
Abstract
Dyadic Developmental Psychotherapy (DDP) is a form of psychotherapy for families where children and young people have experienced early trauma or attachment disruption. This study used longitudinal survey data to understand the format of DDP as it is provided in England for children who are adopted or subject of a Special Guardianship Order (SGO), and to analyse the potential effects of DDP on standardised outcomes of child and caregiver wellbeing. Participants were 150 families who received DDP through funding from the Department for Education’s Adoption Support Fund in England between 2018 and 2021. Adoptive parents and special guardians (caregivers) answered surveys at three timepoints; before therapy was provided (baseline), when therapy had ended (wave 2), and 6 months later (wave 3). Linear mixed modelling demonstrated significant improvements in child/young person difficulties in multiple subscales of the SDQ, including emotional difficulties and conduct problems, between baseline and wave 2. In the same time frame, similar improvements in caregiver wellbeing were also observed, as measured by the SWEMBS. These findings suggest an association between the provision of DDP and an improvement in child/young person and caregiver wellbeing on standardised measures, with these improvements maintained 6 months later. Implications and recommendations for future research to substantiate the findings are discussed.
Introduction
Most children who become adopted or cared for by a special guardian (under a Special Guardianship Order in the UK) have previously experienced abuse or neglect and/or childhood trauma(s) and are at increased risk of having or developing mental health problems including into adulthood (Ford et al., 2007; Paine et al., 2021). Secondary effects of these problems can include parents and guardians with severely challenged parenting resources and reduced psychological wellbeing, which in turn can also have a negative impact on child outcomes (Selwyn, 2017; Hannah & Woolgar, 2018). These and other reasons led in 2015 to the establishment by the Department for Education (DfE), part of UK Government, of an Adoption Support Fund (ASF) for England to meet the therapeutic needs first of children who were adopted and later to include those who were cared for by special guardians. The children accessing a range of therapies through this funding have been identified as having very significantly elevated mental health needs compared with other children in the overall population (King et al., 2017; Burch et al., 2021), with 80–90% having needs in the clinical range (Burch et al., 2021). Similarly, the parents and special guardians caring for these children had significantly worse emotional wellbeing needs compared with the overall adult population (King et al., 2017; Burch et al., 2021).
Dyadic Developmental Psychotherapy (DDP) has been one of the most frequently ‘matched’ therapies with children and families receiving funding through the ASF (Burch et al., 2022). DDP is a type of therapy designed to help children and young people with psychological difficulties resulting from previous trauma and experiences, and their foster carers, guardians, or adoptive parents. The aim is for the child and their ‘caregiver’ to build a healthy and secure relationship, where the child can trust their caregiver and feel comfortable, for example with safe physical contact and expressing emotions (Hughes et al., 2015). The therapy is based on Bowlby’s attachment theory, which explained that children with past trauma will struggle to build secure future attachments (Bowlby, 1988).
In many cases, DDP initially involves only the caregiver(s) in learning about the approach and their role in the therapy. The DDP therapist judges when it is the appropriate time for the child to join in the therapy and, when they do so, the therapist assists the child to communicate their past experiences and feelings with their caregiver(s) (DDP Network, 2022). The therapist interacts with the child through the principles of PACE (playful, accepting, curious and empathic), and a key focus of the therapy is intersubjectivity (Becker-Weidman & Hughes, 2008). The number of sessions involved in this process is not pre-determined.
DDP is currently provided in the UK by private therapists or therapy organisations, adoption and fostering charities, regional adoption agencies, or NHS Child and Adolescent Mental Health Service (CAMHS). Although commonly used as a therapy, it is not supported by NICE, as they recommend that a robust randomised controlled trial must first be undertaken to prove the efficacy of DDP (NICE, 2015).
Current evidence of the effectiveness of DDP for the children of interest to our study is not extensive and focuses mainly on qualitative data from adoptive children and families. The main quantitative study of its effectiveness was undertaken by Becker-Weidman (Becker-Weidman, 2008b). The study followed one group of adopted children who had and another who had not received DDP. At the beginning of the intervention period, the children’s caregivers completed the Child Behaviour Checklist (CBCL) and The Randolph Attachment Disorder Questionnaire (RADQ), and these were then repeated around a year after DDP, and after an average of 4 years. The results of the data collected immediately after DDP (around a year after the first assessment) showed that scores on the CBCL had improved in a statistically significant way for the treatment group, and this was not observed in the control group (Becker-Weidman, 2006). Furthermore, at the follow-up 4 years later, the treatment group were still displaying statistically significant improvements in the RADQ and CBCL measures, whereas the control group had deteriorated, scoring worse than in the initial follow-up (Becker-Weidman, 2008b). However, the methodology of these studies has been questioned, with criticism from at least one research team that the study did not use randomization, and that evaluation was not blinded (Mercer, 2014).
Other studies have been based on qualitative data from interviews with adoptive parents after a DDP intervention has been completed. One such study included semi-structured interviews with 12 parents who had each taken part in at least six sessions of DDP. Themes emerging from these interviews were that DDP had given parents an increased understanding of their child and taught them a new method of parenting with acceptance, with all but one of the parents interviewed feeling the intervention had been beneficial (Wingfield & Gurney-Smith, 2018). Another study of interest was an evaluation of the ‘Nurturing Attachments’ programme, a family intervention informed by DDP. Eight adoptive parents were interviewed and findings included that parents felt the intervention had helped them to form secure attachments with their children, that it had led to a shift in their perspective about their child and their difficulties, and was something they felt confident to continue building on after the intervention ended (Hewitt et al., 2018).
Previous studies have not, to our knowledge, looked at the possible effects of DDP on adoptive parents or special guardians using a quantitative measure to specificially measure their own wellbeing.
Study Objectives and Context
This study aimed to build on the existing research by observing characteristics of the DDP journey and measuring changes in questionnaire measures of caregiver and child functioning from before to after DDP therapy had been provided. The specific areas we measured were (1) caregivers’ emotional wellbeing; (2) adopted children’s emotional and behavioural functioning at three points from baseline (pre-treatment) to 6 months post-treatment. The children and families subject of the study were all recipients of therapeutic support funded by the ASF between 2018 and 2021. The research questions were as follows:
Research Question 1: How does overall child emotional and behavioural functioning change from baseline to after DDP and to 6 months post-treatment?
Research Question 2: How does overall adoptive parents’ and special guardians’ (caregivers’) emotional wellbeing change from baseline to after DDP and to 6 months post-treatment?
Method
Participants and Procedure
Adoptive parents and special guardians (caregivers) notified that ASF funding for therapeutic support had been approved in relation to their child were asked by the local or regional agency who had supported the ASF application if they would like to participate in the evaluation study, which was funded by the Department for Education. Caregivers decided whether to participate based on information that was shared with them in advance about what was involved, including that participation was completely voluntary, and what would happen to their data. The study design was approved by the relevant Research Ethics Committee, reference EOR/SBR/2017/025.
Between November 2018 and November 2021, 1008 caregivers participated in a baseline survey as part of the evaluation of the ASF, with 783 completing a wave 2 survey after therapy had finished, and 683 completing a wave 3 survey, 6 months later. Within this whole group, 150 families were identified who reported at wave 2 that they had received DDP through the Fund or were nearing the end of DDP therapy (the DDP sample). This is the sample of participants whose longitudinal data this paper will analyse.
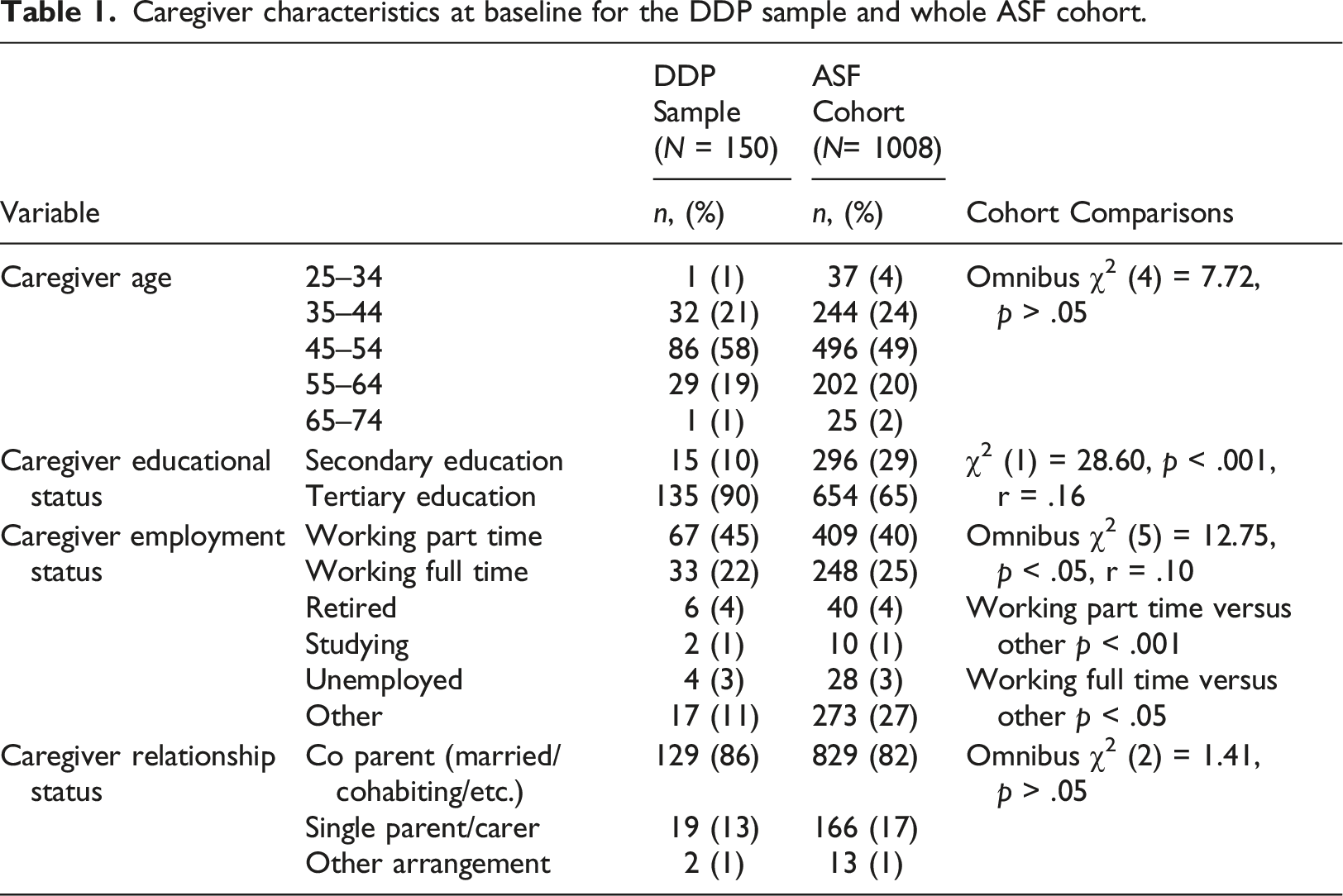
Caregiver characteristics at baseline for the DDP sample and whole ASF cohort.
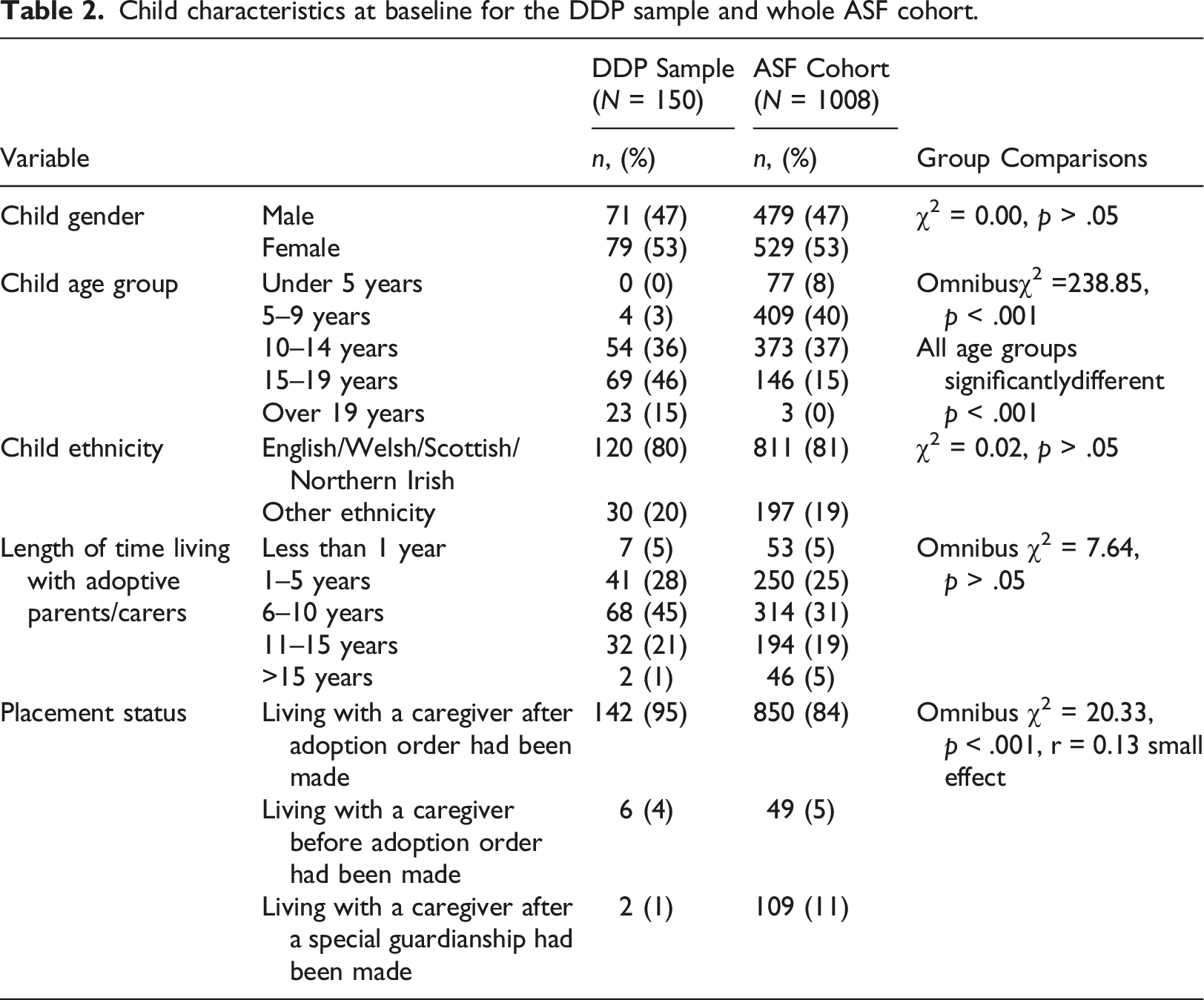
Child characteristics at baseline for the DDP sample and whole ASF cohort.
There was no significant difference between the mean age of the DDP child cohort and the ASF child cohort (mean = 48.84, SD = 8.229), and no significant difference in the frequencies of caregiver relationship status between the two cohorts. The caregivers’ educational status was divided into two levels: secondary education - all levels of secondary school education; and tertiary education - Technical College, professional education or University education. The DDP sample caregiver characteristics differed from the larger ASF cohort regarding caregiver educational status (χ2 (1) = 28.60, p < .001, r = .16 small effect) and caregiver employment status (χ2 (5) = 12.75, p < .05, r = .10 small effect).
142 of the children (95%) in the DDP sample were living with adoptive parent(s) after an Adoption Order had been made, with the other children living with adoptive parent(s) before an Adoption Order was made (N = 6) or living with a special guardian (N = 2). This was significantly different to the placement status frequencies of the whole ASF cohort ((χ2 = 20.33, p < .001, r = 0.13 small effect). 71 of the children in the DDP sample were male (47%) and 79 were female (53%) which was identical to the gender proportions in the full ASF cohort. At baseline, the children in the DDP sample’s age ranged from 5 to 21 years (Mean = 10.16 years, SD = 3.48) with the majority aged 15–19 years (46%, n = 69). The age frequencies of the DDP sample were significantly different to the full ASF cohort (χ2 = 238.85, p < .001, r = 0.45 large effect). There was no significant difference in ethnicity frequencies between the DDP sample and full ASF cohort (χ2 = 0.02, p > .05). The mean length of time living with caregivers in the DDP sample was 7.60 years (SD = 3.82) and this did not differ significantly (p > .05) from the ASF cohort.
Measures
Information from Surveys about DDP Sessions
To gain an understanding of the participating families’ journeys through the DDP sessions, the wave 2 survey asked about the number of sessions accessed and their setup. Furthermore, the survey asked approximately how many sessions were attended by the caregivers or children alone, and how many the family had attended together.
The outcome measures caregivers were asked to complete at each stage of the longitudinal survey are outlined below.
SDQ
The Strengths and Difficulties Questionnaire (SDQ) is a brief emotional and behavioural screening questionnaire for children and young people. This measure was completed by the primary caregiver about their child. The measure consists of 25 items with three response options: not true, somewhat true or certainly true. The items can be grouped into five subscales of five items: emotional problems, conduct problems, hyperactivity problems, peer problems and prosocial behaviour (Goodman, 1997). The subscales are scored according to the manual, obtaining continuous scores from 0 to 10. Higher scores indicate greater problems and increased odds of mental disorder (Goodman & Goodman, 2009). Cut-off scores for each subscale have been established (Goodman, 1997). The SDQ Impact Supplement includes questions about whether the child has a mental health problem, (‘No’, ‘Minor difficulties’, ‘Definite difficulties’ or ‘Severe difficulties’) and if so, chronicity, associated distress, impact and burden related to the child’s difficulties (Goodman, 1999). The measure has good reliability and validity; Cronbach’s alpha = 0.73, test-retest reliability = 0.62 (Goodman, 2001).
SWEMWBS
The Short Warwickshire-Edinburgh Mental Wellbeing Scale (SWEWMBS) was completed by caregivers at each stage of the study. SWEMWBS is used to measure adult emotional wellbeing and contains 7 items, which were originally drawn from the full version of the scale, the Warwickshire-Edinburgh Mental Wellbeing Scale, or WEMWS (Stewart-Brown, et al., 2009). Each item is scored on a 5-point Likert-type scale ranging from ‘None of the time’ to ‘All of the time’.
Studies have indicated that the full WEMWBS scale has good validity and reliability for measuring mental well-being in the UK population who use spoken/written English (Tenant, et al., 2007). The score for SWEMWBS ranges from 7 to 35, where the highest score indicates greater mental well-being. Reliability and validity of the SWEMWBS has not been assessed for most populations but internal consistency has been assessed as good in the UK general population, with Cronbach’s alpha calculated as 0.84 (Ng Fat et al., 2017). Rogers et al. (2018) reported a 2 weeks’ time test-retest reliability index of 0.84 for SWEMWBS in the deaf British sign language user’s population.
Procedure
The data used in the study was collected within the three waves of the ASF evaluation, which ran from 2018 to 2021. Collection was through three surveys online, using Smart Survey. A helpdesk staffed by trained researchers was available in case families had questions when undertaking the surveys. Families were recruited through a local authority or regional adoption agency social worker or support worker, who obtained their mostly verbal consent to take part in the evaluation.
The baseline survey aimed to catch respondent families after they had been approved for the support funding but before support had started, or as close as possible to when support had commenced. The first follow-up (wave 2) survey was completed by families close to the end of their funded DDP, and the final (wave 3) survey around 6 months later.
Changes during the COVID Pandemic
It is important to note that, for some families, the DDP therapy was accessed during a period of COVID-19 Pandemic lockdowns. Therefore, the survey for families completing a wave 2 survey from 29th June 2020 onwards (whose support might be affected) were asked about the effect of the Pandemic on the support they received (whether sessions had been cancelled, provided online rather than in person, or if there was no change to the planned way it provided). The results of this will be outlined in the results section.
Statistical Analyses
The first step in the analysis was to plot the mean standardised measures total and subscale scores by time. Visual examination of the histograms and scatter plots suggested a normal distribution and a linear relationship between time and change. In addition, a normal distribution was found when we plotted the residuals to check the assumptions of an LMM. Assessment intervals varied across participants from Baseline to wave 3.
We chose linear mixed modelling (LLM) for its utility in analysing correlated data typical of longitudinal designs. The reason for this was that only a subset of the sample completed all three surveys and repeated measures ANOVA’s require complete cases (Field, 2018). The mixed model analysis involved several steps and was conducted as an iterative process to identify significant predictors for each of the main measures. To prepare for the mixed model we transformed the dataset from a wide into a long format in SPSS so that each row presented one measurement rather than one case (i.e., one respondent). As a first stage we selected the estimation method (Restricted Maximum Likelihood (REML) or Maximum (ML)). Next, we decided on the covariance structure overall. This was done by comparing -2LogLikelihood (-2LL), Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) scores of the models with different covariance structures. The best-fitting covariance structure was an unstructured covariance matric. Autoregressive, diagonal and compound symmetry covariance structures were tested, but neither resulted in improved fit of the model. Once covariance structure was chosen, we added the fixed effect of intercept and time to the model. As this was significant for four outcome models, we added a random effect for the intercept and slope. Other covariates and factors were added as an iterative process to decide on the best fit for the model. Potential predictors included wave of study, amount of DDP sessions received overall, age, gender, ethnicity of the child as well as demographic information of the respondent. LMM allows for a dynamic understanding of how variables of interest change over time.
Results
Descriptive Statistics
Dyadic Developmental Psychotherapy
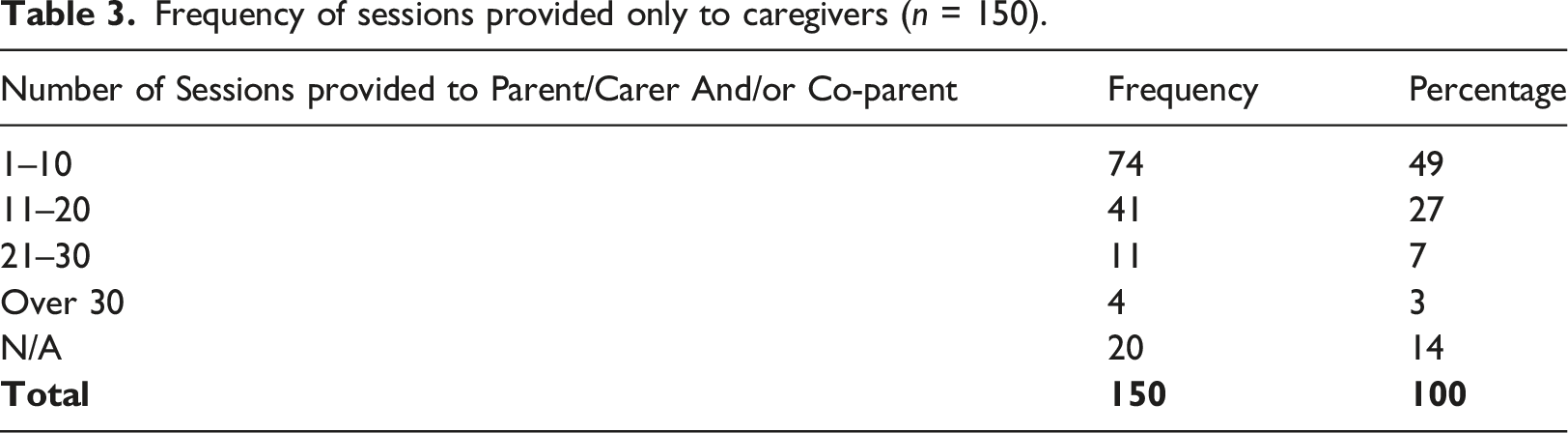
Frequency of sessions provided only to caregivers (n = 150).
Frequency of caregivers and children receiving sessions together (n = 150).
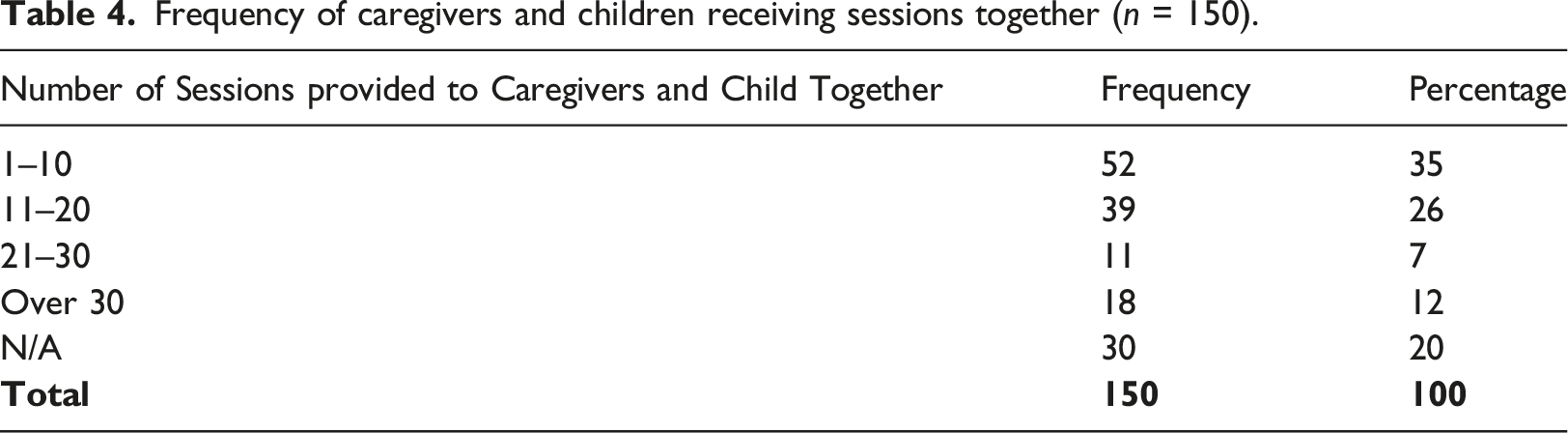
The mean number of DDP sessions of support provided to caregivers on their own was 11 (SD = 8). Nearly three-quarters of caregivers (71%) and/or their co-caregivers had 1-20 DDP sessions on their own with 14% having over 30 sessions without their child being present (Table 3). The mean number of DDP sessions of support given to caregivers together with their child was 15 (SD = 11). Approximately two-thirds (61%) caregivers reported having 1–20 DDP sessions together with their child, with 12% receiving over 30 DDP sessions together with their child (Table 4).
The impact of COVID on DDP therapy
Of the DDP cohort, 43 caregivers (29%) provided wave 2 data before the period of the COVID-19 Pandemic and 107 caregivers (71%) provided wave 2 data during the period of the Pandemic. Ninety-three percent of these 107 respondents described how their DDP support did not continue completely as planned during the period of the Pandemic. Only 7% said that some of their DDP support had been cancelled as a result. Nearly one fifth (17%) reported that some of their DDP support had been suspended for a time but continued later. One third (33%) agreed that, whilst all DDP sessions continued, the way in which the support was provided altered (i.e., switched to using remote methods) and 13% reported that only some of their DDP sessions continued to be provided, mostly switched to using remote methods such as telephone calls and/or online. Statistical analysis of the outcome measures for the Pandemic versus non-Pandemic affected groups revealed no significant differences over time.
Outcome Measures
Descriptive statistics for all outcome measures Total and Subscale Scores by wave of survey.
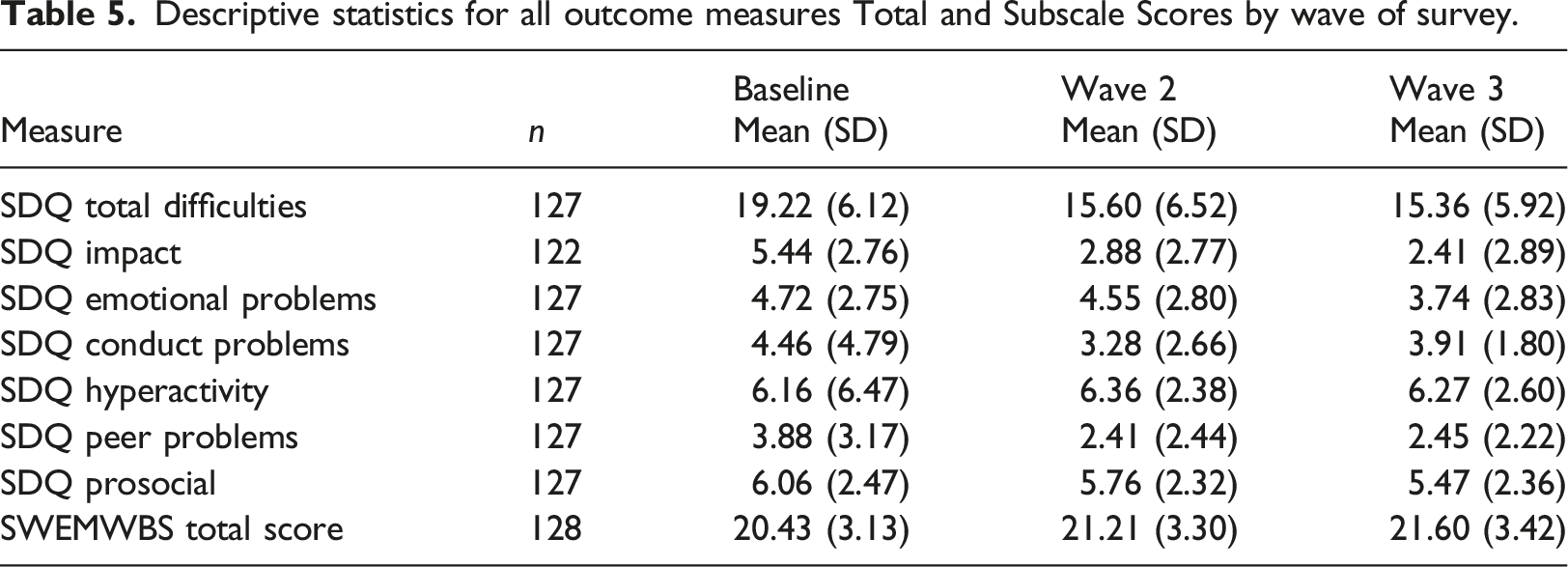
Figure 1 illustrates children and young people’s SDQ Total difficulties scores over time. SDQ Total difficulties by wave of study.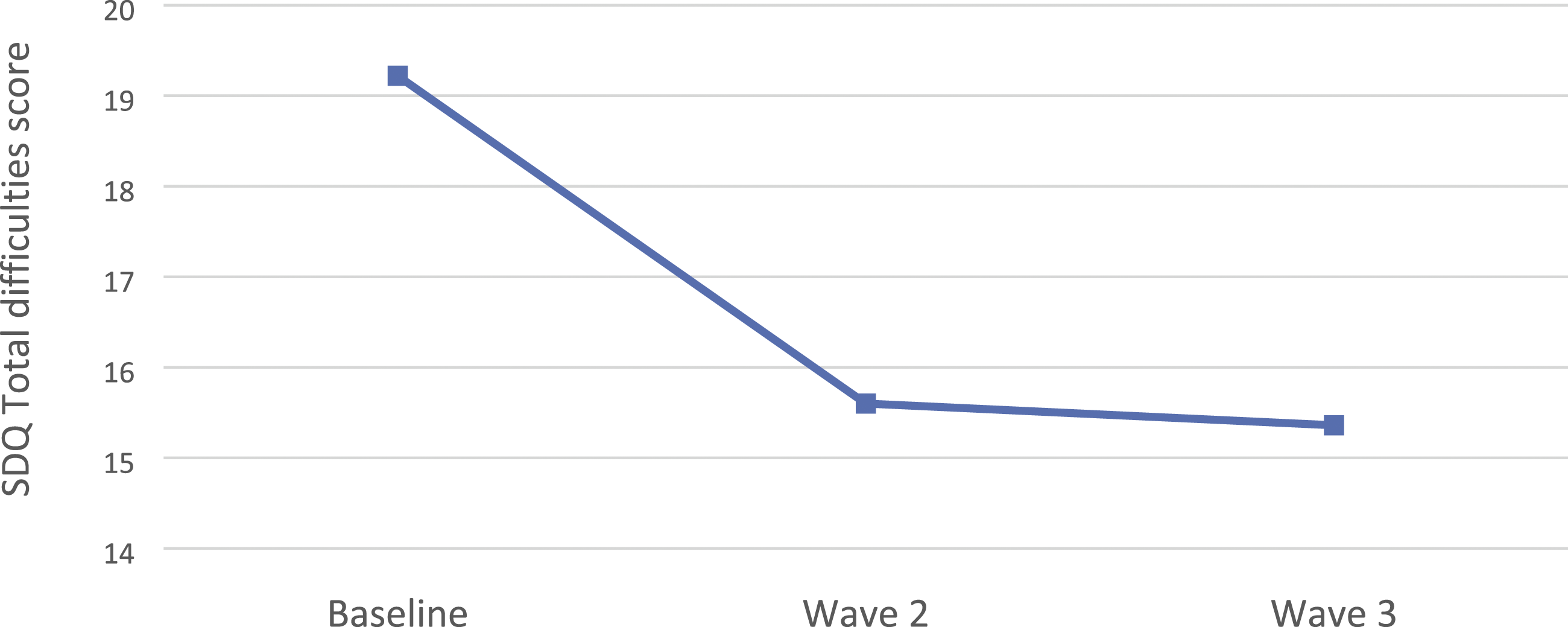
Figure 2 illustrates children’s SDQ sub scale scores over time. SDQ subscale scores by wave of study.Note: E = Emotional problems; C = Conduct problems; H = Hyperactivity; PP = Peer problems; P = Prosocial, I = Impact.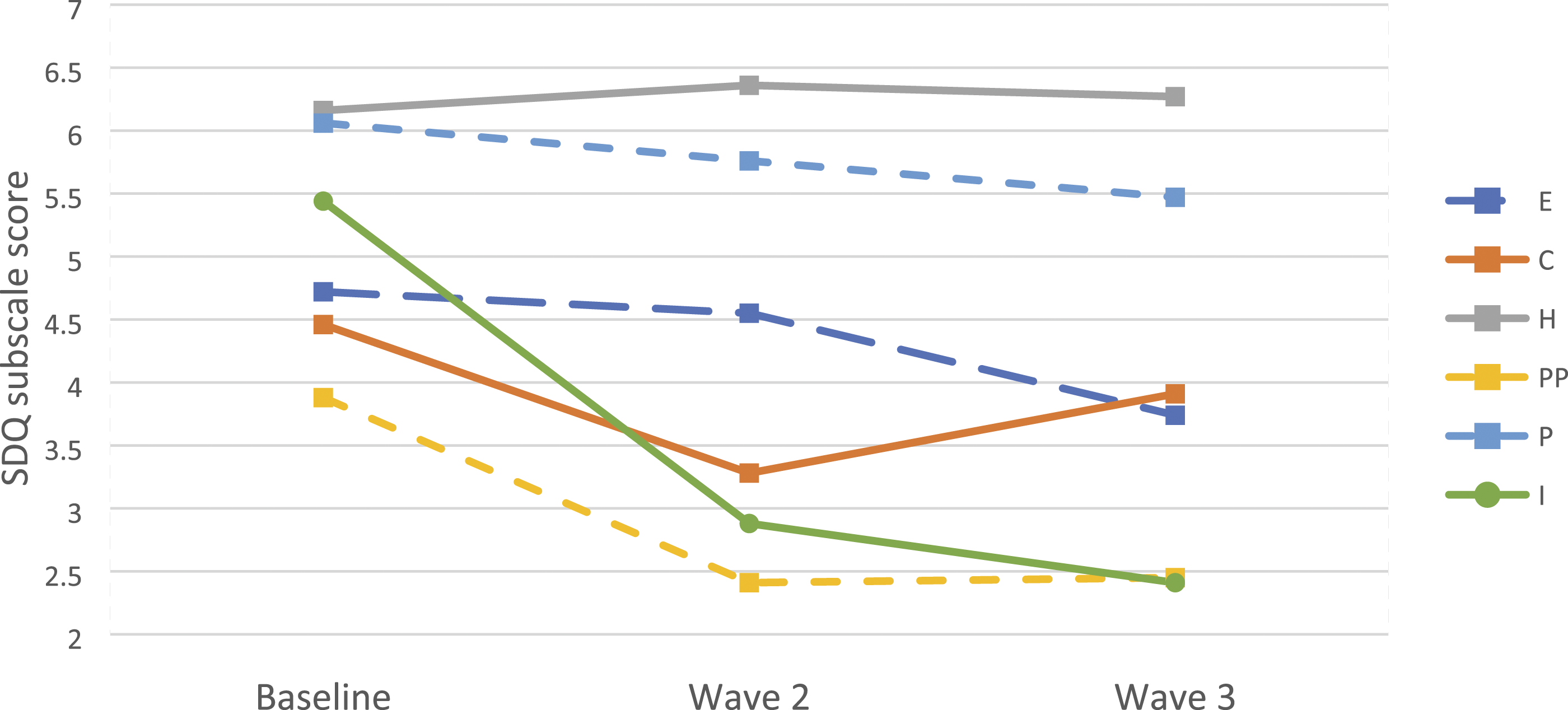
Figure 3 illustrates caregivers’ SWEMWBS scores over time. Caregivers’ SWEMWBS scores by wave of study.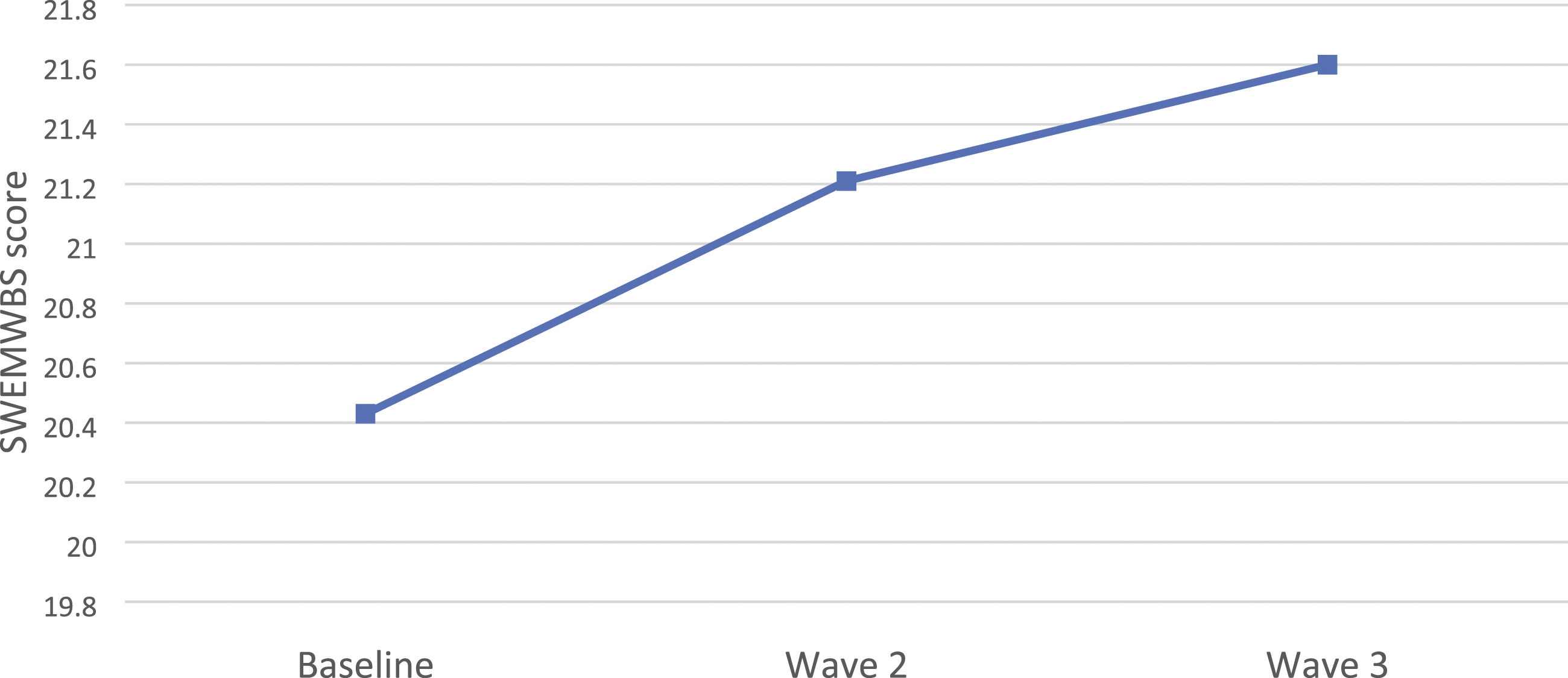
Main Analyses
SDQ Total Difficulties
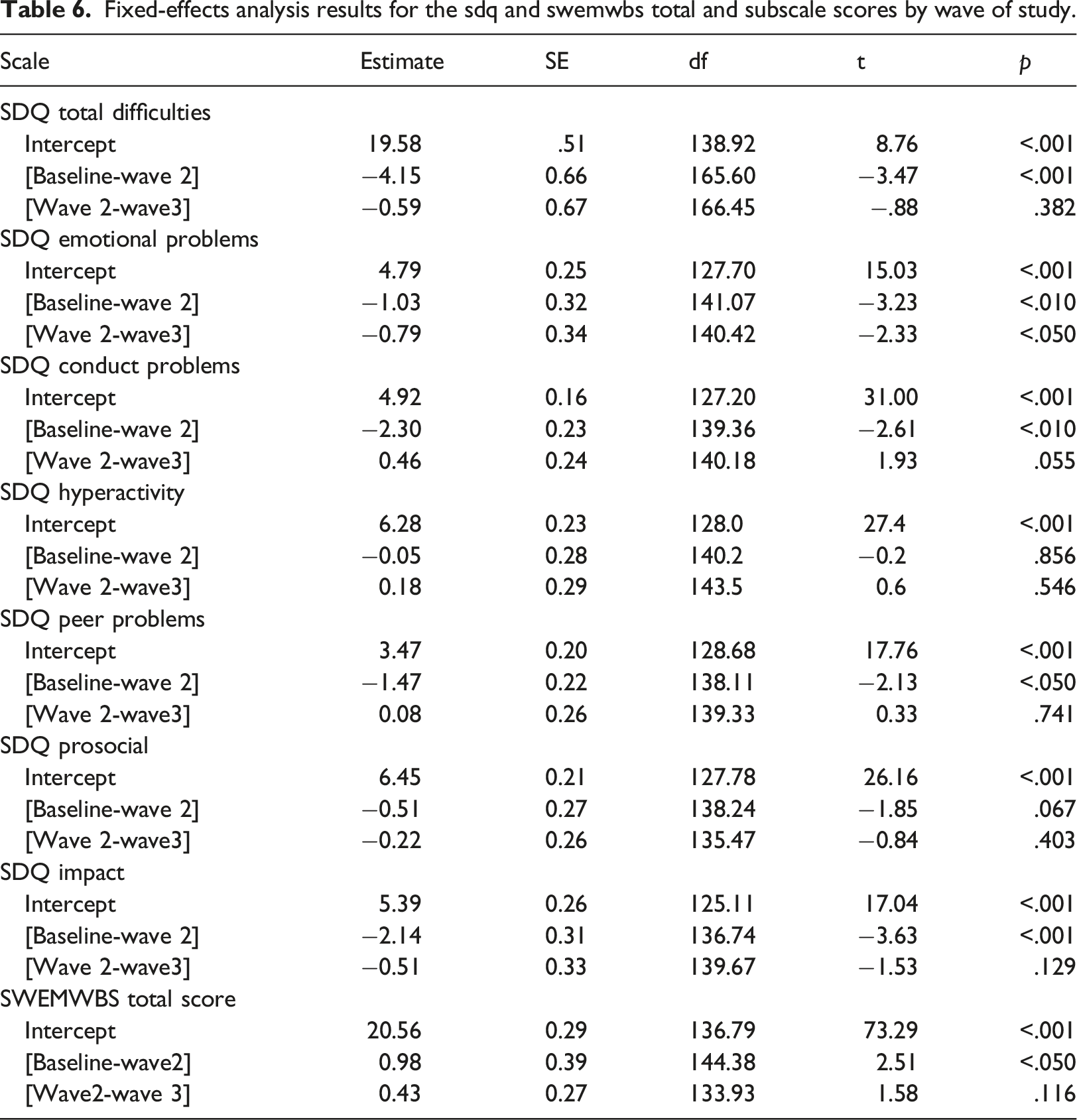
The children’s emotional wellbeing and behaviour (before and after receiving DDP) was explored initially by examining their baseline to wave 3 caregiver-report SDQ Total difficulties, with time as a predictor. As seen in Table 5, the baseline expected SDQ Total difficulties score was 19.58 which is above the British national norm of 8.4. This figure indicates a very high level of pre-intervention Total difficulties based on results from a population-based UK survey (Meltzer et al., 2000).
There was a significant reduction (indicating improvement) in the children’s caregiver reported SDQ Total difficulties scores from baseline before the DDP intervention began, to wave 2, just after the end of the intervention (p < .001, Cohen’s f2 = 0.15, medium effect). Specifically, for change across time for the baseline to wave 2 period, there was an expected 4.15-point significant decrease in children and young people’s SDQ Total difficulties scores (Table 5). From wave 2 to wave 3 (from end of intervention to 6 months’ later), children’s SDQ Total difficulties scores remained stable i.e., did not significantly change (p = .38).
Fixed-effects analysis results for the sdq and swemwbs total and subscale scores by wave of study.
SDQ Impact
At baseline, the expected SDQ Impact subscale score was 5.39. This compares with a British national norm of 0.4 and is classified by the programme developers as ‘very high’ (Youth in Mind, 2016). As shown in Table 5, a significant reduction in the rated impact on the family of 2.14 points occurred from baseline to wave 2 (p < .001, Cohen’s f2 = 0.24, medium effect). The SDQ Impact subscale scores did not significantly change from wave 2 to wave 3. These results suggested that impact on the family reduced from baseline to wave 2 to the lower end of the very high category according to the SDQ developer’s classification (Youth in Mind, 2016). During wave 2 to wave 3 of the study, SDQ Impact scores did not show significant fluctuations.
As with SDQ Total difficulties, inspection of the random-effects analysis results for the SDQ Impact scores (Table 5) indicated that participants varied in both their starting points (p < .001) and rates of change baseline to wave 2 (p < .001) and wave 2 to wave 3 (p < .01). Covariance parameters showed a significant positive association between intercept and change within the baseline to wave 2 period (p < .001). This finding again suggests that a subset of families experiencing the greatest family impact at baseline tended to have greater increases, or less of a decrease, in perceived family impact during the baseline to wave 2 period.
SDQ Emotional problems
As seen in Table 5, the expected SDQ Emotional Problems subscale score at baseline was 4.79. This score can be categorised as high based on the findings from a population-based UK survey of over 10,000 children (Meltzer et al., 2000). Fixed effects analysis results (Table 5) showed a significant reduction in child Emotional Problems subscale scores from baseline to wave 2 (p < .01) of 1.03 points, and a significant reduction from wave 2 to wave 3 (p < .05, Cohen’s f2 = 0.03, small effect) of 0.79 points.
Closer inspection of the patterns and relationships in intercept and change trajectories revealed that participants varied in both their intercept (p < .001) and their rates of change in SDQ Emotional Problems subscale scores baseline to wave 2. Furthermore, the covariance parameters suggest a significant positive association between the intercept and change within baseline to wave 2. This finding suggests that participants with high SDQ Emotional Problems subscale scores at the baseline tended to have greater increases, or less of an improvement, in SDQ-assessed Emotional Problems from baseline to wave 2. There was no significant correlation between the intercept and change within the wave 2 to wave 3 period.
SDQ Conduct Problems
At baseline, the expected SDQ Conduct problems subscale score was 4.92 (Table 5). This is significantly greater than the British norm of 1.6 and is classified as high (Youth in Mind, 2016). The baseline to wave 2 period suggested that there was a significant 2.30-point improvement in children’s Conduct problems (p < .01, Cohen’s f2 = 0.11, small effect). The Conduct problems subscale scores did not significantly change from wave 2 to wave 3.
The patterns and relationships in intercept and change trajectories revealed that participants varied in both their intercept (p < .001) and their rates of change in SDQ Conduct problems subscale scores baseline to wave 2 (p < .001). Furthermore, the covariance parameters suggested a significant positive association between the intercept and change within baseline to wave 2 (p < .001). This finding suggested that participants with the highest SDQ Conduct problems subscale scores at the baseline tended to have increases in the SDQ measured Conduct problems from baseline to wave 2. Like SDQ Emotional Problems, there was no significant correlation between the intercept and change within the wave 2 to wave 3 period.
SDQ Peer Problems
At baseline, the expected SDQ Peer Problems subscale score was 3.47 (Table 5). The baseline to wave 2 period suggested that there was a significant 1.47-point improvement in peer problems (p < .05, Cohen’s f2 = 0.05, small effect). Child peer problems subscale scores did not significantly change from wave 2 to wave 3.
Participants varied in both their starting points (p < .001) and rates of change in Peer problems subscale scores within the baseline to wave 2 period (p < .001). Furthermore, the covariance parameters showed a significant positive association between starting point and change within the baseline to wave 2 period (p < .001) and the wave 2 to wave 3 period (p < .01). This finding indicated that participants with the highest Peer problems subscale scores at baseline reported increases in Peer problems, rather than a reduction like that observed in the main trend, from baseline to wave 3.
Hyperactivity and Prosocial scores
Wave of study did not significantly predict Hyperactivity, F (2144.47) = .94, p = .39 and Prosocial scale scores, F (2141.61) = 2.76, p = .07.
SWEMWBS
At baseline, the expected SWEMWBS score was 20.56 (see Table 5). The baseline to wave 2 period of the study suggested that there was a significant 0.98-point improvement in SWEMWBS total score (p < .05) for caregivers. Caregivers’ SWEMWBS total scores did not significantly change from wave 2 to wave 3.
SDQ and SWEMWBS total and subscale scores, variances, and correlation matrix.
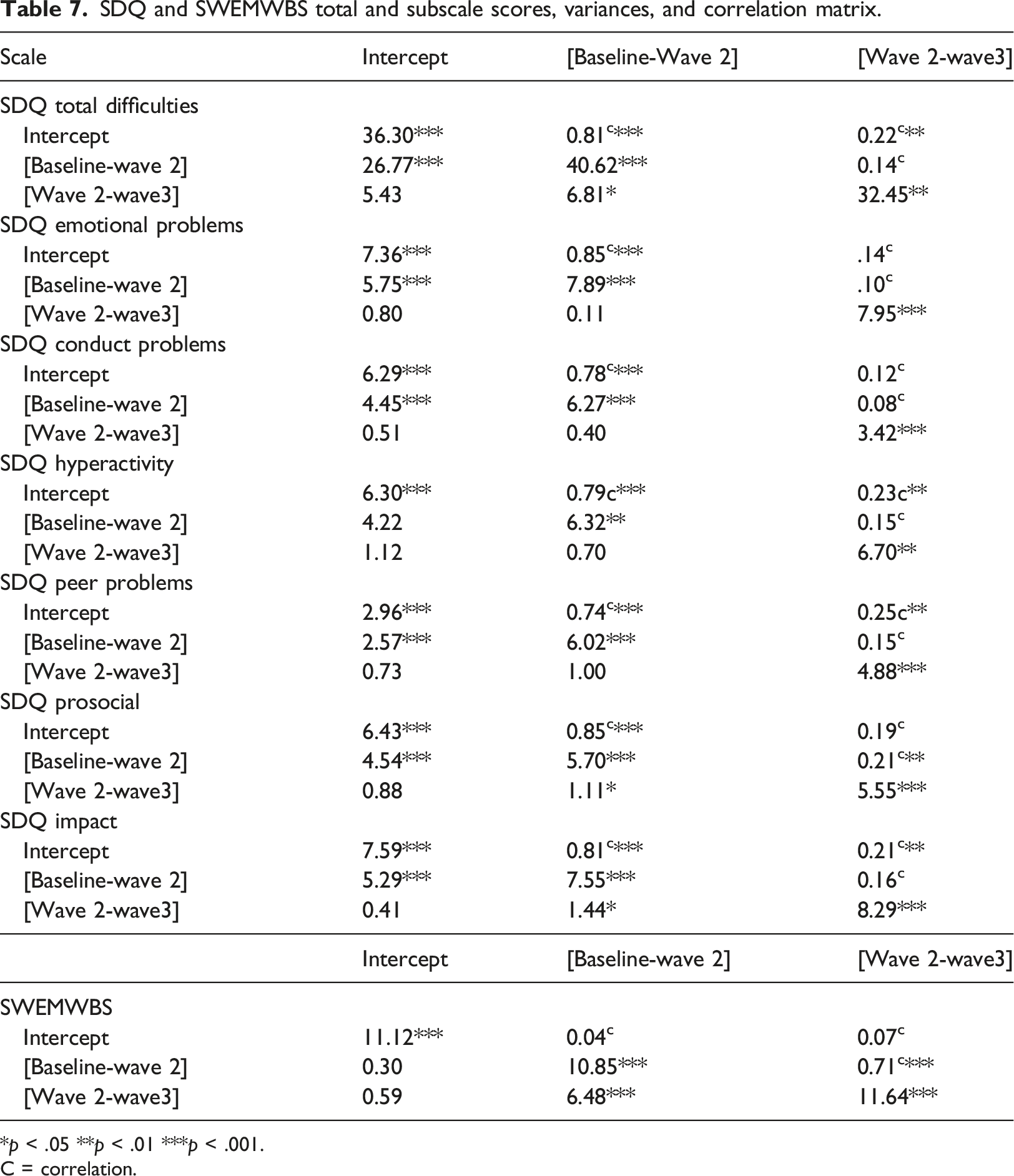
*p < .05 **p < .01 ***p < .001.
C = correlation.
Discussion
SDQ scores of children in the DDP cohort varied in their starting points and rates of change over time. However, on average, caregiver reports suggested that children receiving DDP started their interventions with high levels of SDQ Total Difficulties and showed significant reductions in these difficulties from baseline to wave 2 (around the end of the intervention). Expected SDQ Total Difficulties stabilised from wave 2 to wave 3, as did the constructs captured in three of the subscales of the SDQ: peer problems, conduct and prosocial behaviour. The exception to this pattern were children’s caregiver-reported emotional problems which also decreased in a significant way between wave 2 to wave 3, suggesting ongoing improvements in this area at 6 months after the DDP sessions had ended. Two SDQ subscales - hyperactivity and prosocial – showed non-significant changes over the study duration.
SDQ significant score improvements within most subscales and Total Difficulties were maintained between wave 2 and wave 3. This suggests that any improvements in SDQ ratings, including those that may have been associated with the provision DDP, were maintained approximately 6 months after the period where DDP was provided. DDP aims to support caregivers and their children to develop skills to help to co-regulate the child’s emotions together (Hughes, 2017), and these findings of a maintained improvement in SDQ scores over time suggest that the process could be ongoing and cumulative. However, longitudinal follow-up would be required to validate this, and other factors which could have impacted SDQ score changes over time must be controlled for.
While SDQ total scores and subscale scores remained high throughout the stages of the study compared to British normative values, reductions in participant scores also represented changes in the measure’s pre-determined severity categories (Youth in Mind, 2016). For SDQ total difficulties, the reduction in scores represented a change from very high (5% of the population) pre-intervention to slightly raised (10% of the population) by the end of the study. Impact scores remained in the very high category (5% of the population) but, by the end of the intervention, families’ SDQ impact scores were at the lower end of the category range. However, the fact that the SDQ subscales and impact score remained at the ‘slightly raised’ and ‘very high’ categories does indicate the need for ongoing support. It was noted in an earlier study that adopted young people are likely to demonstrate complex difficulties throughout their development, and repeated intervention and support may be required (Tarren-Sweeney, 2010).
Looking at the caregiver emotional wellbeing (SWEMBS) scores at baseline, the mean overall score was 20.43, which is around 3 points lower than the estimated mean scores of adults in England (Ng Fat et al., 2017). This would suggest that, before DDP was provided, the caregivers in our cohort had lower overall wellbeing than the general population. Similar to the changes in some of the SDQ subscales, there was a significant increase in scores between baseline and wave 2, suggesting an improvement in caregiver wellbeing which could be associated with the provision of DDP in the period between baseline and wave 2. This improvement was maintained at wave 3, i.e. 6 months after DDP had ended. Previous studies have not, to our knowledge, measured the wellbeing of caregivers, including adoptive parents or special guardians over the time period that their family has revieved DDP. Therefore, these results are encouraging. However, it is important to note that we cannot assume causation between the general trends in improvement in child and caregiver functioning and the provision of DDP.
Although the findings suggest that DDP is associated with an improvement in caregiver and child wellbeing, for a small group of the families in our study, the parent-report child’s difficulties and caregiver wellbeing ratings actually worsened during the study period. This was observed in a sub-group of the children or caregivers who had scored very high in the SDQ or SWEMBS at baseline, suggesting they started with the most severe difficulties. It is important to note that this observation in our study was only a within a small subgroup and that, overall, scores improved across timepoints, before and after the provision of DDP. Nonetheless, previous studies of DDP have not explored with which group(s) of children and families the intervention is likely to be most appropriate and potentially helpful, for example by looking at a child’s baseline severity of difficulties, or caregiver’s wellbeing. This could be further investigated through direct research and services in the future, so that DDP can be tailored to adoptive parents, special guardians or foster carers and children most likely to experience associated benefits.
Study Limitations
The major limitation of this study is that it used a convenience sample and a within subjects design without a control group, which allows for potential threats to internal validity. A control group was not possible in our study because all families recruited into it were already on the pathway to accessing therapeutic support, specifically through the ASF. Therefore, we cannot rule out that scores on the SWEMBS and SDQ would have improved over time, regardless of the intervention (Heppner et al., 2015). Children in middle to late adolescence (the modal age group of the children/young people in the DDP cohort was 15–19 years old) have been shown to experience maturation in areas including emotional stability and agreeableness (Klimstra et al., 2009). Therefore, the improvement shown on the measures over time could reflect the process of the young people growing up.
Therefore, without the inclusion of a control group with similar characteristics as our DDP cohort, we cannot conclude that DDP provision was the driver for improvement in the child and caregiver wellbeing measures over time. In order to strengthen the qualitative and observational data that suggests improvements in wellbeing from before to after DDP for adoptive families, a randomised controlled trial is needed.
A second limitation of the study is that it does not track the adoptive families past 6 months after the end of their DDP intervention. Therefore, we are unable to evaluate the longer-term journeys for the families after DDP, including measuring whether the improvements in reported child/young person and caregiver wellbeing noted at wave 2, and maintained at wave 3, continued.
A third limitation is that, because self-report data was used and only one outcome measure, our ability to triangulate the findings was limited.
A fourth limitation is that, because of the relatively long duration of the DDP experience, study data may be susceptible to maturational and historical influences (Shadish et al., 2002).
A final limitation of the study is that researchers were not able to investigate in detail the content of the DDP sessions that different families had. This is because the scope of the wider evaluation was to look at the overall journey of accessing support through the ASF and the impact of that funded support, rather than the specifics of the therapy accessed. It could be argued that this means we cannot assume the content and quality of all families’ DDP was consistent. This is reflected in the differing number of sessions families had and the differences in the makeup of the sessions. However, DDP is adaptable based on the child’s needs whilst still maintaining the key principles of PACE (Hughes et al., 2015). Therefore, it is to be expected that there is variation in DDP experience for each family. DDP was not provided by a consistent therapist in our study, but this reflects the reality of widely used therapies. In order to practice DDP, therapists have received specific training and supervision (DDP Network, 2022), so their core competencies and approach to DDP should have been consistent across England.
Overall, our study suggests that DDP treatment is associated with an improvement in quantitative measures of a child’s difficulties, and child and caregiver wellbeing in adoptive and special guardianship families. The data has not been collected in a clinical trial environment so lacks a control comparison group, therefore we cannot confidently demonstrate that improvements for children and caregivers over time can be attributed to DDP. However, it adds promising evidence and provides an up-to-date insight of DDP provision in England. The study findings support the hypothesis that DDP should continue to be evaluated as a potentially effective therapeutic intervention for care experienced children and families in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department for Education.