
Abstract
The importance of trauma-informed care has recently been recognised more greatly across the United Kingdom and has led to increased efforts to provide training to staff across a range of public sectors. Evaluation of training interventions is often limited to outcomes of staff knowledge and confidence. The current study aimed to evaluate the impact of an attachment- and trauma-informed training intervention for social work professionals on how they understand the young people they work with. 29 social work professionals attended training online and face-to-face. A pre-post design was utilised, with intervention and waiting-for-training groups, evaluating outcomes of professionals’ expressed emotion (EE), reflective functioning (RF), and attachment-informed stance using 5 Minute Speech Samples (FMSS), alongside attitudes towards trauma-informed care (ARTIC) and knowledge, confidence and worries regarding trauma-informed care. A novel Attachment-Informed FMSS coding system was developed and piloted showing good inter-rater and code-recode reliability. Significant interaction effects were found for knowledge (ηp2 = .623, p = <.001), confidence (ηp2 = .281, p = .003) and EE Warmth (ηp2 = .172, p = .025), significant increases were seen pre-to post-intervention for training group compared to waiting-for-training group, and training group had a significant increase in ARTIC scores pre-to post-intervention (r = .412, p = .02). Significant effects of time were found for RF and attachment-informed stance but no interaction effect was found. Training outcomes may not have the intended effect of increasing professionals’ ability to be reflective or attachment-informed but still provide positive changes in knowledge, confidence and self-reported attitudes.
Introduction
Many health and social care professionals work with traumatised young people to support their social and emotional development and manage the impact of their traumatic experiences. It is important that their work is grounded in psychological theory and evidence-based practice to ensure effective support is provided and to minimise the risk of young people being re-traumatised by services (Woodside-Jiron et al., 2019). Attachment theory and models of developmental trauma can help professionals to conceptualise the approach they take to their work with traumatised young people and their families.
Attachment theory seeks to explain the nature and function of a child’s bond to their caregiver and suggests that variations in attachment styles and behaviour are a result of caregivers’ sensitivity to the child’s attachment cues and communication, and that attachment behaviour can be transmitted across generations (Fearon & Roisman, 2017). The theory proposes that caregiver sensitivity, responsiveness and attunement are key to providing the child with a secure base from which to explore the world which contributes to the development of personality and aspects of affect regulation (Fitton, 2012).
Models of developmental trauma suggest that children who are exposed to multiple and chronic interpersonal trauma, particularly when traumas occur in the family environment, are at risk of developing a range of functional and mental health problems including difficulties in attachment and interpersonal relationships (Kisiel et al., 2014). Looked After Children (LAC) are likely to be at greater risk of attachment difficulties as they have often experienced prolonged developmental trauma and have further repeated disruptions to attachments through living in multiple foster placements (Archer & Burnell, 2003). Professional relationships play an important role in the experience and recovery of individuals with developmental trauma and attachment difficulties as the qualities of these relationships have the power to create positive change in a child’s physical and emotional health, or to create negative perceptions of services as ‘demeaning’ or disrespectful which have the potential to lead to further traumatisation (De Boer & Coady, 2006). The development of trust is an important factor within these relationships and research suggests that young people are initial suspicious of professionals but value relationships in which they are seen as whole human being rather than being treated in relation to one problem or disorder (Hill, 1999).
The implementation of trauma-informed care models in foster care and other out-of-home care settings has been shown to improve behavioural and mental health outcomes for LAC (Bailey et al., 2019) and may be a beneficial approach to implement in the wider systems supporting LAC such as social services.
Working with individuals who have experienced disrupted attachments and complex trauma can be challenging for service providers, particularly at times when individuals display behaviours that can evoke unhelpful emotional responses in those around them, such as parents, carers, or professionals. These unhelpful reactions can at times present as non-reflective interpretations of the individuals’ behaviours, which can in turn exacerbate the individuals’ difficulties (Chandler, 2008).
Attachment- and trauma-informed training programmes often aim to increase a person’s understanding of individuals’ behaviours, creating more balanced and less emotionally-driven responses from those working with the individual. However, one of the challenges in conducting research on psychologically-informed staff training interventions is finding appropriate measures that adequately capture relevant change, and studies have attempted to achieve this by measuring a range of different related constructs. Recent studies have explored staff’s knowledge and confidence in trauma-informed approaches, and their attitudes towards trauma inquiry and response (Purtle, 2020). Some training programmes have also measured staff’s levels of empathy (Little & Maunder, 2022) and emotional control (Rose et al., 2019) which are often linked to a secondary aim of improving the relationships between clients and services, creating a greater sense of person-centred working and compassionate care (Purtle, 2020).
Preliminary evidence for the impact of training suggests that providing attachment- and trauma-informed training to education staff in pupil referral units can increase staff’s perceptions of their knowledge and confidence, whilst reducing their worries, about working in a trauma- and attachment-informed way with children and young people (Greenhalgh et al., 2020). This training was delivered by a psychology-led service and consisted of a two-day training package exploring attachment and theory and concepts from Dyadic Developmental Psychotherapy (DDP – a therapeutic approach based on attachment theory and understanding the impact of developmental trauma), followed by six skills development sessions incorporating case formulation into practice. The initial two-day training package is designed to provide education around attachment theory and its application to understanding children’s behaviours, whilst the skills development sessions are designed to foster reflective practice regarding these concepts and support the application of theory to clinical practice using case discussions. Whilst this research suggested a positive impact on staff’s knowledge, confidence and worries regarding trauma- and attachment-informed working, the study’s conclusions are limited by the lack of control group for comparison, and the lack of any clear evidence that this impact translates to a change in the relationship to, and approaches to working with, service users.
One measurable construct that has been linked to observed changes in child-adult interactions and relationships is Expressed Emotion (Weston et al., 2017), which can be defined as a caregiver’s attitude towards an individual as reflected by comments made about the individual, and may include expressions of hostility or warmth towards the individual. This construct is most commonly measured using 5 Minute Speech Samples (FMSS; Sher-Censor, 2015) which consist of an individual speaking for 5 minutes about a child or young person and their relationship with them, and is then coded for specific constructs of interest, such as Expressed Emotion, according to the relevant coding manuals. The FMSS provides advantages over other data collection approaches as it reduces response biases through the use of a general prompt to acquire open-ended responses, rather than using more directive questions which may illicit socially desirable responses.
FMSS coding of Expressed Emotion (EE) has most commonly been used in research with parents or families, however recent research has extended its use to measure professional groups including prison staff (Moore et al., 2011) and teachers (McGrath & Van Bergen, 2017).
Whilst EE is the most commonly measured construct using FMSS, coding systems have been developed to measure other constructs of interest, including Reflective Functioning (Fonagy et al., 1998). Reflective Functioning (RF) explores the ability to recognise or describe mental states such as emotions, thoughts, and beliefs, as well as the ability to relate mental states to behaviour within the self and within others. RF, as measured through the FMSS coding system, has been utilised in research exploring the impact of training for foster and adoptive parents (Bammens et al., 2015) and perceptions of mental health professionals during their professional training (Trowell et al., 2008).
The importance of a foundational knowledge in attachment for social care professionals was highlighted in the Munro (2011) Review of Child Protection, however there has been debate as to the clinical usefulness of the taught curriculum within current social care training programs, as some argue that the dialogue between attachment researchers and practitioners has not always been clear, leading to misunderstandings and misapplication of the use of attachment-informed practice (Foster et al., 2025). Despite the recent rise in provision of attachment- and trauma-training for staff across many public sector services (Welsh Government, 2021), there is currently a lack of appropriate tools to measure the intended aims of this these training programmes, particularly staff’s ability to take an attachment-informed stance in understanding the emotional and behavioural presentations of the young people they work with. The use of a FMSS coding system to identify and quantify this ability within staff could provide new opportunities to understand staff perceptions in a way which may relate more directly to their interactions with service users, and may provide a new tool in which to evaluate the impact of attachment and trauma training packages.
The contribution of attachment theory to therapeutic approaches in psychological services has been well-researched and documented (Cassidy et al., 2013), however the impact of attachment- and trauma-informed training of staff in health and social care teams has not been thoroughly explored within current research literature. The current study aims to build upon previous work by Greenhalgh et al. (2020) to explore the impact of a similar training programme which has been adapted for child social workers. The current study aims to address some of the limitations of the previous research by incorporating a waiting-for-training group, and using the FMSS to measure staff’s levels of EE and RF pre- and post-training. The study also aims to address a gap in the current available literature by developing and piloting a new FMSS coding system to measure staff’s ability to take an attachment-informed stance to understanding the young people they work with.
Methods
Participants
Participants were recruited from teams who had been identified for attachment- and trauma-informed training by a local NHS service. Teams were included if they met the following criteria: (1) a local authority team, (2) working with children and young people up to the age of 25, and (3) had been invited to attend the training between January 2022 and April 2023. Recruitment was conducted through meetings with Team Managers of identified teams in which they were provided with information about the research and given an opportunity to ask questions. If the Team Manager provided consent, individual team members were emailed by the Project Lead to invite them to participate.
115 social work professionals from 11 teams working across the local area were invited to participate in the research. Two additional teams were identified but were not involved in the research due to their Team Managers not providing a response to confirm their consent to recruit their team members.
Of the 115 professionals invited to participate, 36 agreed and completed at least one interview, however three participants did not complete the questionnaire measures at Time Point 1 or the interview at Time Point 2, two participants did not complete the interview at Time Point 2, and two participants did not complete the questionnaire measures at Time Point 2 (19.4% attrition rate). Over a 16 month recruitment period, 29 participants completed all interviews and questionnaire measures at both time points and were included within the data analysis.
Procedures
Ethical approval was granted by the local Health Board Research and Development Department and the local university School of Psychology Research Ethics Committee.
Teams were allocated to one of two possible conditions: training, or waiting-for-training, depending on the planned dates of training and how these fell within the data collection period. Due to the nature of the training provision schedule and availability of social care teams, random allocation to training or waiting-for-training conditions was not possible, therefore any causal inference within the data analysis maybe weakened. Teams scheduled to attend the training were invited to participate as part of the training group. Teams who were identified to receive the training but had yet to schedule training dates were invited to participate as part of the waiting-for-training group. All teams within the waiting-for-training condition would receive their training on their planned dates regardless of their choice to participate in the research or not.
Participants were contacted via email and provided with a Participant Information Sheet and Confidential GDPR Consent Form. Prior to interviews and completion of questionnaire measures at both time points participants were asked to confirm that they had read the Participant Information Sheet and Confidential GDPR Consent Form, that they had been given the opportunity to ask any questions or remove themselves from the study, and that they were consenting to take part in the research. Brief interviews were conducted over the telephone and Microsoft Teams to collect 5 Minute Speech Samples (FMSS) and participants were provided with a website link to complete questionnaire measures anonymously online. Interviews and questionnaires were completed at two time points. For those within the training condition: pre-training (Time Point 1) - approximately one week prior to the first training day & post-training (Time Point 2) - approximately one week after their second training day). For those within the waiting-for-training condition: Time Point 1 was the time of their first interview and Time Point 2 was approximately two weeks later. Participants were offered entry into a £50 prize draw for completion of all questionnaire measures and interviews at both time points. The prize winner was drawn through a random number generator at the end of the data collection period.
Training program
The training program was designed and delivered by a local NHS service. The service described within this research sits within a Child and Family Psychology and Therapies Service and has a brief to improve outcomes for children and young people impacted by disrupted attachments and developmental trauma. The service therefore works with partners in health, social services, education, youth offending housing and any other services and agencies who routinely work with vulnerable children and families. The central ethos of the service is that the most important relationships for children are those closest to them and those they see in their day to day lives. The service therefore seeks to increase awareness and understanding of attachment and trauma with a particular emphasis on developing a shared language and approach across agencies and services within the local community. This is achieved through upskilling and supporting all the people with most contact with children in their day to day lives. More specifically, the current research focused on two particular elements of the service: the delivery of specialist attachment and trauma informed training by qualified clinical psychologists; the subsequent follow-up skill development sessions (SDSs) provided approximately monthly for the 6 months following training where trainees are given further opportunities for consultation and learning around how the skills apply to their work context.
Trauma informed training was delivered both in-person and online depending on the needs of the team. Each training package was delivered over the course of two full days and covered five main themes with the aim to improve knowledge and confidence in the use of evidence-based skills, whilst reducing worries around working with children and young people who have experienced trauma or disrupted attachments: (1) An overview of attachment theory including its history and development (2) Psycho-education and research evidence around the impact of developmental trauma on the body and brain of developing children. (3) Applying this knowledge to understanding children’s behavioural presentations (4) Supporting professional practice through the use of attachment-informed interventions and Dyadic Developmental Psychotherapy (DDP) principles (5) Promoting discussions around self-care within teams.
Ongoing support to embed knowledge into practice was then provided to teams following training via six SDSs delivered monthly. It was not possible within the scope of this study to include a further data collection time point to capture the impact of these SDSs.
Measures
Questionnaire measures
Two questionnaire measures were collected pre- and post-training as part of the service’s standard procedure. Participants within the training group completed the questionnaires at the beginning and end of their training. Participants within the waiting-for-training group were invited to complete the questionnaires prior to their first interview and following their second interview. (1) Knowledge, Confidence and Worries Questionnaire (KCW). The KCW was adapted by the service from a previous trauma-informed training evaluation questionnaire (Walters et al., 2016), measuring three subscales related to providing trauma- and attachment-informed care: knowledge, confidence, and worries. The adapted questionnaire consists of ten questions in the knowledge subscale, four questions in the confidence subscale, and six questions in the worries subscale, with 10-point Likert scales to rate each item ranging from 0 (strongly disagree) to 10 (strongly agree). For example, ‘I have an understanding of what might influence someone to develop specific attachment strategies’. (2) Attitudes Relating to Trauma-Informed Care (ARTIC-10). The ARTIC-10 (Baker et al., 2016) is a 10-item questionnaire that provides a single score of professionals’ attitudes towards trauma-informed care (TIC) that has been shown to have good reliability and validity (Baker et al., 2021). This scale uses a 7-point Likert scale expressing an individual’s alignment between a ‘favourable’ or ‘unfavourable’ attitude towards TIC. Higher scores indicate more alignment towards ‘favourable’ attitudes.
Five minute speech sample (FMSS)
Each professional who chose to participate in the interviews provided a FMSS (Magaña et al., 1986). This involved being given a standardised prompt to speak about a young person they worked with for 5 minutes without any interruption: ‘For the next 5 minutes I would like you describe X to me, what is X like?’. Further prompts were utilised if the participant was silent for more than 30 seconds such as ‘How would you describe X’s personality of temperament?’. A protocol for acquiring speech samples was developed to maintain consistency between interviews. The FMSS for each participant was recorded, transcribed, and coded to measure the variables of interest in the professional-child relationship. The young people discussed were in a range of placements including children’s homes, adoptive placements, foster placements, and living with parents. A sample of FMSS (86%) were also coded by two additional researchers with experience of FMSS coding and inter-reliability was calculated for each of the three coding systems used: (1) Expressed Emotion (EE). The expressed emotion coding system (Caspi et al., 2004) was utilised to measure how often professionals were using Positive Comments and Negative Comments when speaking about young people, along with ratings of their Warmth and Dissatisfaction towards the young people. Using this system Positive Comments and Negative Comments are measured by frequency counts. Dissatisfaction is measured on a 6-point rating scale ranging from 0 to 5, with higher scores capturing a stronger dislike towards the young person and a greater desire for them to change. Warmth is measured on a similar 6-point rating scale from 0 to 5, with higher scores capturing greater sympathy and/or empathy towards the young person and greater enjoyment of being with them. In the present study, inter-rater reliability analysis showed a good level of agreement for Negative Comments (ICC = .82, p < .001), and an excellent level of agreement for Positive Comments (ICC = .92, p < .001), Warmth (ICC = .92, p < .001) and Dissatisfaction (ICC = .90, p < .001). (2) Reflective Functioning (RF). The Reflective Functioning Five-Minute Speech Sample (RF-FMSS; Adkins & Fonagy, 2019) coding system was utilised to measure professionals’ ability to recognise and describe mental states and relate these states to the behaviour of themselves and the young people they work with. The coding system uses a 6-point rating scale ranging from −1 (negative RF) to 9 (full or exceptional RF). Inter-rater reliability analysis showed a good level of agreement (ICC = .81, p < .001). (3) Attachment-Informed (AI). One of the intended outcomes of the training program was for professionals to be able to take a more attachment-informed stance to understanding the presentations of the young people they work with. However, there did not appear to be a measurement tool in the existing literature to capture this outcome. A novel FMSS coding system was therefore developed and piloted for use within this study. The initial coding system was developed through consultation with Clinical Psychologists within the service delivering the training; views were provided on the elements of speech they would expect to be present if a professional were speaking in an attachment-informed way, and which elements may be present if they were not attachment-informed. These elements were then placed within a 5-point rating system from 0 (no attachment-informed stance) to 4 (highly attachment-informed stance), which was reviewed by clinical and academic psychologists with expertise in attachment, trauma, DDP, and use of the FMSS and feedback was incorporated into the coding system. Each point on the scale was given its own criteria. Examples of guidance for ratings of 0 and 4 are available in Appendix A
Data analysis plan
An a priori power analysis was conducted using G*Power 3.1 using a medium effect size based on similar prior research (Adkins et al., 2022). A minimum sample size of 34 was required to achieve a power of .80, however due to difficulties in recruitment this target was not reached. Data analysis was completed using IBM SPSS version 27. There was no missing data with the dataset. Group demographic variables were compared using Fisher’s Exact Test for categorical variables, and independent samples t-tests for continuous data. Mixed ANOVAs were utilised to test for main effects of time and group and any interaction effects. Significant interaction effects were followed up by tests of simple main effects. Where assumptions were not adequately met for ANOVAs, Wilcoxon Signed Rank Tests were used as a non-parametric alternative. Effect sizes are interpreted as small, medium, or large according to proposed guidelines (Cohen, 1988).
Results
Descriptive statistics
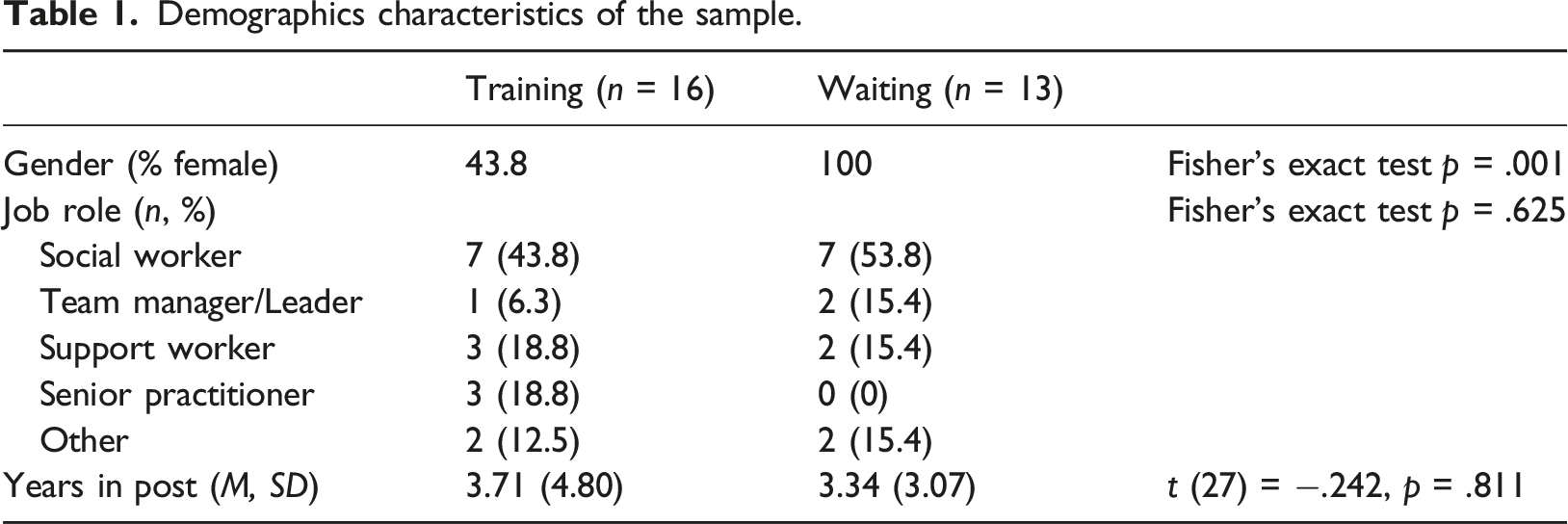
Demographics characteristics of the sample.
Training intervention outcomes
FMSS means, standard deviations, and ANOVA results.
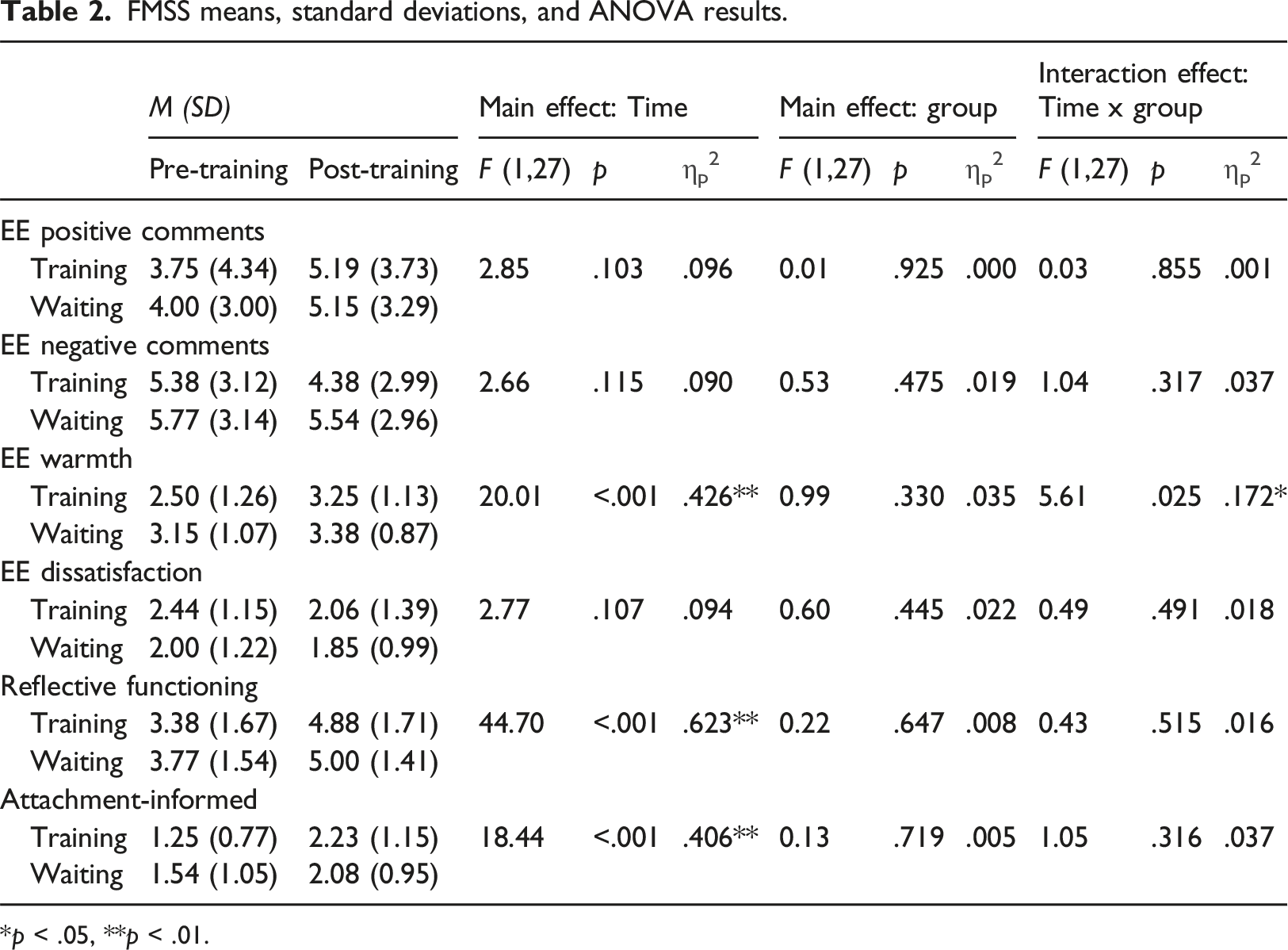
*p < .05, **p < .01.
Questionnaire means, standard deviations, ANOVA and wilcoxon signed rank test results.
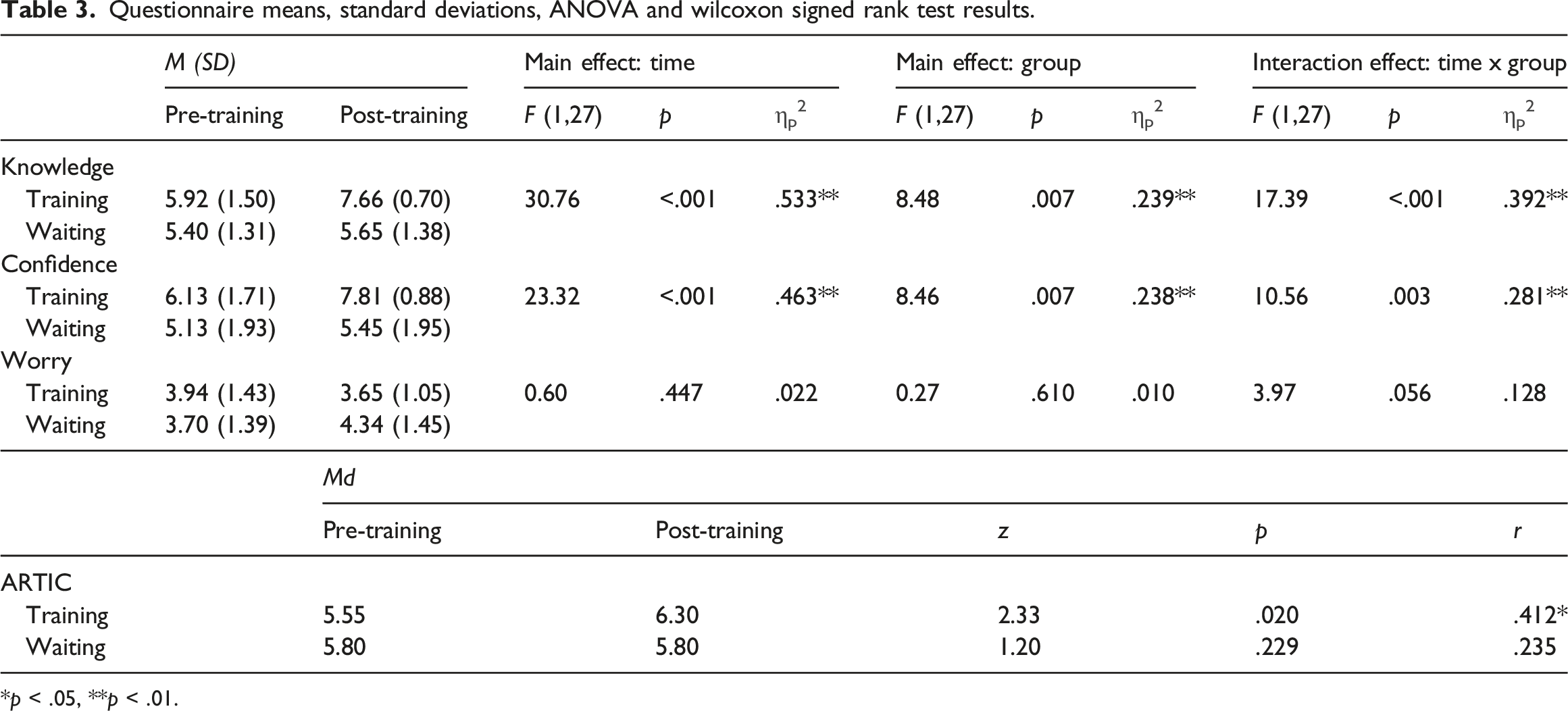
*p < .05, **p < .01.
EE components
No significant main or interaction effects were found for Positive Comments, Negative Comments, or Dissatisfaction. A significant main effect of time, but not group, and a significant interaction effect were found for Warmth with large effect sizes. Follow-up tests revealed that the significant difference was attributable to the training group who displayed higher levels of warmth post-training, with a large effect size (training: F (1,15) = 27.00, p < .001, ηp2 = .643 95%CI = .442–1.058); waiting: F (1,12) = 1.93, p = .190, ηp2 = .138, 95%CI = −.131–.593). For example, one participant’s warmth changed significantly pre-to-post training: “there’s the barriers that she’s putting up for herself and we are trying to knock them down, but she just won’t knock them down” (pre-training); “she’s really arty and like creative and stuff where she’s just brilliant… I’d like to think she is quite deep… quite mindful” (post-training).
Reflective functioning
A significant main effect of time was found for Reflective Functioning, with a large effect size. Main effect of group and interaction effect were found to be non-significant.
Attachment-informed stance
A significant main effect of time was found for Attachment-Informed Stance, with a large effect size. Main effect of group and interaction effect were found to be non-significant. For example, one participant showed a significant increase in attachment-informed language from Time Point 1 to Time Point 2: “she kicks off quite a lot over numerous things… she just flips” (Time Point 1); “she sometimes get frustrated and doesn’t know how to manage that and I think sometimes mum and dad’s reaction to that is not always the best way” (Time Point 2).
Knowledge
Significant main effects of time and group, and a significant interaction effect were found for Knowledge, with large effect sizes. Follow-up tests revealed a significant change in scores across time for the training group, but not the waiting-for-training group (training: F (1,15) = 37.47, p < .001, ηp2 = .714, 95%CI = 1.132 – 2.343; waiting: F (1,12) = 1.74, p = .212, ηp2 = .127, 95%CI = −.160 – .653), and there was a significant difference between group scores at the post-training time point, with the training group achieving higher knowledge scores post-training than the wait-for-training group (pre: F (1,27) = .930, p = .344, ηp2 = .033, 95%CI = -.577 – 1.599; post: F (1,27) = 25.79, p < .001, ηp2 = .489, 95%CI = 1.193 – 2.811), these differences had large effect sizes.
Confidence
Significant main effects of time and group, and a significant interaction effect were found for Confidence, with large effect sizes. Follow-up tests revealed a significant change in scores across time for the training group, but not the waiting-for-training group (training: F (1,15) = 28.92, p < .001, ηp2 = .658, 95%CI = 1.009 – 2.335; waiting: F (1,12) = 1.67, p = .220, ηp2 = .122, 95%CI = −.224 - .878), and there was a significant difference between group scores at the post-training time point, with the training group achieving higher confidence scores post-training than the training group (pre: F (1,27) = 2.21, p = .148, ηp2 = .076, 95%CI = −.382 – 2.397; post: F (1,27) = 18.79, p < .001, ηp2 = .410, 95%CI = 1.239 – 3.466), these differences had large effect sizes.
Worry
No significant main or interaction effects were found for Worry scores.
ARTIC
A significant change in ARTIC scores was found for the training group, but not the waiting-for-training group. The training group’s scores significantly increased from pre-to post-training, whilst the waiting-for-training group’s scores remained stable across time.
Discussion
The impact of attachment- and trauma-informed training for social workers was evaluated by comparing FMSS and questionnaire measures pre- and post-training between a training and waiting-for-training group. Significant increases across time were found in EE Warmth, RF, Attachment-Informed Stance, Knowledge, and Confidence. Significant differences between groups were found in Knowledge and Confidence, and significant interaction effects were found in EE Warmth, Knowledge and Confidence. Significant increases in ARTIC scores from Time Point 1 to Time Point 2 were found for the training group, but not the waiting-for-training group. No significant changes were found across time, group or in any interaction in EE Positive Comments, EE Negative Comments, EE Dissatisfaction, or Worry. These findings suggest that training can increase social worker professionals’ knowledge and confidence in attachment- and trauma-informed principles, their attitudes towards trauma-informed care, and their level of warmth towards young people they work with, however it is unclear whether or not this translates to other changes in their attitudes towards the young people they work with, such as their reflective functioning, level of dissatisfaction, or attachment-informed stance.
The increases found in social work professionals’ knowledge and confidence as a result of the training are in line with a number of US-based studies identified in a rapid evidence review of papers reporting on implementation of trauma-informed initiatives (Bunting et al., 2019). Although each study implemented a different training program, knowledge of trauma-informed care and confidence in implementing trauma-informed practices increased from pre-to post-training consistently across studies and were maintained at follow-up points of three months to one year. The current study’s findings are also in line with those found from trauma-informed training for staff in pupil referral units (Greenhalgh et al., 2020) which found significant increases in staff’s knowledge of, and confidence in using, trauma-informed care which were maintained across six months of skills development sessions. Whilst it was not possible within the scope of the current research to evaluate knowledge and confidence at a follow-up point, the previous research suggests that these gains are likely to be maintained across time. Our findings of no significant change in staff levels of worry differ from those found by Greenhalgh et al. (2020) who found a significant decrease in worry from pre-to post-training, however in both our training and waiting-for-training groups the level of worry was lower at pre-training than those within Greenhalgh et al.’s sample, suggesting that social worker professionals may have a lower level of baseline worry than professionals in pupil referral units.
Significant increases in ARTIC scores from pre-to post-training for the training group are similar to those found by researchers exploring the outcomes of trauma-informed training for teachers (Kim et al., 2021) and psychiatric hospital staff (Niimura et al., 2019), suggesting that trauma-informed training can have a positive impact on professionals’ attitudes towards trauma-informed care across job roles and professional settings. It was initially hypothesised by the creators of the ARTIC that improved attitudes towards trauma-informed care may lead to more trauma-informed behaviours in professionals (Baker et al., 2021), however this had not been formally researched. The FMSS offered a means of measuring whether changes in ARTIC scores also translated to changes in attitudes towards young people. It was hypothesised that the training package would increase both professionals’ ARTIC scores and we sought to explore whether increasing understanding of attachment and trauma would support the development of an attachment-informed stance. However, whilst ARTIC scores significantly changed in the training group, no significant change in attachment-informed stance was found across groups. The lack of significant change may suggest that whilst professionals may have become more aware of what favourable attitudes are in trauma-informed care, they may still have struggled to apply this to specific young people they work with. It is possible that the skills development sessions may have been able to address this discrepancy by building skills in applying knowledge to practice, and further research should be undertaken to explore whether skills development sessions can improve professionals’ ability to take an attachment informed stance. There may have also been an additional significant factor of time; as speech samples were taken just two weeks apart this may not have allowed sufficient time for knowledge, confidence and attitudes to be embedded into practice. Changing practice in a measurable way can take a much greater length of time, and much of the existing research explores outcomes from 6-24 months post-intervention (Dublin et al., 2021; Lang et al., 2016), therefore had the scope of the current research been able to include a later follow-up data collection point, changes in reflective functioning and attachment-informed stance may have been more apparent. Another possible explanation for the lack of significant change across groups is that the attachment-informed coding system may not have been sufficiently sensitive to detect change, therefore further research is needed to measure change over a longer period of time and across different interventions to give greater insight into the measure’s sensitivity. However, further research is needed to understand whether changes in attitudes relate to actual changes in professional practice and outcomes for those utilising such services.
The significant increase in professionals’ reflective functioning across time, but not across groups or within an interaction, is similar to findings of a randomised controlled trial of a mentalising psychoeducational intervention aimed at foster parents (Adkins et al., 2022) which increased FMSS reflective functioning only across time. In both our findings and those of Adkins et al. increases in mean RF-FMSS scores are seen from pre-to post-training in both the intervention and waiting groups, suggesting that reflective functioning may naturally increase through speaking about a child in the same context twice.
In regards to expressed emotion constructs, our findings show that there may be important differences in baseline levels of EE constructs in social workers, when compared to parents in previous research, with our sample of social workers displaying fewer positive comments and greater negative comments than previous parent samples (Scott et al., 2011), and higher dissatisfaction and lower warmth than previous parent samples (Narayan et al., 2014). These differences could have key implications for future research and intervention as it may be beneficial to explore the impact of social workers’ expressed emotion upon the outcomes of children and young people, and potentially for increased efforts to be made to design and implement interventions that prioritise addressing social work professionals’ expressed emotion. The attachment- and trauma-informed training package has shown a promising change in the level of warmth expressed towards young people which could potentially improve therapeutic relationships and warrants further research efforts, and consideration should be given towards ways of reducing negative comments and increasing positive comments when developing future interventions, particularly for this group of professionals. Whilst the real-world clinical significance of these findings on social workers’ interactions and relationships with young people was not able to be directly measured, it is likely that it will have gone on to have positive outcomes similar to those seen in research around the outcomes of increased warmth in other child-adult relationships. Wider research in this area highlights the positive impact of warmth on children’s behavioural and emotional outcomes (Marshall et al., 2024), and the relationship between behavioural issues and placement instability for looked after children (Rock et al., 2015). Therefore, it may be possible that increased warmth of social care professionals towards young people in care could create positive changes in the level of behavioural difficulties in this population and subsequently increase placement stability, which could be a valuable area for future research endeavours to investigate.
In the absence of an existing measures the development of the Attachment-Informed FMSS coding system has provided an opportunity to explore the effectiveness of attachment- and trauma-informed training programs to increase professionals’ ability to take an attachment-informed stance to relating to, and working with, the individuals who access their services. This is the first FMSS coding system developed specifically to evaluate individuals’ abilities to apply attachment-informed principles whilst also taking a reflective stance to understanding individuals utilising the social care system. It goes above and beyond Reflective Functioning coding systems as it incorporates understandings of relational security from multiple sources, contextualising behaviours, and indications of feeling uncontained within the relationship. The findings of the current study suggest that professionals’ ability to take an attachment-informed stance is measurable through this FMSS coding system and that professionals can become more attachment-informed over time, opening up the potential for it to become a useful outcome measure in future research. Although within this study the Attachment Informed coding system has been applied to social care professionals and their reflections on the young people they work with, it has the potential to be applied to a range of roles and settings where the application of attachment principles is essential. Within the initial analysis the coding system has shown adequate code-recode reliability and good inter-rater reliability, suggesting that it may be a suitable tool for future research, however further validation of use with different professional roles and across professional settings may be needed to establish the appropriate breadth of use.
Due to the challenges of recruiting participants from social work teams, the achieved sample size was relatively small leading to the analysis being underpowered. This particularly creates difficulties in interpreting non-significant results within our analysis as we cannot determine whether they are a genuine result or are due to inadequate power. It is important to also take into consideration the gender imbalance within the training and waiting-for-training groups (44% vs 100% respectively) as there is currently not an evidence base from which to understand the potential varying levels of expressed emotion and reflective functioning across male and female professionals, therefore it is not possible to account for this within the current statistical analysis. A potential selection bias may have existed within the groups as social care teams who were more invested in the training package may have given greater time priority to attending the training, leading less invested teams to naturally fall within the waiting-for-training group. We must also consider the possibility that the coding system in its current form may not be sensitive enough to detect change across time and groups and therefore may require further development. It is likely that recruitment challenges in research with social work professionals will persist, particularly following the lasting impact of COVID-19 and nationwide lockdowns upon the complexity of social service teams’ caseloads and resources (Ofsted, 2022). However, given the important role that social work professionals play in the development of healthy and safe attachment relationships for vulnerable young people (Levenson, 2017), it may be prudent to continue making efforts to explore the impact of training interventions on outcomes relating to the relationship between professionals and the young people they work with. An additional limitation of this study may have been the alignment of the outcome measures to the aims of the two-day training package, as this portion of the training was intended to provide an educational foundation rather than develop the application of skills, and the lack of scope to evaluate outcomes following skills development sessions. The training intervention used was focused on providing attendees with education around attachment theory and how this applies to children’s behavioural presentations, whilst the skills development sessions were intended to support attendees to apply this knowledge to individuals on their caseloads. Therefore, the inclusion of a third data collection point, following the skills development sessions, may have provided the necessary opportunity for these skills to be incorporated into participants’ speech samples as they would have had increased occasions in which they could apply these principles to their individual caseloads. While initial evidence suggests that professionals’ attitudes may be susceptible to change following psycho-education interventions (Bammens et al., 2015), this is still a considerably under-researched area and it may be possible that outcomes are dependent on the specific design and delivery of interventions, the psychological model they are underpinned by, or the opportunity to access ongoing skills development. A final limitation may exist in that there is currently a lack of evidence base from which to draw to confidently assert that changes captured within the FMSS equate to actual behavioural change within professionals.
In conclusion, attachment- and trauma-informed training appears to have a positive impact on social care professionals’ knowledge and confidence in their work, their level of warmth towards young people they work with, and their attitudes towards trauma-informed care, however it remains unclear whether training leads to additional intended outcomes of changes in professionals’ dissatisfaction, negative comments, or positive comments towards the young people they work with, their reflective functioning abilities, or their abilities to take an attachment-informed stance to their work. The Attachment-Informed coding system shows promise in its utility for measuring professionals’ ability to be attachment-informed, however further validation is needed across professions and settings. Future research endeavours may be hindered by challenges in recruiting social care staff, however given the importance of their role in the lives of vulnerable young people significant efforts should be made to overcome these challenges and further out understanding of these relationships and how to improve outcomes for young people in the social service system.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This research involves human participants and has received approval from Cardiff University School of Psychology Research Ethics Committee (EC.19.11.12.5893R2A2).
Consent to participate
All participants included in the study provided informed consent verbally.
Data Availability Statement
Data is available upon reasonable request.