
Abstract
Adverse events lead to the emergence of several groups of victims, among which the second victims are medical staff involved in them. The suffering of second victims can lead to new adverse events and new victims. This study describes the cycle of an adverse event and its victims. Using the example of the largest Croatian hospital centre, authors try to understand how deep medical staff experience adverse events, and how different groups of medical staff (by profession, gender, qualification, and position) perceive adverse events. With the help of a special survey using the Bonferroni method from ANOVA, it was established that males feel more mental stress after adverse events than females. The results indicate that medical staff of different professions perceive adverse events differently, e.g. they are the least painful for psychiatrists and microbiologists and the most stressing for emergency and intensive care workers. In addition, nurses are more vulnerable to adverse events and experience various types of mental disorders more deeply than doctors. However, qualifications do not seem to affect the extent to which medical staff perceive adverse events. The results of this study differ from previous data for other countries and suggest new implications.
Introduction
When patients visit their healthcare providers, they are not aware of their state of physical well-being or mental state, nor of potential stressful events that may be occurring in their private lives. Patients assume that their healthcare providers are in optimal physical and mental state and that these always provide qualified medical assistance. There is ample evidence, though, that shows that doctors and nurses are more likely to be involved in adverse events when they are mentally unwell, leading to potential harm and even death of patients.1,2 Moreover, the actual involvement in an adverse event has wide ranging and far-reaching consequences that could be the cause for subjecting healthcare professionals to mental ill-health 3 and sudden identity shift from ‘the potentially infallible’ to ‘the potentially fallible’ health professionals. 4 Indeed, an adverse event can lead to negative consequences for patients and their relatives, but also to healthcare workers, and the institutions. 5 So, in the literature the terms first, second, and third victim of adverse events are being used. The first victim is the patient himself and her/his family (relatives). Unexpected adverse events occur rather frequently, and particularly medical errors are reported as being the third-leading cause of death after heart disease and cancer. 6 The second victim is the doctor, nurse or other healthcare professional involved (directly or indirectly) in the adverse event, whereas the third victim is related to the health institution, which could be connected to the reputation of the healthcare institution. The patient safety professionals who are responsible for investigating the adverse event have been also been considered in this classification 7 (Holden & Card, 2019). Regardless of the debate on the use of the term ‘victim’ in this context, 8 reality is that the impact suffered by patients, professionals, and healthcare institutions (as a set of professional teams that care for patients) is much greater than previously known 9 and in the next turn has a direct impact on the safety of next patients who will require healthcare. 10
At first glance, the main focus of an adverse event is the patient himself, who will suffer, loose health or his/her life. On delving deeper and tracing, the chain of events following the occurrence of an adverse event (Figure 1), the involved healthcare professionals with impaired cognitive functioning from the event, may become the sources of new adverse events, e.g. approximately 79% reported difficulty in concentrating. 11 Therefore, it is very important to not let this chain of events develop, but to prevent it from occurring.. This can be achieved by health organisations, by not only focusing on patients (and their relatives) but also on healthcare workers, mainly doctors and nurses when an adverse event occurs. It is indeed the management's support and their awareness of second victims that can help to prevent and correct adverse events without leading to new safety events.
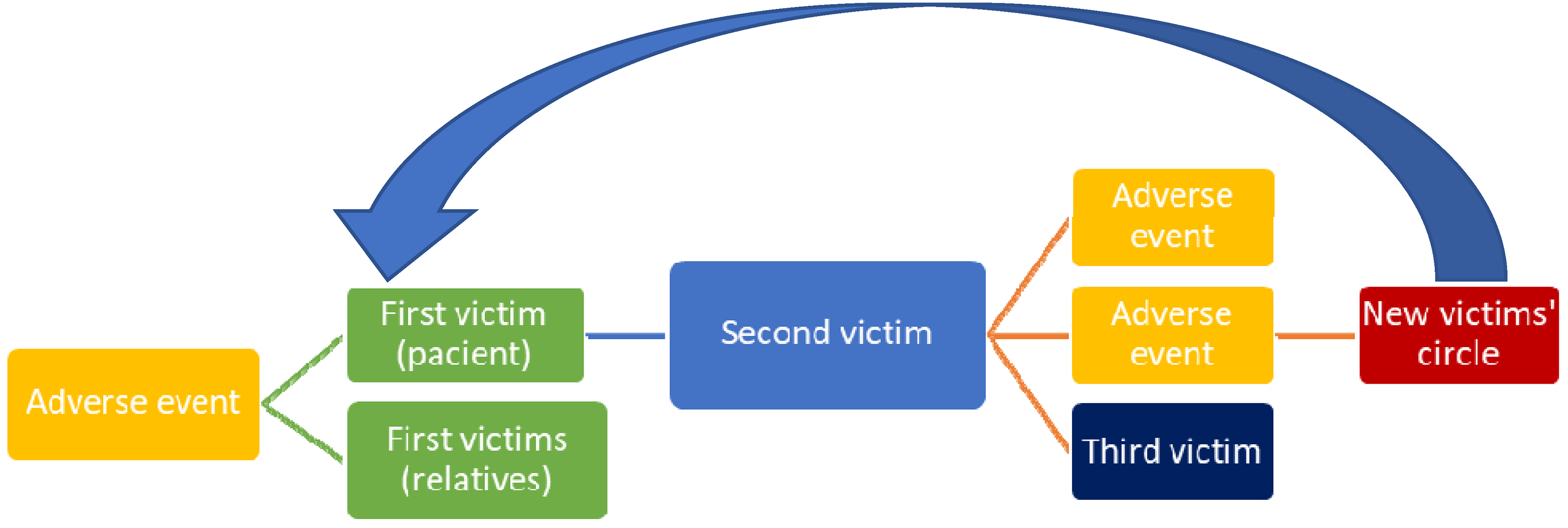
Circle of adverse event and its victims.
As can be seen in Figure 1, it is the second victim that is in the centre of this vicious circle. The development or stopping of the chain of adverse events and their victims mainly depends on the actions and mental state of second victim. It is in the power of the health worker (second victim) to stop this chain. However, for this, she/he must be mentally prepared foremost for possible adverse events in his work, which, as mentioned above, occur quite often. It is the mental problems of a health worker that arise after the appearance of the first victims that can cause new adverse events and, and as a result, new victims 12 called this chain of reactions a ‘domino effect’ and introduced the term ‘fourth victims’ for new patients suffering from new adverse events. Although the fourth victims are, in fact, the first victims that appear as a result of the closing of the cycle, which, if it is not stopped, will cause more and more patients to suffer from adverse events.
The severity of the problem of adverse events can be illustrated by the following reports: in 2015, the annual cost of preventable adverse events to the 30 member states of the Joint Action European Union Network for Patient Safety and Quality of Care in 2015 was in the range of 17–38 billion Euros. Besides, total disability-adjusted life years lost from adverse events was 3.5 million, of which 1.5 million years or about 43% could have been prevented. 13 However, this figure is not including the emotional disturbance suffered by patients, their relatives, and involved medical staff, which cannot be measured in terms of money.
Against this background, the aim of this study is to identify the extent to which various groups of healthcare professionals involved in adverse events developed symptoms of distress and whether they were asking for psychological help. The purpose of the study is to measure the depth of the second victim problem in Croatia, using the case of its largest medical facility, by identifying the most vulnerable groups of medical staff (by profession, gender, qualification, and position) in need of priority support.
Review of the second victim phenomenon
The second victim phenomenon was first described by Wu 9 from John Hopkins University who wrote: ‘Physicians will always make mistakes. The decisive factor will be how we handle them’, the second victim phenomenon was described by Scott et al. 14 in the first empirical study with 31 s victims who were ‘healthcare providers who are involved in an unanticipated adverse patient event, in a medical error and/or a patient related injury and become victimized in the sense that the provider is traumatized by the event’. Recently, this definition has been updated by the ERNST project in accordance to current data, as ‘any health care worker, directly or indirectly involved in an unanticipated adverse patient event, unintentional healthcare error, or patient injury, and becomes victimized in the sense that also the worker is negatively impacted’ [ 15 , p. 6].
The systematic review by Seys et al. 16 found that the prevalence of second victims after an adverse event varied from 10.4% up to 43.3% and that their reactions can be emotional, cognitive, and behavioural. Recently, Wu et al. 17 noted that the prevalence of clinicians emotionally impacted by adverse events is high, ranging in studies of different groups of providers from 10% to 50%. So, being in a state of mental distress, the second victim needs appropriate support, otherwise it may lead to a chaotic, liminal state with a danger and threat 4 for the impacted healthcare worker. Combined with impaired cognitive functioning, like difficulty in concentrating, 11 this can involuntarily increase the risk of him/her being involved in new adverse events (see Figure 1).
Over the past decade, appropriate literature has provided the evidences from various countries and healthcare disciplines of the relationship between patients’ adverse events and the mental state of healthcare professionals. So, recently, the link between second victims, i.e. medical staff that suffer from emotional distress, and that having such distress makes it more likely for new adverse events to occur (see Figure 1) has been confirmed by Wu et al. 18 in Taiwan. The anxiety and fear of failing again, found in second victims in Singapore 19 and Switzerland, 20 can also be a source of stress and lead to new adverse events. Stress at work can affect the ability for work of healthcare workers. 21 Similar possible reasons of adverse events, like emotional exhaustion, 22 work stress, occupational burnout, depression, 23 and low patient safety culture24,25 have been considered on the samples of Taiwanese physicians and nurses. Their research concluded that there may be a causal relationship and emphasised the need for further research to confirm association between staff attitude and the incidence of adverse events. Moreover, they stated the growing number of adverse events and the need for periodic assessment of the status quo of the patient safety culture, e.g. using the Chinese version of the safety attitudes questionnaire. 26
Considering 18 appropriate studies, which are based on the reports of above 11.6 thousand healthcare providers involved in adverse events, Busch et al. 11 found the following most prevalent psychological and psychosomatic symptoms of the second victims of adverse events: troubling memories, anxiety, anger, remorse, and distress. They concluded on the importance of preventive and therapeutic programs aiming at decreasing second victims’ emotional distress. Nydoo et al. 27 also confirmed that the effects of adverse events for the healthcare professional can be ominous, leading to feelings of sadness, guilt, and anxiety, as well as symptoms consistent with post-traumatic stress disorder. Besides, Ullström et al. 28 on a case of 21 health professionals from the Swedish university hospital also confirmed that emotional distress, often long-lasting, follows from adverse events and this distress is related mostly to the organisation's inadequate response to the event.
Therefore, any doubts about the term ‘second victim’, 8 e.g. due to possible lack of empathy for the affected patient and his family (first victims), can be removed, given the level of suffering that the adverse event brings to the medical staff involved. However, the questions remain how deep these suffering are and whether they relate to all categories of medical staff in the same way.
In reviewing the literature on second victims from various medical professions, we found that they occur in a wide variety of departments of medical institutions, ranging from surgery 29 to gynaecology.30,31 Obviously, during the COVID pandemic, 32 they also appeared in specialised COVID-departments of hospitals in the last 2 years.
We also found a few publications on ways of overcoming the problem of second victims. So, confirming that medical staff who experience the second victim phenomenon may be subject to a set of physical, psychological, and psychosocial problems following involvement in an adverse event, McDaniel and Morris 30 found that second victims who establish self-care activities such as diet, exercise, meditation, good peer, or family support, as well as get effective support programs are more likely to recover completely, and more safely resume their careers. Besides, Bohnen et al. 29 on a case of surgeons concluded that certain existing mechanisms to cope with difficult patient interactions after adverse events are healthy, but others are harmful, and could put both career and personal lives at risk. So, since second victims most commonly turn to peers for help, they suggested a peer support program as a mean to support colleagues in times of need. Moreover, Schrøder et al. 31 argued that investment in second-victim support programmes may prove to be an investment in safer and better patient care. Likewise, a cost-benefit analysis of a peer support programme demonstrated substantial hospital cost savings, proposing that the programmes should be developed and implemented in other European healthcare systems like in Denmark. However, such a programme should be strategic 33 to reduce future relapse risks.
Therefore, review of recent publications found the following issues, which will be considered in this study:
The study of medical staff's perception of involvement in adverse events can be organised using special questionnaires that should consider various kinds of mental distresses of second victims to figure out how deep their distresses are; The sample of the examined potential second victims should be divided into categories, including medical professions, experience, age, and gender, to find out whether this is the same problem for all healthcare professionals; Given the wide range of medical professions experiencing the problem of second victims, an expanded sample of representatives of various departments of the surveyed hospital should be considered, including COVID department, gynaecology department, etc. Given the importance of not only measuring the depth of the problem, but also understanding how to solve it, makes it reasonable to include points in the questionnaire related to previous experience of overcoming the consequences of adverse events examined by medical staff.
Moreover, the implementation of the Danish Second Victim Support Program proposed by Schrøder et al.
31
may cause difficulties on the European continent as it is not homogeneous. For example, in countries such as Sweden or Ireland, which have high healthcare performance,
34
similar programs have already been implemented and are not difficult to implement there. On the other hand, in countries with low performing healthcare systems such as Bulgaria or Ukraine,
35
the implementation of such programs may be difficult. Therefore, for this study, we selected a country where such a programme has not been implemented, but, having a level of relative healthcare efficiency above average, it could be successful, namely Croatia.
A pilot study in Croatia
According to the latest study from, 34 Croatia for 7 years had a relatively stable level of relative healthcare efficiency of about 0.7, which indicates the absence of ups and downs of this healthcare system. The Croatian health system is centralised and based on a mandatory health insurance system 36 which consolidates public financing under a single entity, the Croatian Health Insurance Fund. The social health insurance system comes with a nearly universal population coverage and a generous benefits package. According to the 2019 Health Care Act of Republic of Croatia, 37 ‘every person has the right to health care and the opportunity to achieve the highest possible level of health, in accordance with the provisions of this Act and the law governing mandatory health insurance in the Republic of Croatia’. Although Croatian per capita spending is low compared to other EU countries, the share of public spending as a proportion of current health expenditure is high and out-of-pocket payments are low. 38
Croatia has been developing a quality monitoring and analysis system for more than 15 years. The first laws of regulating quality in healthcare were the Act on the Quality of Health and Social Care of 2007 and the Ordinance on Health Care Quality Standards and their Application adopted in 2011. According to this Ordinance, all health care providers must continuously evaluate and improve the quality of their clinical and non-clinical procedures, to report adverse events, analyse them, and to plan corrective actions for their prevention. At the end of 2018, the Government adopted a new Act on Quality in Health Care. 39
In Croatia, there are sufficient physical resources, such as hospital beds, and human resources overall, on a par with other European countries. Accessibility of services is generally high, covering over 99% of the population, with a wide range of services covered by mandatory health insurance. However, some more remote areas, such as the islands of the Adriatic coast and rural areas in central and eastern Croatia face shortages. More people in Croatia (0.7% in 2019, compared to an EU average of 0.1%) reported unmet medical needs due to distance than in any other EU Member State. Central Croatia, mainly Zagreb County and the City of Zagreb, has the largest number of facilities and healthcare workers. 38
University Hospital Centre (UHC) Zagreb is the largest health institution in the Republic of Croatia, considering the number and diversity of health services it provides. This is a hospital with 29 hospital departments, about 1500 hospital beds, and more than 1.500.000 patients per year. In the UHC, there are employed 1200 medical doctors, 2600 nurses, and 1000 other health care workers. Every day, the hospital ensures basic care and highly sophisticated medical procedures for patients from Croatia and abroad.
UHC Zagreb has implemented educational programs about safety culture in all hospital departments. For more than 10 years, Department for Quality Assurance and Improving Quality in Healthcare provided educations and workshops about adverse events and patient safety as well as staff safety. Now, UHC Zagreb has clear procedures for reporting and managing adverse events, a hospital register of adverse events, a quality committee of UHC Zagreb, and analyses adverse events with the purpose of proposing preventive measures. If a serious adverse event happens, initially the healthcare workers have to discuss the issue at the professional meeting of the department where the event took place. In a culture of patient safety manner, healthcare professionals openly discuss the causes of the event. However, there is not enough attention given to the negative impact of adverse events on the mental health of healthcare providers involved in adverse events, or attention to how healthcare professionals feel after an adverse event.
During this pilot study, all departments of the UHC Zagreb had difficult working conditions due to the period of COVID-19 epidemiological measures and new rules, during which they became even more aware of the need for attention to ensure the safety of patients and staff.
The goal of this pilot study is to identify whether the medical staff (doctors and nurses) of the various departments of the UHC Zagreb had any adverse events in their working life, how they felt, and whether they asked for help.
Methods and data
This cross-sectional study was conducted in May 2022 in University Hospital Centre Zagreb in seven selected departments at the hospital. The departments for: psychiatry, microbiology, gynaecology, anaesthesiology – intensive care unit for COVID-19, emergency medicine – COVID-19 unit, and orthopaedic surgery).
During the period of the study, the selected departments employed 517 workers. All doctors and nurses working at the clinical departments were invited to participate in the study. Out of the 517 employees, the questionnaires have been distributed among 124 doctors and nurses, which is about a quarter of all staff at the selected departments.
The questionnaire used for conducting the survey was adapted for the purpose of this pilot study from the pre-designed form (Table 1). To identify the features of the perception of adverse events by medical staff, the following study scheme was proposed. Initially, candidates were randomly selected to conduct a survey from various departments of the hospital. The questionnaire contained various characteristics of the medical staff by gender, age, profession, level of education, etc., as well as a number of questions regarding their perception of adverse events. The survey was conducted anonymously to avoid embarrassment of the interviewed medical staff and to increase the degree of truthfulness of their answers.
Questionnaire for medical staff perception of adverse events.
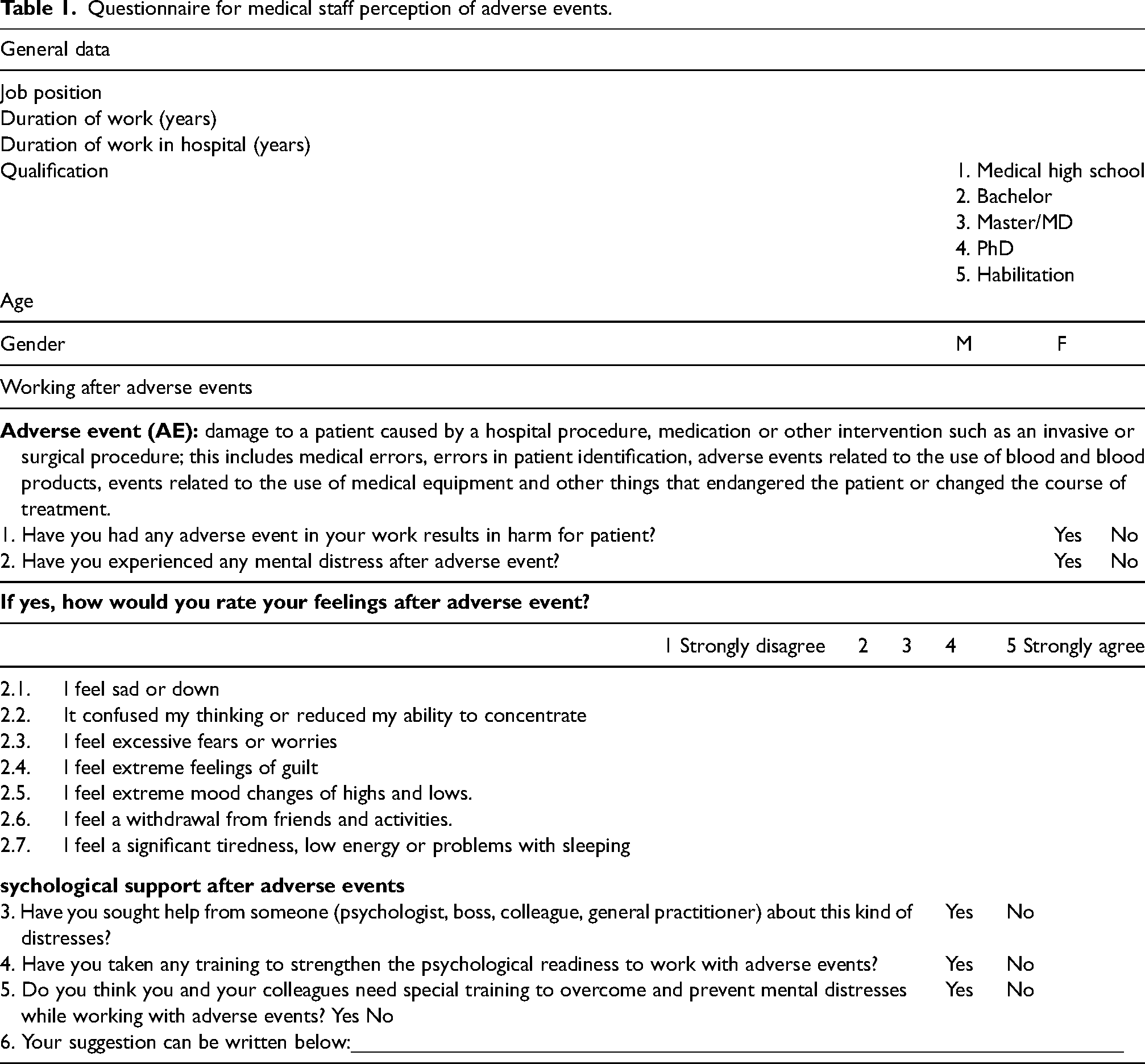
The questionnaire has been printed and distributed among 124 doctors and nurses of Zagreb UHC, which is from 15 to 27% of all the departments’ staff that can be involved in adverse events.
The sample covers about 16% of the entire medical staff of the observed hospital departments.
The Bonferroni method with ANOVA has been applied to compare the results of the questionnaire and compute the confident differences between the groups of medical staff regarding gender, age, profession, duration of work, and perception.
40
Here, the following null hypothesis has been tested: H0: All groups of medical staff perceive adverse events in the same way.
Hence, if, when testing the hypothesis using the ANOVA method, it turns out that the chi-square is sufficiently high, and the probability of this null hypothesis is lower than 0.05, this will indicate that there is a significant difference in perception between the groups of medical staff.
In addition, the Pearson correlation coefficient was used to establish the degree to which medical staff responses were consistent with their attributes. 41
Results
The response rate for the questionnaire was 75% (93 of 124 respondents). As the results of processing the questionnaires showed, more than a third of the respondents, namely 35.5%, had experienced adverse events at work (further – experienced staff). Moreover, males experienced adverse events somewhat more often than females (37.5%). Almost all experienced staff had mental distress after adverse events. However, among experienced female staff more than 10% turned to someone for help. Among males, on the other hand, not a single respondent turned for help. At the same time, not a single female staff received training to improve their psychological readiness (a state of receptivity to an experience) to face, and work with adverse events, while 16.8% of the experienced male staff got training. Nevertheless, most respondents, namely 75.3% (87.5% of males and 72.7% of females), agreed that they need special training to prevent, work with, and overcome mental distresses from adverse events.
Thus, in general, the problem of adverse events concerns every third health worker who is subject to one or another mental distress. The female part of the medical staff is more inclined to seek help from a psychologist, superiors, and colleagues than to undergo special training. The male part of the medical staff is ready to train and solve their psychological problems on their own, without seeking help from the boss, colleagues, or specialists. However, males are slightly more likely to experience such adverse events in their work than female medical staff.
Profession differences
Considering the profession (department) as a group factor, the null hypothesis was disproved for all the response options. As can be seen from Figure 2(a), the probabilities of the null hypothesis for each of the questions were close to zero (within the interval 0.0001–0.0007) with corresponding high Chi-Squared.
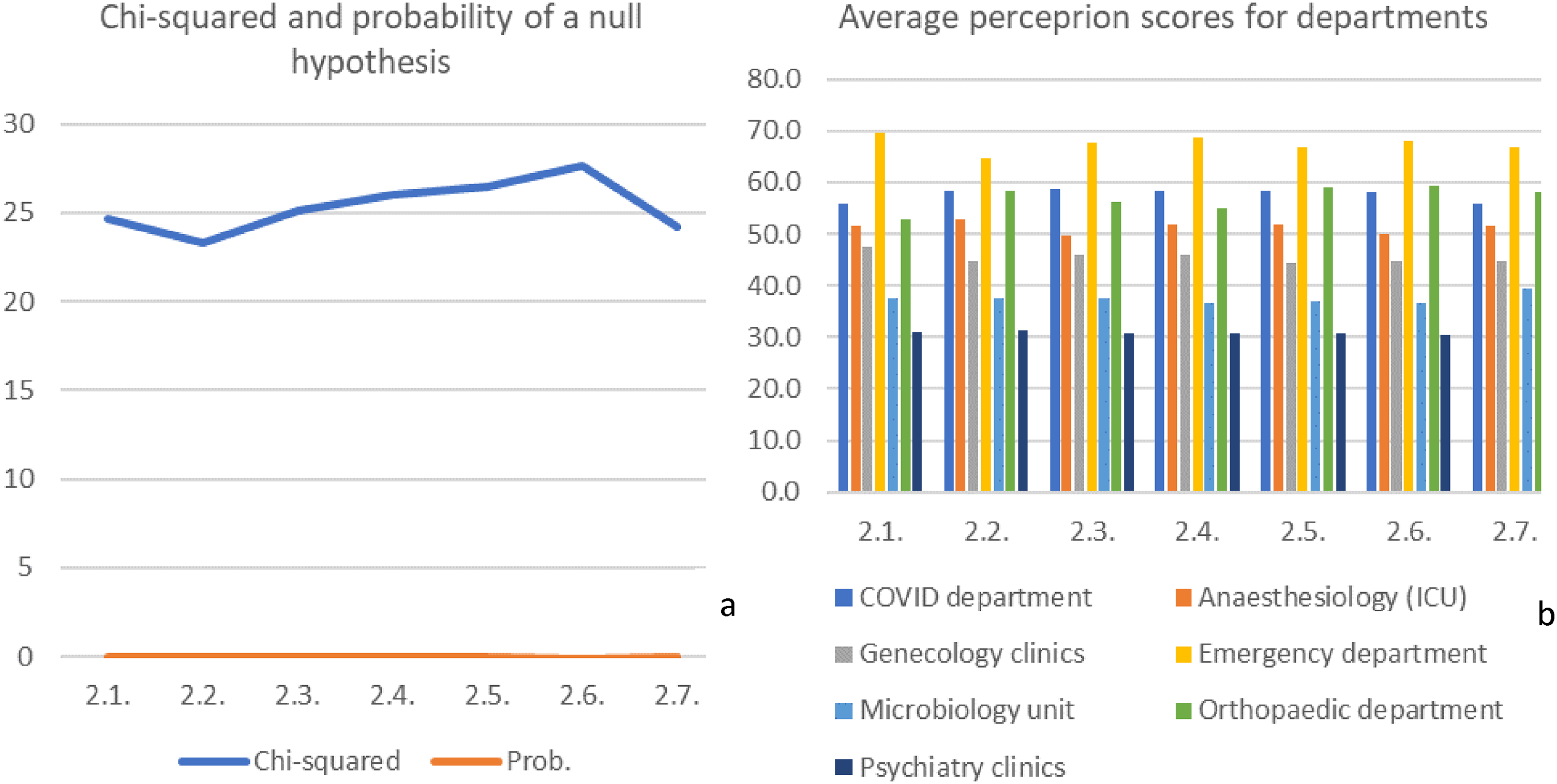
Characteristics of differences between responses of hospital departments (professions).
The most notable differences were recorded in the responses of the Department of Emergency Medicine and Department of Psychiatry and Psychological Medicine, whose average scores for each of the questions differed by more than two times (Figure 2(b)). Also, very high average scores were recorded in the responses of the COVID Department, Orthopaedic Department, and ICU, while the Microbiological Department showed relatively low response scores for all the questions.
Qualification differences
Dividing the medical staff into groups according to qualification level, we were unable to refute the null hypothesis for any of the questions asked. The Chi-squared for all questions was below 2, which gave the probability of confirming the null hypothesis in the range from 0.72 to 0.87. This means that qualifications do not affect the extent to which medical staff perceive adverse events.
Gender differences
Comparing the average scores of the perception of adverse events between the genders, it can be found that male staff experience more mental distress after them than female staff (Figure 3).
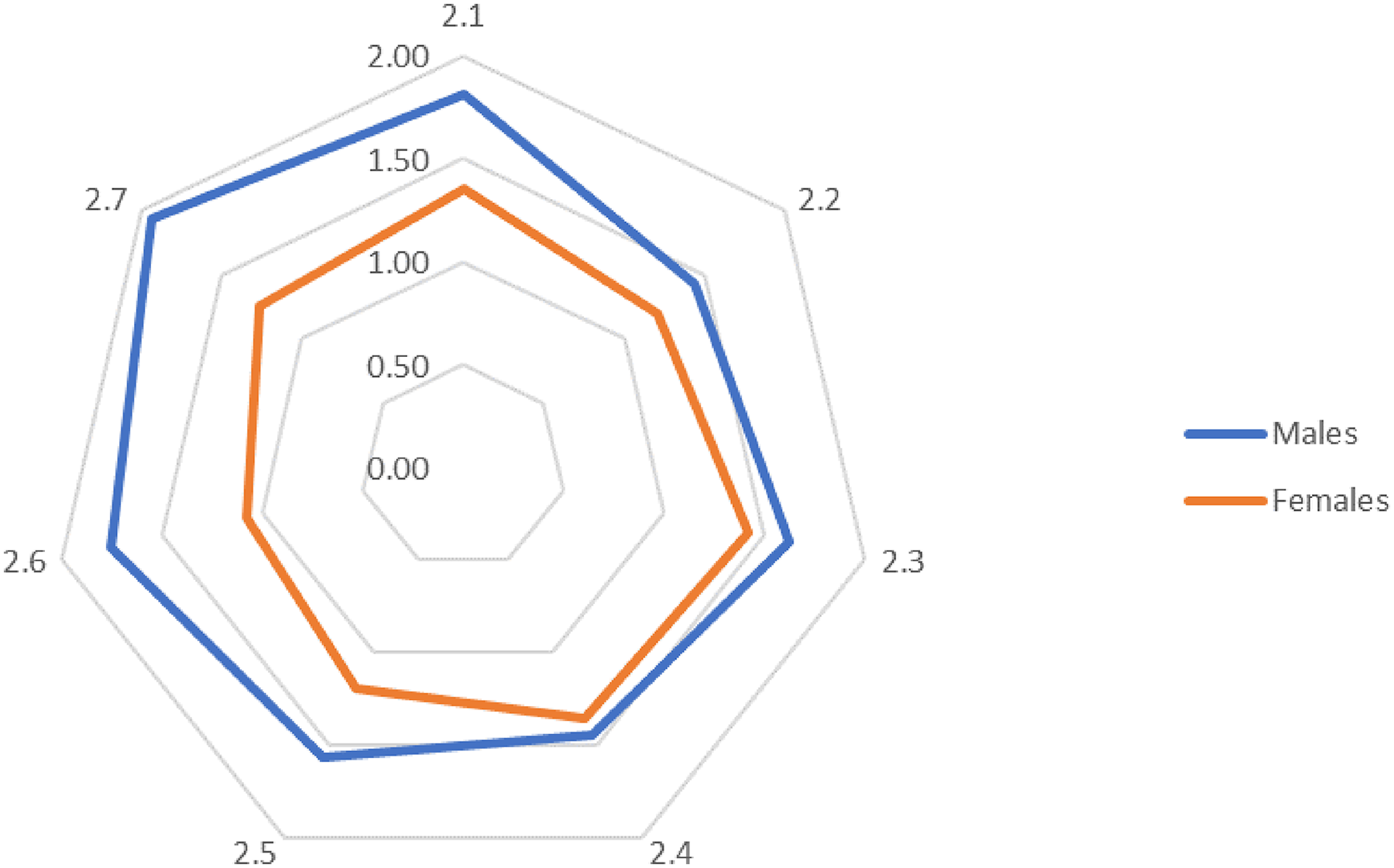
The average scores of responses of female and male medical staff.
Average scores show that among other distresses, male medical staff are most deeply feeling a significant tiredness, low energy, or problems with sleeping after adverse events. At the same time, female staff in similar situations are more vulnerable to feeling excessive anxiety or worry.
However, despite the presence of certain differences between the perception of adverse events by female and male medical staff, the obtained scores of chi-squared and probabilities indicate the absence of significant differences in their perception of adverse events. The most probable difference, with a probability of a null hypothesis of 0.17, was for question 2.6 that indicates a relatively higher degree of males experiencing a withdrawal from friends and social activities after adverse events compared to their female counterparts.
Job position differences
Looking two respondent groups with different jobs and responsibilities, namely doctors and nurses, we were able to find significant differences in their perception of adverse events. As can be seen from Figure 4(a), the most significant differences with a probability of a null hypothesis below 0.05 were recorded for questions 2.5, 2.6, and 2.7.
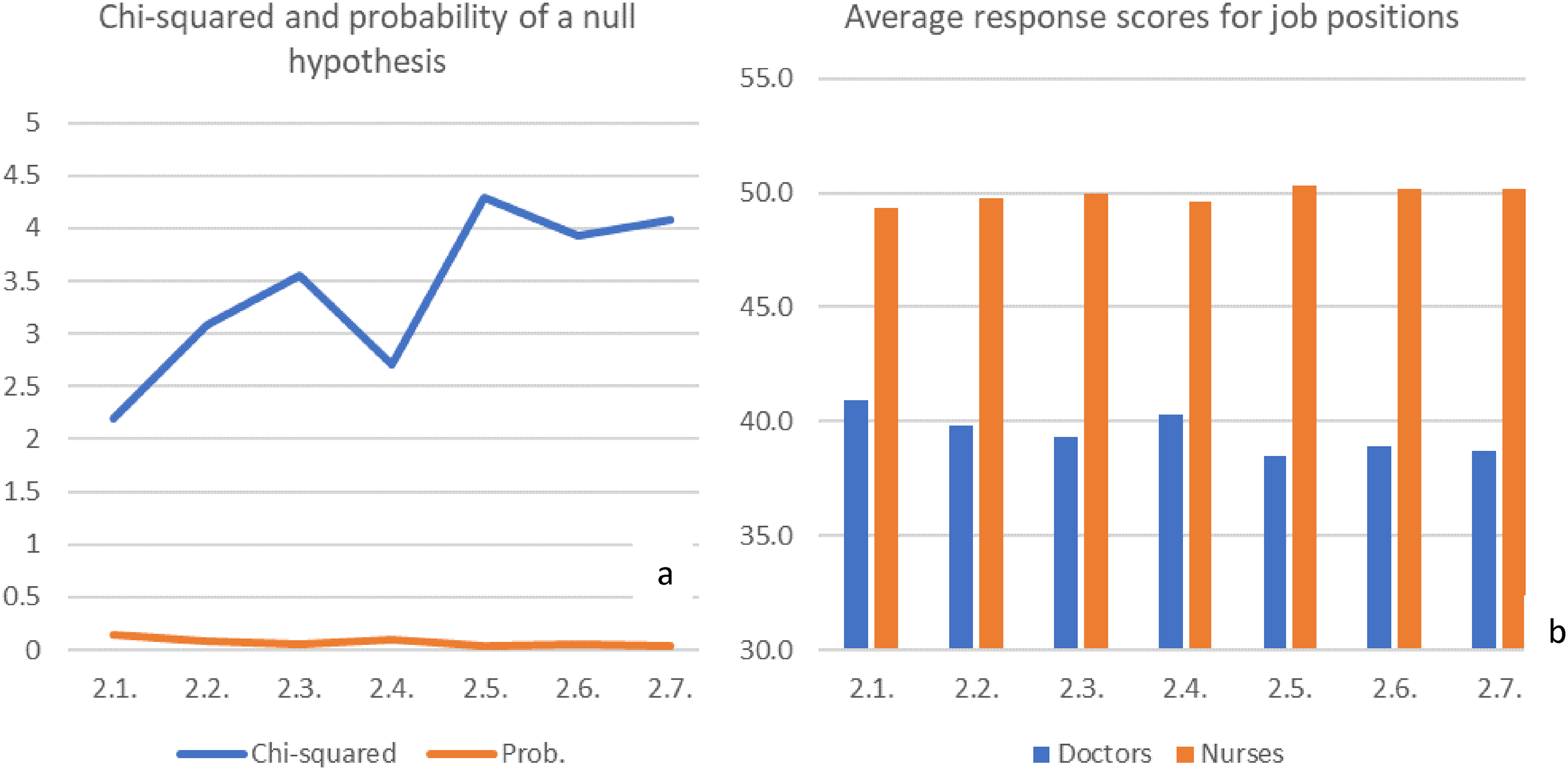
Characteristics of differences between responses of doctors and nurses.
As can be seen from Figure 4(b), the nurses’ perceptions of adverse events on all questions were significantly higher than the doctors’ perceptions. This suggests that nurses are more vulnerable to adverse events, and experience mental distresses after adverse events more deeply than doctors.
Discussion
The results of the survey contrast with previously obtained data for other countries. 35.5% of staff have experience with adverse events, which look quite low in comparison to 76% for physicians in the UK obtained by, 42 86.3% for health professionals in Spain found by, 5 or 42% of health providers observed (23%) or involved (19%) in any type of adverse events in the US. 43
However, the obtained results are comparable to the results of studies from other countries, which consider only serious adverse events with heavy aftermaths from temporary physical disability to death. For instance, in Norway, only 28% of doctors reported that they had experienced at least one adverse event with serious patient injury. 44 In Spain, the level of medical staff with experience of serious adverse events is higher – 57.8%. 5 Andrews et al. 45 found that 17.7% of US patients experienced at least one serious adverse event from temporary physical disability to death, when healthcare providers identified adverse events in 45.8% of patients. In other countries, a wide range of patients with experience of adverse events has been identified, i.e. from 3.3% in Italy 46 ; 5.7% in Netherlands 47 ; 8.2% in eight African and Asian countries 48 ; 12.2% in Ireland 49 ; 12.3% in Sweden 50 and Switzerland 51 ; 12.5% in Portugal 52 ; 15.3% in Canada 53 ; and 21.9% in Australia. 54 Among US paediatric patients, only 1% experienced adverse events, of which 60% may be preventable. 55
The difference between the percent of total adverse events identified by health providers and serious adverse events reported helps to understand the possible difference in the level among experienced workers in Croatia compared to other countries. Apparently, Croatian doctors and nurses do not consider an adverse event as such unless it results in serious damage to the health or death of the patient. Perhaps the experience of the war (at the end of twentieth century) and the harsh transition period, which makes people more patient and less receptive, have raised the threshold of sensitivity of the medical staff in this country. Moreover, the existing culture of blaming 56 and other reasons 57 may be a factor in the reluctance of health professionals to report the facts of adverse events. However, verification of such assumptions regarding the Croatian healthcare workers certainly requires additional study.
As has been found, the problem of adverse events concerns every third Croatian health professional who is subject to one or another mental distress. The female part of the medical staff is more inclined to seek help from a psychologist, superiors, or colleagues than to undergo special training. The male part of the medical staff is ready to train and solve their psychological problems on their own, without seeking help from the boss, colleagues, or specialists. However, males are slightly more likely to experience such adverse events in their work and have a higher level of psychological distress after them than their fellow female medical staff. Moreover, among other distresses, male medical staff are most deeply feeling a significant tiredness, low energy, or problems with sleeping after adverse events, while females are most vulnerable to feeling excessive fears or worries.
It was found that qualifications do not affect the extent to whether medical staff perceive adverse events. However, profession and job position matter.
The findings imply that medical staff in different professions perceive adverse events differently. They are the least painful for psychiatrists and microbiologists. Microbiologist do not have personal contacts with patients and, probably, therefore do not perceive the adverse events in the same way as healthcare workers who are in direct contact with the patients and their relatives. At the other hand, psychiatrist are more experienced than other healthcare workers in how to perceive and cope with mental distress, and they are likely to be less surprised and less affected in this area.
As a contrast, the deepest and most painful experiences of mental distress from adverse events are perceived by representatives of the Emergency department, as well as the COVID and Orthopaedics departments. Apparently, they are more likely than others to experience adverse events that have a stronger impact on their mental state. In the COVID-departments, ICU and Department for Orthopedic Surgery, there are patients with very serious health conditions, and adverse events could potentially cause heavy harm for the patients.
It was also found that nurses are significantly more vulnerable to adverse events and experience various kinds of mental distresses after them more deeply than doctors. This means that nurses are more exposed and sensitive and need priority support.
Conclusion and implications
Based on the results of a pilot study of the perception of adverse events by medical staff in Croatia, results and findings were obtained that allow the following conclusions to be drawn.
Obviously, each health worker is unique and has a particular perception of an adverse event. However, the identified features make it possible to identify those groups of medical staff who primarily need support, since they experience the greatest mental distress after adverse events. Appropriate recommendations can be made to address the problem of second victims step by step. For instance, it is important to pay more attention to preparing medical staff for adverse events and strengthening their stress resistance through special training. First of all, training is needed by male medical staff, who, as it turned out, are not inclined to seek psychological help from specialists, their boss or colleagues. Besides, more support is needed for nurses who are more likely to suffer from adverse events than doctors. And, of course, the greatest efforts to prevent second victims should be directed to frontline healthcare workers, including the emergency, anaesthesiology, and COVID department staff.
The implementation of such recommendations requires the efforts of healthcare management. At the highest level, this is the adjustment and strengthening of support to medical staff of the neediest units (emergency, intensive care and COVID), as well as groups of vulnerable workers in terms of gender and age, for example, in the form of special courses on their mental support. Recommendations can be embedded in the development strategy of hospitals and the entire health care system. In addition, the extent to which these proposals will be implemented depends on middle managers. Their role should be to promote a culture of forgiveness and support for colleagues who find themselves in an adverse event. Apparently, they should give more attention to more vulnerable groups of personnel who require more support and empathy.
The question about the impact of adverse events on the professionals themselves was left open without specifying a time period. As in other studies, the most traumatic experience tends to be the one most remembered and answered.
Further research should be aimed at developing special measures to prevent and solve the problem of second victims, e.g. the introduction of special courses or modules in the disciplines studied by medical students in colleges and universities; conducting special trainings for active medical workers for their psychological preparation for adverse events and their consequences; activation of psychological services at medical institutions. All this will contribute to reduce the problem of second victims in healthcare.
Further research may also be aimed at determining the extent to which blaming culture and other possible factors influence the perception and willingness of healthcare professionals to report adverse events.
Footnotes
Authors’ contribution
AGG conceived of the presented idea, developed research methodology, conducted data analysis, and presented results, discussion, and conclusions. BK collected the data and helped with the manuscript preparation. SB reviewed and improved the manuscript. JJM managed research project and improved the manuscript. All authors discussed the results and contributed to the final manuscript.
Acknowledgements
Availability of data and materials
The data sets analysed are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by the COST Action CA19113 “The European Researchers’ Network Working on Second Victims” (ERNST) under the grant [no number] for short-term scientific mission in UHC Zagreb. This Action is supported by the European Cooperation in Science and Technology.
Ethics approval and consent to participate
The Ethical Committee has proved that this study complies with the ethics of scientific research described in the Hospital Charter of Ethics and Ethical Principles of the Declaration of Helsinki and other applicable ethical principles and legislation (Zagreb, 02/13 AG, 6.07.2022). The Ethics committee in University Hospital Centre Zagreb approved the current research. Furthermore, the institutional research board at each hospital gave an additional permission to carry out and publish the results of the study. Questionnaire was preface with the letter explaining the objectives of the study and assuring the respondents the anonymity and confidentiality of their response. Questionnaires were distributed in non-marked envelopes to each hospital department. All questionnaires returned anonymously in sealed non-marked envelopes to protect participants’ privacy. Participation in the study was voluntary. The informed consent was obtained from all the participants.