
Abstract
Asylum-seeking children presenting in the shutdown state have been the subject of much discussion and controversy—on both government and medical system levels—in Australia and in Sweden. In this article, we conceptualize the shutdown state as an evolutionary response to extreme threat. We adopt a neuroscience approach to present five plausible models for explaining this shutdown state, their strengths and shortcomings, and the overlaps between them. Model 1—the sustained autonomic arousal model—draws on polyvagal theory. Model 2—the innate-defence model—draws on research pertaining to animal and human innate defence responses. Model 3—the catatonia model—draws on clinical and research data with patients presenting with catatonia. Model 4—the hypometabolic model—draws on an emerging body of work pertaining to hypometabolic states in animals and humans. Model 5—the defence cascade model of dissociation—draws on clinical research pertaining to human trauma states that present as dissociation. At present, each of the models provides a plausible pathophysiological explanation—or a component of a potential pathophysiological explanation—and none of them, for the moment, has enough evidence to be either accepted or disregarded. We hope that our discussion of the models advances scientific discussion and opens up possibilities for effective treatment.
Keywords
Researchers and clinicians have yet to reach a consensus regarding the neurobiology of the shutdown state seen in asylum-seeking children. In an effort to advance the scientific discussion and open up possibilities for effective treatment, we present here a range of plausible models for explaining this shutdown state. First, however, in an effort to frame that scientific discussion, we present brief historical overviews of the Australian experience and then, in turn, the Swedish experience, with the specific aim of embedding the scientific discussion and analysis of the shutdown state within a broader historical understanding of serious trauma and its consequences.
Asylum-seeking children in detention: The current situation in Australia
Over the last decade, the number of men, women, and children displaced worldwide by persecution, conflict, violence, human rights violations, or events seriously disturbing public order has continued to rise; by the end of 2019, the United Nations High Commissioner for Refugees (UNHCR) estimated that the number of forcibly displaced persons had reached nearly 80 million, or 1 in 97 persons (UNHCR, 2020b). Of these, 4.2 million were asylum seekers, including approximately a million children (UNHCR, 2020a; 2020b).
In Australia, refugees seeking resettlement have been managed via a two-tier policy dating to the 1980s (p 143) (Silove & Mares, 2019). Persons arriving with refugee visas, as determined by the annual quota, are provided with a comprehensive and humane program of progressive resettlement. By contrast, asylum seekers arriving without formal refugee status—and in particular, those arriving by boat—are subject to mandatory and indefinite detention. Over time, as numbers continued to increase, detention facilities have been extended to offshore facilities that included Christmas Island (an Australian territory 5500 miles west of Australia), Manus Island (a Papua New Guinea island 1000 miles north of Australia), and Nauru (an island country 2000 miles northwest of Australia). Asylum-seeking men, women, and children have been detained at such facilities for periods ranging from months to years while trying to prove their status as refugees. Asylum seekers detained in Australian facilities have come from South Asia, the Middle East, and Africa (Karlsen, 2016).
The official line about offshore facilities—like the facility at Nauru—has been upbeat. As noted by the Nauru government (Doherty, 2018): Children of refugees and asylum seekers on Nauru have access to education, health services, welfare, good accommodation and a range of social services provided by the Nauru and Australian governments. Nauruan children grow up happy and healthy on our island. Activists [are] playing politics and distorting facts.
But the reality has long been far different. In a 2002 submission to the Australian Human Rights and Equal Opportunity Commission’s Inquiry into Children in Immigration Detention, the Alliance of Professionals for the Health of Asylum Seekers and Their Children (2002) mentioned prison-like conditions and the children’s exposure to ongoing trauma: [The children] have no grass, no dedicated area, no space to be with other infants, play and interact, and hence no stimulation. Other pressures facing children in detention are: the ongoing exposure to trauma of parents and siblings, witnessing acts of violence between officers and detainees, self-harm, mutilation and attempted hangings. (p 18)
These conditions gave rise, in 2017, to a preliminary investigation by the Office of the Prosecutor of the International Criminal Court. And though the Court eventually declined, in 2020, to prosecute, the Office of the Prosecutor specifically noted (pp 3−4) (International Criminal Court, 2020) that the conditions of detention appear to have constituted cruel, inhuman, or degrading treatment . . . and the gravity of the alleged conduct thus appears to have been such that it was in violation of fundamental rules of international law. . . . The alleged detentions appear to have been of sufficient severity to constitute the crime of imprisonment or other severe deprivation of physical liberty under . . . the [International Criminal Court’s, 2020] Statute.
The human toll of these harsh conditions has been profound. Helpless, hopeless, and with no idea how long their detention may continue, children in detention have been exposed to ongoing stress, violence, and human rights violations. Many have exhibited symptoms and disorders commonly seen in children exposed to serious stress: nocturnal enuresis, fear of sleeping alone, clinginess, withdrawal, major depression, posttraumatic stress disorder (PTSD), separation anxiety disorder, and oppositional defiant disorder (Steele et al., 2004).
In addition, some children have withdrawn into a shutdown state where they stopped eating, drinking, talking, and responding to family members and the world at large. A 2001 video of a young boy named Shayan Badraie—secretly screened by Debbie Whitmont, an investigative journalist, and aired on the Four Corners current events program on Australia’s public television network—brought this particular problem into public awareness. The video showed the boy, after 14 months in detention, as being (p 664) (Steele et al., 2004) cradled in his mother’s arms, . . . mute, refusing to eat and . . . too weak to walk. He was being wheeled about the detention center by his parents in a wheel barrow.
As background, during the previous 14-month period of being held in remote, and then urban, detention centers (p 664) (Steele et al., 2004), Shayan had witnessed acute distress among detainees, riots, and self-harming behaviors, including attempted self-immolation. He had been distressed since this time with chronic sleep disturbance, nightmares, and bed-wetting. After transfer to an urban detention center, he witnessed a man attempting suicide by wrist cutting and had become withdrawn and mute. Shayan was found to be dehydrated and underweight and was admitted [to hospital] for rehydration.
Later in 2001, the same year as the Four Corners program, the legislation known as the “Pacific Solution” came into force. It prohibited asylum seekers from resettling in Australia and led to a further “erosion of hope” (Sainty, 2018). Over time, more and more asylum children experiencing the trauma of detention withdrew into the same shutdown state as Shayan (Doherty, 2018; Sainty, 2018). By 2019, at least 30 cases had been documented by Australian health professionals (Isaacs, 2019).
As Australian health professionals came to know about the problem, the overall consensus was that the detention conditions—including the uncertainly about the future and the long time to obtain a decision—were traumatic for children and their families, and that the children’s clinical presentations (including the shutdown state) needed to be understood in the context of this ongoing trauma (American Medical Association, 2018; Amnesty International, 2016; Guardian, 2018; Shoebridge, 2015; Steele et al., 2004). But strong tensions developed between health professionals and the Australian government (Shoebridge, 2015), exacerbated by the enactment in 2015 of gag legislation intended to prevent health professionals from disclosing to the Australian public that children in detention were suffering so severely and, in some cases, even entering the shutdown state (Hasham, 2016).
Asylum-seeking children in detention: The current situation in Sweden
Cases of children entering the shutdown state have not been limited to the detention centers of Australia. A similar phenomenon and pattern of clinical presentation have occurred in children coming from severely traumatized, asylum-seeking families in Sweden (Bodegård, 2005b). These asylum seekers came from Russia and other former Soviet republics, the former Yugoslavia, and Iraq/Syria (von Knorring & Hultcrantz, 2020; Wikipedia, 2021a). Many belonged to ethnic or religious minorities in their homelands—for example, Uighurs, Romani, and Yezidis (von Knorring & Hultcrantz, 2020). In a series of publications, Swedish pediatricians described asylum-seeking children who fell into a stupor state—for a period of months to years—often following a negative decision by Swedish immigration authorities (Bodegård, 2005a; von Knorring & Hultcrantz, 2020). In their countries of origin, many of the children had experienced or witnessed extreme violence—rape, killing, or threatened harm—often against family members (von Knorring & Hultcrantz, 2020). “The child who fell ill was usually the one who had been responsible in the family, who often acted as a translator (the oldest or only son), and/or most often the one who [had] witnessed the most traumatic event in the home country (rape of mother, torture or killing of father)” (p 1107). In Sweden, the number of children in the shutdown state ran into the hundreds.
The Swedish Association of Child and Adolescent Psychiatry screened all child and adolescent psychiatry clinics in Sweden in 2004 and found that 424 refugee children and adolescents 0–20 years had been treated from 2003 to June 2005 because of reduced communication, motor skills, and ability to carry out daily routines. Approximately, 1 out of 3 of the 425 were fed by means of a nasogastric tube as they were unable to eat or drink. Those children who needed a nasogastric tube were also mute and were laying down. They were not moving at all, were hypotonic, and totally disconnected from their environment without any formal or emotional contact with other people. Their eyes were closed all the time. The children did not react to touch, sound, pain, or cold. Most had enuresis and encopresis. Some parents managed to take them on a wheelchair regularly to the toilet (p 1103) (von Knorring & Hultcrantz, 2020).
In contrast to the Australian context, where health professionals saw such states as related to trauma, Swedish health professionals articulated varied hypotheses as to why asylum children were presenting in the shutdown state. Was the shutdown state a response to trauma, or were the children faking in order to influence the asylum process (Bendz, 2005)? Were the children being drugged or manipulated by their parents 1 —as in Munchausen by proxy (Pressly, 2017) (Psychiatry Without Borders, 2019; Sallin et al., 2016; Schieveld & Sallin, 2021)? Could the phenomenon be compartmentalized as a socioculturally transmitted, culture-bound syndrome that influenced the children’s beliefs and expectations (Sallin et al., 2016)? Could the phenomenon be considered a conative disorder—a disorder of purposeful action—where the role of trauma is pushed into the background as secondary and where children are considered to be unconsciously using the shutdown state for secondary gain—that is, to avoid or gain something (Schieveld & Sallin, 2021)?
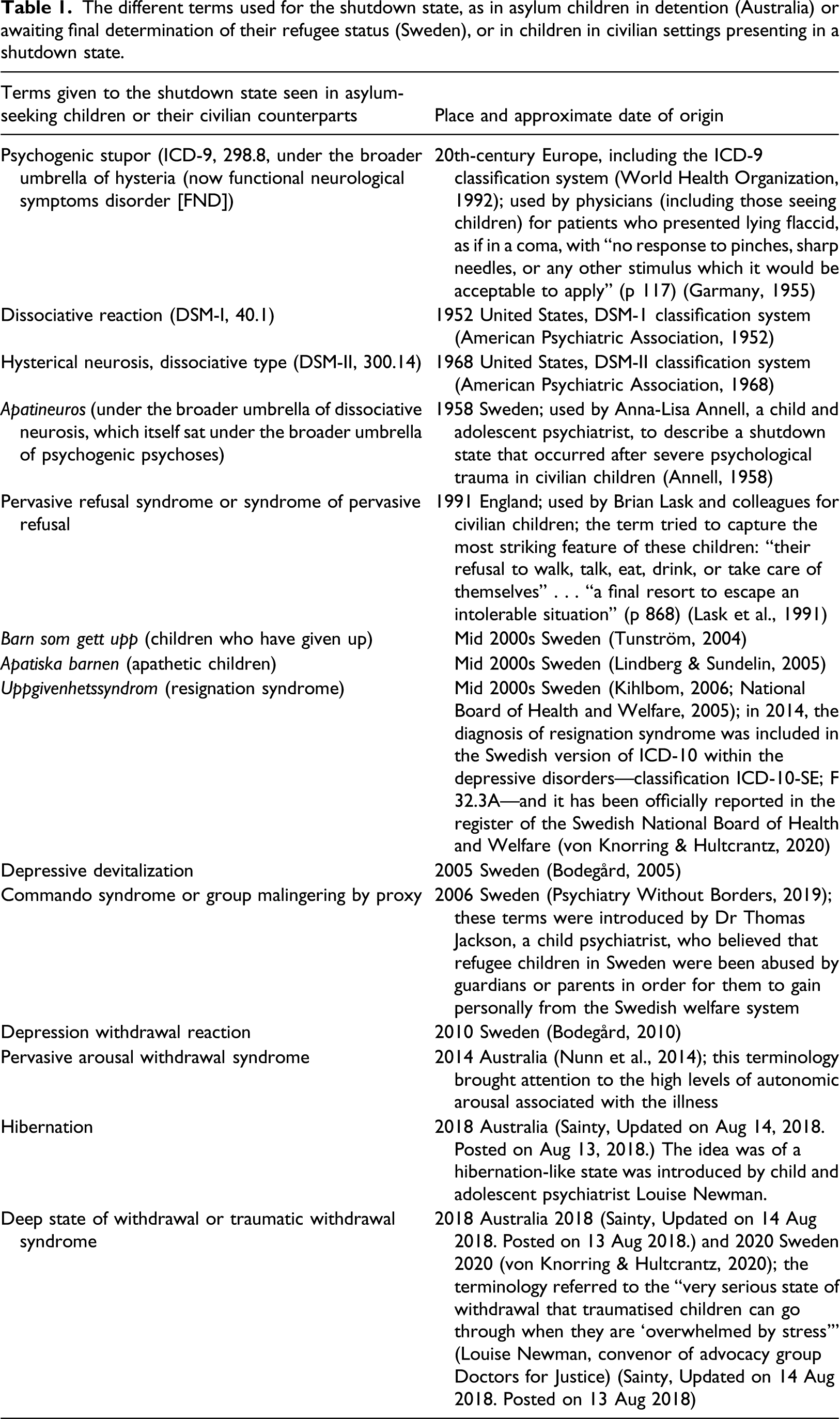
The different terms used for the shutdown state, as in asylum children in detention (Australia) or awaiting final determination of their refugee status (Sweden), or in children in civilian settings presenting in a shutdown state.
The broader picture: Historical understandings of trauma and the responses of health professionals
Seen from the perspective of medical history, the ebb and flow of medical and political opinion are part of a recurring cycle where the psychological impact and wide-ranging manifestations of trauma are “denied, then exaggerated, then understood, and finally forgotten” (p xxii) (Shephard, 2001). At the present time, in relation to asylum-seeking children, we can position ourselves in the cycle between forgetting—“amnesia for the lessons learned” (p 39) (Weisaeth, 2014)—and denial. In this section, we take a brief look at lessons previously learnt because some of the lessons are pertinent to neurobiological models of the shutdown state.
First, as highlighted by Abram Kardiner, “each man has his breaking point” (p 33), which differs from person to person (Kardiner, 1947).
2
Applied to children, Kardiner’s observation is as follows (p 172): An event which creates conditions to which the [child] cannot adapt may be called traumatic, and the point at which the [child]’s adaptive capacities fail may be called the breaking point.
Second, the specific pattern of trauma response—in the face of the same event or type of event—can vary from person to person and from child to child (Lanius et al., 2003). Presumably, these variations reflect, in large part, differences in genetic and epigenetic vulnerabilities carried over from previous generations or from events in the child’s own lifetime (Boyce et al., 2021; Miller, 2021) or the process of priming (Bargh, 2014), where one pattern of response is more likely because it has been activated recurrently in an earlier development phase.
Third, patterns of trauma response can change over time. The types of stressors, combined with cultural and social factors, contribute to the particular manifestations of trauma; in each particular historical/social/political period, each traumatic stressor has a “signature” pattern in which that stressor comes to be expressed (p 39) (Weisaeth, 2014). Because of these different patterns—the changing face of trauma—each new variant may be seen “as a new discovery and given a new label,” though it “may just be a rediscovery” (p 39) (Weisaeth, 2014).
Fourth, along the same lines, the “shutdown” pattern seen asylum-seeking children has been previously described, though given different names, in two different populations: soldiers traumatized in battle and infants separated from their mothers. From the late 18th century to the middle of the 20th century, military doctors working during the French Revolution, Napoleonic Wars, Russian-Japanese War, and World Wars I and II described states of stupor in soldiers who experienced fear or terror responses to the extreme violence or killing of the battlefield (Crocq, 1999)
3
(Crocq & Crocq, 2000). (Clervoy, 2015; Milian, 1915). As one example among many, the French physician Gaston Milian (1871−1945) used the term battle hypnosis (hypnose des batailles) to refer to stuporous posttraumatic states in which soldiers, following military action, were immobile in a lying or sitting position, with eyes open and a fixed stare (Clervoy, 2015; Milian, 1915). And in 1946, in the civilian setting, Renée Spitz described how some institutionalized children (aged 6−11 months), when separated from their mothers, initially experienced a period of separation distress that was followed, four to 6 weeks after the separation, by a shutdown state of anaclitic depression (p 314): A sort of frozen rigidity of expression appeared . . . These children would lie or sit with wide-open, expressionless eyes, frozen immobile face, and a faraway expression as if in a daze, apparently not perceiving what went on in their environment . . . Contact with children who arrived at this stage became increasingly difficult and finally impossible.
Though under a different rubric, this description could just as well apply to asylum-seeking children in a shutdown state.
Moving forward using a biopsychosocial (systems) model
From this point forward, and building on the lessons from history, we specifically adopt a developmental, biopsychosocial (systems) perspective—one in which the shutdown states in asylum-seeking children are understood to emerge via a dynamic relation between children and their context, very broadly conceived (Bowlby, 1988; Engel, 1977; Sameroff, 2014). This systems perspective provides clinicians working in child psychiatry and pediatrics a framework for organizing emerging findings pertaining to the mechanisms by which adverse childhood experiences (ACEs)—for example, maltreatment, family disruption, high parental stress, witnessing violence (including that against a caregiver), caregiver mental illness, criminal behavior in the household, and low socioeconomic status—are biologically embedded to shape adverse physical and mental health outcomes (Agorastos et al., 2019; Appleyard et al., 2005; Boyce et al., 2021; Flaherty et al., 2009; Hyman, 2009; McEwen et al., 2015; Nelson, 2013; Sameroff, 2014). The systems framework allows us to put forward neurobiological models that can help us to understand how the human brain and body respond to extreme fear, terror, or situations from which escape is not possible.
Clinical and neurophysiological findings in children in the shutdown state
Clinical and neurophysiological measures prior to the stupor state, during the stupor state, and during recovery have been documented by pediatricians and child psychiatrists who have been involved in the treatment of individual children. The most informative cohort studies, with larger numbers—n=23 (Bodegård, 2005b); n=29 (Aronsson et al., 2009); and n=46 (von Knorring & Hultcrantz, 2020)—come from Sweden. Symptoms associated with autonomic system activation are a key component of the clinical presentation—and in potential neurobiological models—and we use Stephen Porges’s Polyvagal Theory as a framework for discussing patterns of autonomic system activation
4
. Figure 1 provides the reader with a simplified functional diagram of the autonomic nervous system and its three distinct components: the restorative parasympathetic component, the sympathetic system component, and the defensive parasympathetic component (see Figure 1). A simplified functional visual representation of the autonomic nervous system based on polyvagal theory. Afferent signals from the body to the brain provide the brain with interoceptive information about the state of the body (figure on the left). Efferent signals from the brain to the body—involving both the sympathetic (depicted in red) and restorative parasympathetic (depicted in blue) systems—provide second-by-second fine-tuning of body state (figure on the right). Under conditions of safety and low stress, activation of the restorative parasympathetic system downs body arousal (e.g., by decreasing heart rate), supports a mind-body state that facilitates close emotional connection with significant others, and provides a physiological and subjective state of calm and well-being. The restorative parasympathetic system also supports a broad range of restorative life processes—digestion, energy conservation, and tissue regeneration and repair. Under conditions of stress or in response to signals of danger, the restorative parasympathetic system is withdrawn, and activation of the sympathetic system ups body arousal (e.g., by increasing heart rate, activating sweat glands to cause sweating, activating the secretion of adrenalin [from the adrenal glands], and adjusting vascular tone). The defensive parasympathetic system (depicted in purple) works alongside the sympathetic system in response to threat by activating defensive programs in the gut (causing nausea, vomiting, and diarrhea), bladder (causing urination), and heart (causing threat-related fainting). In asylum-seeking children—who are in a state of high arousal precipitated by fear—one would expect to see withdrawal of the restorative parasympathetic system, activation of the sympathetic system, and activation of the defensive parasympathetic system. © Kasia Kozlowska 2013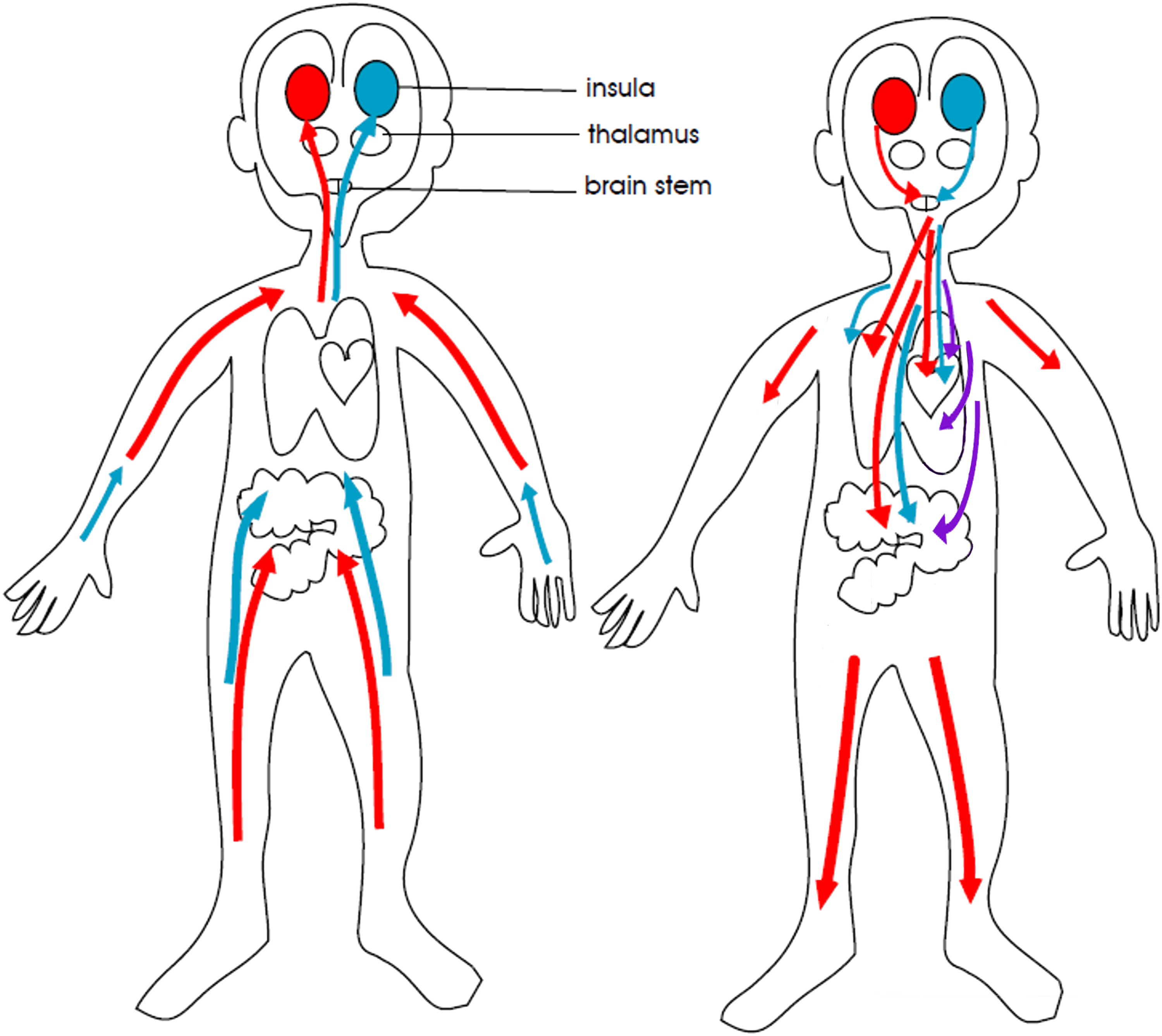
The pattern of adverse childhood events (including trauma) experienced by the children
The pattern of trauma experienced by asylum-seeking children (see introduction) appears to involve cumulative ACEs that have occurred at multiple time points across the family story and during the child’s development: • ACEs (including trauma) in previous generations and when the child was in utero • ACEs (including trauma) experienced in the home country during the child’s lifetime • ACEs (including trauma) experienced in the family system (Timshel et al., 2017) • ACEs (including trauma) experienced as part of the asylum-seeking process
Child and parent antecedent vulnerability factors
Swedish pediatricians have documented that a position of responsibility or role-reversal caregiving within the family system—for example, an elder son, acting as translator, who witnessed traumatic events in the home country—is a vulnerability factor (Bodegård, 2005a; von Knorring & Hultcrantz, 2020). From an attachment lens, children who function as caregivers protect themselves by caring for the parent(s) and take responsibility (blame themselves) for problems in the attachment relationship and for the well-being of their parents and family (Crittenden, 1995 – 2012) 5 . In this context, they are particularly vulnerable to overwhelming anguish when faced with the realization that their efforts to care for their parents and family have failed and that the last-ditch hope of a path of escape has been blocked.
Along the same lines, premorbid personality factors pertaining to the child—described as anxious, sensitive, perfectionist, conscientious high achiever with high self-expectation, and difficulty coping with perceived failure—have also been noted in a review of cases (asylum-seeking and civilian) (Otasowie et al., 2020).
The same authors also reported that in the case series, all the parents of asylum-seeking patients had a history of mental illness (Otasowie et al., 2020).
Symptoms of stress and distress antecedent to the shutdown state
Both Australian and Swedish pediatricians and child psychiatrists have reported a broad range of psychological/somatic symptoms of stress and distress antecedent to the shutdown state, including PTSD (hypervigilant subtype), anxiety symptoms, depression, sleeping difficulties, nightmares, aggressive outbursts, withdrawal, suicidal ideation/attempts, and problems with eating (Bodegård, 2005a; Steele et al., 2004; von Knorring & Hultcrantz, 2020).
The breaking point and the child’s psychological and neurophysiological response
The breaking point—involving the emotional anguish associated with fear, hopelessness, failure, and defeat, coupled with extreme arousal—is followed by an immediate or gradual change of state into shutdown (von Knorring & Hultcrantz, 2020).
Clinician accounts suggest that the child experiences a complete erosion of hope when he or she realizes that the family’s path of escape is blocked. For some children, as in the case of Shayan Badraie, the boy in the Australian detention center (see introduction), the breaking point was reached in the context of ongoing exposure to violent events in the detention center. One can hypothesize that he and his family came to experience a sense of futility and a realization that the family’s stay in detention was interminable. For other children, as in the case of asylum-seeking children in Sweden, the news that asylum has not been granted and that the family was expected to return to the home country—where the child and family had previously been exposed to trauma—appears to constitute the breaking point.
Swedish pediatricians reported that on hearing or reading the negative immigration verdict “some children reacted immediately at that point with vomiting or other physiological symptoms” (p 1107) (von Knorring & Hultcrantz, 2020). Further communication with Dr Anne-Liis von Knorring and Dr Elisabeth Hultcrantz clarified that the above symptoms fell into two clusters (von Knorring and Hultcrantz, personal communication, 2020).
The first cluster reflected symptoms caused by activation of the autonomic nervous system. These include panic attacks, nausea/vomiting, enuresis/encopresis, and fainting. 6
The second cluster reflected symptoms caused by activation of brain regions mediating salience detection, arousal, and emotional states. These include functional neurological symptoms (motor symptoms [e.g., tics, stiffness, and weak legs], vertigo, or tinnitus) and functional pain symptoms (abdominal pain/headache/pain in legs). 7
Importantly, it is now well established that brain regions mediating salience detection and arousal can be activated in a top-down fashion—by mental images (thoughts, memories, and feelings)—to trigger functional somatic symptoms, for example, by hearing bad news or by exposure to a trigger event that brings negative thoughts, memories, and feelings to mind (Gianaros & Wager, 2015; Kanaan et al., 2007). In consequence, appraisal processes—the threat-related meaning that children ascribe to their experiences—as well as anticipatory and predictive processes pertaining to the salience of the threat, are likely to be important elements in the neurobiology of the shutdown state (Edwards et al., 2012; Gianaros & Wager, 2015; Kleckner et al., 2017).
Entry into the shutdown state
There is very little data about pattern of progression into shutdown in children in the Australian setting. As, previously noted, in Sweden, pediatricians have reported that on hearing a negative immigration verdict, the shift into the shutdown state has been immediate or gradual (von Knorring & Hultcrantz, 2020).
Clinical characteristics of the shutdown state
The children present with loss of motor activity, loss of reaction to sensory stimulation (including pain), mutism (no or minimal verbal response), decrease or cessation of drinking and eating, and enuresis and encopresis (Bodegård, 2005a; 2013; von Knorring & Hultcrantz, 2020). Hypotonia is reported in two of the three larger cohort studies (Bodegård, 2005a; von Knorring & Hultcrantz, 2020). The third cohort study did not comment about tone but reported that “22 children could not stand on their legs, whereas seven of the children could walk with the support of one or two persons” (Aronsson et al., 2009). The children are “inaccessible to contact” (Mobile Asylum Team, 2013). Either they lie there with closed eyes (von Knorring & Hultcrantz, 2020) or, if the eyes are open, the children make no eye contact (Aronsson et al., 2009) and may look at the floor and show no or very limited interest in the outside world.
Routine clinical diagnostic workups of these children—blood screen, urine screen, ECG, EEG, and MRI—are typically normal, with the exception of intermittent sinus tachycardia in a subset of children (Aronsson et al., 2009; Otasowie et al., 2020). In children described by Lindberg and Sundelin (2005), the sinus tachycardia was sometimes accompanied by hypertension (Lindberg & Sundelin, 2005). Sinus tachycardia and hypertension are symptoms of autonomic system activation. They involve withdrawal of restorative parasympathetic component (withdrawal of the vagal break) and activation of the sympathetic component (see Figure 1).
Along the same lines, clinical observations of the children by Göran Bodegård—a pediatrician and child psychiatrist—report that children in the stupor state can alternate with intermittent periods characterized by increases of body temperature, fixed tachycardia, profuse sweating and hyperventilation, and panicky refusal or anxiety (panic-like attacks, often with intrusion of flashbacks and nightmares) (Bodegård, 2005b, 2013, 2014). Once again, all these symptoms are mediated by—or are accompanied by—activation of the sympathetic nervous system (and withdrawal of the vagal break) coupled with activation of the motor respiratory system (for hyperventilation).
A handful of small studies suggest changes in steroid metabolism—a key body system involved in energy homeostasis.
Cortisol—a glucocorticoid, the end product of the hypothalamic-pituitary-adrenal (HPA) axis—regulates energy consumption in all cells of the body. A calorimetry study in two children in the stupor state showed low energy expenditure—below the requirement of basal metabolism (Jeppsson, 2013). A small study measuring salivary cortisol in four children in stupor showed a flattened diurnal cortisol profile, compared to two unaffected siblings who showed normal diurnal variation (Bodegård & Rydelius, 2008; Godani et al., 2008).
In addition to its role in producing cortisol as part of the HPA axis, the adrenal gland secretes other steroids—dehydroepiandrosterone (DHEA) and pregnenolone—which pass the blood brain-barrier and contribute to brain levels of steroids (termed neurosteroids). These two steroids modulate a broad range of brain functions and neurotransmitter systems (Rasmusson & Shalev, 2014) and are implicated in the neurobiology of trauma-related presentations that involve various forms of dissociation (Lanius et al., 2014). In a study with 11 children in the shutdown state using high-sensitivity liquid chromatography to measure blood steroid levels, a downward shift in cortisol concentrations (decreased cortisol, as suggested by the previous studies) predicted both the time that the children stayed in the stupor state (symptom score) and the time to recovery (Sondergaard et al., 2012). It also showed that an upward shift in pregnenolone and DHEA was associated with the stupor state (symptom score).
Recovery from the shutdown state
Recovery from the shutdown state takes many months and often involves feeding and rehydration via a nasogastric tube (Aronsson et al., 2009; Ngo & Hodes, 2020). The process of recovery usually begins with some kind of interpersonal communication via touch, eye contact, or head movement, followed by a stepwise return of motor skills (Aronsson et al., 2009). Forslund and Johansson found that all the children in their study (n=5) reported varying degrees of memory loss about their treatment in hospital (Forslund & Johansson, 2013). Other clinicians did not report memory loss (Bodegård, 2005a). Most clinicians highlight that the provision and communication of safety within both the family and sociopolitical (immigration) contexts serve as the cornerstone of treatment (Bodegård, 2005a; Forslund & Johansson, 2013; Isaacs, 2019).
Neurobiological Models
To date, four neurobiological models have been proposed to explain the states of stupor seen in asylum children. After describing those four models, we introduce a fifth. Importantly, an experience of extreme fear or threat is central to all five models.
When reading through the models, the reader will notice that there are significant overlaps between the proposed models. The mechanisms described model 1—the sustained autonomic hyperarousal model are also an element of model 2 and 3. The mechanisms described in model 2—the innate defence model—are an element of model 3 and 5. This design pattern, where “parts of simpler reactions [are] incorporated as components of more elaborate ones, a nesting of the simple within the complex” is known as the nesting principle (p 37) (Damasio, 2003). The nesting principle is a characteristic of living systems. That is, even though each system remains distinct, it is simultaneously a part of a more complex systems that is distinct in its own right (Capra, 1997).
Also important to note is that at the current point in time, each of the models provides a possible pathophysiological explanation—or a component of a possible pathophysiological explanation—and none of them, for the moment, has enough evidence to be accepted or disregarded.
Model 1: Sustained autonomic hyperarousal
The first model posits sustained autonomic hyperarousal involving high energy use characterized by hyperaroused sympathetic and parasympathetic systems in a deadlock, leading to symptoms of numbness, apathy, perplexity, withdrawal, and fatigue or exhaustion (Nunn et al., 2014).
This model is useful if conceptualized in the context of contemporary theories of the autonomic nervous system—polyvagal theory (Porges, 2011). Polyvagal theory posits the parasympathetic system has two functional components that work in an independent and inverse manner, activating in safe, and threatening contexts, respectively (Kozlowska et al., 2020; Porges, 2011) (see Figure 1). Through the polyvagal lens, the sustained autonomic hyperarousal model articulates the idea that in children in the shutdown state, the sympathetic component is in a state of sustained activation, mitigated only by activation of the defensive parasympathetic component. These two defensive systems are activated side by side—in deadlock as it were—so that most of the time, clinical parameters (heart rate, blood pressure) are maintained within normal clinical limits. Concurrently, the restorative parasympathetic component—which activates in contexts of safety—is withdrawn in this situation. Intermittently, when there is a temporary easing in the activity of the defensive parasympathetic to the heart, sympathetic activity is not adequately contained, and the child shows periods of sustained tachycardia, as well as other signs and symptoms typical of sympathetic activation (see the previous section).
The sustained autonomic hyperarousal model accounts for symptoms that are mediated by the autonomic nervous system. Sympathetic activation accounts for periods of tachycardia, hypertension, and profuse sweating. Increased sympathetic activation also accompanies hyperventilation, panic-like attacks, and flashbacks and nightmares. Activation of the defensive parasympathetic accounts for symptoms of vomiting, enuresis, and encopresis and explains why most of the time, the clinical parameters of heart rate and blood pressure are maintained within normal limits; sympathetic activity is attenuated by concomitant activation of the defensive parasympathetic component.
The shortcoming of the sustained autonomic hyperarousal model is that it fails to account for a number of features that characterize the shutdown state: the loss of motor function; changes in sensory and pain processing; the stuporous state itself; and changes in steroid metabolism 8 . Since the autonomic nervous system does not directly control any of these functions, understanding the underlying neurobiological mechanisms requires the involvement of other neural and body systems. Nonetheless, the sustained autonomic hyperarousal model is useful, and it is integrated—either explicitly or implicitly—in most of models that we discuss below.
The treatment implications of this model include interventions that modulate neural activity within the autonomic nervous system. Specifically, neuromodulation could enhance activation of restorative parasympathetic (vagal) activity, thereby facilitating downregulation of defensive parasympathetic (vagal) activity and sympathetic activity. Recently developed non-invasive neuromodulation techniques include the Safe and Sound Protocol (developed by, and based on the work of, Stephen Porges (Porges, 2011))—and Neuro-Stim (developed by Innovative Health Solutions, IN, USA) (Kovacic et al., 2017). Alternatively, sensory interventions that promote interoceptive afferent activity (including vagal afferents) that signal safety and connection with others and that, in turn, modulate top-down regulation of the autonomic system could be considered. Recently developed sensory techniques include slow-stroke psycho-regulatory massage (Arnold et al., 2020; Baumgart et al., 2020). These interventions could potentially support the healing process on the level of the autonomic nervous system by encouraging activation of the restorative parasympathetic system and supporting the shift of the autonomic nervous system from a defensive to a restorative state.
Model 2: The innate-defence model (activation of innate shutdown responses of tonic immobility, collapsed immobility, or quiescent immobility)
The second model proposed in the literature is tonic mobility, an innate shutdown response (von Knorring & Hultcrantz, 2020). Notably, however, tonic immobility is one of three innate shutdown responses—with an overlapping neurobiology—that occur as part of the defence cascade (Kozlowska et al., 2015). Whilst tonic immobility involves high tone—which is not a clinical characteristic of asylum-seeking children in shutdown—the other two shutdown responses, collapsed immobility and quiescent immobility, do involve low tone. Hence, in this section we discuss the three innate shutdown responses of the defence cascade as a group.
In both animals and humans, the innate shutdown responses are activated in three circumstances: (1) in the context of extreme fear, when sympathetic activation has reached an upper threshold, and it is no longer possible either to escape from the threat or to win the fight; (2) when pain is deep or inescapable; or (3) when the individual experiences extreme exhaustion after a period of acute or chronic stress (Kozlowska et al., 2015). Whilst tonic immobility and collapsed immobility are usually short-lived (a time frame of minutes to hours), quiescent immobility—which facilitates healing—occurs over long periods.
On the subcortical, brain stem level, the shutdown responses involve two key components (Keay et al., 2001; Kozlowska et al., 2015): autonomic and motor-sensory. The autonomic component involves a relative withdrawal of sympathetic activity and coactivation of the defensive parasympathetic component (vagus), which together dampen autonomic arousal, shift cardiac parameters downward (to within or below normal levels), and mediate symptoms of nausea, enuresis, and encopresis. The motor-sensory component involves activation of the ventrolateral periaqueductal gray (PAG), which mediates immobility (cessation of all spontaneous motor activity, with reduced muscle tone), lack of response to sensory stimuli, and opioid-mediated analgesia and loss of reactivity to pain (hypo-reactivity to external stimuli [absence of orientation, startle response, or vocalization]).
The innate-defence model accounts for most of symptoms that are seen in the shutdown state in asylum-seeking children: autonomic symptoms, the loss of motor function; changes in sensory and pain-processing; and the stuporous state itself. The shortcoming of the model is that it does not provide us with data as to the neurobiological changes that take place on the cortical level, and it does not account for the changes in steroid metabolism and energy homeostasis (elements not mediated by the autonomic system) that are reported in asylum-seeking children.
The treatment implications of this model include a trial of opioid receptor antagonists—in particular, mu, and kappa types—that could potentially accelerate the child’s recovery from activation of innate shutdown responses (see also model 5). Currently available pharmacotherapeutic agents are naloxone (very short half-life) and naltrexone (longer half-life), both of which are nonspecific opioid receptor antagonists that target both mu and kappa opioid receptors. No published case studies in asylum-seeking children in the shutdown state reported use of these treatment options. Interestingly, Dr Bruce Perry, who is known for his work with maltreated children and adolescents, has used naloxone or naltrexone in more than ten cases of children or adolescents to interrupt states of extended immobility and unresponsiveness; these cases were interpreted as tonic/collapsed immobility responses activated in the context of memories of trauma (Bruce Perry, personal communication, June 2016).
Model 3: Catatonia
The third model posits that the stupor states are a form of fear-induced catatonia. A number of physicians have argued that catatonia—except for the catatonia associated with medical illness or use of neuroleptics—can be conceptualized as one of the fear responses seen in humans. Karl Ludwig Kahlbaum & Pridan (1973), for example, described catatonia as a state involving “profound mental anguish, or an immobility induced by severe mental shock (or being frozen after a great fright)” [our translation] (p 8) (Kahlbaum & Pridan, 1973; Moskowitz, 2004). Perkins (1982) argued that catatonia might be “the ultimate response to fear in a person who is under enormous psychological and physical stress and in whom regression to a primitive form expression has occurred” (p 287) (Perkins, 1982). Moskowitz (2004) used the colloquial term of being “scared stiff” and suggested that catatonia may represent a “‘end state’ response to feelings of imminent doom” (Moskowitz, 2004). And more recently, Dhossche and colleagues have discussed how catatonia can be triggered by extreme fear coupled with high arousal (Dhossche et al., 2012) and that in children it may reflect the child’s response to deprivation, abuse, and trauma (Dhossche, 2012). Catatonia as a potential model for children in the shutdown state has been considered by many clinicians (see Ottasowie for a review) (Otasowie et al., 2020) and is proposed as the best fit by some (Dhossche & Kellner, 2015; Dhossche, 2012; Sallin et al., 2016).
Neuroimaging studies suggest that catatonia involves decreased function in the prefrontal cortex and abnormal “horizontal” cortical-to-cortical modulation (horizontal model of catatonia) or abnormal “vertical” modulation of the cortico-striato-thalamo-cortical circuits (vertical model of catatonia) (Haroche et al., 2020). The latter circuits, which are responsible for modulating motor control, are themselves modulated by converging inputs from the emotion-processing prefrontal and limbic regions (orbitofrontal cortex, cingulate, and amygdala). On the neurotransmitter level, abnormalities of GABA receptor system are supported by both clinical and research data (see Dhossche and colleagues for review) (D. Dhossche et al., 2010). Changes in autonomic function (activation or instability), coupled with changes in temperature regulation and respiratory motor activation, are a cardinal feature in 45% of catatonias (Dhossche, 2012) and are hypothesized to reflect abnormalities in top-down modulation of the hypothalamus (including abnormalities in neurotransmitter function) (Dhossche et al., 2010).
An additional point of interest pertains to a postulated relationship between catatonia and innate defence responses (model 2). In 1977, Gallup and Maser suggested that the brain changes that take place in catatonia may “contain evolutionary-based “fragments of primitive defences against predators that now misfire under conditions of exaggerated stress” (p 357) (Gallup & Maser, 1977). Whilst Gallup and Maser were specifically referring to tonic immobility, shutdown responses characterized by hypotonia would be a better fit (see discussion pertaining to model 2).
Catatonia symptoms that account for the shutdown state in asylum-seeking children.
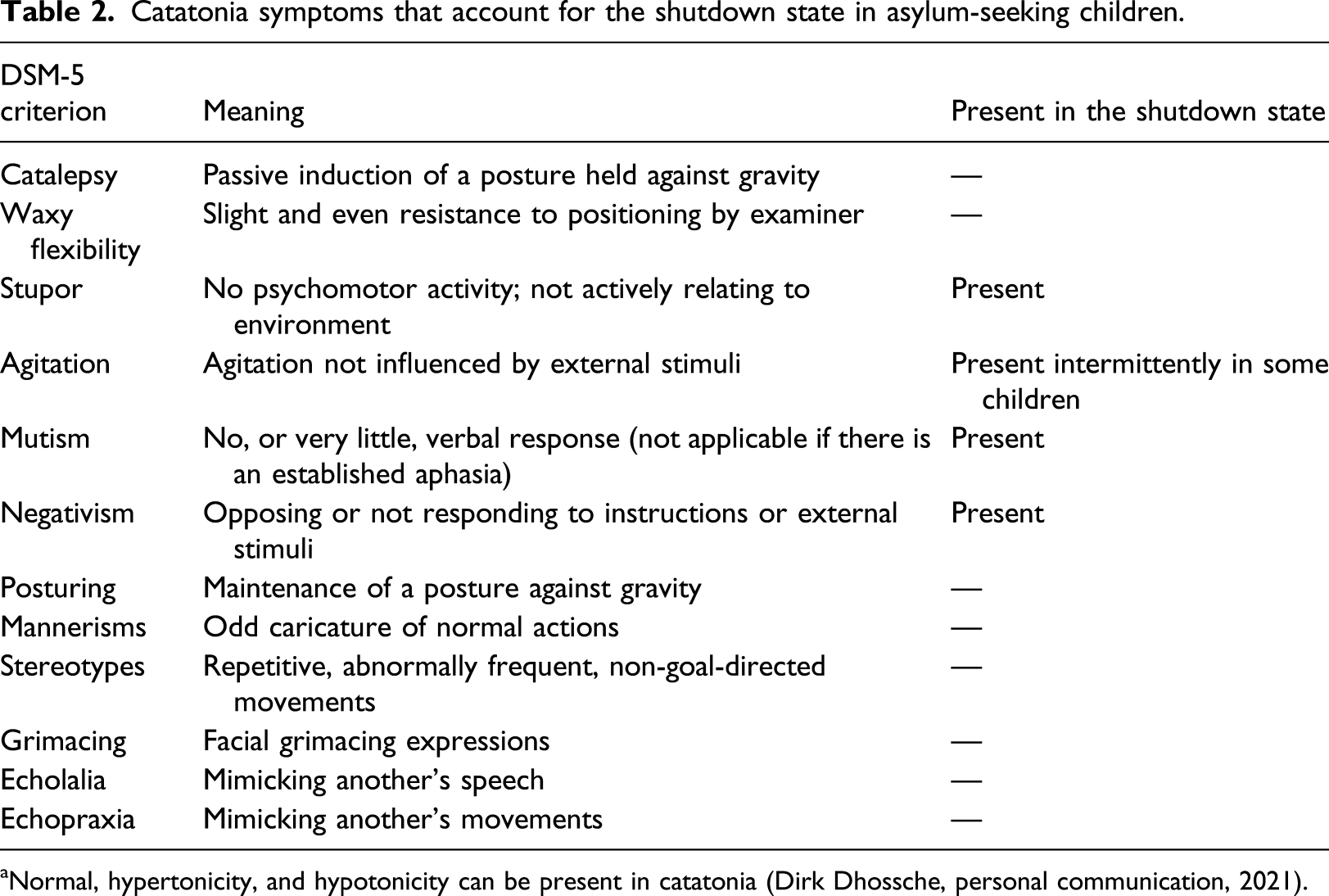
aNormal, hypertonicity, and hypotonicity can be present in catatonia (Dirk Dhossche, personal communication, 2021).
A difficulty with the model is the consistent absence in these asylum children of any other features of catatonia (cataplexy, waxy flexibility (which involves an increase in tone), posturing, mannerisms, stereotypies, grimacing, echolalia, and echopraxia).
Another difficulty is that the autonomic profile of individuals experiencing catatonic stupor involves increases of heart rate, temperature, blood pressure, oxygen consumption, and metabolic rate (Gjessing, 1938, 1974a, 1974b); that is, catatonic stupor is a state characterized by an upward shift in energy use, whereas asylum-seeking children in shutdown show a shift in the opposite direction—a decrease in energy use, along with clinical parameters (heart rate, temperature, blood pressure) that are generally contained within normal limits (see discussion in model 1).
Another difficulty is the findings of hypotonicity (rather than hypertonicity) in asylum-seeking children in shutdown. Interestingly, Dhossche reports that an increase in tone is seen only in 40%–70% of catatonia cases and that the rate of hypotonicity in catatonia is understudied (Dirk Dhossche, personal communication, 2021). Whilst it is understandable that clinicians have focused their attention on hypertonicity because of clinical concerns for creatine phosphokinase elevations and kidney damage, it is possible that this clinical bias has led to underreporting of presentations that involve hypotonicity.
From the clinical perspective, it is readily testable whether the shutdown state in asylum-seeking children is a variant of catatonia. Catatonia responds to benzodiazepines or to seizures induced by electroconvulsive therapy (Dhossche & Kellner, 2015; Dhossche et al., 2020). Most published case studies in asylum-seeking children in the shutdown state did not, however, use those treatment modes or, in the case of benzodiazepine, used doses that were too small (Bodegård, 2005a; Otasowie et al., 2021). Of interest in this context is Bodegård’s clinical observation that two children emerged out of shutdown after premedicating with midazolam prior to inserting a nasogastric tube (Bodegård, 2005a). The catatonia hypothesis remains to be formally tested.
Model 4: Hypometabolic state model (hibernation, dauer, and other hypometabolic states)
Louise Newman, an Australian child and adolescent psychiatrist, suggested that the asylum-seeking children in shutdown could be in a state of hibernation (Sainty, 2018.). In animals, hibernation is an energy-conserving hypometabolic state used to manage environmental stress—winter periods characterized by cold and lack of food (Lant & Storey, 2010; Mathers & Staples, 2019). Other responses involving a hypometabolic state in animals include dauer, diapause, estivation, brumation, and torpor.
An emerging body of work suggests that the study of hypometabolic states may be important area of research in humans and applied science more generally (Lee, 2008; Lee et al., 2016; Staples, 2014). In a recent article, Bartsiokas and Arsuaga (2020) review archaeological evidence showing that certain extinct human species living in glacial environments went into hibernation and that the genetic basis and physiology for a hibernation-related hypometabolic state could be preserved in some contemporary humans (Bartsiokas & Arsuaga, 2020). They also discuss historical reports, discussed by Dirks and colleagues, from famine areas in the Pskov region of Russia (east of contemporary Latvia) pertaining to “an almost uninterrupted sleep” (called loijka) during winter; possibly the human equivalent of hibernation, loijka involved entire families of peasants “huddling together on top of huge stoves” to conserve energy and warmth (p 28) (Bartsiokas & Arsuaga, 2020; Dirks et al., 1980).
Based on emerging data from metabolomic research, Robert Naviaux has suggested that the shutdown state that manifests as severe chronic fatigue syndrome may be a manifestation of a hypometabolic state—similar to dauer—in response to adverse environmental conditions (Naviaux et al., 2016). Naviaux proposes that during this hypometabolic state, cells of the body enter a cell danger response, a state in which mitochondria—the organelles in the cell that regulate and produce energy on a cellular level—shift into a defensive mode in which they decrease mitochondrial metabolism to enable the organisms to survive a hostile environment.
Whilst data are lacking, theoretically, it is possible that the changes on the cellular level described by Naviaux—or other processes involving energy metabolism (Mathers & Staples, 2019; Picard et al., 2018)—may also be part of the neurobiology of the shutdown state seen in asylum-seeking children. More broadly—and in line with the nesting principle—such changes could also underpin the changes in energy homeostasis seen during the quiescent immobility response (see model 2) and in prolonged states of dissociation (see model 5).
Model 5: The defence cascade model of dissociation
The fifth model for the shutdown state seen in asylum children—which we introduce the reader to here—is the defence cascade model of dissociation (Lanius et al., 2018). Dissociation is “characterized by a disruption of and/or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, and behavior” (American Psychiatric Association, 2013). Dissociation has been conceptualized as an evolutionary adaptation that, in the face of specific types of threat, involves immobility, increased pain tolerance, and changes in consciousness and in autonomic function. The relevant types of threat include the following: proximity of a perpetrator; presence of body fluids presenting a danger of contamination; situations in which body integrity has been breached; and other situations dominated by helplessness (Kozlowska et al., 2015; Schauer & Elbert, 2010). The defence cascade model of dissociation builds on and incorporates the defence cascade model (see model 2) (Kozlowska et al., 2015) and Mobbs’ threat-detection model (Mobbs et al., 2009, 2010). It is also informed by research with patients suffering from PTSD: whereas patients with the hypervigilant PTSD subtype respond to trauma scripts with hyperarousal coupled with an action tendency to fight or run away (activation of the innate flight-or-fight response), patients with the dissociative PTSD subtype respond with derealization, depersonalization, and hypo-arousal, and sometimes also with motor immobility (activation of the innate shutdown response [model 2]).
According to the defence cascade model of dissociation, the neurobiology of the shutdown state seen in asylum-seeking child is as follows. On the subcortical, brain stem level, dissociative responses presenting as shutdown involve the components previously described for the innate shutdown responses (see model 2, along with model 1 for a more in-depth discussion of the pattern of autonomic system activation). On the cortical level, increased activation in the prefrontal cortex deactivates the amygdala and enables activation of innate shutdown responses in the brain stem (see changes on the subcortical level [model 2]) (Lanius et al., 2018). On the level of the thalamus, reduced integration of sensory stimuli contributes to the lack of response to sensory stimuli (known as cortical-sensory deafferentation) (Lanius et al., 2018). Activation of mu and kappa opioid systems across the neural network contributes to disruptions in consciousness (stupor) and reduced somatosensory integration (thalamus, claustrum, and orbitofrontal cortex), as well as to analgesia, immobility, suppressed vocal responses, and downregulation of the sympathetic nervous system via the ventrolateral PAG (Lanius et al., 2018).
The above-described neural pattern of findings is inverse to that seen in active responses to trauma—flight or fight, and the hypervigilant PTSD subtype—which involve decreased prefrontal activation, increased amygdala activation, and, when the flight-or-fight component of the defence cascade is switched on, activation of the lateral PAG. But many traumatized individuals cycle between active and shutdown responses to trauma, between different components of the defence cascade, and between hypervigilant PTSD (an active response that may include episodes of flight and fight) and dissociative PTSD (a shutdown response that may include motor immobility) (Hashemi et al., 2019; Kozlowska et al., 2015; Lanius et al., 2018; Roelofs, 2017). Clinical descriptions suggest that asylum children also show this cycling pattern across time (von Knorring & Hultcrantz, 2020) (G. Bodegård, 2014) (Aronsson et al., 2009). Prior to the onset of stupor, when the threat is perceived to be imminent, many of the children (especially the boys) experienced hypervigilant PTSD—or elements of PTSD—an active response to trauma. On hearing the immigration verdict, when the child perceives the threat to be inescapable, there is a transition—immediate or gradual—from the active response to trauma, to the shutdown state. “Shifting between passive and active defensive modes is implemented by the ventromedial prefrontal cortex” and, in particular, by the anterior cingulate cortex, which in turn projects to the central nucleus of the amygdala and to the ventrolateral PAG (p 3) (Roelofs, 2017).
An additional point of discussion is the overlap between the construct of dissociation and shutdown states that are diagnosed as dissociative seizures. 9 In the International Classification of Diseases (ICD-11), dissociative seizures sit under the umbrella term dissociative neurological symptom disorder (previously dissociative [conversion] disorders, previously hysteria) (World Health Organization, 2018). In the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), they sit under the umbrella term functional neurological symptom disorder (previously conversion disorder, previously hysteria) (American Psychiatric, Association, 2013). Relevant to the discussion here is one subtype of dissociative seizure—the unresponsive presentation where the child presents as unresponsive to social interaction, sensory stimuli, and pain for a period of minutes, hours, or occasionally days. 10 Interestingly, as previously mentioned, von Knorring and Hultcrantz report that prior to the shutdown state, many of the children experience other dissociative/functional neurological symptoms (von Knorring and Hultcrantz, 2020).
The defence cascade model of dissociation accounts for most of the symptoms that are seen in the shutdown state in asylum-seeking children: autonomic symptoms, the loss of motor function; changes in sensory and pain processing; and the stuporous state itself. The finding that prior to the shutdown state, many of the children experience PTSD (hypervigilant subtype), as well as other dissociative/functional neurological symptoms, is easy to conceptualize alongside this model.
One shortcoming of the model is that it does not account for the length of time that the children stay in the shutdown state. If the shutdown state does reflect a dissociative process, then the clinical presentation of the children in shutdown reflects dissociation in its most extreme form. Another shortcoming is that the model does not account for the changes in steroid metabolism and energy homeostasis (elements not mediated by the autonomic system) that have been reported in asylum-seeking children. In this context, if dissociation is the neural process that underpins the shutdown state seen in asylum children, then further research will need to elucidate whether concomitant changes on the cellular level (see model 4) facilitate a hypometabolic state over the weeks or months of the illness.
Because the defence cascade model of dissociation builds upon and incorporates models 1 and 2—consistent with the nesting principle—the treatment implications of this model include those outlined for model 1 and 2. However, because the model hypothesizes the activation of mu and kappa opioid systems across the neural network—both in subcortical structures implicated in activation of the innate defence responses (the PAG) and more broadly (thalamus and claustrum in the subcortex and orbitofrontal region in the cortex), changes in function in these regions would presumably be measurable on a group level analysis using imaging technologies and a pre- and post-treatment research design.
Limitations
Our presentation of five plausible models for explaining the shutdown state in asylum-seeking children is not able to address all relevant factors. One important consideration that needs to be factored into future formulations is the child’s stage of development when the trauma occurs, the duration of trauma, and the different body systems affected by trauma in light of the child’s developmental stage. Another important consideration is that all the models discussed in this article assume that the child is endowed with an intact neurophysiology that is functioning at the extremes. Because a subgroup of children presenting in shutdown may have been exposed to substantial deprivation and institutionalization—and experienced the associated neuroendocrine effects 11 —it may be important to consider the interplay between neuroendocrine deficits and the activation of evolutionary responses to extreme threat.
Conclusion
Asylum-seeking children presenting in the shutdown state have been the subject of much discussion and controversy—on both government and medical system levels—in Australia and in Sweden. In this article, we have taken the perspective of Australian pediatricians and child psychiatrists—as well as many colleagues from Sweden and elsewhere—that the shutdown state seen in asylum-seeking children reflects a neurobiological response to trauma. We have also availed ourselves of systems thinking and introduced the reader to the nesting principle, a design pattern that underpins biological systems, where simpler systems are incorporated into more elaborate ones (Damasio, 2003). Working from these perspectives we have presented a range of plausible neurobiological models that clinicians can use to inform their clinical practice.
Of particular interest are two distinct and mutually exclusive models: the catatonia model and the defence cascade model of dissociation. Both states involve significant disruption in neural network function accompanied by immobility, increased pain tolerance, and changes in consciousness and in autonomic function. The key difference between the states—and the patient’s response to treatment—may reflect the pattern of prefrontal cortical function and the predominant patterns of neurotransmitter response. In the catatonia model, prefrontal cortical function is decreased; the pattern of neurotransmitter response is dominated by perturbed central GABA metabolism; and patients are most likely to respond to benzodiazepines (targeting GABA receptors) and electroconvulsive therapy. In the dissociation model, prefrontal cortical function is increased; the pattern of neurotransmitter response is dominated by perturbed central opioid metabolism; and patients are most likely to respond to opioid receptor antagonists (targeting opioid receptors). Testing of these models—in terms of treatment response—is yet to be undertaken in the clinical setting but will, in the future, provide valuable information.
An interesting consideration—and a potential point of overlap between the catatonia and dissociation models—is that they may both reflect an evolutionary adaptation to extreme threat.
12
Fear-induced catatonia and fear-induced dissociation are both characterized by immobility, increased pain tolerance, and changes in consciousness and in autonomic function. The two conditions may sit on a spectrum. Patients in whom the neural network disturbance is primarily underpinned by changes in central GABA metabolism will likely respond to treatment with benzodiazepines (left-hand side of diagram), and patients in whom the neural network disturbance is primarily underpinned by changes in central opioid metabolism will likely respond to treatment with opioid antagonists (right-hand side of diagram) (see Figure 2).
13
. The hypothetical relationship between fear-induced catatonia and fear-induced dissociation.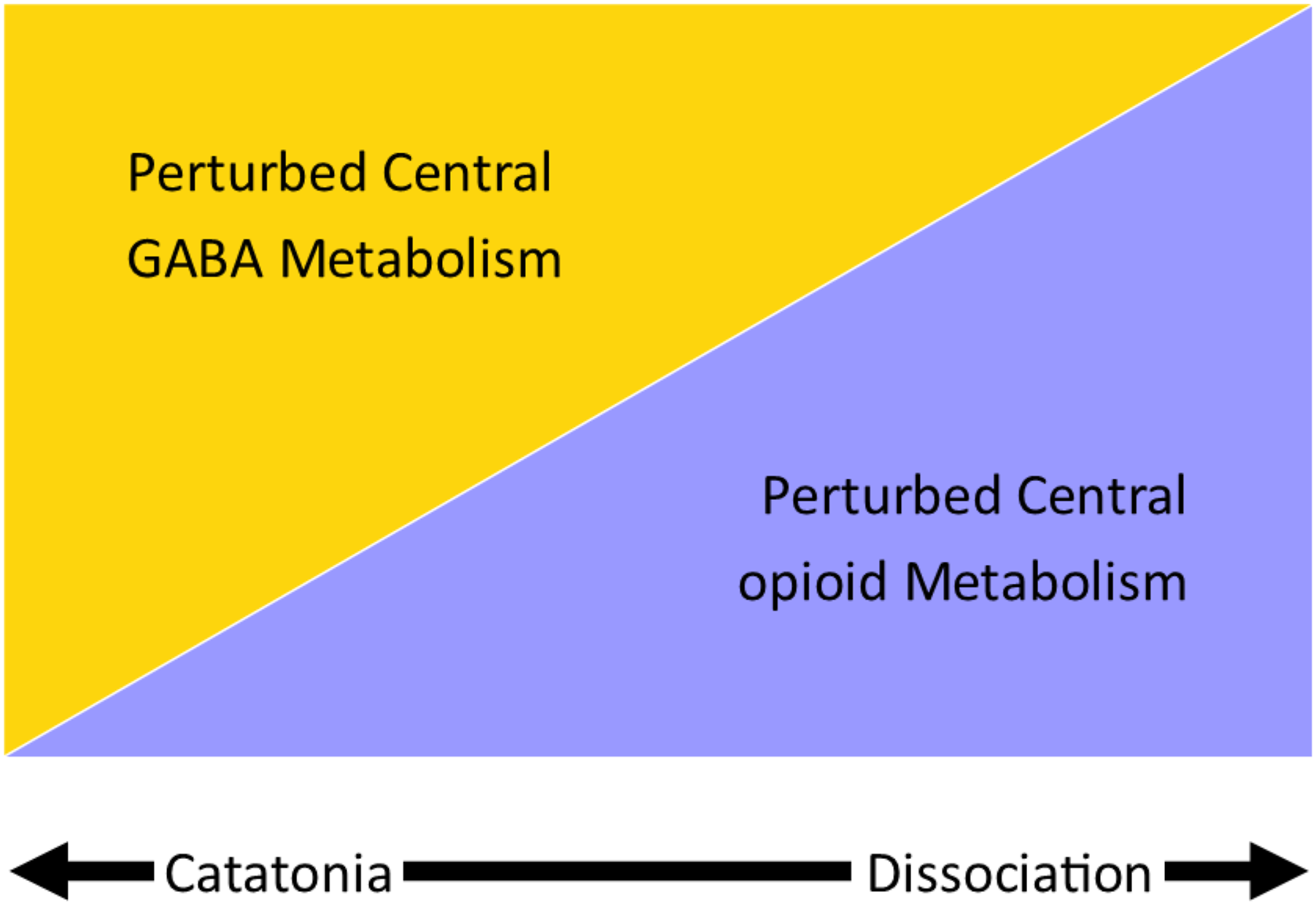
A third model of particular interest is the hypometabolic state model. Whilst data pertaining to hypometabolic states in humans is sparse, the advent of new methodologies—such as the measurement of metabolites via metabolomics (using mass spectroscopy) (Clish, 2015)—is likely to yield new information in the near future and may help us better understand the pattern of changes in energy metabolism that accompany the shutdown state in asylum-seeking children. In the meantime, it is our hope that the neurobiological models presented in this paper will lead to new conversations, open up broader ways of thinking about the sequelae of trauma, and provide clinicians with additional treatment options—alongside provision of nutrition, safety, and stability—when managing traumatized children in shutdown.
Footnotes
The authors would like to acknowledge Professor Dirk Dhossche for our conversations about the catatonia model, Professors Mark Edwards and Mark Hallett for our conversations about the use of the term psychogenic as a modifier of symptoms vs. syndromes, and Judy Longworth for assistance with psychopharmacology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.