
Abstract
Research suggests that among all children living in social care, those in residential care have the highest mental health need. This systematic review and meta-analysis is the first to establish the type and prevalence of mental health disorders and symptoms among children in residential care. A systematic search of PsycINFO, MEDLINE, Scopus, Web of Science Core Collection, ASSIA, IBSS and grey literature databases from January 1989 to July 2022 was conducted (N = 11, 246). Articles were eligible for inclusion where they: (1) included a sample living in residential provision similar to that provided in the UK, (2) used standardised screening tools or psychiatric assessments, using diagnostic classification systems, and (3) reported prevalence estimates. Pooled prevalence estimates were calculated using random-effects meta-analysis. 21 articles with prevalence rates for a total of 4287 children, adolescents and young adults were included. Almost half the children had symptoms indicative of a probable mental health disorder (46%; 95% confidence interval (CI) 35–58). Externalising problems (49%; 95% CI 34–65), were more common than internalising problems (39%; 95% CI 26–53) and prevalence rates for conduct disorder (34%; 95% CI 17–55), depression (26%; 95% CI 18–35), emotional symptoms (17%; 95% CI 8–28), and somatic symptoms (14%; 95% CI 8–20) were estimated. The findings provide evidence that the prevalence of mental health disorders and symptoms are particularly high among children in residential care. These pooled estimates should be interpreted with caution due to high heterogeneity and further epidemiological research is needed to guide policy in different countries.
Introduction
Article 20 on the UN Convention of the Rights of the Child specifies that the state is responsible for delivering alternative care which provides protection and support for children who are temporarily or permanently deprived of their family environment or who cannot be allowed to remain there (United Nations General Assembly, 1989). Residential care is a type of group home offered to some of these children. The homes usually accommodate 3 to 5 unrelated children, who are looked after by multiple residential care staff (Berridge et al., 2012). The international landscape of residential care is very mixed due to differences in the level of staff training, in-house therapeutic support, staffing ratios, and preference for family-based, compared to institutional care (James et al., 2021; Whittaker et al., 2022). The review will focus on the model of residential care seen in the UK and other countries where a similar structure of care is provided. The term “residential care” will be used to encompass children’s homes, therapeutic/high support units, secure care, specially commissioned provision for single children and supported accommodation in preparation for independence. This definition aligns with the ‘models of residential care’ outlined by Hart, La Valle, and Holmes in their rapid review of the literature on residential care (2015). The ‘models of residential care’ was used to identify countries with residential care that resembled the UK provision, which led to the inclusion of further Western countries in the current review.
Several countries, including the UK, have reduced their use of residential care (Ainsworth & Thoburn, 2014). In England, its provision peaked in the mid-1970s when 40,000 children were accommodated in residential settings (Narey, 2016). These numbers drastically reduced, and between March 2021 to 2022, just over 13,000 children were living in residential care in England (Department for Education, 2022). This reduction was driven by a preference for family-based placements such as foster or kinship care (Thoburn, 2016), leading to a minority of children being placed in residential settings (Department for Education, 2022). However, despite an overall reduction over the last 50 years, the proportion of children in care that live in residential placements recently increased from 13% in 2020 to 16% in 2022 (Department for Education, 2020, Department for Education, 2022). Given the significant policy preference for family-based care, residential care has increasingly been characterised as a therapeutic 'last resort' for children who are not able to live in foster families due to high levels of emotional distress and behavioural difficulties (Hart et al., 2015; Schoenwald et al., 2022).
The use of residential care has been questioned due to poor psychosocial outcomes seen among young people living in these settings, coupled with higher placement costs compared to family-based care and a history of institutional abuse (Berridge et al., 2012; Mollidor & Berridge, 2017). Nonetheless, residential care offers the opportunity for intensive and specialist support and an alternative to family-based placements (Narey, 2016). For some children, this type of care can offer the best chance of positive outcomes (Holmes et al., 2018), such as educational attainment and can be their placement of choice (Hart et al., 2015). The place for residential care in the child welfare system has been established in the UK (Hart et al., 2015), and its role was recently affirmed in the Independent Review of Children’s Social Care (MacAlister, 2022).
Mental health of children living in residential care
Children’s adverse experiences prior to coming into care play a key role in their mental health outcomes (Engler et al., 2022; Meltzer et al., 2003). In the UK, 92% of children in care are placed due to the risk of abuse or neglect and family dysfunction (Department for Education, 2022). Evidence suggests that a decision to place a child in a residential setting often follows a combination of factors, including family breakdown, childhood sexual exploitation, going missing and/or mental health issues (Ofsted, 2022; Schoenwald et al., 2022). Children are typically placed in residential care at an average age of 14 years old, following a longer period of unmet need (Berridge et al., 2012; Department for Children, Schools and Families, 2014; Narey, 2016). While living in residential care, they can experience a lot of instability both in their placements, where on average, they have more placements than those in family-based care and in their schools, often due to fixed term exclusions (Schoenwald et al., 2022). Despite these challenging experiences, some children show healthy adaptation linked to protective factors (Pinheiro et al., 2022). However, children who live in residential care are consistently reported to have the highest mental health need and worse outcomes in adulthood compared to children living in family-based care (Campos et al., 2019; Dregan & Gulliford, 2011; Ford et al., 2007; Li et al., 2019; Strijbosch et al., 2015). Yet, there is a limited evidence base about the children’s mental health needs that can be used to inform residential care practice (Hart et al., 2015; Holmes et al., 2018).
Review rationale
A clear understanding of the mental health of this population is needed to build the evidence base informing what constitutes effective residential care. To date, two reviews have systematically looked at the prevalence of mental health disorders among children living in care. One meta-analysis by Bronsard et al. (2016) found that almost half of the overall sample of N = 3104 living in the child welfare system in five Western countries met the criteria for a mental health disorder. The most common disorders identified were disruptive disorder (27%), including conduct disorder (20%) and oppositional defiant disorder (12%), attention-deficit/hyperactivity disorder (11%), anxiety and depressive disorders (18%) and post-traumatic stress disorder (PTSD; 4%). More recently, a systematic review by Engler et al. (2022) evidenced the higher prevalence of mental health disorders among children living in foster care compared to the general population. To our knowledge, this will be the first systematic review and meta-analysis specifically investigating the type and prevalence of mental health disorders and symptoms among children living in residential care.
Methods
Definitions of mental health disorders and symptoms
For the review, mental health disorders are defined as clinically significant psychological difficulties associated with distress and increased risk of suffering (Stein et al., 2010). They can be categorised using formal taxonomic systems, providing distinctions between different mental health disorders. The most used systems are the Diagnostic and Statistical Manual of Mental Health Disorders (DSM; American Psychiatric Association, 2022) and the International Classification of Diseases (ICD; World Health Organisation, 2019). Structured psychiatric assessments, such as the Development and Well-being Assessment (DAWBA; Goodman et al., 2000), use classification systems to diagnose children with mental health disorders.
Mental health symptoms refer to behavioural symptoms that may be of clinical concern, suggesting that a child has a probable mental health disorder. Screening tools such as the Child Behaviour Checklist (CBCL; Achenbach, 1999) and the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) are used to detect such symptoms prior to further diagnostic assessment. The screening tools have standardised cut-off scores, which reflect clinically significant difficulties requiring further assessment and possibly the need for evidence-based psychological intervention (Wright et al., 2019). Some screening tools include a measure reflecting the overall extent of emotional and behavioural problems, referred to as ‘total behaviour problems’. Composite scores for externalising and internalising behaviours are also assessed, ‘externalising problems’ reflect rule-breaking, aggression, impulsivity, and inattention behaviours, and ‘internalising problems’ reflect depression, anxiety, social problems, and somatic symptoms. The screening tools also assess a child’s ‘emotional symptoms’, which reflect anxious and depressive symptoms, which commonly covary. Both mental health disorders and mental health symptoms were included in the present review.
Search strategy
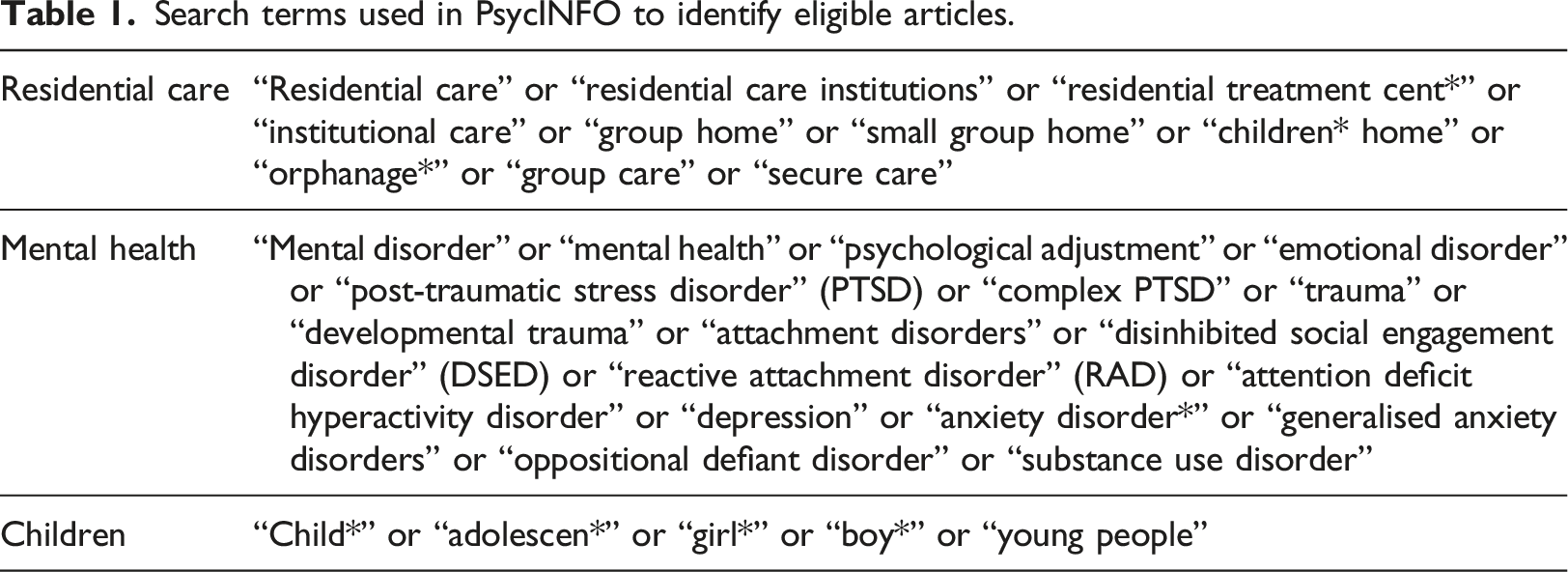
Search terms used in PsycINFO to identify eligible articles.
Information sources
We conducted electronic searches for eligible studies within the following databases: PsycINFO, Web of Science Core Collection, MEDLINE, ASSIA, IBBS, and Scopus from January 1989 through July 2022. Articles published prior to 1989 were not eligible for inclusion due to the establishment of the Children’s Act (Children Act, 1989) and the UN Convention on the Rights of the Child (United Nations General Assembly, 1989), which altered the governance of children’s rights and care when living in social care settings. Electronic searches based on the final PsycINFO search strategy were conducted in the following grey literature databases: Social Care Online, BASE, OpenAIRE, EThOS and ProQuest (Dissertations and theses).
Criteria for selecting the articles
We included published and unpublished observational and intervention studies and randomised control trials. Studies were not required to have a comparison group to be included in the review. A scoping review found insufficient literature in the UK, so wider countries were included in the review. To determine countries eligible for inclusion, ‘the models of international residential care’ published in a rapid review of the literature on residential care was used as it indicated countries offering residential care which resembles UK provision (Hart et al., 2015). The eligible studies had to meet the following criteria: (1) a sample including any children (under 18 years of age) living in residential care (children’s homes, therapeutic/high support units, specially commissioned provision for single children, secure care, and supported accommodation) due to child protection or welfare services (Hart et al., 2015), (2) use of a standardised mental health screening tool or psychiatric diagnostic assessment using semi-structured or structured interviews alongside an international diagnostic classification system (DSM or ICD), (3) reported prevalence estimates for current mental health disorders or symptoms, (4) published in English, (5) published in a peer-reviewed article, dissertation, or unpublished article since 1989, (6) studies set in children’s residential care settings from the UK, USA, Denmark, Germany, France, Canada, Spain, Italy, Australia, Finland, Israel, Netherlands, Norway, and Sweden. (1) a sample of fewer than 18 participants, as samples larger than 18 are recommended in cross-sectional studies when prevalence is expected to be greater than 5% (Pourhoseingholi et al., 2013), (2) results published in a literature review, conference abstract, poster, or letter, (3) children living in any residential care setting that does not meet the criteria outlined in the eligibility section (4) use of incorrect mental health assessment if (1) an unstandardised assessment tool was used, (2) mental health was established based on health or court records, or (3) mental health was not assessed, and carers just reported the presence or absence of disorders.
Articles were excluded based on the following criteria:
Selection process
The review team was led by MW and included DD, SH, AV, AKD, SD, and SR. Two reviewers (MW, AV) independently screened the first 10% of titles and abstracts for inclusion, with 88% concordance. The main reviewer (MW) then reviewed all titles and abstracts. Three members of the review team (MW, SD, SR) then screened 10% of the full texts of the potentially eligible studies, with 90% concordance. Any disagreements over the eligibility of studies between the reviewers were resolved through discussion with a third review team member, and in no case did the second reviewers identify any additional papers already identified by the first reviewer. The main reviewer then screened the full text of all potentially eligible studies. Two members of the review team (MW, AKD) screened 10% of the grey literature prior to the main reviewer screening all remaining publications.
Reasons for exclusion were recorded. Where there were multiple reports for the same data set and clear repetition based on sample characteristics, only the original full sample was included in the review. In addition, where both a thesis and peer-reviewed publication reported on the same data, the publication containing less relevant information was excluded. Where studies appeared eligible but details on the specific composition of the sample were not reported, the studies were included.
Data collection process
Two review authors (MW, AV) independently extracted data from three out of the 21 eligible texts using a structured data extraction form in MS Excel to check reliability; 95% concordance was reached before discussion, raising to 100% following discussion. The main reviewer extracted data from the remaining eligible texts. The following information was extracted from the studies using a standardised form: first author, year published, geographic location, study setting, sample size, study population and participant demographics, study design, study methodology, criteria used to identify mental health disorder or symptoms, informant, outcome(s) measured estimated prevalence results, information for the assessment of the risk of bias and comments.
Critical appraisal
The scientific strength of the articles was assessed using a checklist based on the ‘Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data’ (Munn et al., 2015). The main reviewer led the assessment, and any queries were resolved through a discussion with the wider review team.
Synthesis methods
Several decisions needed to be made in extracting or estimating prevalence rates based on the available data in the eligible articles. Where studies reported prevalence estimates using both standardised and unstandardised tools, prevalence estimates calculated using unstandardised tools were not extracted or assessed within the risk of bias appraisal (Jozefiak et al., 2016; Schmid et al., 2008). Where studies reported on the severity of the outcome, rates for moderate, severe, and clinical levels of need were combined to produce one prevalence estimate (Hibbard et al., 1992; Li et al., 2001; Markee, 1997). Where studies reported on borderline and clinical rates, just the clinical rates were extracted (Kavemann et al., 2018). Where prevalence rates were reported for two thresholds, the recommended threshold was used (Li et al., 2001). Where the number of participants assessed to have a particular mental health disorder or symptom were missing, the reported prevalence and total sample were used to calculate the raw figure (Collin-Vézina et al., 2011; Ford et al., 2007; Jozefiak et al., 2016; Martín et al., 2018; Schmid et al., 2008). Where articles reported separate prevalence rates for more than one eligible group of children living in residential care, a total prevalence rate was calculated using the raw scores (Carroll, 2011; Li et al., 2001; Martín et al., 2018; Sourander et al., 1997). One study estimated prevalence using two different measurement tools (CBCL and TRF) and two informants (carer and teachers); for this article, estimates from the CBCL were selected for inclusion in the meta-analysis as no other articles included teacher report (Sourander et al., 1997). One study reported prevalence estimates using two different tools (CBCL and YSR) and informants (carers and youth); only YSR were included in the meta-analysis (Schmid et al., 2008) as the review team prioritised including the perspective of the young person.
Operationalisation of mental health disorders and symptoms, and therefore grouping of articles for the meta-analysis, was established based on the assessment criteria used in individual articles. Articles were included in a meta-analysis where there was a minimum of five articles for the mental health disorder or symptom. This minimum was set because five or more articles consistently have greater powers in random effects meta-analysis (Jackson & Turner, 2017).
A random-effects meta-analysis was performed to provide a pooled prevalence estimate for ‘total behaviour problems’, ‘internalising problems’, ‘externalising problems’, ‘depression’, ‘conduct disorder’, ‘emotional symptoms’, and ‘somatic symptoms’. Heterogeneity was assessed using the I2 statistic, and 75% heterogeneity was indicative of considerable heterogeneity. Sensitivity analyses were performed where outliers were identified, and publication bias was explored using funnel plots. Meta-analyses were performed using R (R Core Team, 2021). The prevalence rates for mental health disorders and symptoms that were not included in the meta-analyses are summarised in Appendix 2.
The common types of mental health disorders and symptoms are summarised, and articles showing higher rates of mental health disorders and symptoms among children living in residential care are described. Sources of heterogeneity were discussed.
Results
Literature search
The review was conducted and reported using the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA; Page et al., 2021). The PRISMA statement flow diagram outlines the literature screening and article selection, indicating reasons for article exclusion (see Figure 1). The search resulted in a total of 11,246 articles, of which 21 were eligible for inclusion in the narrative synthesis and meta-analysis. PRISMA 2020 flow diagram.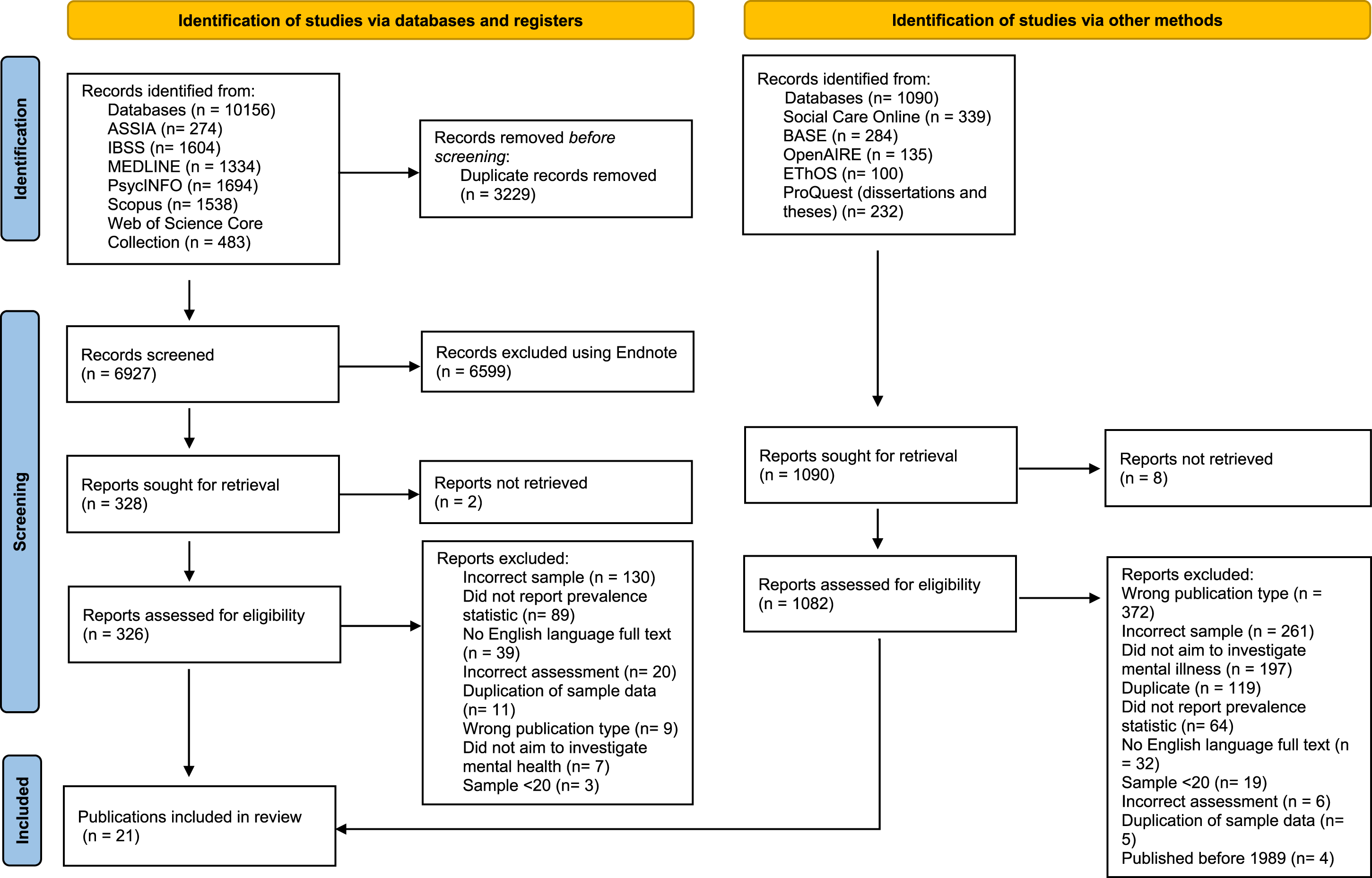
Main characteristics of included articles
The characteristics of the articles are presented in Appendix 3. The designs of the study differed; 17 were cross-sectional, and four were longitudinal. The articles were published between 1992 (Hibbard et al., 1992) and 2020 (Águila-Otero et al., 2020) and included samples from the following countries: France (n = 1), Norway (n = 1), United Kingdom (n = 1), Scotland (n = 1), Canada (n = 3), Germany (n = 3), the United States (n = 3), Spain (n = 4), Finland (n = 3); 1 article included a sample of children from Finland, Ireland, Scotland and Spain. Most articles reported prevalence estimates using standardised screening tools for mental health symptoms, such as the CBCL, and four articles used standardised diagnostic classification criteria to diagnose mental health disorders (DAWBA, DISC 2.25, CAPA and the DISYPS-KJ). The assessment informant varied in the articles; 10 used youth report, eight used carer report and three used a combination of parent, teacher, and youth report.
The sample sizes of children living in residential care ranged from 36 to 875. The residential care setting differed by article and included children living in both ‘small and large group homes’, ‘special homes’, ‘secure care’, ‘therapeutic residential care’, ‘single gender youth residential facilities’, ‘residential establishments’, and ‘autonomy programs for adolescents’. The level of detail provided about the residential care setting was variable.
Most articles had a sample of girls and boys (n = 18), one included a sample of just girls (Kavemann et al., 2018), and two included samples of just boys (Carroll, 2011), with one including only male unaccompanied refugee minors (Sierau et al., 2019). All articles included children and young people ranging from 3 to 20 years, with a mean age under 18 years.
Critical appraisal
Critical appraisal of the included articles.
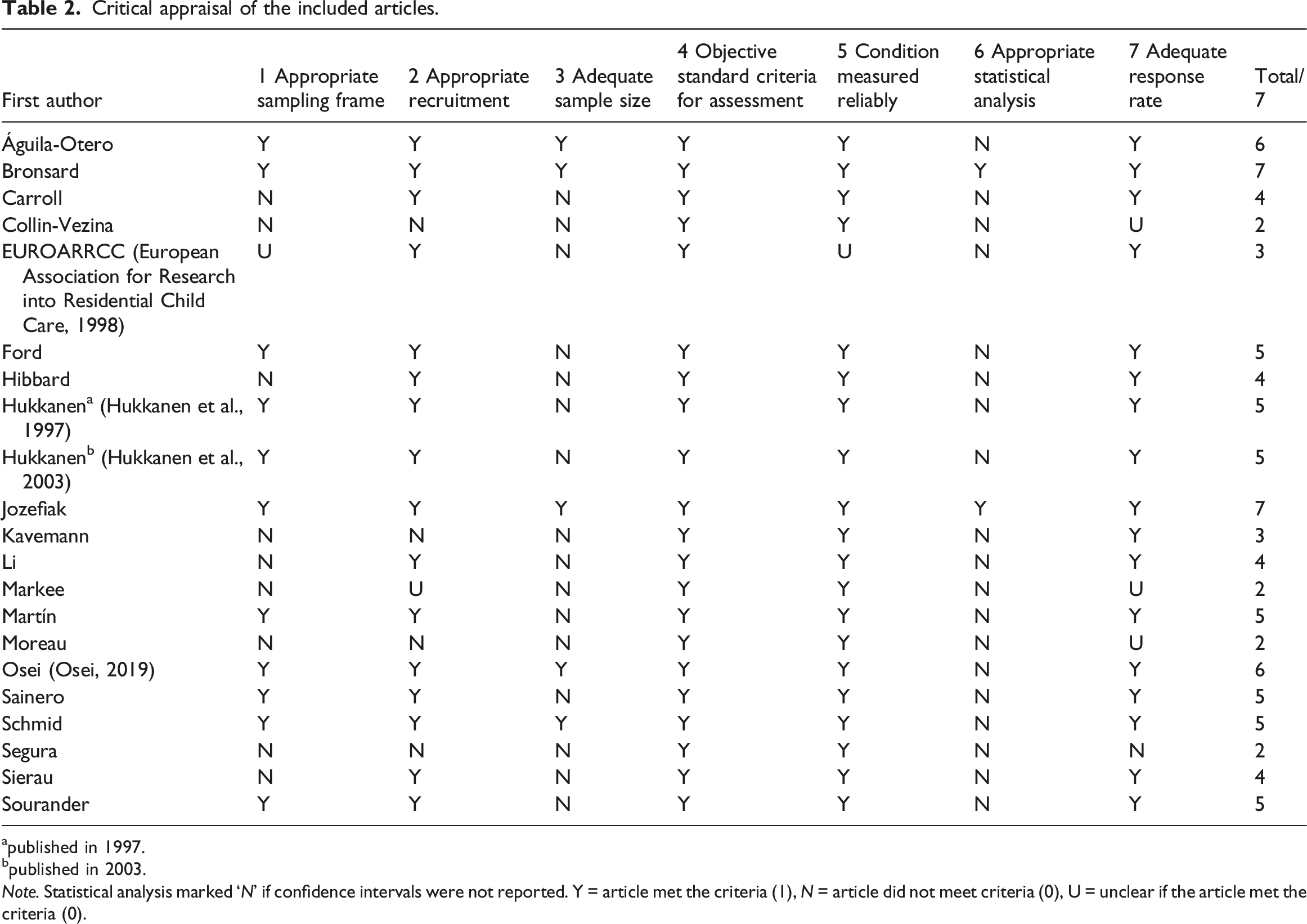
apublished in 1997.
bpublished in 2003.
Note. Statistical analysis marked ‘N’ if confidence intervals were not reported. Y = article met the criteria (1), N = article did not meet criteria (0), U = unclear if the article met the criteria (0).
Meta-analysis
The meta-analysis estimated the pooled prevalence rates of the mental health disorders and symptoms commonly reported by the articles. The funnel plots were quite asymmetrical, and Egger’s regression intercept was not statistically significant (p < .05), suggesting an absence of publication bias (see Appendix 4). Sensitivity analyses were used to explore the impact of excluding studies where the prevalence estimate or sample make up was substantially different from the other included articles. Sensitivity analyses revealed only minor changes to the pooled prevalence estimates (1%–7%). Therefore, the pooled estimates remained largely unchanged, showing they are relatively stable (see Appendix 5).
Total behaviour problems
Eight articles, including 1541 subjects, provided data about total behaviour problems (Figure 2 Prevalence of total behaviour problems among children living in residential care.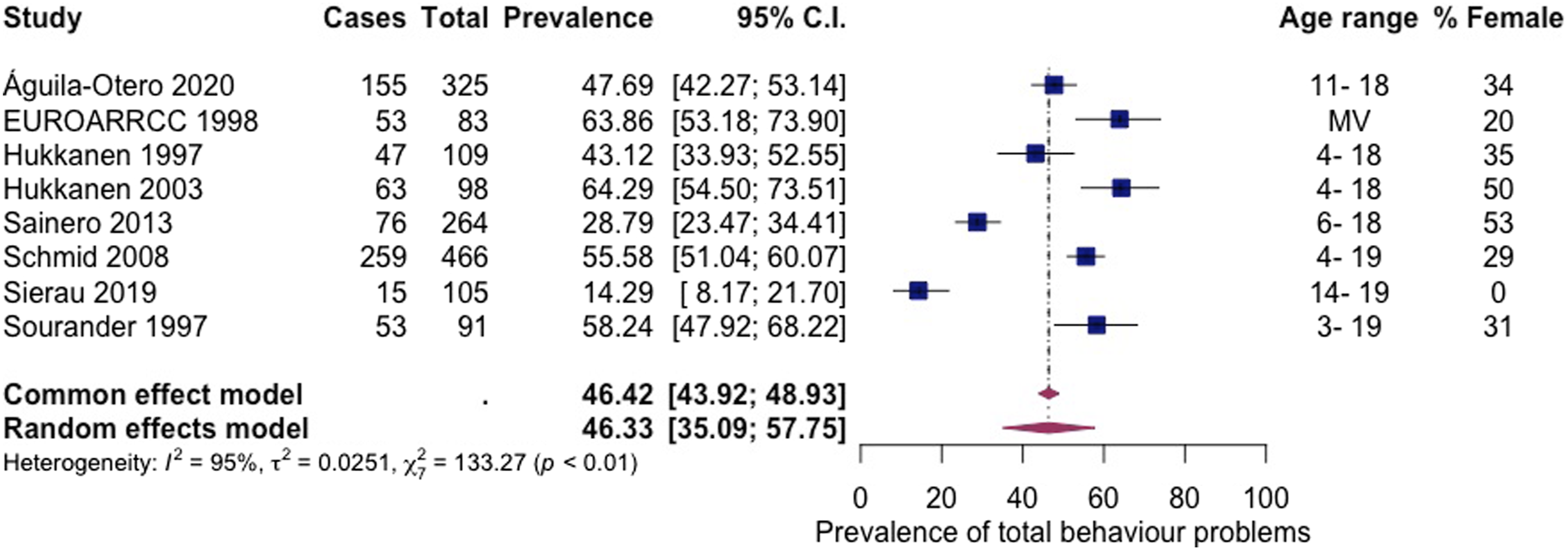
Externalising problems
Six articles, including 1489 subjects, provided data about externalising problems (Figure 3 Prevalence of externalising problems among children living in residential care.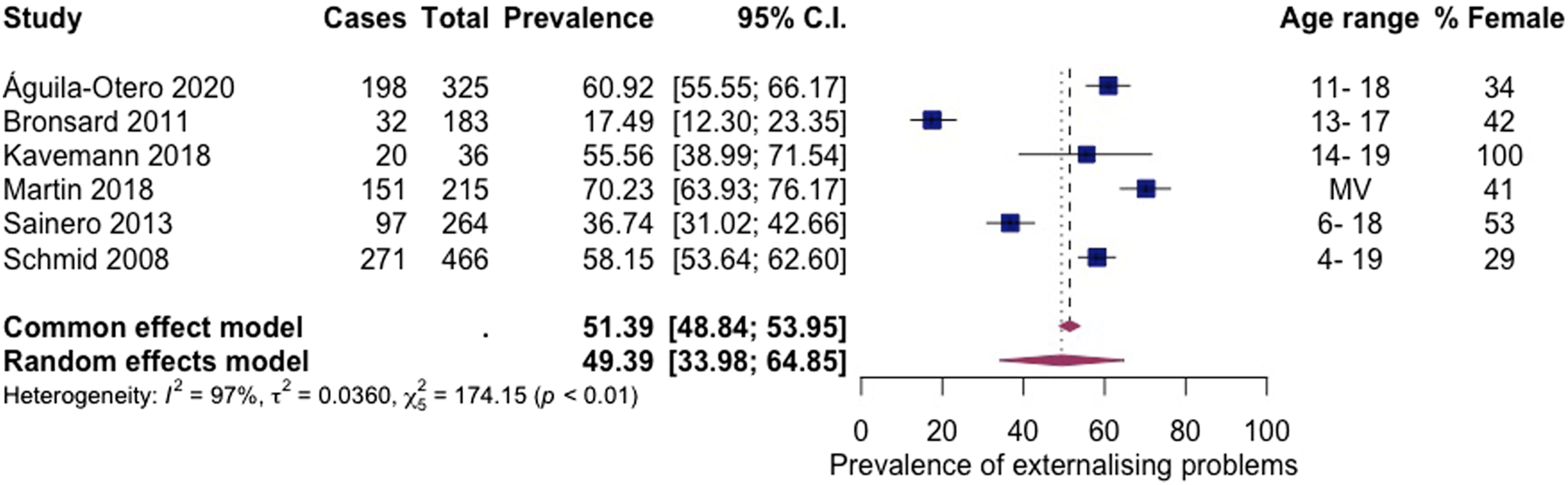
Internalising problems
Seven articles, including 1768 subjects, provided data about internalising problems (Figure 4 Prevalence of internalising problems among children living in residential care.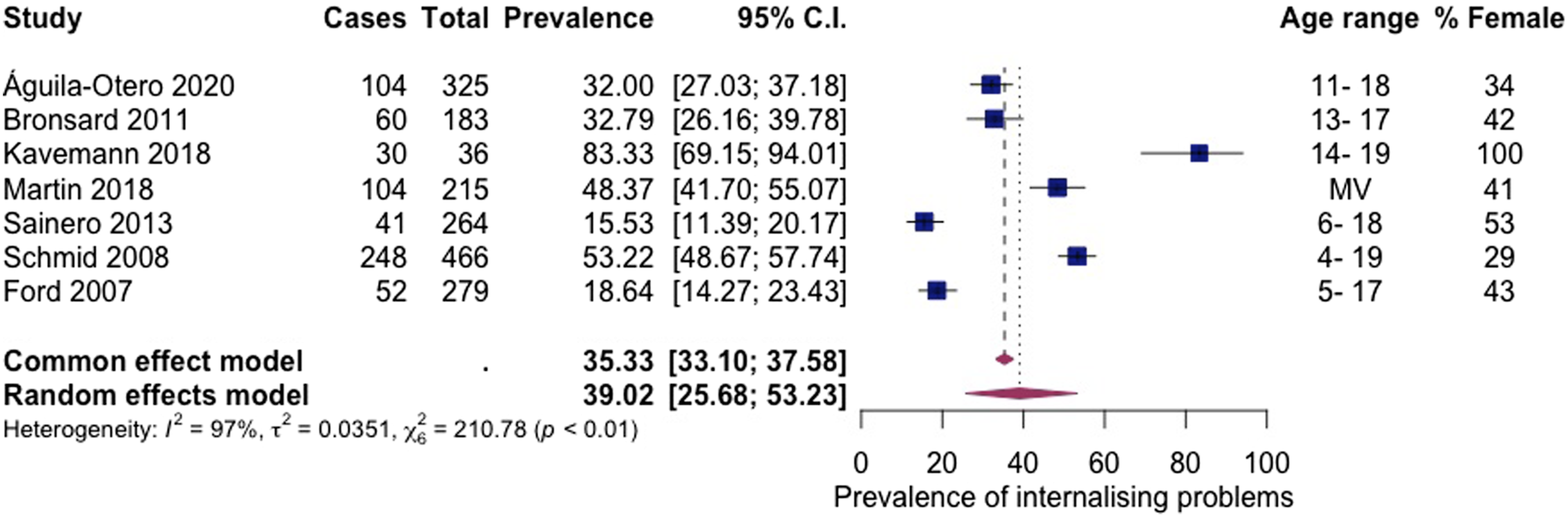
Conduct disorder
Five articles, including 2136 subjects, provided data about conduct disorder (Figure 5 Prevalence of conduct disorder among children living in residential care.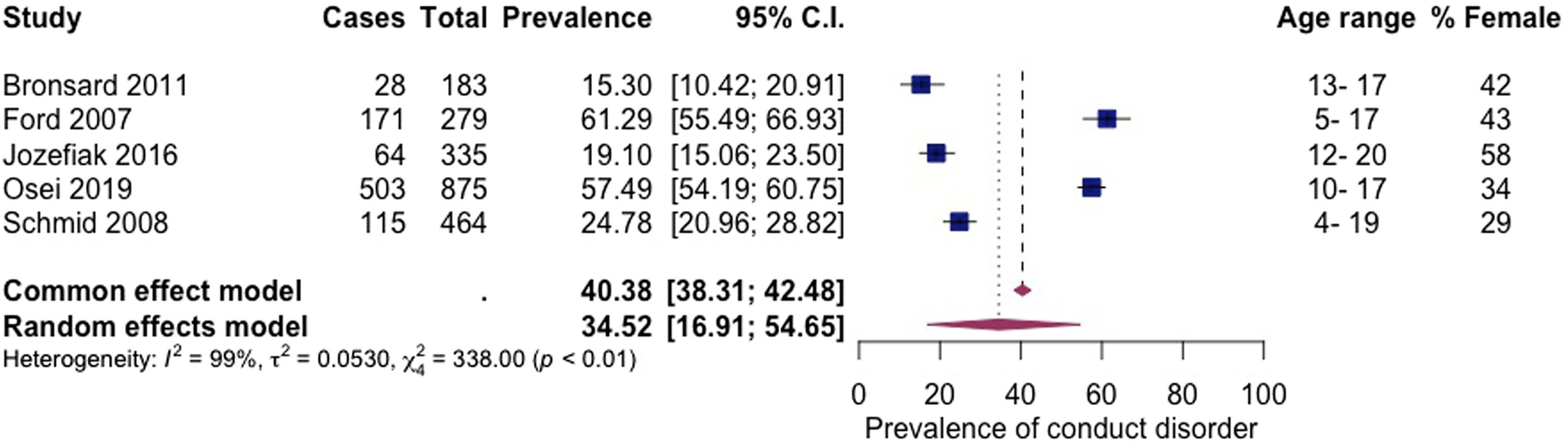
Depression
Nine articles, including 1238 subjects, provided data about depression (Figure 6 Prevalence of depression among children living in residential care.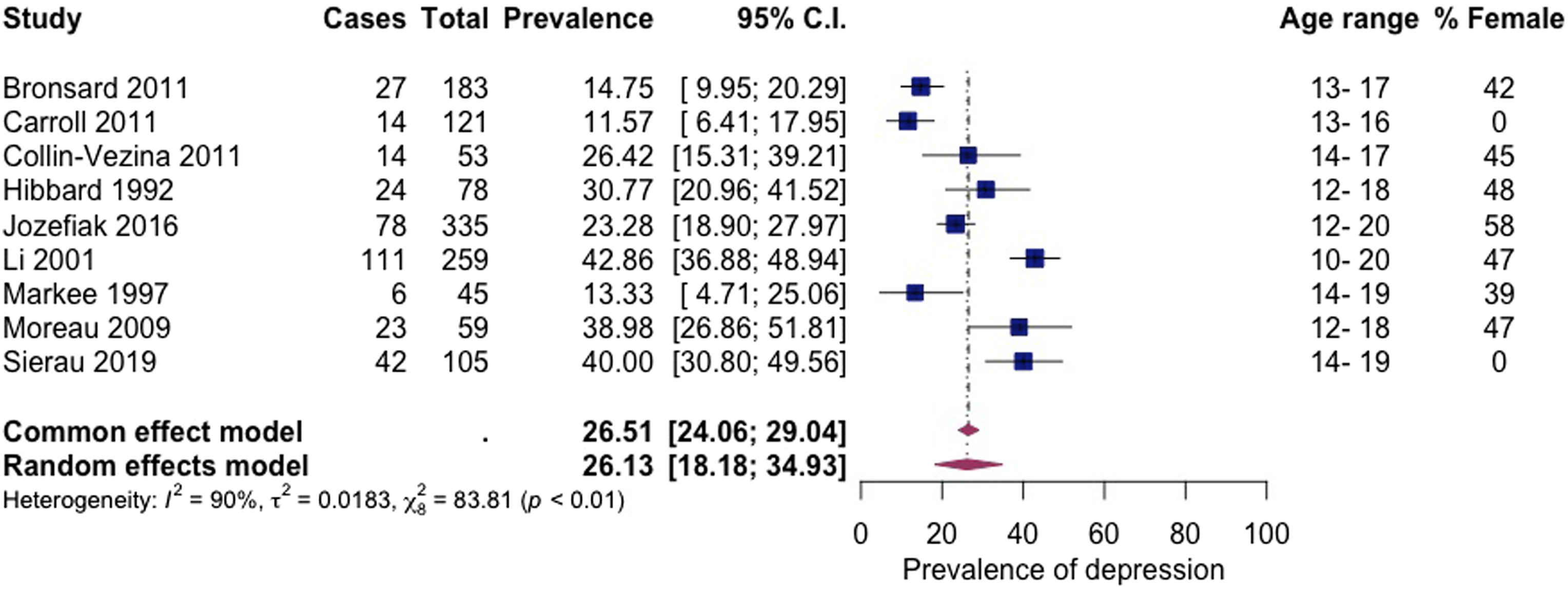
Emotional symptoms (anxious/depressive symptomatology)
Five articles, including 1806 subjects, provided data about emotional symptoms (Figure 7 Prevalence of emotional symptoms among children living in residential care.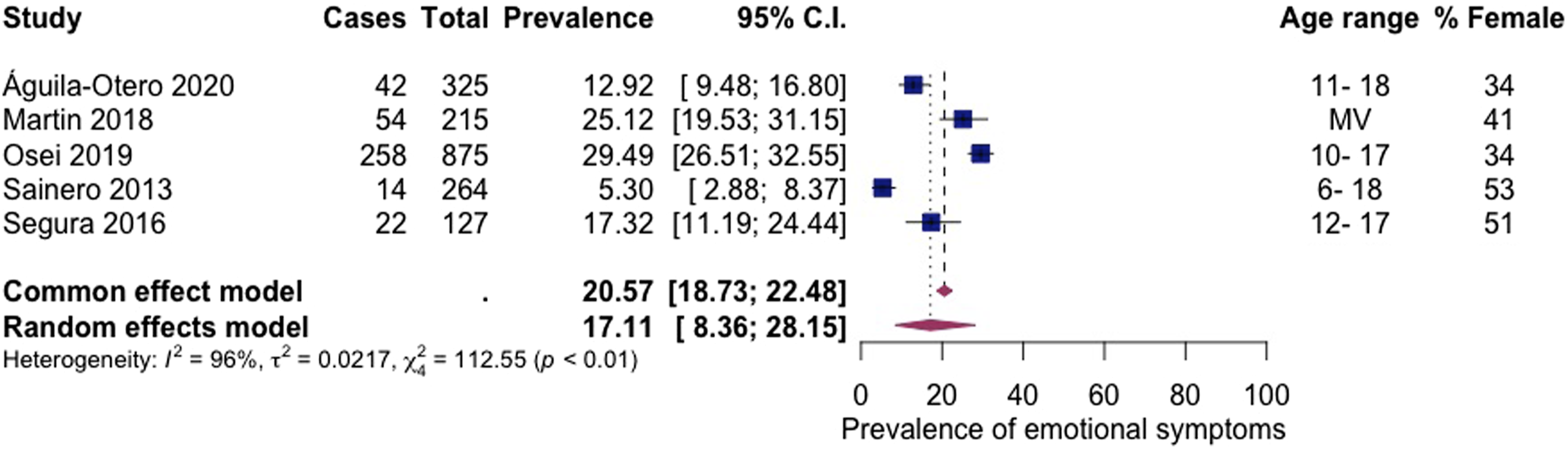
Somatic symptoms
Five articles, including 1036 subjects, provided data about somatic symptoms (Figure 8 Prevalence of somatic symptoms among children living in residential care.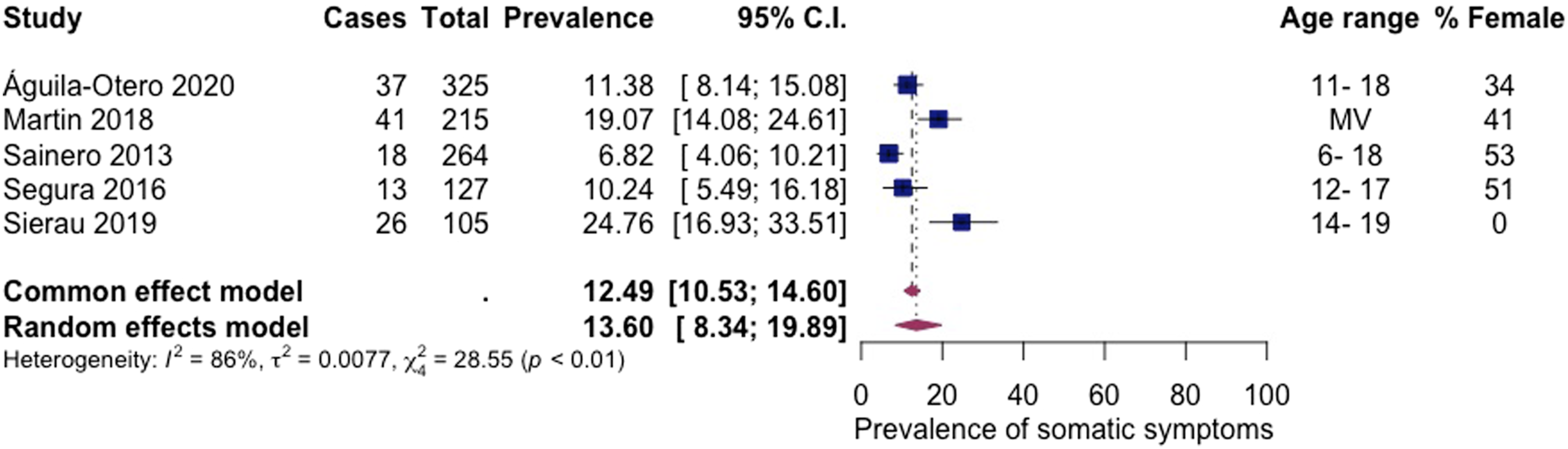
Prevalence of any mental health disorder
Four articles reported a binary outcome of ‘any mental health disorder’ (Ford et al., 2007; Jozefiak et al., 2016; Sainero et al., 2013; Águila-Otero et al., 2020). Five articles were required for the meta-analyses; therefore, a pooled prevalence estimate was not calculated. The prevalence rates for children with ‘any mental health disorder’ ranged from 44% to 76% (see Appendix 2).
Discussion
This systematic review and meta-analysis is the first to evidence the high prevalence rates of a range of mental health difficulties among children living in residential care. The review identified 21 articles that included a total of 4287 participants and reported on 36 mental health disorders and symptoms. Meta-analyses were performed on eight of these outcomes. The findings are consistent with previous reviews, which show higher prevalence rates among children living in care compared to children living in the community (Bronsard et al., 2016; Engler et al., 2022).
The prevalence rate of children who had any mental health disorder or problem ranged from 44% to 76% (Águila-Otero et al., 2020; Ford et al., 2007; Jozefiak et al., 2016; Sainero et al., 2013). Similar prevalence rates have been reported among children living in other types of child welfare settings, with estimates ranging from 37% to 67% and a pooled prevalence of 49% (Bronsard et al., 2016). The current finding also suggests that the prevalence of mental health disorders among children living in residential care appears to be considerably greater than that of children in the general population. For example, a recent meta-analysis of children in the general population living in high-income countries found an overall mental health disorder prevalence of 13% (Barican et al., 2022). Our findings indicate that the pooled prevalence for total behaviour problems among children living in residential care was 46%. In contrast, lower rates of total behaviour problems, of around 10%, are found in the general population (Goodman & Goodman, 2012). This observed difference in the prevalence of children’s mental health can partly be attributed to their experiences of adversity.
All children living in residential care experience the loss of living with their family of origin, often following a period of unmet need (Narey, 2016). They generally have traumatic experiences, such as abuse and neglect from caregivers, which contribute to their entry into children’s social care (Department for Education, 2022). This adversity can impair a child’s capacity to seek help from others due to the breach of trust with the individual (Teicher & Samson, 2013). In response, children often feel unsafe, and their behaviours adapt to elicit care, leading to behaviours that help regulate unmanageable states of distress (Van der Kolk, 2005). Children living in residential settings are likely to have the greatest disruption in their care due to multiple placement moves (Schoenwald et al., 2022). Poor attachment and trauma can cause mental health difficulties (Howell et al., 2021), and researchers have suggested that impaired ability to mentalise is a transdiagnostic mechanism underlying this vulnerability to psychopathology (Luyten et al., 2020). Mentalising describes a child’s capacity to understand themselves and others through intentional mental states such as attitudes and feelings, which can impact their ability to self-regulate.
The current findings indicate that approximately half the children living in residential care have externalising problems. The pooled prevalence for externalising problems was 49%, and conduct disorder was 34%. Similarly, conduct disorder and oppositional defiant disorder were identified as some of the most common diagnoses among children living in foster care (Engler et al., 2022). The figures from the current review are notably higher than the pooled estimates of conduct disorder for all children in all child welfare services (20%) and among children in the general population (1%) (Barican et al., 2022; Bronsard et al., 2016). Compared to the general population, children in residential care are more likely to have been exposed to interpersonal trauma in early childhood, which is associated with later behavioural problems (Holmes et al., 2015). Behaviour such as rule-breaking, physical and verbal aggression can be challenging to manage and can put the child or carers at risk of harm (Loades & Mastroyannopoulou, 2010). Despite carers’ best efforts, some children’s needs cannot be met in foster care, and children’s distressed and distressing behaviour can contribute to placement in residential care (Luke et al., 2014). Once in residential care, children can be exposed to aggression, bullying and peer victimisation (Mazzone et al., 2018) and may display those behaviours through the harmful effects of ‘peer contagion’ (Dishion et al., 1999).
The observed pooled prevalence of internalising problems (39%), depression (26%), and emotional symptoms (17%) suggest that internalising problems are less common than externalising problems among children living in residential care. These findings are consistent with previous research about children living in child welfare services (Bronsard et al., 2016). In contrast, secondary school-aged children in the general population are more likely to have a probable emotional rather than behavioural difficulty (Co-Space, 2022). There are known differences in prevalence rates of mental health associated with a child’s sex. Most children living in residential care are boys (Berridge et al., 2012), and most participants included in the current review were boys. Therefore, the prevalence of externalising problems may appear particularly heightened in the current findings. Articles included in the review evidenced gender differences showing girls had higher levels of internalising problems than boys (Bronsard et al., 2016; Jozefiak et al., 2016; Li et al., 2001; Águila-Otero et al., 2020) in line with research from the general population (Yoon et al., 2022). Girls may develop internalising problems due to early pubertal timing (Ge et al., 2001) and greater interpersonal vulnerability, contributing to a greater reactivity to stressful interpersonal events (Leadbeater et al., 1999). Internalising problems are particularly concerning as they are linked to self-harm and suicidal behaviour in adolescents (Gutman & Codiroli McMaster, 2020).
Some children have very challenging experiences before and during their time living in social care (Berridge et al., 2012; Department for Education, 2022). These experiences can be traumatic, and some children may develop PTSD. The current review included three articles which reported prevalence estimates for PTSD ranging from 1% to 30% (Collin-Vézina et al., 2011; Jozefiak et al., 2016; Sierau et al., 2019) and rates of trauma-related symptomatology such as dissociation (28%), sexual concerns (34%) and anger (19%) (Collin-Vézina et al., 2011). The range in prevalence estimates is likely due to the different methodology between articles, with lower prevalence reported when psychiatric diagnostic assessments were used compared to screening tools. Internalising and externalising problems can reflect PTSD symptoms, meaning the high pooled prevalence rates observed in this review may be indicative of wider PTSD symptomatology. There is not enough research to estimate the pooled prevalence of PTSD, but these initial findings suggest the need for further research in this area.
This review did not report prevalence estimates for other trauma- and attachment-related disorders such as RAD and DSED. Although these disorders are more common among children exposed to maltreatment, their relevance and validity in children over five years have been questioned (Zeanah et al., 2016). For inclusion in this review, reported prevalence estimates must have been calculated using a standardised screening tool or a diagnostic assessment interview. Most included articles used tools such as the CBCL and SDQ, designed for children in the general population, which do not assess these disorders (Lehmann et al., 2016). One included article (Jozefiak et al., 2016) reported a prevalence rate for RAD (21%); however, the estimate was not eligible for inclusion as the authors did not use a standardised screening tool. An adapted version of the Preschool Age Psychiatric Assessment (PAPA) was used (Egger et al., 2006), as the childhood version does not assess RAD. The authors acknowledged the limitations of their approach as three items were excluded due to their irrelevance to adolescent behaviour, and they did not have parental information about participants’ behaviour under five years (DSM-IV criterion A). The prevalence of attachment- and trauma-related disorders among children living in residential care remains unclear, therefore requiring future research investigating the relevance and assessment of such disorders in this population.
Strengths and limitations
The current meta-analysis is the first of its kind to investigate the prevalence of mental health disorders among children living in residential care. A comprehensive search was completed, including six research databases and five grey literature databases. Despite these efforts, several limits of the review are acknowledged.
A high level of heterogeneity in the results was observed between the included articles in the meta-analyses. Comparable levels of heterogeneity have been observed in meta-analyses about children living in care and in the general population (Barican et al., 2022; Bronsard et al., 2016). Bronsard and colleagues explored sources of heterogeneity and found that country, sex ratio, mean age, sample size, informants and diagnostic assessment contributed significantly to the heterogeneity of their samples of children in care. Due to a dearth of literature available in the UK, countries where the residential provision was comparable to the UK were included in the review. Every country has a different legislative framework that influences the reasons children enter social care, placement decisions, staff training, education, income, attitudes to reunification, and approaches to therapeutic interventions (James et al., 2021; Whittaker et al., 2022). These differences may challenge the comparability of international samples.
The included articles had varied methodology, often using unrepresentative samples due to an inadequate sampling frame and a small sample size, different informants, and a range of mental health assessments. The review included articles that reported prevalence rates calculated using both diagnostic and screening assessments. Both assessments were included due to the debate around the applicability of a diagnostic frame to understand the mental health of children in care and the limited number of articles using diagnostic assessment. Children in care often have complex attachment- and trauma-related symptomatology that are not captured well by the current diagnostic framework (Tarren-Sweeney et al., 2019), meaning the children may require support from a specialist mental health service but not meet criteria for psychiatric diagnosis (DeJong, 2010). Screening tools are helpful assessments as they can capture symptoms that would not meet diagnostic threshold but require support. Nonetheless, it should be noted that in this review, where diagnostic assessments were used to calculate the estimates, lower prevalence rates were generally reported. These methodological differences are longstanding challenges that are likely to have contributed to the high levels of heterogeneity in the pooled prevalence estimates (Polanczyk et al., 2015). Although heterogeneity was high, meta-regression was not appropriate for sub-group analyses, as a minimum number of ten articles are recommended for these analyses to achieve adequate power (Higgins et al., 2022).
The current review offers a synthesis of research published in English using a search strategy consisting of Anglocentric terms for residential care. There is huge variety in the terminology used to refer to children’s residential care therefore, relevant articles may have been omitted. The challenge of inconsistency in the terminology used internationally to define types of residential care is not novel to this review (James et al., 2021; Porter et al., 2020). Cross-national collaboration between researchers is needed in future research to increase the consistency in the provision of and language surrounding children’s residential care. Although the search strategy included a range of terms for mental health disorders and symptoms, a greater number of terms related to disorders were included meaning some relevant articles about mental health symptoms may have been omitted.
Recommendations for research
This review confirms the need for a more robust evidence base around the prevalence of mental health among children living in residential care internationally. Epidemiological research is needed that uses a robust methodology to assess the prevalence of mental health among children living in residential care and compare these rates to children living in other care settings. The current review included a small number of studies with high levels of heterogeneity in the results; therefore the reliability of the prevalence estimates is unclear, requiring verification in a larger meta-analysis. The seminal paper by Ford and colleagues was the only peer-reviewed article in the review, which included a comparison group of children living in foster care, kinship care and the community. Their results evidence the higher prevalence rate of mental health disorders among children living in residential care (Ford et al., 2007). However, the dearth of such research limits our understanding of the distinct mental health and support needs of the residential care population, as well as causal pathways to their mental health difficulties. A clear description of the definition and type of residential care, including the children’s characteristics, should be included in the articles.
Several groups of children are under-represented in research about mental health among children living in residential care, which is reflected in the current review. The included articles reported on the ethnicity of the participants to differing extents, and no articles compared the prevalence rates of mental health difficulties between ethnic groups. Research should study the mental health of these children including those from minority ethnic groups, children with intellectual disabilities, UASC and LGBTQ youth and children. Research should also assess the prevalence of PTSD, rule-breaking behaviour, aggressive behaviour, psychosis, sexual concerns, dissociation, and social problems, as this research was generally lacking in the review.
Recommendations for practice
The review findings highlight the importance of routine and comprehensive mental health screening. Assessment of children’s mental health whilst living in residential care should not be considered in isolation from wider social challenges (Hiller et al., 2022). In addition to carer report, where possible, the perspectives of children, social workers and teachers should be included in mental health assessments (Luke et al., 2014). This screening should be used to inform social care professionals’ understanding of the child’s needs to guide care planning and the provision of support. There should be streamlined processes, without extensive wait times, for children who require access to further specialist mental health input. Mental health practitioners need training to accurately diagnose mental health difficulties and make decisions about appropriate evidence-based treatment for children living in residential care (McGuire et al., 2022).
At every level, there should be an understanding of the children’s mental health and services available to meet this need. Children’s relationships with residential care staff should be recognised as key to accessing support, as caregivers are often gatekeepers to mental health services (Schneiderman et al., 2012). Children need consistent carers whom they can trust and share their experiences with in order to establish a sense of security in their environment (Moore et al., 2018). However, there is a lack of stability in residential care due to the high turnover among staff (Porter et al., 2020). Factors such as the absence of appropriate training, support, and supervision contribute to this lack of staff retention (Colton & Roberts, 2007).
Research has shown that children in residential care do not always receive mental health support when there is an identified clinical need (Sainero et al., 2014). In line with the National Institute for Health and Care Excellence (NICE) guidelines, children in residential care should be offered a range of child and adolescent mental health services tailored to their needs (NICE, 2021). The guidelines state that these services should be longer-term, trauma-informed, relationship-based, and not impacted by placement changes. Both social care and mental health professionals need training and supervision to effectively implement trauma-informed practice (Sweeney et al., 2016).
Conclusions
This systematic review and meta-analysis is the first study to investigate the type and prevalence of mental health disorders and symptoms among children living in residential care. Despite large heterogeneity between articles, the review evidences the high prevalence of mental health difficulties among the children. Almost half of children living in residential care had behaviours indicative of a clinical level of mental health concern. Externalising problems were more common than internalising problems, and trauma-related symptoms were common among the children. The review suggests that children and adolescents with higher levels of mental health symptoms and disorders might well be managed in residential care settings, given the higher levels of support. However, more research is needed to understand the children's mental health difficulties and how to support them best.
Supplemental Material
Supplemental Material - A systematic review and meta-analysis of the type and prevalence of mental health disorders and symptoms among children living in residential care
Supplemental Material for A systematic review and meta-analysis of the type and prevalence of mental health disorders and symptoms among children living in residential care by Meryl F. Westlake, Saul Hillman, Asa Kerr-Davis, Andrei Viziteu, Miriam Silver, and Dominika Dykiert in Developmental Child Welfare
Footnotes
Acknowledgements
Shade Davies and Shadia Robertson who supported the double screening of the articles.
Author Contributions
Meryl Westlake: Conceptualisation, Article screening, Formal Analysis, Writing- Original draft Saul Hillman: Methodology
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by BERRI Ltd.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.