
Abstract
Purpose
Previous literature identifies increased burnout in female surgeons and contributors to fatigue outside of work. However, it is not yet understood whether there are gender discrepancies of contributors to fatigue or coping mechanisms for workplace fatigue in surgeons. This study aims to identify gender differences in causes of fatigue, how fatigue occurs and any interventions/strategies that surgeons may use/know to try and mitigate the effects of fatigue.
Methods
Using an online questionnaire at a single hospital in England, the questionnaire asked whether surgeons had been subject to any contributors to fatigue at work and what contributes to their fatigue at work using a list of multiple-choice answers.
Results
97% of surgeons suffer from at least one contributor to fatigue. Females were statistically more likely to suffer from musculoskeletal injuries at work than males and more likely to suffer from mental exhaustion. Females were significantly more likely to contribute fatigue to prolonged static postures, lack of control during the shift and high levels of demand. To mitigate fatigue, females were significantly more likely to change positions whilst operating. Males were less reluctant to adopt Microbreaks during surgery to reduce musculoskeletal fatigue.
Conclusions
Our analysis identifies gender differences with coping mechanisms and the onset of fatigue. There is still a stigma attached to workplace fatigue in surgeons. Acknowledgement of these gender differences in fatigue is critical to reducing the statistical likelihood of fatigue onset in both genders. Further research should identify whether surgical operating rooms are adequately suitable for females.
Introduction
Shift workers often struggle with chronic fatigue as a result of their inability to obtain sufficient sleep due to a variety of factors, such as an interrupted circadian rhythm cycle prompting wakefulness or sleepiness each day, causing incomplete homeostatic recovery and consequently fatigue as a bi-product. 1 Of these shift workers, intensive care unit staff, particularly surgeons, work around the clock, maintain on-call hours, and engage in overtime, which ultimately increases the likelihood of medical errors due to fatigue, which will likely cause patients harm. 2 Long hours with constant interruptions, complex patient care needs and draining emotional interactions may heighten the risk for the development of a poorer professional quality of life. 3 The physical nature of the work and high levels of concentration can all heighten the impact of fatigue, with higher demanding tasks requiring more energy to complete thus exacerbating the effects of fatigue over time. 4
There is good evidence to support the use of ‘microbreaks’ (∼1 min pauses every 20–40 min with the opportunity to stretch, relax and reflect on the operation) in the operating theatre to reduce the likelihood of musculoskeletal injuries sustained during a surgical career and consequently improve patient safety and surgeon longevity.5–11 However, fatigue in surgeons goes beyond the operating theatre and limited studies exist monitoring the fatigue of surgeons throughout their shifts, as well as other contributors to fatigue, such as mental exhaustion, compassion fatigue or environmental constructs such as bright lights and/or lack of food during shift. 12
The surgical workforce has changed in recent years, with an increase in female surgeons. Recent studies have evaluated the gender differences in junior residents for perceptions of patient safety, resident education, well-being and job satisfaction, recognising females as more likely to be dissatisfied with patient safety, overall wellbeing and time allocated with family. 13 Other research aimed at assessing the gender differences in surgeon burnout and psychological wellbeing determined that female surgeons have less rest between shifts, working a higher proportion of >80 h weeks as well as increased reports of losing sleep over worrying, feeling unhappy and losing confidence in themselves. 14
Other previous research has aimed to examine gender-related differences in surgeon fatigue and identified a number of causes that occur outside of the working day. A systematic review identified increased emotional exhaustion in females due to unbalanced time spent on non-work roles such as parenting, resulting in worse work–life balance in comparison to males. 15 Whilst the systematic review found four studies reporting significantly higher levels of burnout in females, five studies showed no statistical difference. Despite the breadth of previous research, there is still a paucity of evidence specifically around gender-related differences in surgeon fatigue during the workday.
Limited evidence exists in the literature for identifying the causes of fatigue at work, as well as any contributors to fatigue, to practically mitigate the onset. Contrary to previous publications, this study aims to identify the gender differences for the causes of fatigue in surgeons within the workplace, understand how fatigue occurs and explore any interventions/strategies that surgeons may apply to try to mitigate the effects of fatigue in the workplace. The authors hypothesise heightened levels of fatigue in female surgeons throughout their shift due to the negative work-life balance and heightened levels of compassion fatigue found in previous research.3,14 Drivers for fatigue in female surgeons are hypothesised to be higher perceived levels of demanding work and patient outcomes, and it is hypothesised that younger surgeons will be more susceptible to fatigue than their older, more experienced counterparts. 15
Method
The study was approved by the University of Liverpool's Ethics Committee on 30/01/2020. Data were analysed by the research team in line with the University of Liverpool's ethical guidance. Data was only accessed and analysed by the research team. For data collection, the online questionnaire website ‘SmartSurvey’ was used to collect anonymous data from surgeons at a northern hospital based in England, UK. Similar to previous research, data was collected from one hospital. 16 Participants gave informed consent before participating in the questionnaire. All surgeons working at the hospital were eligible to take part. Surgeon participation was voluntary and they could stop the questionnaire at any point. Surgeons were under no obligation to answer all of the questions.
The 14-part questionnaire (Online Appendix A) contained four demographic questions; age range, gender, duration of surgical experience and department of work. The estimated time of completion was 5–10 min. The questionnaire then asked whether surgeons had been subject to any contributors to fatigue at work (e.g. musculoskeletal, physical or mental exhaustion), what contributes to their fatigue at work and whether they have attempted to minimise these conditions at work (including but not limited to surgery), using a list of multiple-choice answers. For these questions, surgeons were asked to relate to their previous month of work. For the purposes of homogeneity across our sample, other questions included average sleep per night, average hours worked per week, whether they were aware of any intervention strategies to mitigate workplace fatigue and their opinions on taking ‘microbreaks’ during surgery to reduce fatigue. Additionally, we asked participants their thoughts on wearable technology capable of monitoring their fatigue levels whilst at work and whether they are likely to drive a car whilst fatigued. The purpose of these questions was to understand surgeon willingness to have their fatigue levels observed in real-time for future research. For all questions, surgeons were given the option to specify ‘other’, make comments on the question or select the option ‘prefer not to say’.
For the purposes of data collection, a liaison at the hospital distributed the questionnaire on behalf of the research team. The survey was first distributed in March 2020 and the survey was closed in May 2021. At this time, there were three prompts for surgeons to complete the questionnaire; March 2020, September 2020 and April 2021. Prompts were delivered via email, including a web link to the questionnaire.
Data analysis where appropriate was carried out using SPSS Statistics 24. Relationships between contributors to fatigue and gender were examined by the χ2 test. A p-value < 0.05 was used for statistical significance. Cross-tabulation with contingency tables was used to split results by gender for the prevalence of fatigue, what contributes to their fatigue and any mitigation strategies implemented in the workplace.
Results
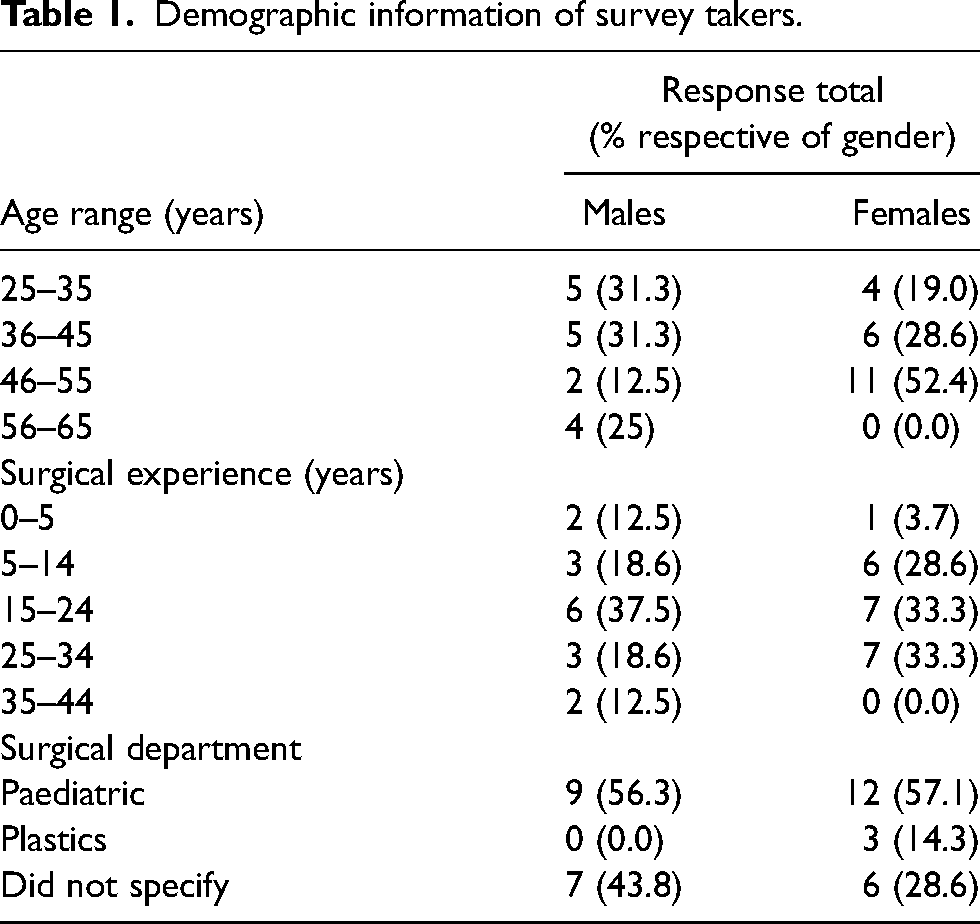
For the questionnaire, there was a response rate of 56% (37 out of 66 surgeons completed the questionnaire, with an additional 22 partial completions. Responses included 16 male and 21 female surgeons. Table 1 shows the demographic information collected from the questionnaire. No partial completions were included in the final analysis. Figure 1 shows the occurrence of fatigue contributors prevalent in surgeons.
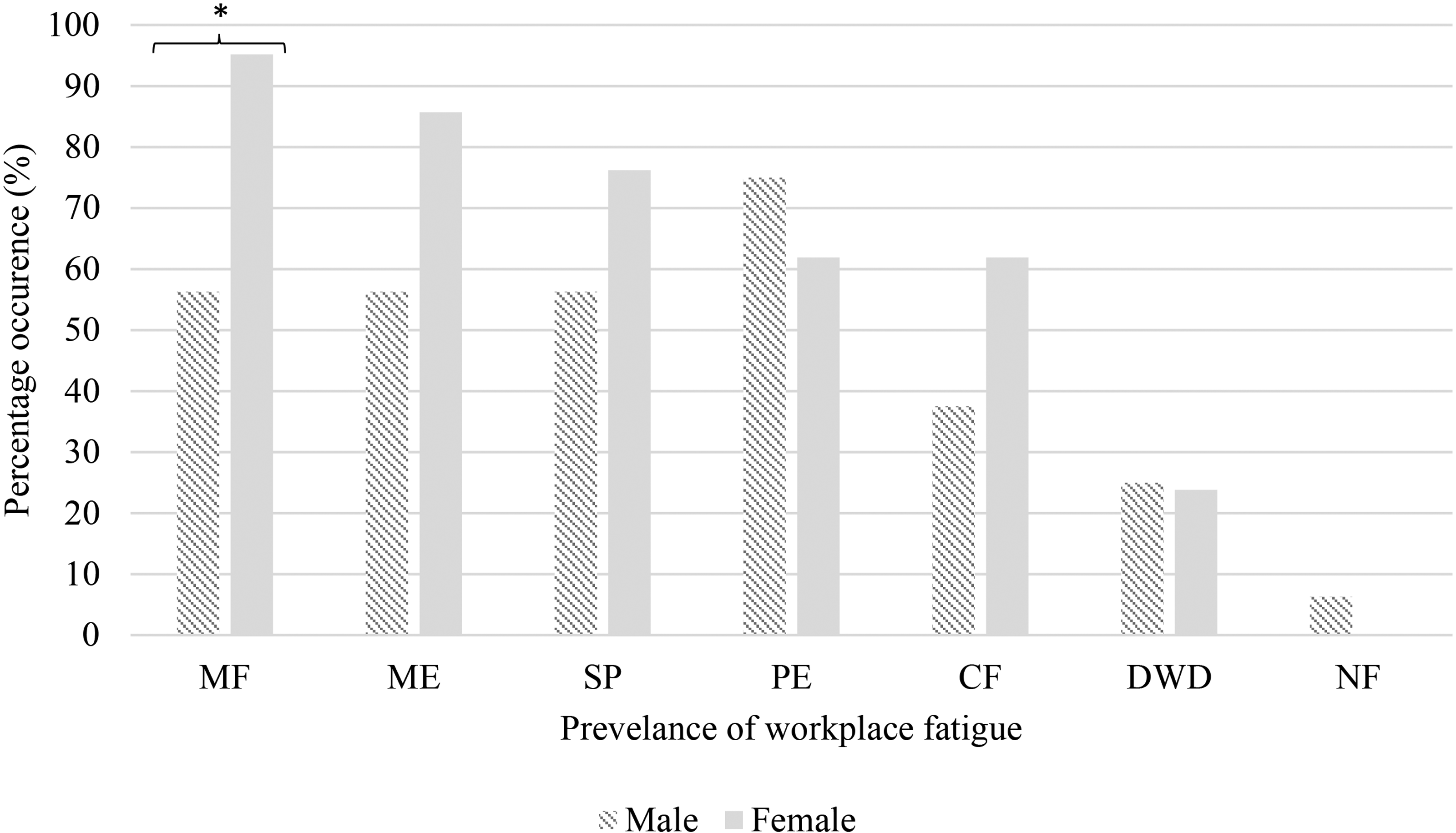
Prevalence of workplace fatigue split by gender in descending order for females (MF: musculoskeletal fatigue; ME: mental exhaustion; SD: sleep deprivation; PE: physical exhaustion; CF: compassion fatigue; DWD: drowsiness whilst driving; NF: no fatigue). *p = <0.05.
Demographic information of survey takers.
On average, 34 surgeons had at least 6–8 h of sleep per night, leaving three surgeons with at least 4–6 h of sleep. Tables 2 and 3 show the contributors to fatigue whilst performing surgery and the interventions to minimise these conditions at work and during surgery, respectively. For hours worked per week, three surgeons worked 30–40 h, 14 worked 40–50 h, 15 worked 50–60 h and five worked 60 + h. Sleep per night and hours worked per week were homogenous for male and female surgeons.
Contributors of existing fatigue at work/whilst performing surgery were categorised by gender in descending order for females.
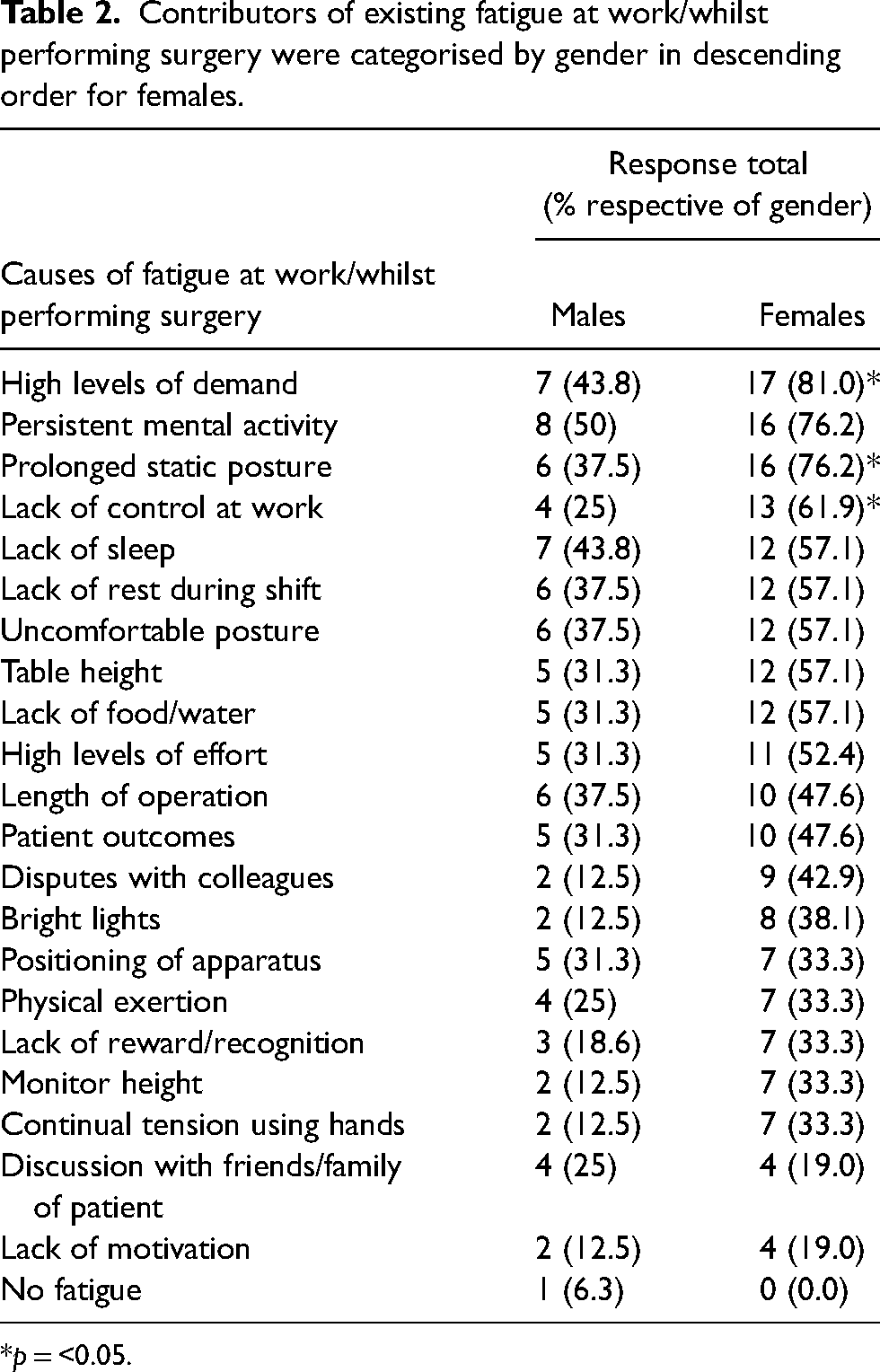
*p = <0.05.
Interventions to minimise fatigue at work/during surgery categorised by gender, in descending order for females.
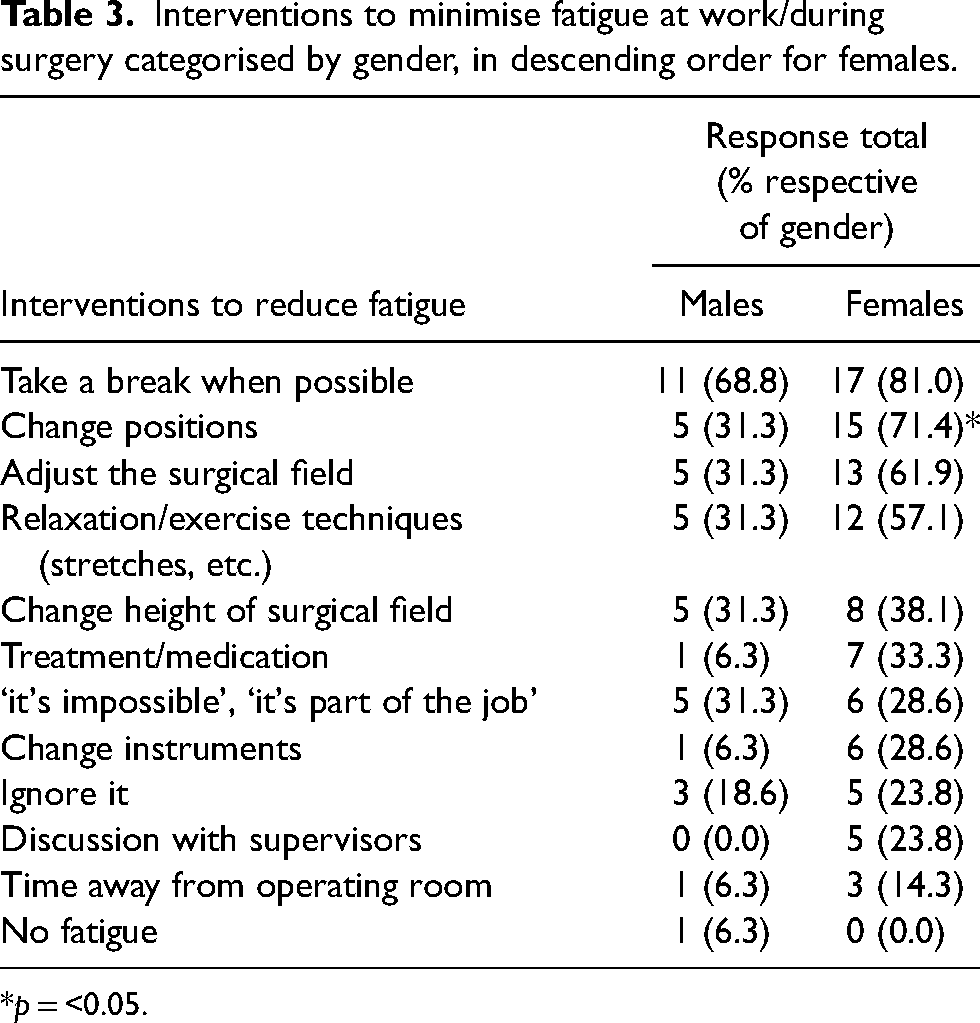
*p = <0.05.
Seventeen surgeons agreed that microbreaks may be a possible intervention to reduce fatigue during surgery. Surgeons were asked whether they were aware of any intervention strategies to mitigate workplace fatigue. Twenty were not aware, nine were aware of interventions but do not use them and one did not need to use them as they were not subject to fatigue. The rest used interventions such as taking rests, yoga, mindfulness activities and disconnecting from work where possible.
Females were statistically more likely to be suffering from a musculoskeletal injury (95% vs. 56%, χ2 (1, N = 37) = 8.15, p = 0.012) and though not statistically significant, mental exhaustion (86% vs. 56%, χ2 (1, N = 37) = 4.00, p = 0.067) in the workplace (Figure 1). Females were significantly more likely to allocate their fatigue to prolonged static postures (76% vs. 38%, χ2 (1, N = 37) = 5.64, p = 0.018), perceived lack of control on allocated tasks during the shift (62% vs. 25%, χ2 (1, N = 37) = 4.98, p = 0.026) and high levels of demanding work (81% vs. 44%, χ2 (1, N = 37) = 5.52, p = 0.019) (Table 2). To minimise fatigue, females were significantly more likely to change positions during their shifts (71% vs. 31%, χ2 (1, N = 37) = 5.90, p = 0.015) (Table 3). Females were more likely to discuss with supervisors over their level of workplace fatigue (28% vs. 0%, χ2 (1, N = 37) = 4.41, p = 0.057). All other fatigue contributors, causes of fatigue and interventions were homogenous across our sample.
We asked the surgeons their thoughts on wearing a base-layer vest capable of monitoring their fatigue levels during their shifts. We found 15 surgeons were inclined to wear the vest, whilst 17 are either hesitant or would need more information. The remaining surgeons would not wear the vest. Finally, we asked if surgeons found themselves fatigued after a shift, whether it would influence their decision to drive home, to which we found 21 would drive straight home, eight would take a break/nap before driving home and five are aware they should not drive, however, have errands to run.
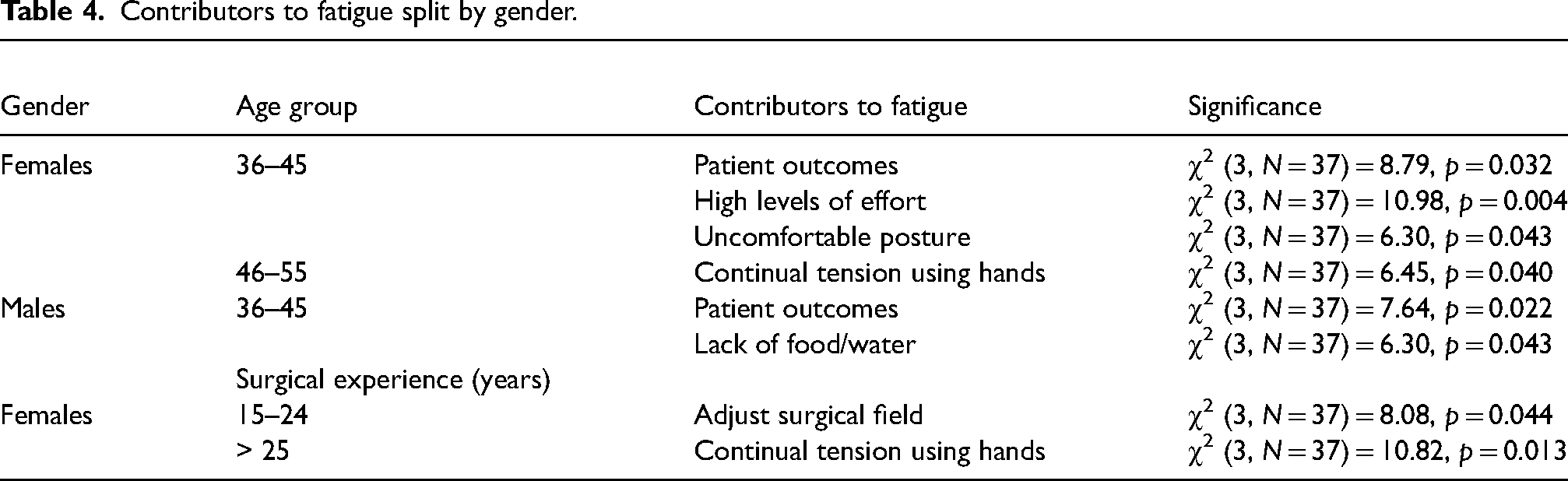
When participants were split by gender, χ2 analysis identified significant differences in the contributors and interventions for workplace fatigue amongst age groups and surgical experience (Tables 3 to 5). Additionally, males who reported the presence of musculoskeletal injuries in the workplace were significantly more likely to adopt microbreak practices and wear a vest on shift capable of monitoring fatigue levels (χ2 (3, N = 37) = 16.00, p = 0.007, χ2 (3, N = 37) = 6.79, p = 0.034, respectively). There were no significant differences between genders for hours of sleep or driver fatigue.
Contributors to fatigue split by gender.
Interventions to mitigate fatigue split by gender and age group.

Discussion
This questionnaire shows the prevalence of fatigue derived from the workplace, with 36 surgeons suffering from at least one contributor to fatigue. Only five surgeons suffered from one fatigue contributor whilst the rest suffered from two or more contributors to fatigue (see Figure 1). Overall, there were 23 separate contributors to fatigue at work or whilst performing surgery. This vast amount of variables suggests how widespread workplace fatigue can be.
Interestingly enough, some surgeons commented that it was not performing surgery that prompts fatigue, but other aspects of the job. Many of the factors in Table 2, such as persistent mental activity, high levels of demand, and prolonged static postures are inevitable, uncontrollable and a consequence of the surgical profession. Similar to previous findings, physical exertion is not highly recognised as a main contributor to fatigue for the majority of surgeons, however, it is still prevalent (Figure 1). 17 Additionally, those who suffer from compassion fatigue are at greater risk of reduced quality of life when combined with other contributors of fatigue. 3 Mitigating these factors is difficult without the incorporation of adequate rest periods to allow the opportunity for recuperation. Table 3 shows interventions to reduce fatigue, which includes taking breaks when possible at the top. From the evidence we can deduce that surgeons are simply not getting adequate rest periods in their shifts in order to help alleviate mental exhaustion. While some types of fatigue, such as musculoskeletal fatigue, may be mitigated rather easily with interventions such as room rearrangement, mitigating other types of fatigue, such as mental exhaustion, require a significantly greater time and resource investment.
Females more commonly reported the presence of musculoskeletal fatigue than males. This seemingly develops from prolonged static postures, which require changing positions at a greater frequency than males. This finding may identify that the operating theatre is more suitably designed for the male stature. Females may benefit greatly from the use of microbreaks when compared to males and future research should look at the gender differences of intra-operative fatigue.
Similarly, females were more likely to suffer from mental exhaustion than males, which could be attributed to higher levels of perceived demand and lower levels of control over their workload in the workplace. This finding may coincide with previous literature and the negative work–life balance which females more frequently experience.15,18 Considering that only half of the surgical cohort answered the questionnaire, this result should be analysed cautiously. However, whilst only a proportion of females would discuss their levels of fatigue with supervisors, there is evidence that significant stigma is attached to fatigue and thus reluctance to discuss fatigue with supervisors. It is previously addressed that males perceive to have more consistent leadership support than females, expressing concern that there may be gender bias encountered in the workplace, or inadequate support for females and their negative work–life balance. 18 Nevertheless 97% of our cohort suffer from fatigue however 16% discuss fatigue with their supervisors. Evidence to explain why surgeons do not adopt intervention strategies is limited. One previously identified reason may be the ‘feeling of invincibility’ which can be accounted for by 30% saying ‘it's part of the job’ to encounter fatigue (Table 3). 8 Whilst it is understandable that rigorous training prepares surgeons for complex shifts, complex patient interactions and quick decision making, workplace fatigue can easily cause sleepiness and impaired judgement, which if ignored, leads to compromised patient safety.
Our female surgical population has a greater amount of contributors to fatigue than males (Tables 2 and 4). When split by age group, females aged 36–55 had significantly more contributors to fatigue than other age groups. Similarly, surgical experience over 15 years for females had the same outcome. It was hypothesised that younger surgeons would be more susceptible to fatigue, however, the opposite is identified in this study. There may be underlying conditions that effect the longevity of surgical careers, such as long hours with inadequate rest over a sustained period of time. 2 Females reported continual tension using their hands and uncomfortable postures at work as contributors to fatigue, which were not apparent in male surgeons. Further research should identify whether the surgical equipment and operating room are adequately suitable for females to reduce the contributors to physical fatigue over time.
Male surgeons aged 36–45 contributed ongoing fatigue to a lack of food/water on shift. Figure 1 identifies an increased likelihood of physical exhaustion in males which may be a direct result of a lack of food and/or water on the shift, however, it is not known why only this age group contributes fatigue to a lack of food/water. Male and female surgeons aged 36–45 were both significantly more likely to associate fatigue with patient outcomes. It is not known what specific responsibilities the surgeons in this age category are accountable for, there may be more compassion fatigue associated with the job role, responsibilities and experience of surgeons in this age group when compared to other age groups.
Following on, female surgeons aged 36–55 were significantly more likely to mitigate their fatigue symptoms by changing positions during the shift (Table 5). Female surgeons aged 36–45 adjust the surgical field and adopt relaxation techniques. As aforementioned, the ergonomics of the operating theatre may play more suitably to the strengths of male surgeons. Though not significant, females more commonly reported adjusting the table and monitoring height. Thus, it may be important to adjust the surgical field in the pre-operative set-up so that it could reduce the uncomfortable posture associated with 57% of the female cohort when operating.
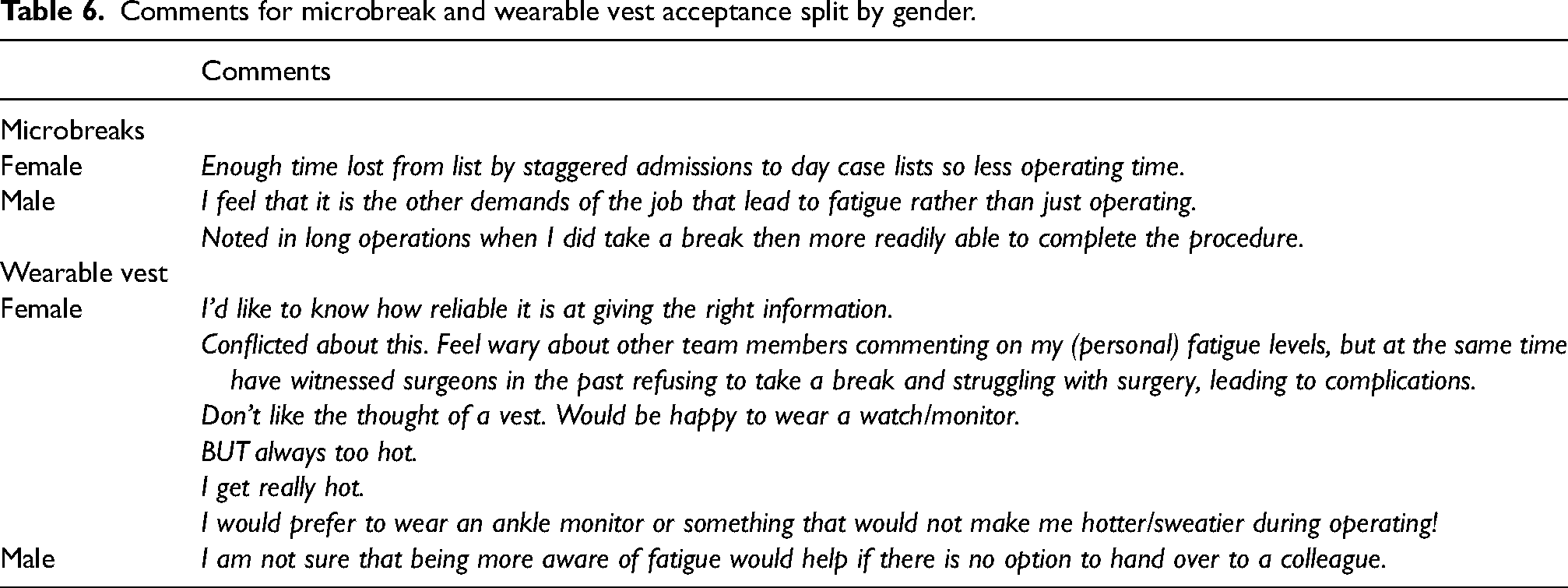
Whilst female surgeons had a greater amount of contributors and interventions to mitigate fatigue in the workplace, males currently suffering from musculoskeletal injury were significantly more likely to adopt microbreak practices and wear a vest capable of monitoring fatigue levels at work, showing promise for the market of wearable technology in the future. Surgeons had the option to write comments for microbreaks and base-layer technology (Table 6). When wearable vest acceptance was split by gender, it is clear to see there are more concerns for females wearing the vest than males, regarding temperature in the workplace. For microbreaks, one male participant demonstrated knowledge of the benefits of adopting them, however, one female participant suggested there is not enough time to adopt them due to staggered admissions. As such, more research is required into the gender differences of user acceptability for the possible widespread application of microbreaks and wearable technology in the workplace.
Comments for microbreak and wearable vest acceptance split by gender.
In order to mitigate the onset of fatigue, acknowledgement of these gender differences in fatigue are critical to reducing the statistical likelihood of fatigue onset in both genders. 19 Making fatigue challenges overt through support programmes may help strategize shift patterns and improve work–life balance to reduce the onset of preventable errors made in the workplace to improve patient safety.
There are limitations to this research analysis. Firstly, we can only base our research on the sample of data we have collected. The questionnaire has 22 partial completions. Surgeons who are currently suffering from fatigue may have an increased likelihood to respond to the questionnaire resulting in bias.
Conclusion
Our findings indicate a substantial prevalence of gender-based differences in fatigue in the workplace for surgeons, as well as the key contributors to fatigue. The study identified an increase in the prevalence of mental exhaustion and musculoskeletal fatigue in females, possibly due to a perceived lack of control over workload, high levels of demanding work and prolonged static postures at work. Our findings indicate that workplace fatigue is prevalent across all demographics and mitigating fatigue from the start of surgical careers could help reduce the onset of drivers of fatigue, such as musculoskeletal injuries, mental exhaustion and time missed from work as a result of workplace fatigue. Future studies may consider why females are reporting higher levels of demanding work and lower levels of perceived control over work, as this may directly impact the level of mental exhaustion felt by so many female surgeons.
Supplemental Material
sj-doc-1-cri-10.1177_25160435231185389 - Supplemental material for Gender differences of fatigue in the workplace for surgeons
Supplemental material, sj-doc-1-cri-10.1177_25160435231185389 for Gender differences of fatigue in the workplace for surgeons by Jacob Thomas Merriman, James E Humphries, Roberto Ferrero and Iain Hennessey in Journal of Patient Safety and Risk Management
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported financially by Engineering and Physical Sciences Research Council (grant number EP/S515504/1).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.