
Abstract
Little is known about adoptive parents’ experiences of and satisfaction with statutory child and adolescent mental services (CAMHS) in the UK, nor of parental concerns about their adopted children’s mental health and well-being. Ninety-eight adoptive parents completed an online survey about their satisfaction with services as well as their mental health concerns for their child currently and retrospectively at the point of adoption. Parental concerns were diverse, and many overlapped with issues that CAMHS could normally help with. Attachment was the primary concern initially, but this decreased over time in placement; while challenging behaviour was the highest rated current concern, along with aspects of general functioning such as peer relations, social skills and education. Unexpectedly, trauma was a relatively low concern at both timepoints. There were very high levels of dissatisfaction with CAMHS, evident across questions of access, engagement and quality of services, all at levels much higher than typically reported by general samples. Adoptive parents’ substantial dissatisfaction with CAMHS occurred despite an apparent fit between many parental concerns and the kinds of services typically offered in CAMHS. There remains a significant challenge to develop a shared understanding between parents and services of adopted children’s needs, especially given the absence of data about adopted children’s mental health and wellbeing problems.
Introduction
Post-adoption support services are important for promoting child well-being, family functioning and the stability of the placement (Selwyn et al., 2014). However, not enough is known about the kinds of services adoptive parents want or what their concerns are (Alves et al., 2022). What data there is suggests wide ranging concerns partly due to the broad remit of what is included under post-adoption support (potentially covering financial help, social care and educational involvement as well as help for general or specific mental health issues) but also due to significant variations in studies. Reviews of the quality of adoption support have found large sample heterogeneity and multiple sources of bias (Harris-Waller et al., 2018) and as a result have been unable to provide clear messages or “point in any clear direction” (e.g., Drozd et al., 2017, p. 339). Therefore, investigations of post adoption support should clarify what domain of support is being considered (e.g., child mental health and well-being) as well as the adoption context of the country being studied. For example, there are important differences in adoption practices in the UK compared with Europe and the US, namely the majority of children in the UK are adopted from within the care system, rather than transnationally (Mignot, 2015). Within-country adoptees from the care system have higher rates of mental health issues than international adoptees (Juffer & van IJzendoorn, 2005; Keyes et al., 2008), and therefore much of the existing international research cannot be easily transported into the UK context.
A further complication for the UK context is that little is known about the formal mental health needs of adopted children in the UK, although the mental health disorders and associated impairment amongst children looked after (CLA) in the UK has been reported in a high-quality study, albeit conducted over 20 years ago (Ford et al., 2007). Compared with children living in birth families, findings indicated higher rates of all mental health disorders in UK CLA, including behavioural problems, learning problems and neurodevelopmental disorders, such as autism and Attention Deficit/Hyperactivity Disorder (ADHD), anxiety disorders and depression (Ford et al., 2007), conditions for which statutory Child and Adolescent Mental Health Services (CAMHS) should be able to routinely provide help. In the absence of specific data for adopted children in the UK, most of whom are adopted from care, these findings suggest that many children adopted in the UK would meet criteria for a mental health disorder routinely treatable by CAMHS.
Adding to the uncertainty, little is known about how well CAMHS are meeting the needs of adopted children in the UK. One the one hand, satisfaction with statutory CAMHS services in the general population is very high, regularly over 80% for questions about whether the respondent would recommend the service to their friends and family (NHS, 2016); on the other, adopted families report significant barriers to accessing appropriate mental health services (Selwyn et al., 2014). One hypothesis about the barriers faced by adoptive families accessing appropriate healthcare is that their concerns may be different to those traditionally offered by mental health services, and especially with a focus on attachment issues (Barth et al., 2005), which may not be understood in CAMHS and are often confused with other common disorders, including behavioural problems in the UK and US (Allen & Schuengel, 2020; Woolgar & Baldock, 2015). Indeed, a recent US survey of the parents of adopted and fostered children reported low levels of satisfaction with mental health services specifically to treat attachment and the family, while indicating that their primary concern was child behavioural problems (Barnett et al., 2018).
Comparisons of lay versus professional understanding of mental health disorders in general populations reveal some superficial agreement but also important differences that can drive patient dissatisfaction (e.g., Butlin et al., 2019; Tse & Haslam, 2023). Thus, while formal psychiatric diagnoses typically shape how statutory mental health services are organised, when inquiring of parental concerns, it may be helpful to use descriptions of problems and concerns rather than suggestions of frank psychiatric disorders. For example, a recent study of adopted parents in Portugal using descriptive rather than formal psychiatric terms reported a wide range of concerns, of similar form to those reported by birth families (Alves et al., 2022). Similar wide-ranging descriptions of concerns have also been found in UK samples (Meakings et al., 2018) and US samples (Houston & Kramer, 2008; Waid & Alewine, 2018).
Research has also indicated that there may be different levels of need at different points in the adoption journey, but also that the research messages can vary by adoption context. For example, parents in Portugal identified the first few years as especially difficult (Alves et al., 2022) contrasting with research in the US which found needs increased over time (e.g., Waid & Alewine, 2018).
The current study will examine: adoptive parents' satisfaction with statutory CAMHS services in the UK for addressing adopted children’s mental health needs; perceived barriers to access; as well as the range of the specific concerns for their children’s well-being. These concerns will be explored both at the point of adoption (measured retrospectively) and currently, to account for the possibility of changes in concerns over the course placement.
Methods
Participants and procedures
The sample was self-selected on the basis of adverts in adoption-specific media, including newsletters and magazines produced by adoption agencies and local authorities. The adverts presented a brief summary of the research and a link to the online survey, hosted by the Bristol Online Surveys platform [https://www.onlinesurveys.ac.uk/]. The first page of the on-line survey, prior to any data collection, contained an information sheet about the research, including the anonymisation and confidential storage of the data collected; continuation with the survey beyond the information sheet implied consent. Once the survey had been completed, participants were given an opportunity submit an email to claim an online voucher for £5. Both the information sheet and the exit page of the survey contained information for accessing further support for participants who experienced any anxiety or distress as a result of completing the survey, as well as contact details for the researcher. The research was approved by King’s College London Research Ethics Committee (PNM/14/15-74), and data collection was conducted between October 2015 and January 2016.
Inclusion criteria were that respondents had to have had at least one adopted child either currently or in the past. A total of 127 adoptive parents completed the on-line survey. Of these, 29 participants reported the current age of their adopted child over 18 years, and these were excluded from the current analyses, to ensure a sample that was still potentially involved with CAMHS, for a final maximum target sample of N = 98.
Measures
The questionnaire was developed with stakeholder input from Adoption UK, the UK’s largest national charity for adoptive families, to ensure the questions asked met the concerns of adoptive families, especially with regard to the descriptive account of likely parental concerns (see Appendix S1 for the survey). Questions assessed several areas in the birth parents’ background history, including predisposing risk factors, pregnancy and perinatal history. Areas related to adoptive family composition, education, adopted parents’ satisfaction with level of information about the children, as well as initial and current concerns were also examined.
Parental concerns were presented as a list of 18 specific items, as well as five ‘others’ left as open text for parents to describe issues that were not represented, these other categories were counted as part of the total number of concerns, but their content is not reported here. Parents were asked for retrospective concerns initially at adoption as well as currently to a) indicate any that were problems and b) to rank up to 5 top concerns. The concern data presented here includes a) the sum of any endorsement as a concern; b) the primary concern at each time point; and c) the top 3 concerns at each time point.
Satisfaction with mental health services provided to adoptive families were queried including: overall satisfaction with CAMHS and other service providers, as well as further dimensions of satisfaction for CAMHS specifically focusing on: access; satisfaction with treatment; and the quality of the collaborative relationship. In the current analyses, for all questions regarding satisfaction, the original categories of “very poor”/“not satisfied” were recoded as “negative”; “adequate” was recoded as “neutral”; “good”/“excellent” were recoded as “positive” ratings. Parents were also asked to complete the NHS Friends & Family questions about their CAMHS experiences (“How likely are you to recommend the service to friends and family if they needed similar care or treatment?”) as this simple service user satisfaction question is routinely asked across all statutory health services in the UK, including CAMHS. Lastly, adoptive parents completed a section on perceived barriers to accessing CAMHS Services, including time taken to receive services.
Data analysis
The survey data were exported into IBM SPSS Statistics 22 for analysis. We report absolute (n) and relative frequencies (%) to describe all categorical variables and means and standard deviations for continuous variables.
Results
Demographic characteristics
Parental respondents identified as 90.3% females and 9.7% males, with a mean age of 46.58 (sd = 6.53, range 31–61). A total of 79.3% of the sample lived as a couple (68.1% as a heterosexual couple, 8.2% gay or lesbian and 3.0% did not specify), 13.4% were single and 7.2% were either separated or divorced. Index children had a mean age at the time of the questionnaire of 10.53 years (sd = 3.91, range 2–18) and 54.1% were male. 83.7% were White, 6.7% were Black or Black dual heritage, 4.0% Asian and the remaining 5.6% identified as other mixed/multi-ethnic groups.
Over two-thirds (69%) of the sample reported multiple experiences of abuse or neglect in the child’s early life, (41.8% physical abuse, 62.2% emotional abuse, 15.3% sexual abuse and 78.6% neglect), whereas only 6% reported their child experienced none of these.
Life placement chronology and adoptive family
Children were on average 2.18 years (sd = 1.78, range 0–7) when they were removed from birth families and 3.74 (sd = 2.10, range .7–10) when adopted. By the time respondents participated in the evaluation, children had spent an average of 7.01 years in their current placement (sd = 3.66, range 1–14). In 89.7% of the cases the children were still living at home. Nine children had moved out (at a mean age 14.2 years, sd = 1.85, 11–17), of whom 3 had done so as a result of a formal disruption. Two children were adopted from outside the UK, but now resided in the UK, and one child who was adopted from within the UK, had accessed CAMHS in the past, but was no longer UK resident.
The majority (66.0%) of children attended mainstream school, with 14.4% in specialist schools and the remaining 19.6% were: home educated (8.3%); in nursery provision (3.0%); or not in education (8.3%). Half of the adopters (50.0%) described the support they were currently receiving in educational settings as ‘not adequate’ to meet their child’s needs. A further 8.5% reported that whilst they were satisfied with their current level of support, previous support was inadequate.
Satisfaction measures and parental concerns
Satisfaction with services
All but 16 cases reported having attended CAMHS (N = 82, 83.6% of the sample). Of the 16 who had not accessed CAMHS, thirteen parents had wanted a service (81.2%). The three parents who had not sought a referral had children under 8 years old at the time of the assessment. Of the thirteen declined a referral, 12 (92.3%) were dissatisfied with the reasons given and of the nine offered alternatives to CAMHS, only one (11.1%) considered the alternative satisfactory.
Figure 1(a) shows that the majority of respondents who had attended CAMHS were dissatisfied (Ns for each subsample in brackets), with 80.2% (N = 76) and 58.0% (N = 31) negative ratings for general and specialist CAMHS, respectively. Ratings were less negative for services provided by Local Authority post-adoption services (45.9%, N = 87) and Paediatrics & child health (33.6%, N = 57). Meanwhile, the support offered by Charity or peer support groups and Private adoption services was viewed much less negatively (4.3%, N = 46 and 7.6%, N = 13, respectively), albeit the latter from a much smaller sample. (a). Levels of adopted parents’ satisfaction with CAMHS and other agencies. (b) Levels of adopted parents’ satisfaction with the experience of CAMHS.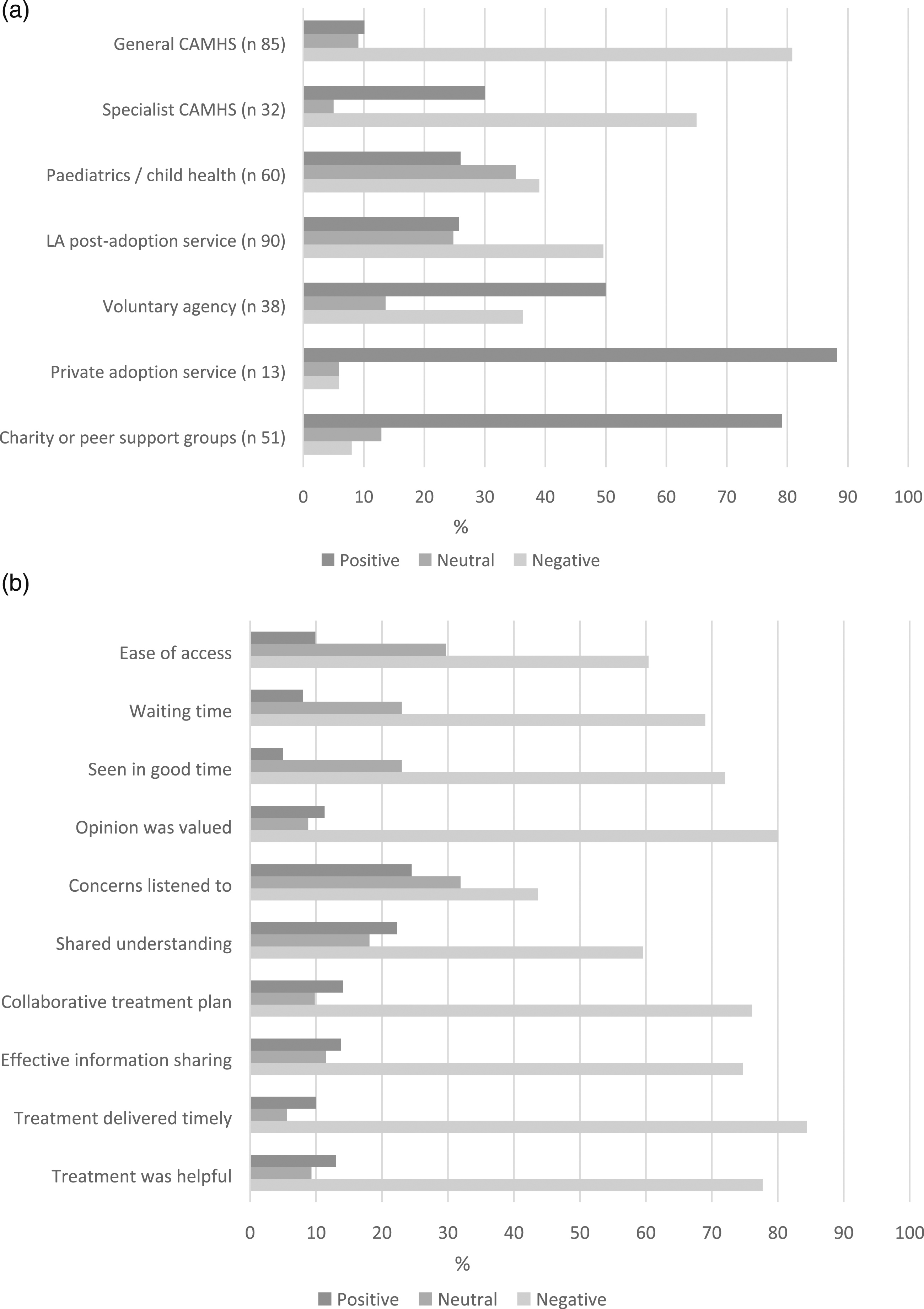
Parents’ experiences of CAMHS specifically were further explored in terms of accessing services; their satisfaction with the treatments offered; and the quality of the relationship (Figure 1(b)). In terms of access to CAMHS, families’ experiences were mostly negative. Ease of Access; Waiting Time; and Being Seen in Good Time were rated negatively by 60.4%, 69.0% and 72.0% of respondents, respectively. Satisfaction with CAMHS experiences was also overwhelmingly negative: 84.4% disagreed that Treatment was Delivered in a Timely Fashion; and 77.7% did not find Treatment was Helpful. In terms of collaborative relationships: 76.1% reported that treatment was not Collaborative; 80.1% did not feel their Opinion was Valued; levels of Information Sharing were poor (74.7%) and the development of a Shared Understanding (59.6%) was also primarily negative. The most positive aspect about CAMHS was that respondents’ Concerns were Listened to, albeit in a minority of cases (24.5%). According to the Friends and Family question, nearly three quarters (72.9%) of the sample would not recommend CAMHS services to friends and family for similar issues, and only 14.1% would be likely to do so.
Of the parents’ perceived barriers for accessing CAMHS, the highest rated barrier was issues around Funding (77.5%), closely followed by concerns that services were not adoption specific (68.3%).
Adoptive parents’ concerns at the point of adoption and currently
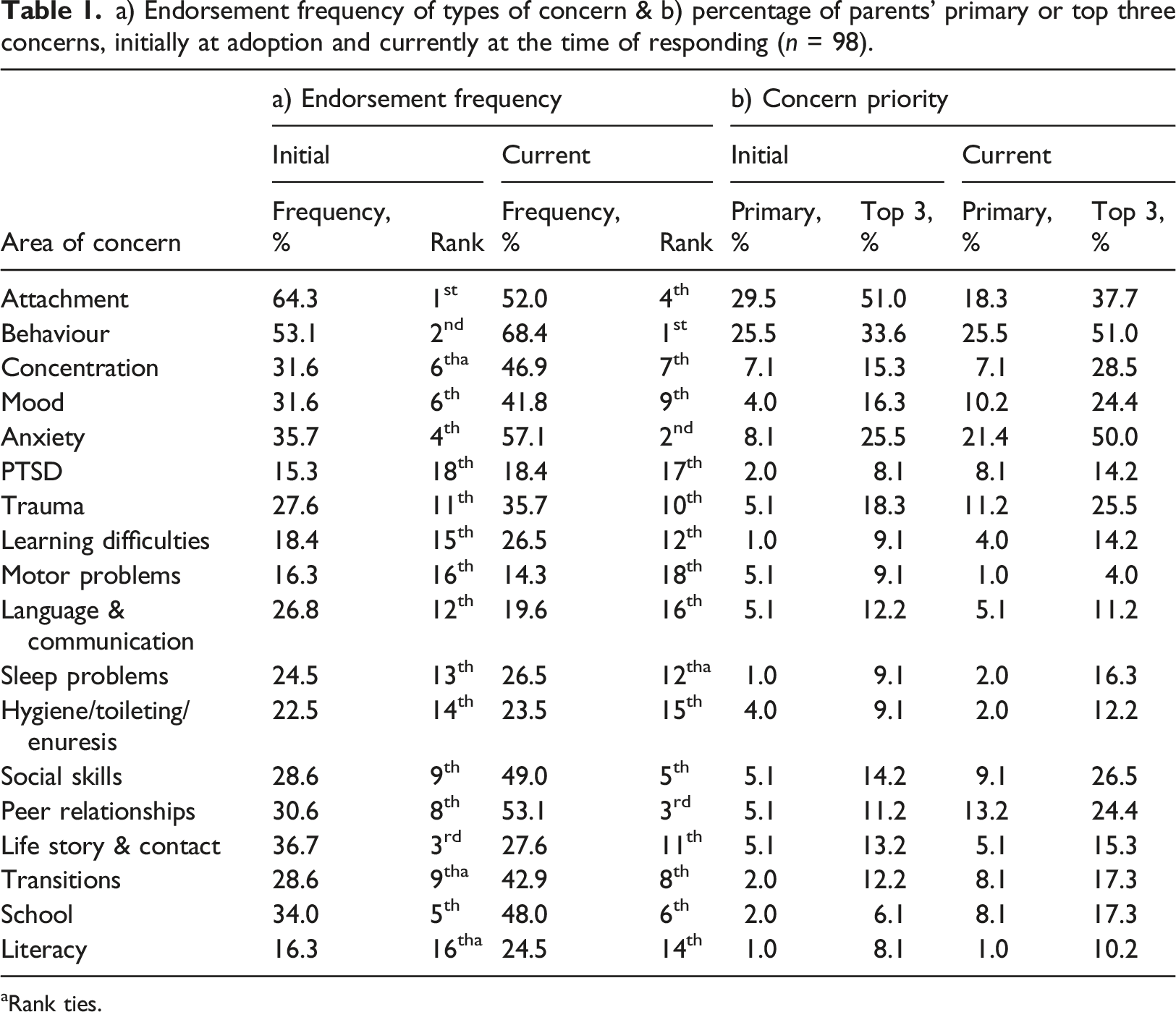
a) Endorsement frequency of types of concern & b) percentage of parents’ primary or top three concerns, initially at adoption and currently at the time of responding (n = 98).
aRank ties.
The most common initial concerns were for attachment (64.3%) and behaviour (53.1%). Regarding current concerns, behaviour was the most common concern having risen to just over two-thirds of the parents (68.4%) while attachment reduced to a concern for approximately half (52.0%), fourth overall. Indeed, concerns about attachment showed the greatest reduction over time for all concerns (−12.3%).
At the point of adoption parents reported initial concerns about mood and anxiety approximately a third of the time (31.6% and 35.7%, respectively), more than they were concerned about either specific post-traumatic stress disorder (15.3%) or generic trauma (27.6%). Regarding current concerns, both mood (41.8%) and anxiety (57.1%) had increased significantly, indeed anxiety showed the second largest increase over time (+21.4%) and was the second biggest current concern after behavioural problems. Concerns about PTSD stayed roughly the same over time (18.4%), but generic trauma increased to about a third of the respondents (35.7%), ranked 10th overall for current concerns. Issues with concentration/attention was a notable concern initially (31.6%), and this had risen to almost half the parents (46.9%) reporting current concerns (seventh rank).
Overall, there was a wide range of parental current concerns, including behaviour; anxiety; peer relationships; attachment; and social skills; but also for school issues; concentration/attention; transitions; mood; and generic trauma (respectively, first through 10th current concerns). The biggest increases in concerns over time were reported for social aspects such as peer relationships (from 30.6% to 53.1%, to third ranked current concern) and social skills (28.6%–49.0%, to fifth ranked current concern) as well as school (34.0%–48.0% sixth ranked) which were all reported to be current concerns for approximately half the parents.
Given the wide range of problems identified it is helpful to consider parental prioritisation of concerns, and the top 3 current concerns are presented (see Table 1). The standout issues were for behaviour and generic anxiety present in (51.0% and 50.0% top three concerns, respectively). The next most frequent occurrences within current parental top three concerns, were notably lower for attachment (37.7%); concentration/attention issues (28.5%); social skills (26.5%). Generic trauma issues were only reported in the top three concerns for 25.5% of families and PTSD for 14.2%.
Finally, it is possible that either age of the child or the duration spent in the adoptive home might have influenced the frequency of specific current concerns; for example, issues with social skills and peer relationships may have become more relevant for older children. Similarly, attachment concerns may have reduced as function of the time within the family. Therefore, current parental concerns were correlated with a) child age and b) time in the adoptive home. No significant associations (at p < .05) were found in any the 36 tests conducted [see Supplementary Table S1], indicating that neither child age nor absolute time in the family home predicted the level of specific concerns.
Discussion
The current study considers adoptive parents’ satisfaction with statutory child mental health services and their range of child mental health and well-being concerns in the UK context. There was an overwhelming picture of parental dissatisfaction with statutory services but they were especially negative about their experience of CAMHS. For instance, 4 in 5 parents expressed explicit dissatisfaction with generic CAMHS services and on a measure used across all NHS physical and mental health services, much lower than the very high levels of satisfaction with CAMHS nationally (over 80%) from a similar time period (NHS, 2016). Similarly, a study of service satisfaction across 41 CAMHS services in the UK with over 7,000 respondents reported the highest level of satisfaction of ‘certainly true’ between 70 to 80% of the time for most questions, e.g., “My views and worries were taken seriously”, rising to 92% about being ‘treated well’ (Brown et al., 2014). Thus, these adopted parents reported highly divergent levels of dissatisfaction with CAMHS compared with national indicators.
Of the 16 families who had not accessed CAMHS, the majority had tried but had been unsuccessful, and reported high levels of dissatisfaction about the reasons given for being declined services. Of those attending CAMHS, over three quarters of parents did not find the treatment helpful, which is clearly very negative, but also hard to compare with existing research as treatment outcomes are usually measured in relation to specific disorders or service models. The extent to which parents felt satisfied with elements of a collaborative approach were especially negative, with only a quarter satisfied their concerns had been listened to. By way of contrast, previous research with non-adoptive families has revealed over 90% of parents reported positive relationships with CAMHS staff (Brown et al., 2014). This particular disappointment with components of collaborative engagement and shared understanding is especially concerning and while the onus should be upon services to actively promote accessibility and effective engagement, it may also support the suggestion that adopters desire services that are not easily met within mainstream statutory services (e.g., Barth et al., 2005). In support of this, albeit based on a small sample in this study, there were much higher levels of satisfaction with the private and voluntary providers, who typically have a different narrative to CAMHS about adoption support, and parents also identified the lack of adoption-specific services as a barrier to accessing CAMHS in over two-thirds of cases.
A wide range of concerns were identified by parents at the point of placement and currently. Moreover, many parents reported multiple concerns, the mean number at placement being over five, rising to nearly seven concerns at the current time. Children who have been exposed to maltreatment and neglect are likely to have both high rates of common mental health disorders, but also high rates of comorbidity (Coughlan et al., 2022; Haugaard, 2004). Many of the concerns that were identified were issues that could normally fall under the remit of CAMHS provision (behaviour problems, anxiety, mood, attention and concentration, PTSD, learning disability etc.), therefore the high rates of dissatisfaction cannot be easily explained by parents seeking help for concerns that were not part of normal CAMHS service. International adoption research also reports elevations of concerns about common mental health problems including ADHD, behavioural problems, anxiety disorders and depression (Behle & Pinquart, 2016).
In addition to the wide variety of concerns there were also notable changes in concerns over time, and this would likely pose problems for services offering post-adoption support, not least because there was no evidence that either child age nor time in the family home predicted the type of concern. To cover all possibilities, services would need to offer a wide range of assessments and treatments, but also be responsive to different concerns at different times, and thus open to longitudinal assessment and review, an approach that has been recommended for nearly two decades as best practice for assessing children with maltreatment histories (e.g., Chaffin et al., 2006; Hiller et al., 2023). The challenges for service delivery to adequately meet the changing needs of this complex set of young people may be driving some of the dissatisfaction with services, but this needs further exploration.
The overall number of concerns increased over time, and it was notable that some non-diagnostic terms such as unspecified anxiety, generic trauma, as well as social skills, school problems and peer relationships showed the biggest increases, and were amongst the most frequently expressed concerns. One possibility is that the increase in generic concerns may reflect secondary functional impacts derived from primary disorders, i.e., that the earlier concerns have not gone away, but that their impact on functioning becomes more important for families. However, such generic, non-disorder based concerns may not be an easy fit with standard CAMHS care pathways, and so a service that is responsive to adoptive parents’ concerns would need to be open to deriving treatment goals that reflect this wide-ranging set of concerns. In so doing some of the issues around the low levels of effective collaboration, engagement and shared understanding might also be addressed. Such an approach could still use evidence-based approaches of course, but more tailoring of the goals to parental concerns is likely to increase collaboration and engagement.
Adoption provision is frequently organised around themes of attachment and trauma, yet attachment and trauma were not the standout concerns for parents seeking support, occurring in approximately a third and a quarter of parents’ top three current concerns, respectively. Instead, behavioural issues and anxiety were the most frequent issues in the current top three parental concerns, each of them being reported by approximately half of the parents. Indeed, the main findings here are of a very wide range of parental concerns, many more than just attachment and trauma, but ones which also change over time and extend beyond frank mental health issues into school, and social relationships.
In terms of study limitations, the sample was self-selected, and thus cannot be assumed to be representative of all the concerns about mental health and well-being of adoptive parents’ who have had contact with CAMHS. However, we know very little about the mental health needs of children adopted in the UK, because this has never been systematically collected, but if available it would be possible to compare the range of issues and concerns described here with an epidemiological sample, similar to the data for UK CLA collected over 20 years ago (Ford et al., 2007). Indeed, the lack of epidemiological data for the mental health and well-being needs of adopted children makes service delivery and innovations difficult to implement and to evaluate. However, the sample demographics presented here are similar to the Adoption UK ‘State of the Nation’ (Adoption UK, 2019) as well recent large samples of UK adopters (e.g., Neil et al., 2020), which suggest this sample is not a profoundly different group from UK adopters in general. What we have shown is that for adoptive parents who had had contact with CAMHS, they had significant mental health concerns about their children, their concerns were wide-ranging, and certainly not restricted only to issues of attachment and trauma, and when these families had accessed CAMHS they had been deeply dissatisfied.
The initial parental concerns were accessed retrospectively, and therefore may be subject to recall bias. However, there were changes in perceptions of current concerns and the contemporaneous retrospective accounts of initial concerns, suggesting parents were recognizing notable changes over time. A further potential confound is that the children had been living with their parents for varying amounts of time, and therefore for some parents there was a greater distance between the retrospective recall of initial concerns than with others. Ideally, these concerns would have been measured at the point of adoption and then followed up at specific time points. Finally, a count of number of concerns does not take into account the possibility of increasing severity focused on a smaller number of concerns, including more global social impairments.
A further possible limitation for this self-selected sample is the risk of bias towards those who have had negative experiences of CAMHS. One solution for this going forward, would be to ensure that services routinely collect satisfaction data for children who are adopted (or who are in the care system). This would help to monitor service quality regarding the overall level of satisfaction for these vulnerable children, and to monitor levels of satisfaction compared to those in birth families, assuming adopted versus non-adoptive cohorts were reliably identified. Finally, missing from this study are the voices of the young people themselves, especially as ideographic descriptions of what children and young people want has been shown to improve both their engagement with mental health services and treatment response (Tollefsen et al., 2020).
Since this survey was conducted, some of the statutory provisions in the UK for adopted children’s support, including mental health have changed, most notably in England with the introduction of the Adoption Support Fund (ASF). The fund places an explicit emphasis on providing support for attachment and trauma, yet as noted above, these were not the majority concerns for parents in the current study. So, while potentially increasing access to services for adopted children, the target of the fund may not address the majority of the parental concerns identified here.
Several evaluations of the ASF in England have been conducted (Department for Education, 2022a), and a survey-based evaluation has been published reporting data on the presenting issues for 1,008 children and young people aged between zero and 18 years, accessing the ASF in England between 2018 and 2021 (899 adopted children and 109 on an alternative permanency arrangements). The report indicates that the vast majority had significant mental health issues, for example, 84% over the age of 5 had problems within the clinical range on the CBCL and concerningly, 33% of the ASF baseline evaluation sample reported that their child ‘sometimes or often’ self-harmed or attempted suicide (Department for Education, 2021). The most common problems for over 5s, indexed by borderline or clinical levels of problems on the eight CBCL Syndrome scales included aggression; anxious/depressed, attention problems and thought problems (all reported in approximately three quarters of the sample) and an overall mean of 4.43 syndromes for the sample (unfortunately, no range or standard deviations can be calculated from the published data). These figures align with the kinds of concerns parents identified in the current study, as well as the observation of co-occurrence of multiple problem domains (albeit with the addition of thought problems i.e., psychosis related issues, in the evaluation as one of the eight syndromes reported in the CBCL data – something the parents in the current study had not reported as concerns).
Another set of evaluations presented qualitative studies with social workers and commissioners and revealed concerns that CAMHS is increasingly withdrawing services from adopted children because adoptive families in England would have the opportunity to access services via the ASF instead (Department for Education, 2022b), which would suggest an unintended consequence of the ASF is an exacerbation of the barriers adoptive families could face accessing CAMHS. It is worth noting that the ASF was set up to increase post-adoption service provision from the private and voluntary sector, and the current study suggests that prior to the introduction of the ASF parents were more satisfied with private and voluntary services than statutory services (although the numbers accessing these services in the current study were much smaller than for CAMHS). Therefore, a relative reduction in numbers accessing CAMHS would be expected, especially as the majority of CAMHS services would be unable to use the ASF funding mechanisms to accept referrals. Nonetheless, the qualitative evaluations suggest that the increased barriers to accessing CAMHS were perceived as a problem for social work commissioners.
Overall, the evaluations of the ASF so far supports the findings here of high levels of wide-ranging mental health needs that could traditionally have been met through statutory CAMHS services, even while the barriers for accessing these services may have inadvertently increased. Unfortunately, the instruments used in the evaluations were unable to identify issues specifically to do with trauma or attachment, so it is not possible to compare levels of difficulties in the evaluation sample with the concerns raised by parents in the current study in these domains, nor indeed to address the extent to which the ASF has been successful targeting attachment and trauma issues specifically.
Regarding implications for practice, parental concerns about attachment issues in the current study were high, even though there is little research to suggest that attachment problems are the primary mental health issue for adopted children. Indeed, where research has been conducted on looked after or maltreated children, the evidence suggests a wide range of associated mental health disorders, (e.g., Coughlan et al., 2022; Ford et al., 2007; McLaughlin et al., 2020) not at all restricted to attachment or trauma related issues. One question that follows from this is what adoptive parents meant by “attachment concerns”? It is likely to vary considerably, as we already know that practitioners vary considerably in how they conceptualise what attachment means applied to clinical settings (Beckwith et al., 2022), but also regarding what the appropriate services are for attachment problems (Woolgar & Baldock, 2015; Wright et al., 2023). It seems reasonable to expect that adopters’ own understanding of attachment concerns, interacting with the variation in understanding present in clinical services is likely to lead to significant mismatches between parental expectations around attachment concerns, and the services offered, something that has been hypothesised previously as driving adopters’ dissatisfaction; namely that therapists blame the parents for the current problems and, conversely adoptive parents have difficulties trusting therapists who do not take the child’s history into account (Barth et al., 2005).
Secondly, given the importance of trauma approaches in organising much post-adoption support, it is notable that trauma was a relatively low-level concern for parents compared to a wide range of other issues. This is consistent with recent research on UK adoptees in which less than a fifth of children had clinical or borderline clinical post-traumatic stress symptoms (Anthony et al., 2022). Again, we know very little about how adopters understand trauma, nor indeed how practitioners conceptualise trauma in relation to adoption or care experienced children, but it seems likely that a similar issue of notable variations in understanding apply here as for attachment (e.g., McGuire et al., 2022), and there has been concern that ‘concept creep’ has applied especially to the construct of trauma (Baes et al., 2023) and that has led to a psychiatrization of everyday experiences (Haslam et al., 2021). In the absence of epidemiological data on mental health issues, nor knowing how the various stakeholders, including families and young people, conceptualise these issues, then high levels of dissatisfaction with shared understanding and collaborative goals are likely to persist.
A first epidemiological study of UK adopted children’s mental health needs is overdue, especially given the investment in mental health support that has already been committed in the absence of knowledge about the extent or form of the problems. Such a study should explore the mental health conditions used in many CAMHS services, but also go beyond frank psychiatric disorders and include questions about broader concerns that adoptive parents note using terms and concepts that makes sense to them (e.g., social skills, peer relationships and school). Furthermore, a mixed method study could assess the extent to which parental concerns map onto the standard problem-conceptualisations informing care pathways and the extent to which adoptive parents’ experience of CAMHS has been collaborative and based on a shared understanding, building on initial work that has sought to understand how adoptive parents and their children understand mental health issues in CAMHS and the importance of negotiating an agreed understanding of the issues (O’Reilly et al., 2016). A third study of practitioner beliefs about mental health support for adopted children, to include not only CAMHS practitioners but also independent providers, social workers and education staff could help bridge the various divergent narratives, e.g., between standard mental health service provision and adoption-specific social care commissioning. Based on the wide range of parental concerns, it seems likely that similar presentations are classified differently in different contexts, and a thorough understanding of these overlaps and any differences in narratives could improve collaboration between services and promote engagement with families.
Conclusions
Adoptive parents expressed very high levels of dissatisfaction with mental health services, although many of the concerns they wanted addressed overlapped with the typical remit of mental health services. Despite the overlap, parents were dissatisfied with the shared understanding of problems and the majority reported concerns about a lack of an adoption-specific focus in services. Research is needed to characterise the range of mental health disorders in adopted children, alongside research to understand parental, young person and professional conceptualisations of problems, especially for attachment and trauma, to better fit family concerns with service models and promote collaborative practice and shared understanding throughout the network.
Supplemental Material
Supplemental Material - Adoptive parents’ satisfaction with child and adolescent mental services and their mental health concerns over time: A question of fit?
Supplemental Material for Adoptive parents’ satisfaction with child and adolescent mental services and their mental health concerns over time: A question of fit? by Matt Woolgar, Carmen Pinto and Rafael A. González in Developmental Child Welfare.
Supplemental Material
Supplemental Material - Adoptive parents’ satisfaction with child and adolescent mental services and their mental health concerns over time: A question of fit?
Supplemental Material for Adoptive parents’ satisfaction with child and adolescent mental services and their mental health concerns over time: A question of fit? by Matt Woolgar, Carmen Pinto and Rafael A. González in Developmental Child Welfare.
Footnotes
Acknowledgements
The authors wish to thank Adoption UK for their input in creating the survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.