
Abstract
Affordable and appropriate physical and mental health care has long been conceptualized by many as a basic human right (Curtice & Exworthy, 2010; D’Oronzio, 2001; Kinney, 2000; Toebes, 1999). However, in the United States, healthcare access and healthcare quality are often determined by social policies impacting one’s options for health insurance coverage (Han et al., 2015). Being uninsured is associated with a variety of adverse health outcomes including symptom progression, declines in functioning, failure to diagnose preventable health conditions and premature mortality (Hoffman & Paradise, 2008; Sommers et al., 2015, 2017; Woolhandler & Himmelstein, 2017). Not having insurance also serves as a barrier to ongoing treatment and symptom control, such as accessing prescription medications for chronic conditions such as type II diabetes, which may be cost prohibitive for many young adults without insurance coverage (Kesselheim et al., 2016; Sommers et al., 2015; Watanabe et al., 2018).
Having health insurance and access to affordable and appropriate physical and mental health care is particularly important for youth with lived experience in foster care, who often experience complex physical, mental and developmental health concerns (Szilagyi et al., 2015). Youth with a history of out of home care are significantly more likely to experience mental health conditions such as depression, anxiety, attention deficit hyperactivity disorder (ADHD) and post-traumatic stress disorder (PTSD) (Child Welfare Information Gateway, 2022; Fechter-Leggett & O’Brien, 2010; Gypen et al., 2017). They are also significantly more likely to experience chronic physical health conditions such as type II diabetes, asthma, obesity, speech, hearing and vision problems and developmental delays than their peers without child welfare involvement (Child Welfare Information Gateway, 2022; Deutsch & Fortin, 2015; Gypen et al., 2017; Szilagyi et al., 2015). Foster youth in all 50 states and DC are eligible for public health coverage, such as Medicaid or other types of state sponsored group coverage.
Although the majority of states now offering extended out of home care services to youth up until age 21 (Child Welfare Information Gateway, 2022b), youth may “opt” out of participating due to the employment/education requirements associated with them or due to prior negative experiences while in foster care, choosing to discontinue involvement with the public child welfare system all together upon reaching the age of majority, regardless of the potential support that continued engagement with child welfare may offer (Bettencourt et al., 2021; Jones, 2019; Martin et al., 2016; Napolitano et al., 2015; Park et al., 2023).
Changes resulting from the Patient Protection and Affordable Care Act (2010), such as Medicaid expansion and allowing youth to remain on a biological or adoptive parent’s employment based health insurance until age 26, have resulted in a significant increase in the overall percentage of young adults with insurance coverage (Buchmueller et al., 2016; Jones, 2019), with the percentages of adults ages 18–64 who were uninsured decreasing from 22.3% in 2010 to 10.3% in 2021 (Cha & Cohen, 2022). However, as a group, foster youth alumni may not have equal access to the benefits brought about by the Affordable Care Act (Wilson-Simmons et al., 2016). Although expansion of Medicaid coverage in 39 states has enabled more transition age youth to access insurance coverage in adulthood, youth in the 11 remaining states are often left without health insurance options outside of the marketplace or employer sponsored plans. (Bullinger & Meinhofer, 2021; Wehby & Lyu, 2018; Wilson-Simmons et al., 2016).
Current research suggests that even with the implementation of the Affordable Care Act, sociodemographic characteristics are associated with insurance coverage related disparities. Recent statistics on healthcare coverage for adults in the United States indicate that non-Hispanic White individuals are significantly more likely to have health insurance coverage than Black, Indigenous and other People of Color (BIPOC) (Buchmueller et al., 2016; Sohn, 2017; Wehby & Lyu, 2018). This could have important implications for BIPOC youth transitioning out of care as BIPOC youth are both overrepresented within child welfare systems nationwide and have consistently reported adverse physical and mental health outcomes relative to non-Hispanic White youth (Dworsky et al., 2010; Gypen et al., 2017). Research also suggests that men are less likely to have insurance coverage than women, and also are less likely to be covered by public health insurance plans, such as Medicaid, due to gender specific differences in qualifying health conditions, such as pregnancy (Courtemanche et al., 2019; Manuel, 2018).
Disparities in health insurance coverage also exist in the general population related to one’s sexual orientation, gender identity and expression (SOGIE) (Buchmueller et al., 2016; Jackson et al., 2016; Lewis et al., 2019; Washburn et al., 2024). Researchers have argued that negative social climate toward LGBTQ + individuals and associated non-affirming social policies, along with anti-LGBTQ beliefs of healthcare providers, can serve as a barrier to health care utilization among LGBTQ + individuals (Aleshire et al., 2019; Romanelli & Hudson, 2017). Thus, LGBTQ + foster youth alumni may also face multiple barriers in obtaining insurance and to receiving needed physical and mental health care.
Given the importance of having insurance coverage for meeting one’s healthcare needs, the research team sought to answer the following research questions and explored the following research hypotheses: 1. Are foster youth alumni with health insurance coverage more likely to access physical and/or mental health care when needed relative to foster youth alumni without insurance? (a) Foster youth alumni with insurance coverage would be less likely to forgo physical and mental health care when needed. 2. What combination of sociodemographic characteristics of foster youth alumni are associated with differences in insurance coverage over time? (b) Sociodemographic characteristics such as reason for exit from care, race/ethnicity, gender and LGBTQ + status will predict changes in insurance coverage over time. (c) State level factors such as Medicaid expansion and having state level protections specific to LGBTQ + foster youth will predict changes in insurance coverage over time.
Methods
Data for this study were drawn from the longitudinal Jim Casey Youth Opportunities Initiative restricted release data set, which investigates a variety of health and wellness outcomes for youth ages 14–26 with lived experience in foster care. Starting in 2003, youth foster care alumni residing in the 16 Jim Casey Initiate site states 1 were recruited by local agencies serving this population were invited to participate in the biannual online Opportunity Passport Participant Survey (OPPS). This survey, administered online in either English or Spanish between 2003 and 2022. The self-report survey inquires about participant sociodemographic characteristics and domains of functioning including housing and financial stability, mental and physical health, education, employment, and permanency. In 2018, youth over the age of 18 could opt to have their de-identified past and current survey data included in a restricted use data set to be used by external researchers. Therefore, while only youth already 18 and over could consent to have their past survey data used by researchers, the compiled dataset included some entries from older youth who had started participating in the survey between 14 and 17 years of age. Access to the most recent download of these data was granted in July 2022. These data can be used for cross sectional analyses as well as longitudinal analyses. Longitudinal data used for this study (n = 2,420) were drawn from all waves of data collection between 2012 (the beginning of Medicaid expansion) and 2022. Our sample was comprised of foster youth alumni ages18 years and older who were not participating in extended foster care. A more detailed description of the methods used in the initial data collection process can be found in JCYOI (2008).
Predictor variables
Demographic variables
To help protect the privacy of participants, age in the restricted use data set was dichotomized by its creators into two categories: participants who were 18–21 years old coded as (0) and those 22–26 years old, coded as (1). Race/ethnicity was originally distributed across seven categories but due to the complexity of the planned analyses, these data were recoded into a variable that compared White youth (0) to non-Hispanic Black youth (1), Hispanic/Latino youth (2) and other race/ethnicity youth (3). The LGBTQ + identity variable, constructed by researchers at the Jim Casey Initiative combined data on sex assigned at birth (available within the data set used) and data on sexual orientation and gender identity (data that was collected within the survey but not available to external researchers). 2 LGBTQ + identity was categorical variable based on respondents that self-reported identifying as LGBTQ + at any point in time (1), or those who never self-reported identifying as LGBTQ+ (0). Reason for exit from care was collapsed into three categories for analysis: emancipation or exiting care due to age (0), guardianship or adoption by someone outside the family (1) or kinship (e.g., reunification with birth parent or living with another relative) (2).
Predictor variables potentially impacting insurance coverage
Existence of LGBTQ + affirming policies
The research team conducted an online review of state level social policies related to LGBTQ + individuals as well as a review of child welfare policies and non-discrimination statements specific to LGBTQ + youth residing in the states where the Jim Casey data were drawn. This variable was included because it is reasonable to believe that LGBTQ+ youth residing in states without affirming policies may be more likely to have experienced secondary trauma resulting in ongoing physical and mental health concerns as a result of their child welfare involvement. Multiple data sources such as the Movement Advancement Project (https://www.lgbtmap.org/equality-maps/non_discrimination_laws), Human Rights Campaign State Equality Index https://www.hrc.org/resources/state-equality-index), and the Lambda Legal State-by-State analysis of child welfare systems (https://www.lambdalegal.org/child-welfare-analysis) were used to group the participating Jim Casey sites into 2 groups as “Non-affirming” meaning that the state had no explicit protections for LGBTQ + individuals or any rules specific to child welfare offering equal protection or prohibiting discrimination and overall protections for LGBTQ + individuals within the state in general and “Partially-affirming/Affirming” meaning that they had at least some state level protections or child welfare specific protections for LGBTQ+ individuals. States designated as “Affirming” were coded as (1); while “Non affirming” states were coded as (0). Criteria used to classify these states are presented the Appendix.
Medicaid expansion
The impact of Medicaid expansion was considered a time-varying covariate for subsequent analysis, as former foster youth’s opportunity to access health insurance through their state Medicaid plan may change over time. If a participant was surveyed prior to Medicaid expansion in their state, the interview was coded (0) as “no possibility of benefiting from Medicaid expansion.” If a participant was interviewed during the year of Medicaid expansion in their home state or after, the interview was coded (1) as “possibility of benefiting from Medicaid expansion.” All respondents from states that have not expanded Medicaid as of 2022 were coded as (0) across all interviews.
Outcome variables
Seeking physical or mental health care
Respondents were asked to respond to the item “Has there been any time over the past six months when you thought you should get medical care but you did not?” Those that reported “yes” were coded as (1) and those who responded “no” were coded as (0). Participants were also asked to respond to the item “Has there been any time over the past six months when you thought you should see a mental health professional for a problem such as depression, substance abuse or anxiety, but did not?” Those that reported “yes” were coded as (1) and those who responded “no” were coded as (0).
Health insurance
Respondents were asked to respond to the item “Do you have health insurance?” Those that reported “yes” were coded as (1) and those who responded “no” were coded as (0). Those who responded “I don’t know” (n = 766 or 6.6% of responses) were coded as “missing” and excluded from these analyses as to not inflate estimates of youth with insurance coverage. Health insurance was explored as the primary outcome variable, as well as a predictor of seeking physical and/or mental health care when needed.
Data analysis
Data were reviewed for missingness and normality. Only one item, exit reason, had missing data and the missingness was minimal (n = 14 out of 2,420 participants, 0.58%). All respondents included in this sample had a valid response to both the predictor and outcome variables in at least one of the survey waves. Descriptive analyses were conducted to determine counts and frequencies of categorical data and means/standard deviations for scale data. Analyses were conducted using SPSS Statistics version 27 and Stata 16.1. Binary logistic regression with robust standard errors for each cluster was first used to answer the first research question. The authors then conducted a series of hierarchical linear modeling to answer the second research question. Hierarchical linear modeling was the analytic approach used as it allows for both within-subject change and between-subject change while including both time-varying and time-invariant predictors.
The research team used a bottom-up approach to build a series of models The empty model analyzed the amount of within-individual and between-individual variance. In growth model, we explored the change trajectory in health insurance coverage over the 10 years and its correlation with Medicaid expansion. Thus, the growth model included the time varying covariates—sequence of survey and Medicaid expansion. Next, individual-level time invariant predictors (demographic variables and other covariates) and state-level protections for LGBTQ+ people were used to predict the intercept of health insurance coverage. Three interaction terms between LGBTQ+ identity and state-level protections, between LGBTQ+ identity and race/ethnicity, and between LGBTQ+ identity and sex assigned at birth were also added into the intercept-as-outcome model. The final model—Intercept-and-slope-as-outcomes model— included the random intercept from previous model and added a random effect for the change trajectory, predicted by state-level protections for LGBTQ+ people, LGBTQ+ identity, race/ethnicity, sex assigned at birth, and type of exit from care.
Results
Descriptive statistics of predictors and outcome variables.
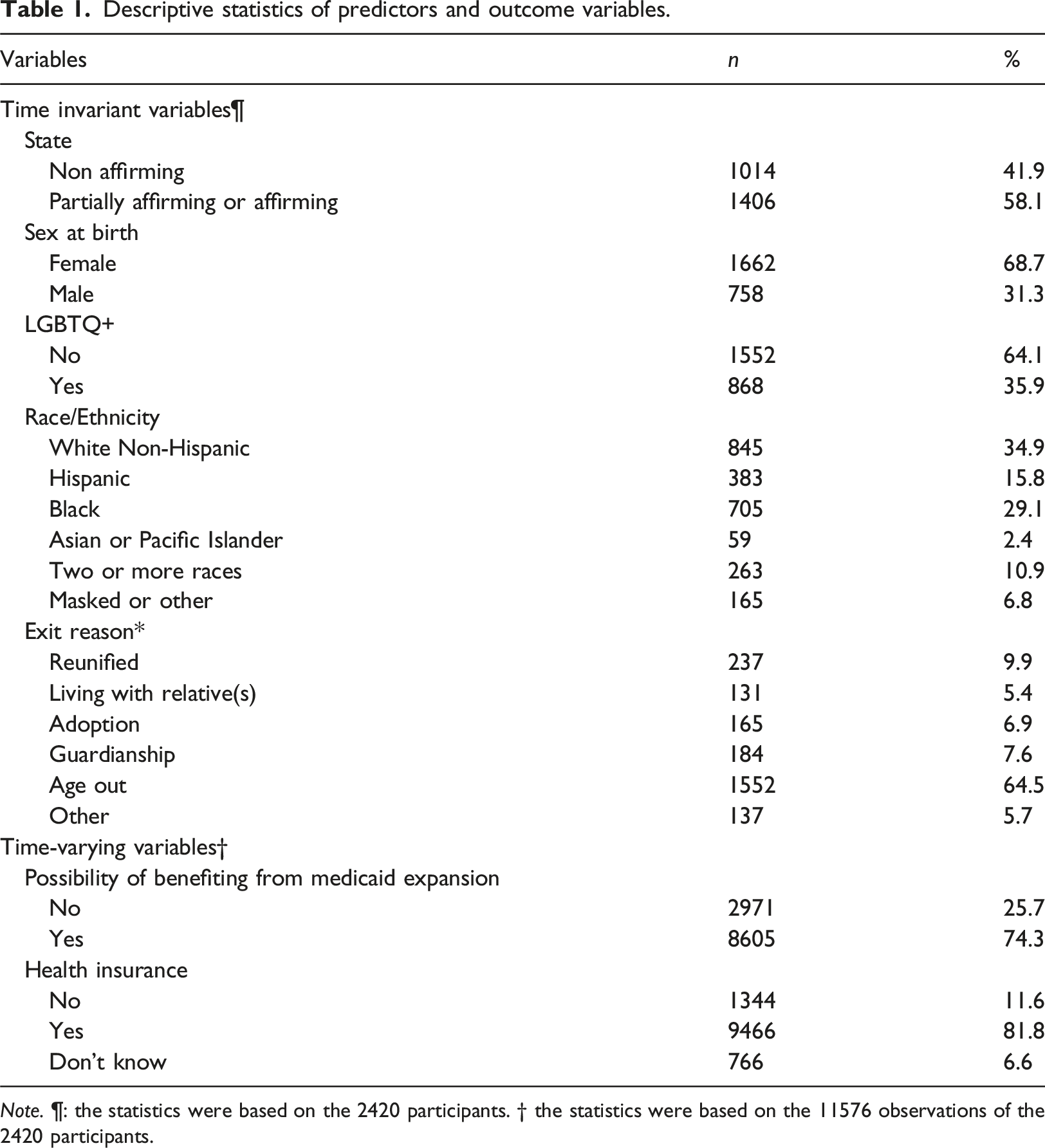
Note. ¶: the statistics were based on the 2420 participants. † the statistics were based on the 11576 observations of the 2420 participants.
White (n = 845, 34.9%) with approximately one third identifying as LGBTQ+ (n = 868, 35.9%). The most frequent reason given for exiting care was aging out (n = 1552, 64.5%). Over half of the respondents lived in states with at least some protections in place for LGBTQ + people (n = 1,406, 58.1%) and 25.7% of the responses (n = 2,971) came from participants who lived in the three states that opted to not expand Medicaid coverage or were interviewed prior to Medicaid expansion in their state. The majority of responses across data collections periods indicated that the youth had health insurance coverage (n = 9,466 responses, 81.8%). Approximately one third of all responses indicated that youth did not seek medical care when needed (n = 3,564, 30.8%), with slightly more reporting not seeking mental health care when needed (n = 3,778, 32.6%).
Research question #1
After adjusting the standard error for cluster sampling (each individual could potentially respond at multiple waves of data collection), data indicated that having health insurance significantly lowered the likelihood of a young person not seeking physical health care when needed (OR = 0.41, robust standard error = 0.03, p < .001). Similarly, having health insurance significantly lowered the likelihood of a young person not seeing a mental health professional when needed (OR = 0.81, robust standard error = 0.07, p = .01).
Research question #2
In the unconditional model, the intraclass correlation was .67, with 67% of the variance in the outcome variable occurring among individuals. In Model 2, having health insurance within individuals did not change significantly with time (indicated by the sequence of surveys) (b = 0.04, p = .13). However, the model fit for the fixed effect of time was significantly worse than when we included a random effect for time (Likelihood ratio (LR) χ2(df = 2) = 62.41, p < .001, and therefore was modeled as a random effect in the subsequent models. For individuals who lived in states with Medicaid expansion, the likelihood of having health insurance increased significantly over time (b = 1.07, p < .001).
Hierarchical linear model of having health insurance among former foster youth, N = 2420.
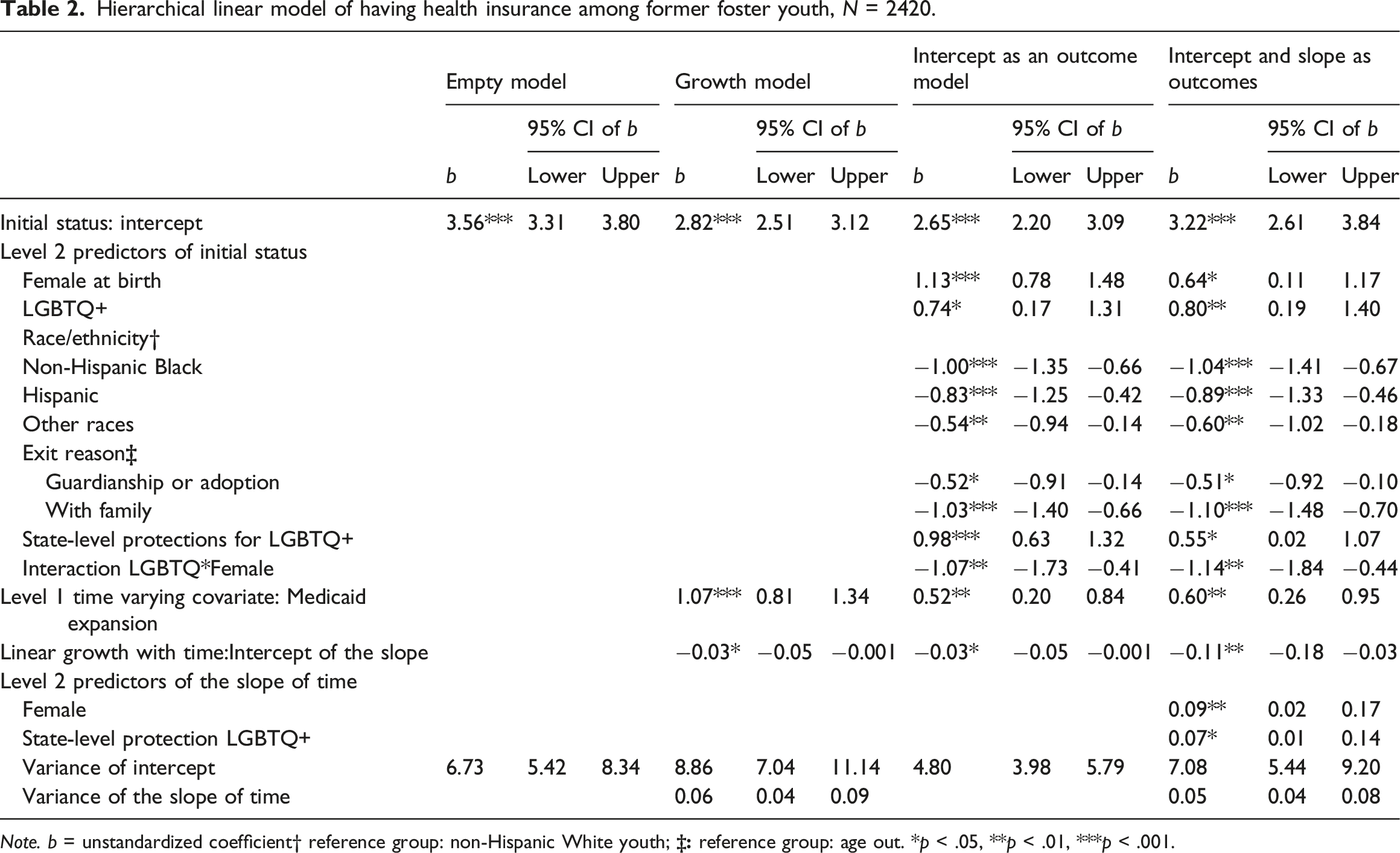
Note. b = unstandardized coefficient† reference group: non-Hispanic White youth;
Intercept-and-slope-as-outcomes model predicted the random slope of time using state-level protections for LGBTQ + individuals, exit reason, LGBTQ + identity, sex assigned at birth, and race/ethnicity. The interaction between time and sex assigned at birth and the interaction between time and state-level protection for LGBTQ + individuals were significant. This model also improved model fit compared to Intercept-as-outcome model (χ2 (df = 8) = 71.93, p < .001). The final Intercept-and-slope-as-outcomes model is the trimmed version of Model 5 with the two nonsignificant interaction terms excluded (see Table 2). In the final model, for an individual changing from having no possibility of benefiting from Medicaid expansion to having a possibility of benefiting from Medicaid expansion, the likelihood of having health insurance increased significantly (aOR = 1.82, p = .001, 95% CI: 1.30–2.58).
When compared with youth who aged out, youth under guardianship or reported being adopted had lower odds of having health insurance (aOR = 0.60, p = .02, 95% CI: 0.40–0.90); youth living with family members also reported lower odds of health insurance (aOR = 0.33, p < .001, 95% CI: 0.23–0.50). Compared with non-Hispanic White youth, all groups of BIPOC youth reported lower odds of having health insurance (non-Hispanic Black youth aOR = 0.35, p < .001, 95% CI: 0.24–0.51; Hispanic youth: aOR = 0.41, p < .001, 95% CI: 0.26–0.63; other race/ethnicity youth: aOR = 0.55, p < .001, 95% CI: 0.36–0.84). In terms of other demographic predictors, the interaction between LGBTQ + identity and sex assigned at birth was significant (b = −1.15, p = .001) and therefore needs to be reported jointly. For those assigned male at birth, identifying as LGBTQ + increased the likelihood of reporting having health insurance, compared to non-LGBTQ + youth (aOR = 2.26, p = .01, 95% CI: 1.23–4.13). However, the LGBTQ + identity was not significantly associated with health insurance among those assigned female at birth (aOR = 0.71, p = .07) (Figure 1). Interaction between SOGIE and sex assigned at birth on health insurance status.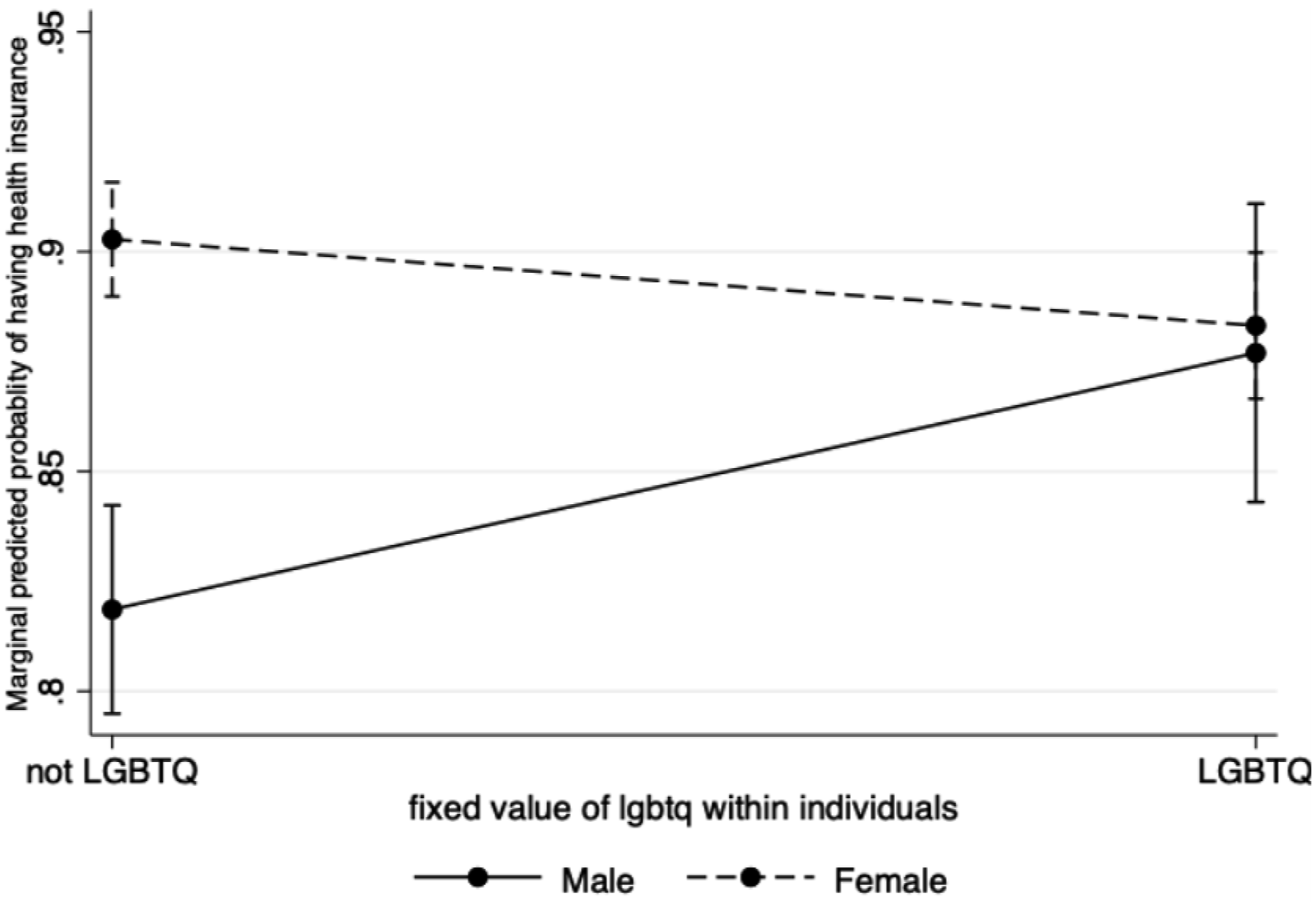
The interaction between time and sex assigned at birth was significant (b = 0.10, p = .01) and therefore needs to be reported jointly. For those assigned male at birth, the likelihood of having health insurance decreased with time (aOR = 0.90, p = .004, 95% CI:0.83–0.97). For those assigned female at birth there was no significant change over time (aOR = 0.99, p = .73) (Figure 2). Interaction between SOGIE and time on health insurance status.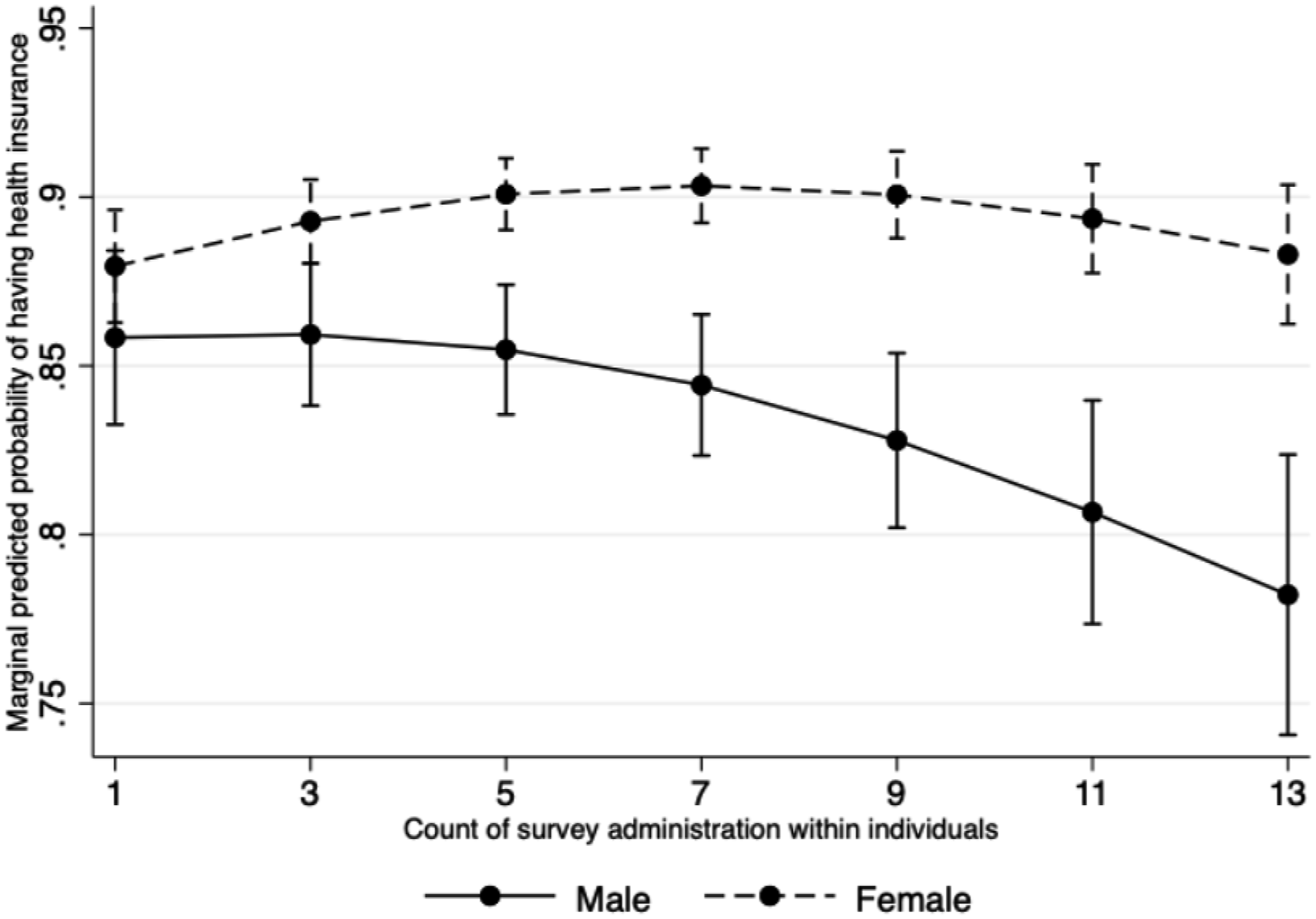
The interaction between time and state-level protection for LGBTQ+ individuals was significant (b = 0.08, p = .03) and therefore needs to be analyzed jointly. For those residing in states with non-affirming policies, participants’ likelihood of having health insurance decreased with time (aOR = 0.90, p = .004). For those residing in affirming states, there was not significant change over time (aOR = 0.97, p = .37). To analyze the interaction from another angle, i.e., treating state-level protection for LGBTQ + individuals as the focal variable, we can see that at the beginning of the study, the youth in affirming states were more likely to report having health insurance than youth from non-affirming states (aOR = 1.75, p = .04), and over time, the difference in the probability having health insurance between residents of non-affirming states and affirming states became even larger (Figure 3). Interaction between time and state level protections on health insurance status.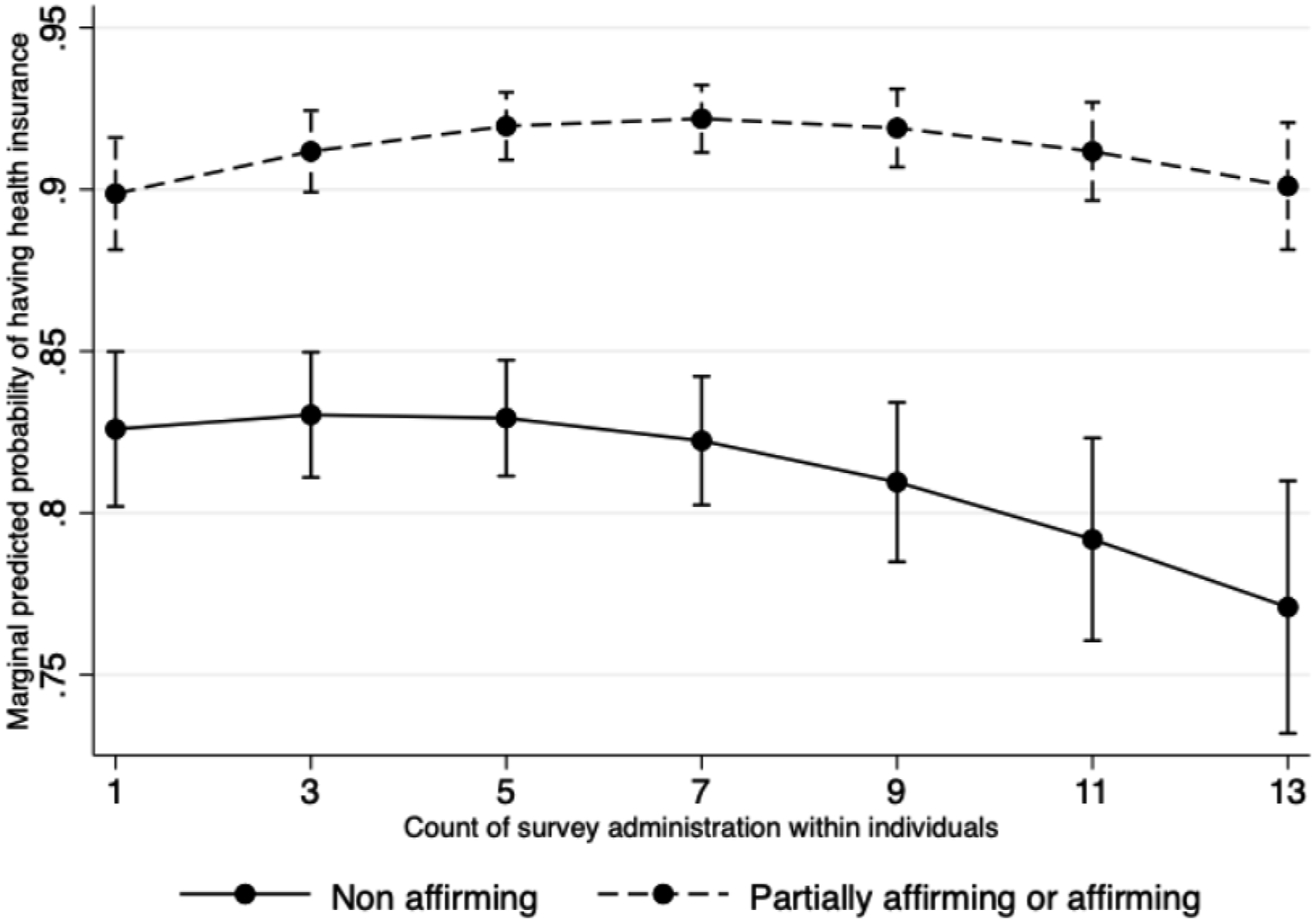
Discussion
These findings add to our understanding of the relationship between state level policies (LGBTQ_ protections, Medicaid expansion) and sociodemographic variables which may be associated with insurance coverage. This was consistent with our first hypothesis that insured youth would have lower odds of not seeking physical and/or mental health care when needed was supported. This finding is consistent with the overall body of literature highlighting that the relationship between health insurance coverage and help seeking across various populations of young adults (Anderson et al., 2007; Douthit et al., 2015; Sommers et al., 2017) and now may be extended to foster youth alumni. As health insurance coverage is consistently associated with higher levels of healthcare access, it is important for youth transitioning out of care (and beyond) to be afforded opportunities to enroll (or be automatically enrolled) in affordable public health insurance programs, such as Medicaid. It is recommended that Medicaid eligibility in all 50 states and DC is updated so that if one had formerly been in foster care, that regardless of exit reason, that person will automatically qualify for Medicaid benefits until the age of 28, or ten years post exit to support any ongoing healthcare needs that they may have once exiting care.
Our second hypothesis concerning the relationship between health insurance coverage and respondent sociodemographic characteristics was partially supported. Compared to youth who are living with family, were in kinship care or were adopted, those who had emancipated or aged out of care were more likely to report having health insurance. One possible explanation is that even though youth exited care to a family environment, this alone does not ensure that they will have increased access to health insurance after age 18, as youth who exited to kinship care may not be eligible to be on the insurance plans of relatives who are not their biological parents. It is also possible that the biological parents of these youth are employed in jobs do not offer health insurance coverage that could be extended to their dependents. This finding may be also a result of youth who emancipated “age out” having to more fully assume adult roles and responsibilities, such as addressing their healthcare needs without the help or support of others. Youth who were preparing to age out may have had increased access to independent living preparation services compared with youth who were officially connected with some form of “family” upon whom they (presumably) may rely upon at age 18 and beyond. Prior research has found that youth in foster care who receive independent living services are more likely to have concrete independent living skills, such as knowledge of how to obtain health insurance and addressing their health care as needed, than their peers who did not receive services (Lemon et al., 2005).
BIPOC foster youth alumni were more likely to lack insurance coverage than non-Hispanic White peers. The magnitude of this difference among the different groups of BIPO youth was small (ranging from aOR = 0.35 to aOR = 0.55), indicating that there may systemic issues that may be preventing BIPOC youth from accessing health insurance at the same rate as their White non-Hispanic peers, despite Medicaid expansion in many states. This finding is also consistent with prior research concerning health insurance coverage of American adults as a whole and in relation to other samples of foster youth alumni (Buchmueller et al., 2016; Gonzales & Ortiz, 2015; Macapagal et al., 2016; Sohn, 2017; Wehby & Lyu, 2018), This issue warrants further investigation and additional research concerning which subgroups of BIPOC individuals are most disproportionately without insurance coverage is needed.
No main effects were found in relation to health insurance coverage for sex assigned at birth and for health insurance coverage in relation to identifying as part of the LGBTQ + community. However, there were some interaction effects related to these predictors which warrant additional discussion. There was a significant interaction effect for gender and SOGIE. LGBTQ + individuals assigned male at birth were more likely than their non- LGBTQ + male peers to have health insurance. This finding builds upon prior studies which have shown inconsistent findings on the relationship between LGBTQ + identity, insurance status and accessing needed health care in the general (non-foster youth) population. For example, Heck and colleagues (2005) have found that men in relationships with other men were more likely to access health care than men in relationship with women, while Buchmueller and Carpenter (2010) found that men in same sex relationships were less likely to have health coverage and access healthcare when needed. As these prior studies were conducted a number of years prior to the current study, factors influencing healthcare seeking pattens in men may have changed over time, or that they are not as applicable to young male foster care alumni as a distinct group. It is also possible that our finding may reflect the high volume of public health messaging around prevention of HIV and other sexual health risks that that have been specifically targeted at gay/bisexual/queer men (Keuroghlian et al., 2017; Mustanski et al., 2015), presumably making them more cognizant of their overall healthcare needs, which may also include health insurance.
Another interesting finding was that for those assigned male at birth, the likelihood of having health insurance decreased over time/with age, but not for those assigned female at birth. It is possible that these sex difference could be attributed to a higher percentage of those assigned female at birth (and still presenting as female) engaging with healthcare systems to secure birth control or to address their pregnancy and postpartum related needs. Moreover, those assigned months post birth, making them more likely to have insurance over time.
Two findings related to state level policies, such as Medicaid expansion and having affirming policies for LGBTQ + people were also of note. Not surprisingly, youth who reported being uninsured at their first point of data collection had almost double the odds of becoming insured over time in states where there was Medicaid expansion. It has consistently been demonstrated that the expansion of Medicaid is associated with reductions in uninsured rates across most major demographics including sex assigned at birth, SOGIE, race/ethnicity and age (Buchmueller et al., 2016; Courtemanche et al., 2019). Thus, ongoing advocacy efforts related to expanding Medicaid the states that currently have not engaged in Medicaid expansion is warranted.
There was also a significant interaction between time and state level protections for LGBTQ+ individuals. Overall, those in affirming states were more likely to report having insurance coverage than those in non-affirming states. Unfortunately, the gap between affirming and non-affirming states has increased over time indicating that those who live in non-affirming states continue to have lower odds of being insured, regardless of Medicaid expansion or their SOGIE. It is possible that the overall social climate in states that don’t have affirming/inclusive policies protecting their LGBTQ + residents are in general less favorable for any minoritized group, including foster youth alumni, impacting their ability to effectively find and enroll in affordable healthcare coverage.
Limitations
`As with any study, there are limitations of this work which should be highlighted. These data were drawn from a non-random sample of youth who consented to share their survey responses for research purposes. Thus, these findings may not be representative of youth who opted to not participate in this survey or youth who did not consent to data sharing. Data on participants’ state of residence was based on the place where youth had resided at the time of data collection. However, since the youth included in this study had all aged out of care at the time of data collection, some of these youth may have potentially moved to a new state after exiting care. Data provided to the research team combined sexual orientation and gender identity information into a composite LGBTQ + variable. Thus, the research team was unable to determine if differences in outcomes for LGBTQ + youth were related to their sexual orientation, gender identity or both. Similarly, many state level policies and protections may have evolved during the ten year sampling frame that was used for these data. Classification into “affirming” vs. “non-affirming” states was based on a review of state level policies in Spring of 2022, which resulted in the most conservative way to categorize these state level policies. Despite these limitations this work has contributed to our growing body of knowledge concerning foster youth alumni, health insurance coverage and healthcare seeking.
Conclusion and Recommendations
When considered together these results indicate that BIPOC foster youth alumni are less likely to have insurance coverage, expanding Medicaid eligibility led was associated with greater percentage of foster youth alumni reporting insurance coverage, and that insurance coverage contributes to if foster youth alumni may not seek needed medical and/or mental health care despite their own appraisal that they needed assistance in these areas. However, this is not the only reason why youth in need of care may not seek it when needed. Prior work in this area indicates that mistrust of medical providers and other authority figures was consistently a barrier to accessing healthcare for young adults, and in particular for those identifying as LGBTQ+ (Green et al., 2020; Han et al., 2015; Yen et al., 2009).
Thus, advocacy and policy revision efforts should focus on the following areas (1.) expanding Medicaid coverage in all 50 states; (2.) increasing health literacy in former foster youth, particularly BIPOC youth, to build skills around healthcare enrollment selection and knowledge of automatic eligibility to enroll in state sponsored Medicaid until age 26. This could be facilitated by having states provide automatic enrollment in adult Medicaid for all foster youth alumni once they reach the age of majority, rather than requiring these youth to complete the enrollment process; (3.) increasing the number of culturally competent and affirming physical and mental health care providers. This could be achieved through increasing the number of BIPOC healthcare providers and the expansion of professional training curriculum and professional standards to more adequately prepare healthcare professionals to engage with diverse groups of clients, as well as ending “religious refusals” which allow practitioners in certain states to decline to provide care, services and medications due to their personal religious beliefs and (4.) working on building increased trust between foster youth alumni and public systems of “care” such as healthcare, in order to increase the percentage of foster youth alumni with insurance coverage and maximize engagement with healthcare systems to truly be able to address their ongoing healthcare needs. Foster youth alumni are some of our most vulnerable young adults and to help assure their success in adulthood, their physical and mental healthcare needs must be adequately addressed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
Appendix
Note. (-) = does not have state level protections related to sexual orientation or gender identity, (+) = has state level protections related to sexual orientation and gender identity.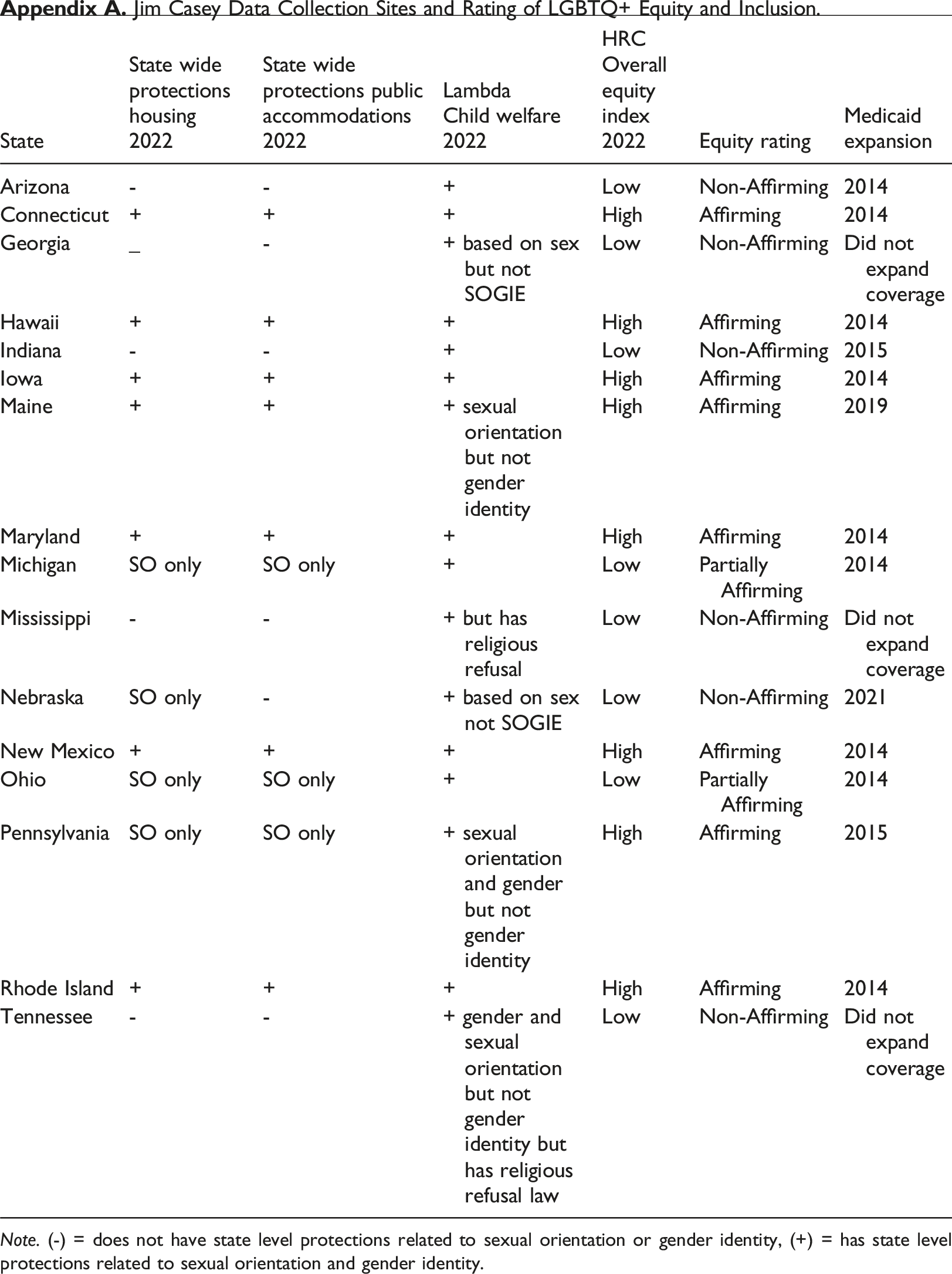
State
State wide protections housing
State wide protections public accommodations
Lambda
HRC
Equity rating
Medicaid expansion
Arizona
-
-
+
Low
Non-Affirming
2014
Connecticut
+
+
+
High
Affirming
2014
Georgia
_
-
+ based on sex but not SOGIE
Low
Non-Affirming
Did not expand coverage
Hawaii
+
+
+
High
Affirming
2014
Indiana
-
-
+
Low
Non-Affirming
2015
Iowa
+
+
+
High
Affirming
2014
Maine
+
+
+ sexual orientation but not gender identity
High
Affirming
2019
Maryland
+
+
+
High
Affirming
2014
Michigan
SO only
SO only
+
Low
Partially Affirming
2014
Mississippi
-
-
+ but has religious refusal
Low
Non-Affirming
Did not expand coverage
Nebraska
SO only
-
+ based on sex not SOGIE
Low
Non-Affirming
2021
New Mexico
+
+
+
High
Affirming
2014
Ohio
SO only
SO only
+
Low
Partially Affirming
2014
Pennsylvania
SO only
SO only
+ sexual orientation and gender but not gender identity
High
Affirming
2015
Rhode Island
+
+
+
High
Affirming
2014
Tennessee
-
-
+ gender and sexual orientation but not gender identity but has religious refusal law
Low
Non-Affirming
Did not expand coverage