
Abstract
Background
Effective teamwork and communication are crucial in surgical settings to ensure patient safety and deliver high-quality care. Operating Room Nurses (ORNs) play a critical role in managing complex technological environments and coordinating with multi-professional teams. Despite the recognised importance of teamwork, limited research exists on how ORNs perceive and experience teamwork and learning in paediatric operating rooms.
Aim
This study aimed to explore the perceptions of operating room nurses regarding teamwork and learning processes within paediatric perioperative care settings.
Method
A phenomenographic design was employed, involving semi-structured interviews with ten ORNs who had completed an advanced course in perioperative paediatric care. Participants were selected through purposive sampling from six hospitals across Sweden. Data were analysed using a seven-step phenomenographic approach to identify variations in understanding.
Results
Two distinct approaches to teamwork and learning emerged: a team-oriented approach, emphasising shared experiential learning and communication within the team, and a personoriented approach, focusing on individualised patient care and preparation through diverse informational resources. Subcategories included ‘Communication ‘and ‘Reading about the patient, ‘highlighting the importance of interprofessional collaboration and holistic patient understanding.
Conclusion
The findings highlight the dual perspectives of teamwork and learning among ORNs, with implications for improving patient outcomes and safety. Integrating both team-oriented and person-oriented approaches in training programs may promote adaptive teamwork and interprofessional learning. Further research is needed to explore team maturity and its impact on clinical practice.
Introduction
Teamwork, leadership, collaboration, and situational awareness are essential for delivering quality care and ensuring patient safety, as complications can often be attributed to communication failures. 1 Effective teamwork is a prerequisite in surgery 2 ; adverse events may occur when team members misinterpret or fail to communicate effectively, which can create stress and compromise patient safety. Health professionals require skills, and knowledge 3 and must adapt to changing situations and pressures. 4 Social interactions in clinical settings assist and establish reference frameworks, enhancing learning. 5 Research suggests that teamwork requires a broad definition, considering assumptions about its nature, study methods, and limitations. 6 Advanced medical technologies ensure patient safety,7,8 yet their complexity raises potential for human error. Thus, surgical safety demands adaptive teamwork strategies for coordinated performance.1,9 Operating room nurses (ORNs) must use various technological devices and understand how to perceive teamwork and learning in the paediatric operating room (OR), as collaboration among all team members is crucial to providing optimal patient care. 10 Yet, ORNs often work without formal supervision, relying on self-directed learning to advance their professional careers. This makes it crucial to explore how ORNs perceive learning processes and perceptions of teamwork and learning processes in the paediatric (OR).
Review of literature
Multi-professional team in the operating room –HTO perspective
In the paediatric OR, teams operate within an environment where human, technology, and organisational (HTO) elements are interwoven, performing complex surgeries with advanced technology. 5 The HTO framework integrates knowledge from fields as nursing, medicine, engineering, and behavioural sciences to design systems that consider human, technological, and organisational interactions, supporting human needs, abilities, and limitations. 5 Safety is thus enhanced by addressing these interactions at an organisational level, which affects roles such as the OR nurse's ability to perform effectively. According to Berglund et al., 5 healthcare professionals function as both individuals and organisational members. Research identifies two organisational levels to prevent system failures: the micro-level perioperative team and the macro-level organisation. 6 At the macro level, system failures may stem from inadequate planning, high attrition, limited organisational learning, workflow issues, equipment shortages, financial constraints, or preventable surgery cancellations. At the micro level, the perioperative team should enhance situational awareness, conduct briefings and debriefings, engage in simulation training, use checklists, improve non-technical skills, and provide regular feedback.6,7
Team and organisation
A team is a specialised group requiring shared goals and mutual dependence among members to function effectively. 8 Bolman et al. (2009) emphasise that a common purpose and interdependence are core elements. In the OR, the core team comprises a multi-professional group. 9 including ORNs, nurse anaesthetists, assistants, surgeons, and anaesthetists, each fulfilling distinct roles. The team's primary aim is to ensure safe, high-quality patient care, improving clinical outcomes.10–14 Challenges such as poor communication, lack of teamwork, and insufficient leadership can compromise patient safety.15,16 Despite recognition of teams ‘importance, understanding factors enabling practical team function in the paediatric OR is still limited.17,18 Teams are widely regarded as optimal for guiding diverse groups toward improved outcomes. However, managing experts with different skills and perspectives can be challenging. 8 Operational teams, comprising 2–10 members who collaborate on shared tasks in proximity, require both individual expertise and practical teamwork skills. 19 Teams often fall short of expectations due to factors such as poor communication, unclear roles, or inadequate teamwork preparation. 20
Team structure and capacity
One approach to OR structuring is the use of fixed teams, where the same team of surgeons, nurses, anaesthesiologists, and residents remains together throughout the day. 21 Stepaniak et al. 21 highlight positive effects of fixed teams on patient outcomes, teamwork, safety climate, and procedure duration. A key benefit is that each member is familiar with the planned surgical steps, allowing the team to focus more on the procedure itself and less on non-essential tasks. 21 Consequently, staff are clear on their roles. 21 Fixed teams enhance adaptive capacity, the ability to synchronise tasks in routine or novel situations, enabling teams to respond effectively to situational demands.22,23 Members often perceive team leaders ‘actions as indicators of expected team behaviour influencing future interactions. 24 Therefore, leaders should creatine conditions that promote reflexivity, enhance psychological safety, and improve team performance. 24
Work, learning, and technology in team-based perioperative care
The clinical environment has a profound influence on clinicians ‘learning, particularly when knowledge is constructed through meaningful interactions. 13 This environment supports the development of skills, enabling the reshaping of reference frames to enhance communication with patients, peers, supervisors, and other healthcare professionals. Effective learning relies on both internal conditions within the learner and external, supportive environmental factors, promoting lasting changes in understanding, behavior, and reasoning. 25
Although the importance of teams in healthcare organisations is well recognised, further research is needed to deepen our understanding of teamwork dynamics in clinical settings. 9 The OR exemplifies a HTO context, where multidisciplinary teams integrate diverse knowledge from nursing, medicine, and technology, emphasising communication and patient safety. 5 The way communication across these three subsystems is learnt within the clinical environment remains underexplored, despite its critical role in safety, system well-being, and performance. 5 Understanding how these interactions support perioperative care is vital. Individuals in healthcare are continually shaped by their experiences and learning contexts. 30 Nurses, as professionals, are responsible for establishing care standards for their patients, though these standards are often subtle and not immediately visible to outside observers. 31 To grasp how nurses interpret their practices, concerns, and experiences, direct inquiry into their perspectives is essential. Wenger emphasises that learning is inherently social, involving an intricate interplay between social competence and personal experience. 32
Additionally, research demonstrates that relationships with supervisors play a significant role in fostering effective clinical learning environments.33–36 Therefore, the purpose of the present study was to uncover the perceptions of operating room nurses regarding teamwork and learning processes in the paediatric OR by research questions as:
How do operating room nurses perceive and experience the phenomenon of learning processes within the paediatric OR environment? How do operating room nurses perceive and experience teamwork within the paediatric OR environment?
Method
Design
To achieve the study's aim, a phenomenographic design was employed. Data were obtained through semi-structured interviews with ten ORNs working in perioperative paediatric operating units in Sweden. Using semi-structured interviews is a standard data collection method within phenomenography. 26 Phenomenography investigates the qualitatively different ways individuals experience and understand phenomena. 26 It emphasizes participants’ perceptions and reasoning in specific contexts, using interviews to elicit reflections on actions and decision-making. 27 The approach seeks to reveal variations in conceptualizations, 28 rather than establish a singular truth. 29
According to Marton and Booth, 26 an individual's understanding of a text, problem, or learning situation is inherently shaped by its context; in learning settings, these elements are interdependent and inseparable from the circumstances in which they are experienced.
Phenomenography emphasises the structural aspects of understanding, assuming a part-whole relationship in human experience, where the same concept may be perceived in varied ways depending on the individual's perspective.29,30 Individuals in healthcare are continually shaped by their experiences and learning contexts. 26 Regarding phenomenographic studies, they enhance understanding about how learners familiarise themselves with the same phenomenon in qualitatively diverse ways and illuminate what learners need to discern to experience a phenomenon in more powerful ways. 31
Sample
A purposive sampling was employed. Participants were ORNs who had completed an advanced course in perioperative paediatric care. All participants provided informed consent for participation in the interview study.
Information about the study was presented orally immediately following the course, and details were also provided about the researcher and the fact that the study is part of a doctoral thesis. One group completed the course in Spring 2018, and another in Spring 2019, resulting in a total of 19 eligible ORNs. A follow-up email was sent to all qualified participants, reiterating the study information provided orally and including a request to sign and return the consent form for participation. Monthly reminders to participate in the study were sent to possible participants for up to six months after course completion. Out of 19 ORNs, ten 10 accepted the invitation to participate and were contacted by the researcher. This group of ten participants represented six different hospitals across Sweden, providing a range of diverse settings, organisational cultures, and work structures. There were no dropouts from the study. As participation was voluntary and required an active response, we have no information about the nine ORNs who chose not to participate.
Sample characteristics
The informants were all nurses specialised in ORN care; their ages ranged from 26 to 58 years. They had work experience as ORN between 2 and 30 years, and from the field of paediatric operations, 1 to 15 years. Eight of the ten informants worked in paediatric surgical departments, and two informants worked in operating departments that also provided paediatric surgery. All informants had experience with general and advanced operations. The informants had completed an advanced course within perioperative paediatric operating room care. Ten females and no men participated. All ten participants were qualified and had given their consent to participate.
Inclusion and exclusion criteria
ORN with specialities in operating nursing care were included. The exclusion criterion was individuals with ORN who did not seek to participate.
Data collection
Interview
The interviews were conducted by the first author (a PhD student with training in interviewing and qualitative research), either in person or via Teams, a digital communication platform, by each participant's preference. Interviews were audio-recorded and transcribed verbatim. The interviewer had no prior relationship with the informants. Participants were given the flexibility to choose the time and location for their interview, a purposeful decision designed to maximise participation. The interview guide began with introductory questions on topics such as participants ‘knowledge and learning opportunities in the OR, aimed at helping them feel at ease and encouraging them to reflect on the everyday context where the phenomena under study regularly occurred. The interviews, which lasted 30 to 70 min, were designed to capture a wide range of perspectives and variations in experiences of the phenomenon. The interview questions were designed to encourage participants to share their own understanding of the phenomenon sought after. All interviews started with the questions: “Can you tell me about a situation in your daily work where you felt that you learnt something new?”, “How do you acquire this knowledge you describe?”. The interviews continued until there was a recognition of how participants conveyed their understanding of the phenomena sought after, best described as an ‘aha’ experience. A thematic semi-structured interview guide, building on Benner (1984) and Benner et al. (1999), was developed and pilot-tested with three ORNs. No changes were, however, made to the interview guide. In all cases, the interviewer obtained informed written consent before beginning. Participants were informed of their right to withdraw from the interview at any time without further explanation.
Institutional review board approval
Permission to conduct the study was obtained from the Head of the Clinic, and an ethical permit was obtained from the regional ethical vetting board at the Karolinska University Ethical Committee, EPN 20171129/Dnr: 2017-1722-3/1. The study was conducted in accordance with the research ethical guidelines outlined in the Declaration of Helsinki. 32
Data analysis
The data analysis followed a phenomenographic approach, which consists of seven steps as described by Sjöström et al.,33,34 to explore phenomena within the everyday clinical environment of ORNs. Throughout the entire analysis process, the research group engaged in a discussion about how to understand the collected data, what the participants described, what they meant, and how participants perceived the phenomena being sought. Step one was familiarisation, where the researchers (IA, JM) became thoroughly acquainted with the interview text. It meant reading and rereading the transcribed interviews. The second step, condensation, involved all authors selecting and reducing the most significant statements from each interview. In the third step, comparison, statements were compared and discussed to identify variations or agreements in the understanding of the phenomena.
The fourth step, conducted by the authors (IA, JM), involved grouping descriptions with similar content into six preliminary classifications. The fifth step, articulating, conducted by the authors (IA, JM), involved describing and categorising the essence of each group. In the sixth step, labelling, all researchers discussed the analysis, and each category was named to reflect its core understanding. At this stage, the preliminary groups were re-analysed and merged into two categories and two subcategories. The final step, contrasting, involved comparing the categories to evaluate the levels of understanding expressed by the informants at a meta-level. In phenomenography, this phase is referred to as the “outcome space.” The varying perceptions of the informants were analysed to assess how well they aligned with those in other categories. Throughout the analysis, paragraphs were condensed into shorter, more powerful quotations, 33 and the processes of grouping and articulating were repeated multiple times to refine them.
Results
The results from the interviews were analysed, focusing on Team and Learning processes. The contrasting on a meta-level unfolded two diverse ways of understanding the meaning of team and learning in the operating room. A team-oriented understanding, where the team is the driver for what learning and communication will be directed towards. The learning is focused more on general knowledge about operational techniques and patient recovery processes. The personoriented perspective, places the individual patient's needs at the core of the team's focus. Here, the team's learning and communication are guided by the unique needs of each patient and are tailored to the patient in the specific situation. Learning is shaped by the situation and the operation performed, with a focus on the individual's needs. Here, the team's learning and communication are guided by the unique requirements of each patient, adapting to specific surgical contexts. Learning is framed by the situation and centres on addressing the individual patient's needs throughout the procedure, resulting in a more personalised approach to patient care (Table 1).
Overview of the results.
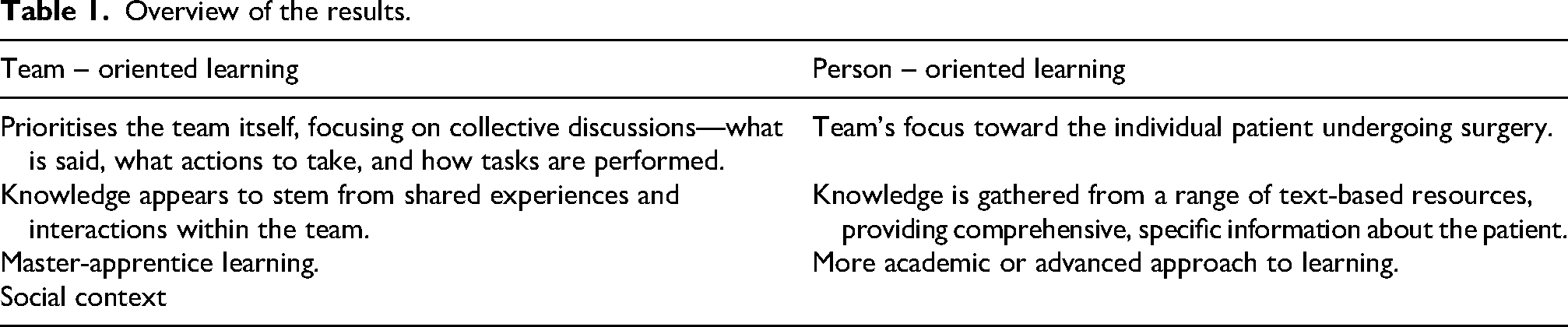
The results reveal two categories: Team-Oriented and Person-Oriented, with one subcategory each, illuminating the ORN perceptions. The category team-oriented demonstrates how the team's teamwork skills influence the value of perioperative care, particularly in task performance. The subcategory communication highlights that there are diverse ways to communicate in the team to work as a team. The category person-oriented demonstrates how learning is related to maintaining focus on individual patient needs during surgery, being prepared for the necessary task distribution. The subcategory Reading about the patient highlights how the ORN draws on various sources to gain a comprehensive understanding of the patient. In the team, people direct their conscious attention towards whom or what they care for, and how assistance is given or received.
Team oriented
In this category, the informants are oriented towards the team. In situations where the team is active, the activities establish a model for how to act and what to do. The informants proposed that the problem is the driver of what to orient one's consciousness towards. The situation that unfolds with the team provides the informants with a frame of learning, a way of being within the team. The excerpt below demonstrates this: “An authentic clinical scenario is happening. I like situations like that. That's when I work best.” “I observe a lot. If I give him the needle holder with the needle in this position, and then I observe that he corrects it by 2 millimetres, then I correct those 2 millimetres myself for the next time. He should not have to do that; it is my job. So, you observe, that worked, he wanted it like that, a little angled to the right there, yes, like that.” (I, 2.). “I inquire the doctor what happens to the patient afterwards… how they perceive. And it is the big things that are very special. This every day, they just proceed routinely.” (I, 1.).
The excerpt above highlights how inter-professional learning becomes natural and an integrated part of a team that provides space for learning. The team members are open and inviting towards questions and reflections.
Communication
This subcategory emphasises the importance of communication from diverse perspectives in establishing a common foundation of information for effective teamwork: “.. We do these check-ins every morning to ensure you communicate with the whole team.” (I, 5).
By giving themselves a brief review or time out, the communication becomes a joint decision. It is directed towards what the team is working on together, refocusing on the essential aspects of the operation at hand.
Person oriented
In this category, the team is oriented towards the patient. The excerpt below demonstrates this: “Complex situations when there is a multi-trauma, a bomb situation, I find more and more that my job extends beyond what I read. If we are in surgery now, I read inside the operating room. I do a quick overview, then I contact anaesthesia; I also contact the surgeon. “(I, 5.).
In more challenging situations, the informant directs the concerns towards the patient's needs.
They strive to be prepared and act in the best interest of the patient.
Reading about the patient
In this subcategory, reading is highlighted as a source of knowledge. In preparation for surgery, the ORN reads from diverse written sources available to them. Collecting the details about the person coming into the surgery. This collection of various written resources builds on the person's own history of needs, lab results, and PMs that are expected in the situation, as well as other evidence-based resources. The excerpts below highlight this: “.. I consider if there is something special with the patient, we always read on before we take in the patient so you have a preliminary understanding.” (I, 6).
In this subcategory, reading emerges as a key source of knowledge. In preparation for surgery, the ORN consults a variety of written resources available to them.
Discussion
The findings in this phenomenographic study revealed two distinct approaches to teamwork and learning: a team-oriented approach, where knowledge is shared experientially within the team, and a person-oriented approach, which focuses on addressing individual patient needs through various informational resources. Effective teamwork is crucial for achieving safe surgical outcomes, as communication failures can result in delays, unplanned reoperations, complications, and even increased mortality.1,2,8,9
Extensive evidence2,10 suggests that effective teamwork is crucial for achieving safe surgical outcomes. Additionally, communication failures are associated with delays, unplanned reoperations, serious complications, and increased mortality.1,4 This prompts a discussion on whether specific teams are inherently more effective in collaboration and if their learning processes differ. Teams often consist of experts with varied experiences and skills, which can lead to diverse perspectives on any given issue, thus adding complexity to achieving cohesive teamwork.6,8 The team-oriented learning prioritises the team itself, focusing on collective discussions, what is said, what actions to take, and how tasks are performed. The patient as a person is invisible. Knowledge in this approach appears to stem from shared experiences and interactions within the team. This aligns with the concept of master-apprentice learning, where knowledge is acquired experientially, as the ‘apprentice’ observes and learns from the ‘master’ within a social context. 35 The person-oriented learning, on the other hand, directs the team's focus toward the individual patient undergoing surgery. Hence putting the patient in the foreground, as knowledge is gathered from a range of text-based resources, providing comprehensive, specific information about the patient. This could be considered a more academic or advanced approach to learning. Lave and Wenger's concept of situated learning acknowledge this as shifting focus from individual learning processes to the social context in which individuals interact and learn collaboratively (Lave & Wenger, 1991, p. 36).
A situated approach to learning suggests that all learning occurs within a social context. Wenger & Trayner 37 describe a Community of Practice as a group of individuals who share a common concern or passion for an activity and continuously learn to improve their practice through regular interaction. Knowledge is generated through active participation, as well as through meetings and interactions between individuals across various environments. In this study, communities of practice resemble the working dynamics of ORNs, where learning occurs within the team as they engage in shared tasks and collaborative problem-solving.36,38
The two distinct approaches to understand teamwork and learning within the team, uncovered in this research, may impact the quality of care and preparedness for adverse events in the OR. It can be argued that the person-oriented team functions cohesively by actively gathering information and addressing knowledge gaps before entering the OR and attending to the patient undergoing surgery. This approach may be described as interprofessional, as common knowledge is shared among team members, enabling collaborative preparation. The personoriented team adopts a holistic approach to patient care, attending to the patient from multiple perspectives. According to Benner and colleagues, this aligns with a lifeworld perspective, encompassing the relief of pain, prevention of suffering, and promotion of safety, development, and overall well-being.35,39
Within perioperative nursing care, essential aspects include alleviating vulnerability and promoting comfort, dignity, and, when necessary, a peaceful death. 35 In contrast, the teamoriented approach often presents a fragmented understanding of the patient, as knowledge is primarily exchanged within the team and in the moment, with a stronger emphasis on surgical techniques than on the patient undergoing surgery. Research 40 indicates that nurses may hesitate to communicate openly in the OR, particularly when they fear contradicting colleagues perceived as higher in the hierarchy; concerns about seeming “unpleasant” also pose barriers to effective communication. 40 Communication among healthcare professionals is crucial for delivering safe and effective care. 41 Studies have shown that adverse events (AEs) decrease in settings that utilise structured communication protocols to detect and address preventable issues.41,42 However, speaking up to a senior colleague can be challenging, as hierarchy and chain of command can influence safe patient care practices. 43 These findings may reflect differing levels of team maturity, an area that warrants further research to understand the complexities of teamwork and collaborative learning. Additionally, this study could assist in identifying strategies for building effective, high-performing teams capable of delivering high-quality care while minimising AEs. 4
Strengths and limitations
This study, though based on a small sample, prioritises participants ‘personal perceptions and experiences, focusing on their individual insights rather than assessing “correct” or “incorrect” interpretations of learning. While perceived expectations may influence interview responses, they most likely reflect the nurses’ genuine perspectives. The study aims to capture how nurses express their understanding, offering a basis for potentially shaping ways of thinking and, ultimately, clinical practice.
Rigour and credibility of the study
This phenomenographic study employed rigorous methodology to uncover ORNs ‘perceptions of teamwork and learning within paediatric perioperative environments. In establishing the study's trustworthiness, four criteria – credibility, dependability, transferability, and confirmability were considered. 33
Credibility
Credibility ensures that the findings accurately represent participants’ perceptions. 44 This study enhanced credibility through the use of semi-structured interviews, a standard approach in phenomenographic research, 26 to elicit authentic and detailed responses. The interviews allowed ORNs to articulate their subjective experiences and interpretations of teamwork and learning. By pilot testing the interview guide and refining the questions, the study further ensured that the questions were appropriate and facilitated a deep exploration of the phenomena. Additionally, the study maintained reflexivity, with the primary researcher, a trained interviewer, actively considering any potential influence on the participants’ responses.
Dependability
Dependability, which concerns the stability and consistency of findings over time, was assured through adherence to a rigorously documented phenomenographic process, thereby promoting transparency and reproducibility. 33 Data analysis followed the seven-step procedure outlined by, 33 encompassing phases from familiarisation and condensation to contrasting. Each stage was meticulously described, and the iterative nature of phenomenography allowed for multiple cycles of analysis and refinement of categories, ensuring robustness. Furthermore, comprehensive audit trails and detailed documentation of analytic decisions reinforced the dependability of the study.
Transferability
Transferability refers to the degree to which findings may be applicable in other contexts. Although the sample comprised a relatively small cohort of ORNs (n = 10), participants were purposively drawn from diverse paediatric surgical units across six Swedish hospitals, thereby enhancing the potential relevance of the findings to similar clinical environments. 45 Rich descriptions of participants, their organisational settings, and the specific context of paediatric operating rooms were provided, enabling readers to assess the applicability of the findings to their own circumstances. Nevertheless, as a phenomenographic study, transferability remains inherently constrained, given its emphasis on capturing particular perspectives rather than generating broadly generalisable conclusions. 46
Confirmability
Confirmability, which addresses objectivity in qualitative research, ensures that interpretations are grounded in participants’ accounts rather than researcher bias. 47 Throughout the analytic process, the research team engaged in critical dialogue regarding participants’ descriptions, meanings, and perceptions of the phenomena, thereby mitigating subjective influence. The analysis adhered to established phenomenographic principles, and verbatim quotations were incorporated to exemplify participants’ experiences, providing transparency in the derivation of themes and supporting the confirmability of the findings.
Conclusion
The findings offer insight into two distinct approaches to teamwork and learning in the paediatric OR: a team-oriented approach, focusing on shared knowledge and interprofessional collaboration, and a person-oriented approach, emphasising individualised patient care and specific preparation. These diverse perceptions could influence care quality and preparedness for AEs, as they reflect different focuses on the team versus the individual patient.
The study's insights also underscore the importance of adaptive teamwork approaches in perioperative care, with implications for improving patient outcomes, supporting collaborative learning, and addressing communication barriers associated with hierarchical structures. The study contributes valuable knowledge on how ORNs perceive and approach teamwork and learning in high-technology clinical settings. Further research could explore the concept of team maturity to better understand how teamwork and learning evolve and their impact on clinical practice. Such research would assist in identifying strategies for fostering effective, highperforming teams capable of delivering high-quality, safe patient care, minimising AEs.
Implications for practice
The findings of this study highlight important considerations for enhancing teamwork and learning processes among ORNs in paediatric perioperative care. Emphasising both teamoriented and person-oriented approaches in practice could lead to improved patient outcomes and safer surgical procedures. Integrating these approaches within training programmes for ORNs may enhance preparedness for complex cases and foster a culture of collaborative, interprofessional learning. Such training programmes could consist of team-oriented training and person-oriented preparation, addressing hierarchical barriers, and continuous professional development. By enhancing these practices, healthcare organisations can support ORNs in delivering high-quality, safe, and patient centric perioperative care.
Footnotes
Acknowledgments
A sincere thank you to the ten ORNs who participated in this study, generously sharing their insights and experiences regarding their learning processes throughout their careers. The majority of these participants worked in children's operating departments within academic hospitals, while some were employed in regional hospitals, serving both paediatric and adult patients in operating departments.
Ethics approval statement
The study was approved by the Karolinska University Ethical Committee and follows the Swedish ethical regulations and the Declaration of Helsinki (World Medical Association, 2018). Permission to conduct the study was also obtained from the heads of the Intensive Care Units before the study started. Karolinska University Hospital in Stockholm, EPN 20171129/ Dnr: 2017-1722-3/1
Participants consent statement
The participants were given written and verbal information about the study before the interviews. Participation was voluntary, and the participants could withdraw without explanation without any effects on their work situation. All informants gave their written consent to participate.
Author contributions
All authors have been working together in this study, and contributed as decided within the team.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will not be available due to the protection of the participants’ integrity
Permission to reproduce material from other sources
N/A.
Clinical trial registration
N/A.
Conceptualization
Irini Antoniadou, Janet Mattsson.
Data collection
Irini Antoniadou.
Formal analysis
Irini Antoniadou, Janet Mattsson.
Methodology
Irini Antoniadou, Janet Mattsson, Sebastiaan Meijer, Gunilla Björling.
Supervision
Sebastiaan Meijer, Janet Mattsson, Karin Pukk Härenstam, Gunilla Björling.
Validation
Gunilla Björling.
COREQ checklist has been followed.