
Abstract
On a hot summer afternoon, there is a huge commotion around the Jawnpore District Hospital. There is passionate sloganeering by the ruling party supporters competing with protests by the opposition party activists against the alleged lack of personnel and infrastructure in the district hospital. Not far away from this hullabaloo, Grameen Arogya, a non-governmental organization, stages a satyagraha to silently protest against the official silence on dysentery deaths in the region. A motorcade of government cars enters the hospital grounds. The local leaders of the ruling party and the District Hospital Superintendent are waiting to welcome and garland Shri Jagatprakash Goel, Union Health Minister, visiting the hospital. Goel ji joins the doctors in their regular ward rounds and inspects the hospital. Then he addresses the public and the medical community including a few office bearers of the medical association (the association of registered doctors). The moment Goel ji concludes the address, Mr Das from Grameen Arogya, rushes to the podium and hands a memorandum to Goel ji. He grabs the microphone and makes an emotional account of the deplorable healthcare situation in Jawnpore. He discusses the difficulties arising due to a lack of registered doctors and rampant absenteeism in the public hospital, particularly when there is no private provider of healthcare. He proposes that the only practical way to alleviate these difficulties in providing rural healthcare is to ‘mainstream the quacks’ and cites a 2006 multi-national survey-based research study (Chaudhury et al., 2006). He appeals to Shri Jagatprakash Goel, the minister, to make provision for special training of informal providers (Ips), to fill the need for medical practitioners in rural areas. Supporters of the ruling party and members of the medical community run to the dais to stop Mr Das from speaking further. But the minister asks the crowd to calm down and handles the situation. He assures Grameen Arogya that he will investigate the issue.
THE ROUNDTABLE
Goel ji, back in the capital, asks his ministry to organize a policy roundtable to make an informed assessment of the situation. The organizers invite a wide range of stakeholders, including the WHO Country Chief, National Medical Association (NMA) representatives, patient forums, NGO representatives working in the health sector among others to the forum. Shyama, a health economist whose research focuses on health equity, makes an opening presentation on the situation of formal healthcare and the dependence on informal providers (Ips) in the country. She elaborates on findings from a recent study relevant to the current issue.
The findings draw from the unique patient audit study that was conducted as a census of all providers in the healthcare market that catered to sampled villages in a representative sample for the state of Madhya Pradesh. It is found that 46% of all providers and 70% of all private providers were Ips without formal medical training. These Ips account for 77% of household visits. The Ips remain the dominant providers of care in most settings, accounting for 74% of all visits even when a public provider is in the same market. They account for 60% of visits even when an MBBS doctor is in the same market. MBBS doctors account for only 4% of all patient interactions. Even public facilities have many unqualified providers. While these support staff are supposed to assist a qualified doctor, it is quite common for them to act as the primary healthcare providers in public clinics and prescribe medication given high doctor absence rates (Das et al., 2016). Earlier in 2012, a set of paid actors were trained and sent as patients to health providers practising in the city of Delhi (n = 64) and select villages of Madhya Pradesh (n = 241) as a part of a similar patient audit study. They were trained to behave as patients with unstable chest pain, asthma, or a father of a child at home with dysentery. About 250 such unannounced visits by decoy patients to different clinics were conducted. They were treated as ‘real’ patients by healthcare providers. In both Delhi and rural MP, there were minor differences between trained doctors and informal providers in areas such as adherence to clinical checklists and no differences in the likelihood of providers giving a diagnosis or correct treatment. The quality of care provided by doctors, irrespective of their training, was found to be poor when measured for parameters such as accurate diagnosis, appropriate treatment, time spent and adherence to checklists of essential and recommended care. The average consultation time for all providers was as low as 5.3 minutes. The rate of correct diagnosis and treatment was just 21.8% and 45.6%, respectively (Das et al., 2012).
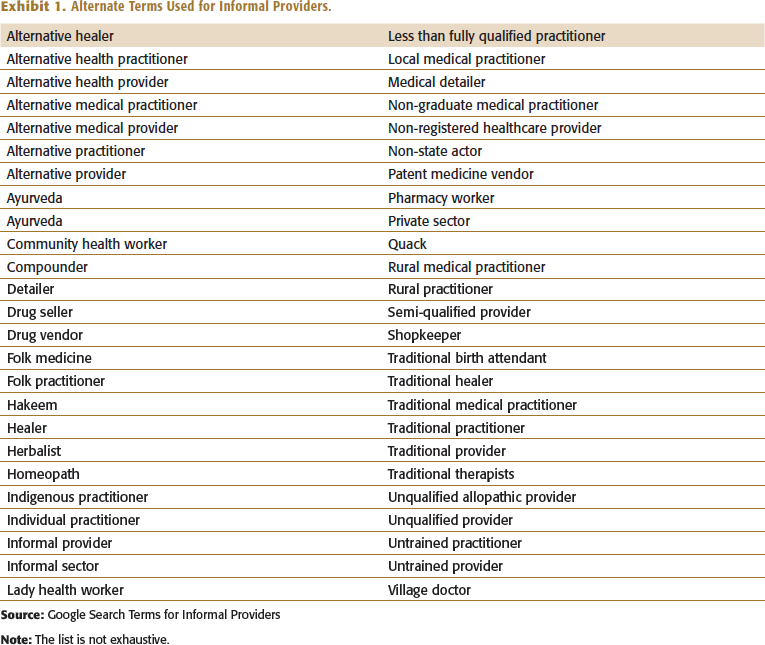
An independent researcher observes that it is hard to distinguish between a trained provider and an informal provider in large parts of rural India, urban slums and lower middle-class localities. But there is a question, ‘who is this informal provider?’ Shyama fast-forwards her presentation to a slide with a table which lists all possible alternate terms used for informal providers (Ips) slides (Exhibit No.1). She clarifies that the term ‘informal providers’ would serve as an umbrella term for a heterogeneous group of providers with differences in the type of training, regulatory frameworks, and services provided (Sudhinaraset et al., 2013). The Ips would refer to doctors without a registered medical degree (MBBS and its equivalents or an AYUSH degree). Thus, they would refer to practitioners without a legitimate license to practice.
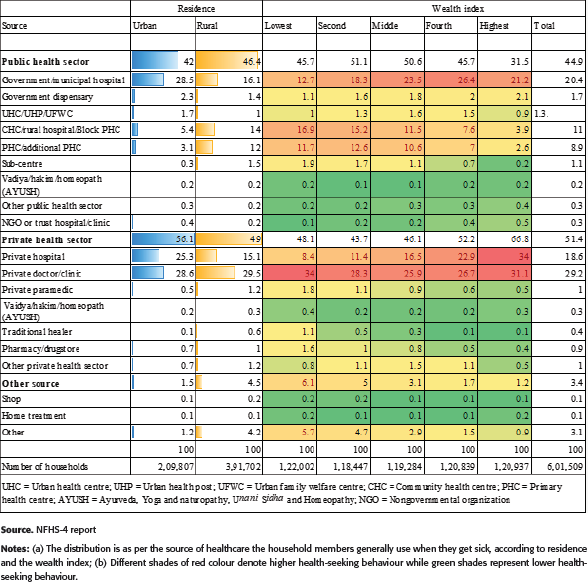
Alternate Terms Used for Informal Providers.
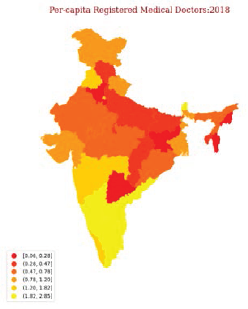
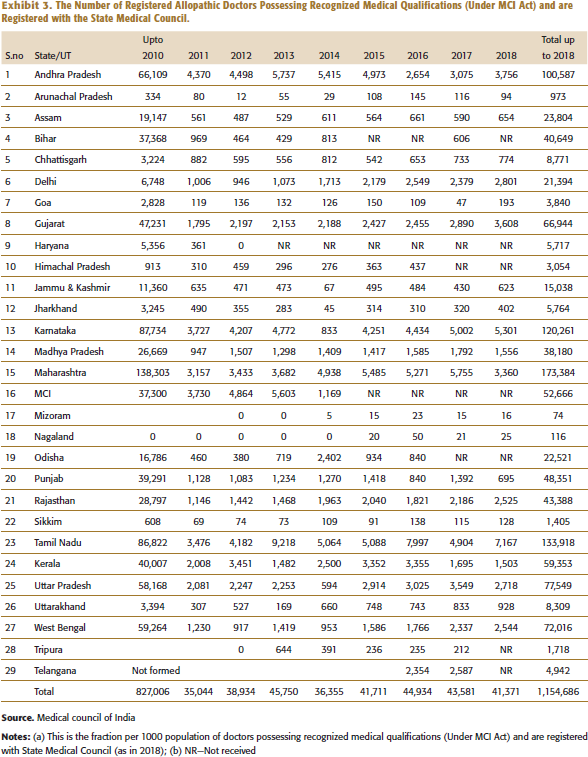
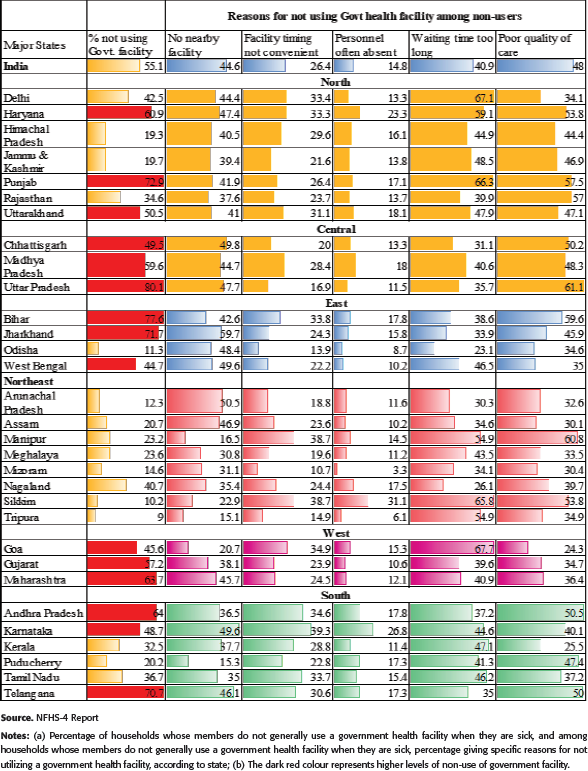
Shyama shows a choropleth map and a data table to describe the state-wise distribution of the number of registered allopathic doctors, registered dental surgeons, and AYUSH doctors who have recognized medical qualifications (Exhibits 2 to 3). States with poor health, such as Bihar, Madhya Pradesh, Rajasthan, and Uttar Pradesh, have 36% of the country’s population but only 15% of the medical colleges. Private medical colleges dominate, accounting for 65% of medical schools in the five south-western states and 50% of medical schools in the four states with poor health. Despite the increase in medical schools and graduates, medical students from public and private medical colleges are not attracted to employment in rural areas or the public sector. High capitation and tuition fees for medical education mean that students are more likely to seek employment in the private sector, where they can earn more money (Rao et al., 2011). She also points to the inequities in healthcare across socio-economic categories and lists out the various reasons for not visiting a government health facility (see Exhibits 4 and 5). Next, the delegates from Medical Association dwell at length on quackery, and problems associated with informal providers in the Indian health sector. They list out statistics on the numerous cases in which quacks were arrested following the death of patients being treating. The NGOs object to the use of the term ‘quacks’ for informal providers. Without a clear path forward, the Roundtable closes. Shyama re-emphasizes the concerns faced by the citizens and the different perspectives of each stakeholder. Goel ji thanks everyone for their input and requests for another Roundtable meeting in the next quarter in a continued attempt to find a way forward.
THE UNREPRESENTED
After the wrap-up of the Roundtable, Shyama wants to get views of the unrepresented. She contacted her former student Sonam who was working on her field project on healthcare access in rural Madhya Pradesh. Briefed by Shyama, Sonam visits a Bangali Daktar (an informal provider in the local parlance).
There is huge prevalence of Cholera in summer due to unhygienic food options. In a nearby village, about 100 people got infected with Cholera recently. There was no facility in the nearby government hospital to treat it. Two of the patients came for my treatment, and slowly then, more started coming in. A boy who was taken to the government hospital was brought to me. I could not save him. But I could save 22 other lives.
BD: I got my medicines from nearby town and I was administering 10–42 bottles each day. I did not demand any money from the patients. They were expected only to spend on their medicines.
MAINSTREAMING
Shyama listens to the audio file of the interview with the Bangali Daktar and is satisfied that she has the views of at least one IP. She continues following the debate in the academic literature. She finds reports that there are around 1.6 million private IPs all over India providing essential doorstep health services to millions of rural households.
The patient audit studies unveil the unsettling finding that there is no difference in quality and correctness of diagnosis between formal (MBBS doctors in public clinics) and informal providers (unqualified practitioners in private clinics). Das et al. (2016) attributes this phenomenon to the higher effort exerted by the majority of IPs vis-à-vis the public providers. IPs performed no worse on diagnosis and treatment compared to their formal counterparts. The doctors who had dual practice (a qualified medical doctor practices both in public sector clinic and in their private clinic) were found to have spent more time with patients. They were more likely to offer correct treatment in their private practices than in their public practice. Even though informal providers exert higher effort, they are rendered less effective by their low level of medical knowledge, as they do not have any formal medical qualifications. On the other hand, public sector clinics that are supposed to be staffed by qualified providers have lower provider effort. Vacant posts and frequent absenteeism of qualified medical personnel imply that even in a public sector clinic, the patient often sees a provider without formal training (a helper or a health worker who steps in as the one who diagnoses and prescribes treatment). She gathers substantial evidence from several studies that the majority of private providers in rural areas (whom most of the villagers refer to us as a private doctor or village doctor) are informal service providers (Chowdhury et al., 2016; De Costa & Diwan, 2007; Dror et al., 2011; Gautham et al., 2014).
Shyama is aware that Section 15.2(b) of the Indian Medical Council (IMC) Act, 1965 makes it illegal for anyone without a university medical qualification to practice modern medicine. But legal prohibitions have not prevented IPs from operating freely in rural area as there are not enough alternatives for the healthcare seeker. The common understanding in the policy circles of Bihar, Madhya Pradesh, Rajasthan and Uttar Pradesh is that the first provider of rural healthcare will shut-down without any alternatives if IPs are banned from practice. The harsh realities of little formal rural healthcare, combined with the unwavering support for IPs among the local communities, make it difficult for the system to put them behind bars. Shyama finds that the registered medical doctors’ guilds are going overboard with their highly aggressive stand concerning IPs, given that there is hardly any interest among the registered medical doctors to work in these belts.
As Shyama sees no significant break in the impasse between poor health outcomes, lack of formal care and the existence of the IPs to fill the healthcare gap, she stumbles upon a unique randomized control study on IPs. The study evaluates the effects of the training of IPs in the state of West Bengal where they underwent a rigorous, a multi-topic training program spanning 72 sessions of training over nine months to attend to the basic healthcare needs of people. The Liver Foundation, a public health organization based in West Bengal, designed and executed the training program. The organization invited 360 providers across its district of operation to participate, out of whom 304 providers expressed interest and were randomized equally into training and control groups. Members of the training group were admitted to the Liver Foundation Rural Health Care Practitioner Training Programme. The efficacy of the training programme was measured using visits by unannounced standardized patients (‘decoy patients’) along with the aforementioned randomized controlled trial design. Despite a mean attendance rate of 5 in the foundations’ training program, trained IPs managed more cases accurately, and successfully closed half the gap with public sector doctors. IPs who completed the entire training course accurately managed cases, often at par with public-sector doctors. However, the training had no impact on the avoidance of unnecessary antibiotics. Moreover, training did not lead informal providers to violate rules with greater frequency or worsen their clinical practice, which were the major allegations of Medical Associations against IPs (Chowdhury et al., 2016).
This study shows that medical training may be a good short-run strategy to utilize the potential of IPs for meeting the unmet healthcare needs in the rural sector. Taking cue from the study, the state governments of Andhra Pradesh, West Bengal, and Bihar started initiatives for training IPs as community paramedics. Informal providers have also been engaged in many successful public health initiatives such as United Nations International Children’s Emergency Fund’s (UNICEF) Social Mobilization Network, in primary healthcare programs such as in reaching out to tuberculosis patients and reporting epidemics. Steps to include them in the screening for non-communicable diseases and in doing systematic triage and referrals have already been initiated. They are being trained to manage emergencies as first responders. Such training programmes are also being used to sensitize the informal providers about the high levels of resistance to common antibiotics among the Indian population, resulting from unregulated sales and promotion of antibiotics by the pharma companies through informal providers.
The Number of Registered Allopathic Doctors Possessing Recognized Medical Qualifications (Under MCI Act) and are Registered with the State Medical Council.
EPILOGUE: DIGITAL PLATFORM
Shyama moots a plan for a possible digital platform targeting all rural health workers and aiding the delivery of primary healthcare services and products. The proposed digital platform plans to train and certify the local healthcare worker’s knowledge of fundamentals and operational aspects of primary care, diagnosis and pharmacy. It would also regularly update them on the advances in technology, new drugs and new diseases. Before ideating on such an interface, she surveys the recent ventures in the rural health space
One of the first health ventures targeting the hinterland, e-Health Points units started in 2009. It aimed to provide families in villages with clean drinking water, medicines, comprehensive diagnostic tools, and advanced telemedical services that ‘bring’ a doctor and modern, evidence-based healthcare to their community (Hamermesh et al., 2011). Indura was created by the leading Indian pharmaceutical company, Dr Reddy’s Laboratories (DRL), as a business unit dedicated to the rural market. This strategic decision resulted from the shift in the corporate strategy to focus on the domestic market and rural areas, translating the new ‘Health for All’ vision of the incoming CEO. But the plan met with numerous implementation hurdles (Dhanaraj et al., 2015). However, such implementation hurdles are not rural-specific. This is evident when we look at the experiences of mHealth apps in their nascent days.
Numerous mHealth apps operate in India, providing doctor consultation-related services either online or offline. Practo, MFine, DocsApp, 1mg, Netmeds, Lybrate, MediBuddy, and Medlife were the eight most popular ones, with over a million downloads. While Practo, MFine and Lybrate offer doctor consultation through chat, audio, and video calling, Netmeds and DocsApp offer doctor consultation through both chat and audio calls. 1mg offers free chat consultation, while MediBuddy and Medlife offer audio call consultation only. Practo, MFine, 1mg, and Lybrate are the only mHealth Apps which help the patient book doctor appointments for offline consultation (Agarwal & Biswas, 2020). Practo could build a transactional mHealth platform that allowed doctors to list their services and manage patient interactions. It provided an array of services for patients, mainly for booking interactions with doctors and maintaining a consistent medical history (Srinivasan, 2015). But Practo, in its development stage, faced hiccups in training the medical professionals, their support staff and clinical staff on how to participate and use the platform. There was huge resistance from providers who found it challenging to shift from pen and paper to the digital mode of transactions. Providers, especially the administrative personnel, found it difficult to learn the software just by the instructional video lessons sent from Practo. Eventually, Practo had to infuse fresh creativity in its training activities for the providers and personnel so that they could work.
Shyama is now aware of the practicalities of digitally targeting rural health workers and practitioners. She does not give in to the oft-repeated claims that a smartphone can effectively bridge the fragmented markets in healthcare. But she is also convinced that there will soon be a policy consensus on mainstreaming Informal Providers in rural healthcare. So she begins to wonder if this portal can truly become revolutionary if the widely available informal service providers was to be made the target of this platform. Could presenting this idea in the next Roundtable meeting provide a breakthrough moment for this policy issue?
The Conversation with the Unrepresented section took place between an IP (Bangali Daktar) in the Bundelkhand area (border regions of Uttar Pradesh and Madhya Pradesh) and a social researcher. We thank Sonam Mahiwal and Professor Asmita Kabra (Ambedkar University Delhi) for arranging this interview. One of the authors participated in the Stanford India Health Policy Roundtable led by Professor Grant Miller that convened policymakers, academics, entrepreneurs and practitioners in January 2015 to discuss the role of the informal healthcare providers (IPs). We are thankful to the organizing team and the participants for insights. All the names used for persons and the start-up idea described in this case are fictitious and have no intentional resemblance to any real persons or entities. The event in the prologue is inspired by an actual incident in 2014. All the statistics used are from cited research studies, surveys, and secondary data sources. This case is intended to be used as a basis for class discussion rather than to illustrate either effective or ineffective handling of an administrative situation.
SUPPLEMENTAL MATERIAL
Supplementary materials for this article are available online.
Supplemental Material for To Rx or Not: Mainstreaming Informal Providers by Althaf Shajahan, Arnab Mukherji, in Vikalpa: The Journal for Decision Makers
Footnotes
ACKNOWLEDGEMENT
The Conversation with the Unrepresented section took place between an IP (Bangali Daktar) in the Bundelkhand area (border regions of Uttar Pradesh and Madhya Pradesh) and a social researcher. We thank Sonam Mahiwal and Professor Asmita Kabra (Ambedkar University Delhi) for arranging this interview. One of the authors participated in the Stanford India Health Policy Roundtable led by Professor Grant Miller that convened policymakers, academics, entrepreneurs and practitioners in January 2015 to discuss the role of the informal healthcare providers (IPs). We are thankful to the organizing team and the participants for insights. All the names used for persons and the start-up idea described in this case are fictitious and have no intentional resemblance to any real persons or entities. The event in the prologue is inspired by an actual incident in 2014. All the statistics used are from cited research studies, surveys, and secondary data sources. This case is intended to be used as a basis for class discussion rather than to illustrate either effective or ineffective handling of an administrative situation.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship and/or publication of this article.
NOTE
e-mail:
e-mail:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.