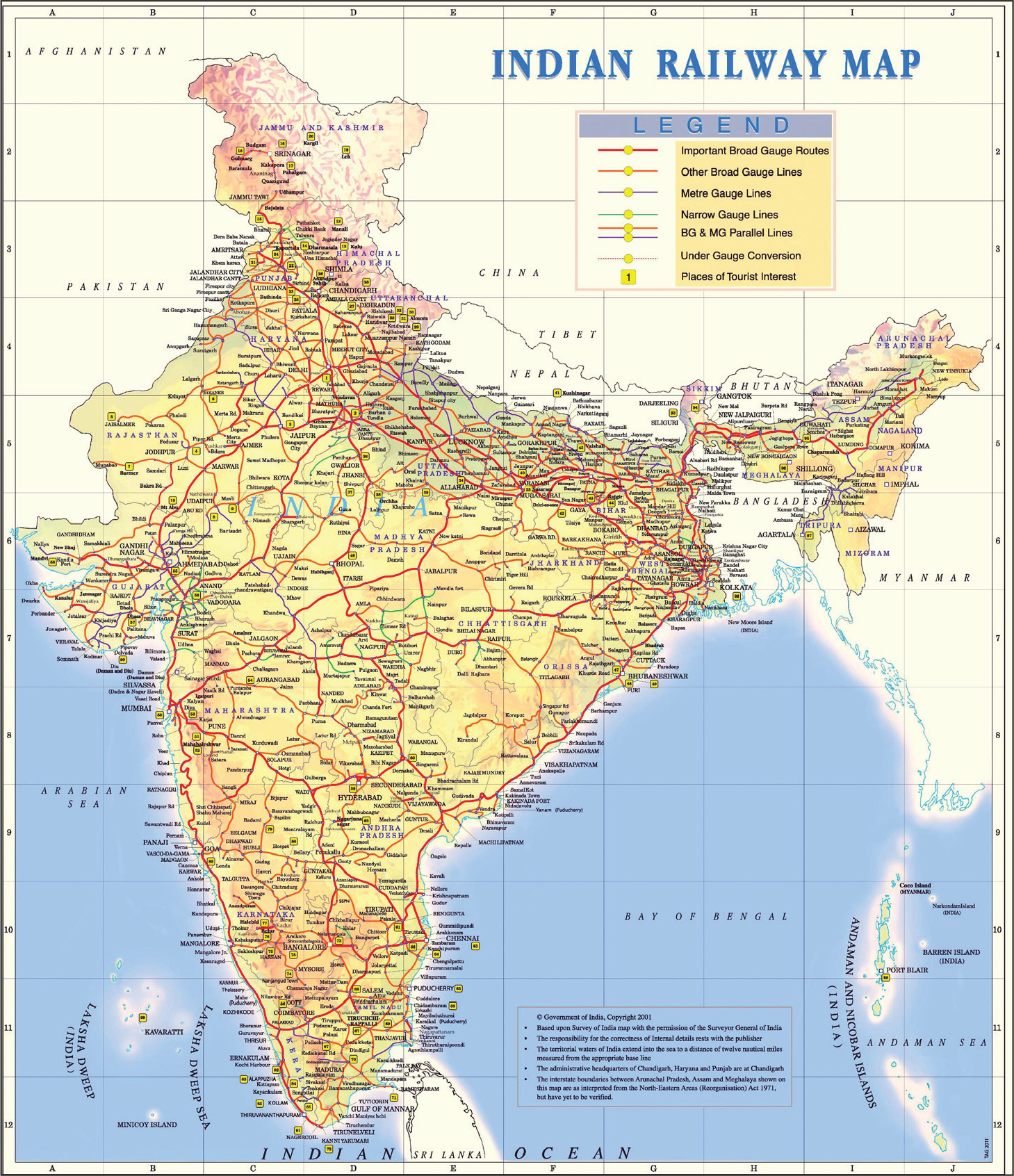
As of this point, it is clear that in India, the public healthcare system is undergoing a state of affairs where it is acutely underserved. As a result, the general people are prone towards or in other words left for the private sector to serve. Evidently, the expenses of private healthcare services are not affordable for rural people considering their economic state (Somvanshi, 2018). The citizens who have the economic ability to avail private healthcare, they are not bothered about it. In the real picture, the majority of the population is actually suffering due to lack of proper healthcare. To add to this, one of the concerning issues for public healthcare is access to healthcare services. Approachability to hospitals and medical centres is hard for people living in rural areas. The basic consideration of access to healthcare could be determined by the physical reach of the healthcare facility (Kasthuri, 2018). Conversely, the spatial inequalities are affecting the rural population in terms of their healthcare and well-being which remains deficient in quality (Krishna & Ananthpur, 2013). In an instance like this, initiatives of LLE are essential for this country. Nonetheless, the question here is about the railway lines throughout India. Is LLE prepared to thoroughly reach through the railway lines of India? Figure 6 shows a detailed Indian railway map. According to Nath (2019), the train has treated more than one million and has performed surgery on more than 100,000 people. It has fulfilled social welfare aspirations by providing doorstep medical assistance to the people residing in rural India by leveraging the route length of more than 67,000 km of India’s vast railway network. However, one of the challenges would be to reach the places where the general people do not have access to railway transportation. How will LLE serve that part of the population?
Currently, the world faces one of the biggest pandemic caused by deadly COVID-19. This can be addressed as one of the most substantial challenges that LLE will ever face. India itself had faced the biggest lockdown in the world and the impacts are enormous. ‘The Indian capital, home of 20 million people, simultaneously recorded its highest single-day cases on 17th September, with more than 10,18,454 cases according to the recent most Worldometers Info while local government data showed that of the roughly 13,400 beds allocated to COVID-19 patients in the city, around 6,200 were occupied’ (tbsnews.net, 1 June 2020). From the end of August 2020 to the midway of September 2020, the number of cases soared high daily on a subsequent manner with daily added cases near to almost a hundred thousand and no less than fifty thousand. This led to a total number of around 7 million cases and still rising. Although the weight of the recovered cases precedes the volume of death rate, the ratio is somewhat as a 6 million with a hundred thousand, but the current status us still worsening even as we speak. The data totally indicates that there will be a shortage of beds in hospitals in the city. In continuation of the massive spread of this uncontrolled virus will surely create a shortage of beds in hospitals throughout the whole nation. A result of such mismanagement has given birth to two thousand deaths in one single day, which is so far recorded the highest death cases recorded in India on 16 June, making India the second top country with the highest number of COVID-19 cases right after the USA (Worldometers.info Coronavirus Update, 22 October 2020). As most of the countries are struggling to control the wrath of this virus and not succeeding on a larger scale but still finding a way to fight against it, India is doing the same. Apparently, India has taken the initiatives to serve the patients by increasing the beds and adding more ventilators to the hospitals. Since the outbreak, the ministry declared for every railway to stop usual transportation and get prepared to make its wards ready for treating COVID-19 victims (KPMG India, 2020). However, the aim is to reach 20,000 coaches of which 5,000 have already been deployed to counter the pandemic. These coaches have around 80,000 beds. ‘The idea of converting these coaches was to ensure that in rural areas, in regions where medical facilities were not available, care for COVID-19 patients could be provided. The health ministry has decided to guide us, and we will deploy these trains. We will maintain them and make sure they are in good condition’, an official said (The Economic Times, 2020). As per government’s attempt, ‘Indian Railways converts coach into COVID-19 isolation ward’ (The Indian Express, 2020). The idea is quite similar to one of the Lifeline’s main agendas which are using the train to serve the affected people in remote areas. To add with it, ‘We have converted a non-AC coach with all necessary modifications. These can travel to remote locations of India if needed and be in service in India’s fight against Coronavirus’, Arun Arora, Principal Chief Mechanical Engineer, Northern Railway told The Indian Express. Nevertheless, there are issues of maintaining hygiene, the air-conditioning compartments require daily and regular cleaning facilities, and the toilets and equipment need frequent care as well. Most importantly, LLE will have to come up with a feasible solution to this issue soon to support the government as well as the people of India or otherwise it will be too late.
Moving Forward
LLE is also known as ‘The Magical Train’ because of its remarkable success in providing medical services in remote areas where formerly it seemed impossible to get healthcare. The Magic Train of India has certainly created an outstanding example for the world to watch. Following its success, other countries have also created their own wonders for medical advances. Starting with only three coaches now the train has a total of seven coaches serving a variety of medical treatments. Since the train is reaching the unreachable areas with excellent healthcare. Since 1991, there have been few other countries who have also undertaken such projects through railways. To exemplify, China in 1997, came up with a rainbow painted train called ‘Eye Train’ which provided cataract surgery and later on introduced more train lines to cater to medical facilities. There are also the Phelophepa trains in South Africa which provide general health, dental and eye checks, visiting up to 70 remote rural communities annually. Two more trains traverse the Russian Federation, one of which is the Saint Lukas train, which travels through the vast regions of Krasnoyarsk and Khakassia for 10 months every year (WHO, 2020). None of these trains originated as government-funded programs, all were established as philanthropic or corporate initiatives. However, one thing is for sure, India over the last three decades have redesigned, developed and refurnished the LLE in every aspect and being the first mover in this sector, Lifeline Express certainly deserves a global recognition especially if India wants to tackle its situation in a dire time like now with the COVID-19 outbreak!