
Abstract
Background
Prescribing errors are common, occurring in 7% of in-patient medication orders in UK hospitals. Foundation Year 1 (F1) doctors have reported a lack of feedback on prescribing as a cause of errors.
Aim
To evaluate the effect of implementing a shared learning intervention to Foundation Year 1 doctors on their prescribing errors.
Methods
A shared learning intervention, ‘good prescribing tip’ emails, were designed and sent fortnightly to F1s to share feedback about common/serious prescribing errors occurring in the hospital. Ward pharmacists identified prescribing errors in newly prescribed in-patient and discharge medication orders for 2 weeks pre- and post-intervention during Winter/Spring 2017. The prevalence of prescribing errors was compared pre- and post-intervention using statistical analysis.
Results
Overall, there was a statistically significant reduction (p < 0.05) in the prescribing error rate between pre-intervention (441 errors in 6190 prescriptions, 7.1%) and post-intervention (245 errors in 4866 prescriptions, 5.0%). When data were analysed by ward type there was a statistically significant reduction in the prescribing error rate on medical wards (6.8% to 4.5%) and on surgical wards (8.4% to 6.2%).
Conclusions
It is possible to design and implement a shared learning intervention, the ‘good prescribing tip’ email. Findings suggest that this intervention contributed to a reduction in the prevalence of prescribing errors across all wards, thereby improving patient safety.
Introduction
Patient safety is a priority for the NHS and healthcare systems worldwide. 1 Reducing medication errors is a key improvement required for the NHS and to meet this challenge healthcare professionals must identify and implement changes to their practice. 2
Medication incidents are the fourth most reported type of incident reported to NHS improvement. 3 Prescribing errors are common in UK hospitals, occurring in 7% of in-patient prescriptions, 4 and causing harm in ∼1% of in-patients. 5 A common theme in studies of doctors' attitudes towards error causation is receiving insufficient feedback about their prescribing which creates a barrier to learning and changing prescribing behaviours.6–9 A large, multi-centre investigation into the causes of junior doctors prescribing errors (EQUIP study) recommended that trainees receive effective feedback on their prescribing performance and that interventions to improve prescribing practice and patient safety should be explored. 6
Audit and feedback has been extensively investigated as a tool to improve healthcare professionals' behaviour and patient outcomes.10,11 However, published data exploring the effect of feedback interventions on prescribing error rates in UK hospitals describe complex interventions combining pharmacist-led feedback with one or more additional educational strategies.11–18 Methodological differences make it difficult to compare studies and draw robust conclusions about the efficacy of interventions.
Research has shown that junior doctors have a high opportunity for error due to their large volume of prescribing. 6 In the UK, improving feedback to junior doctors about prescribing practice has been recommended to improve their awareness about prescribing errors and reduce patient safety incidents. 6 It was considered that, as recent graduates, Foundation Year 1 (F1) doctors were likely to have different educational needs than more experienced prescribers. F1 doctors are medical graduates who have entered the first year of the Foundation Programme, a 2-year generic training for junior doctors. Therefore, it was decided to investigate the impact of a shared learning intervention on this grade of doctor.
The study hospital has a good culture of reporting medication incidents.19,20 However, in agreement with findings from the EQUIP study, hospital stakeholders identified a need to improve the way that feedback about prescribing errors was shared with prescribers. Shared learning is an important mechanism to spread health-service improvements. 21 Therefore, the research question was ‘can a shared learning intervention (the prescribing tip email) help reduce prescribing errors?’
The objectives of this study were (1) to develop a shared learning intervention (the prescribing tip email); (2) To send the prescribing tip email to all F1 doctors; (3) to compare prescribing error prevalence pre- and post-intervention.
Methods
The study design was a single site before, and after study. It was conducted at an NHS teaching hospital with 669 in-patient beds, operating a typical UK clinical pharmacy service. This service involved pharmacists visiting wards for 2–6 h on weekdays, reviewing all prescriptions and if necessary contacting the prescriber directly, or via an intervention note to clarify any ambiguities and correct any errors of omission or commission. All medical and surgical wards (10 medical, 6 surgical) at the in-patient hospital site were studied. These were chosen to allow representation of different individuals working environments and prescribing contexts, as these factors are associated with prescribing errors. 22 Paper prescription charts are used for in-patient prescribing, and discharge prescriptions are computerised.
At the time of the study, the junior medical workforce included 27 F1 doctors and 28 F2 doctors. Interventions already in-place which incorporated feedback on prescribing errors included three hours of scheduled education a week based on the Better Training Better Care programme pilot, and the SCRIPT safer prescribing e-learning programme.23,24 Ward based pharmacists also provided verbal and written feedback, using an ‘intervention note’ in the day-to-day course of delivering hospital pharmacy services.
The intervention
The shared learning intervention used in this study was a ‘good prescribing tip’ email (Figure 1) which is a validated group feedback intervention.11,25,26 Although previous work did not show a significant reduction in prescribing error rates, qualitative findings suggested improvements in doctors' engagement with safe prescribing. 11 Furthermore, the intervention is designed to support prescribers meet the Royal Pharmaceutical Society Prescribing Competency Framework. 27 Therefore, it was decided to investigate the impact of this intervention in our hospital.
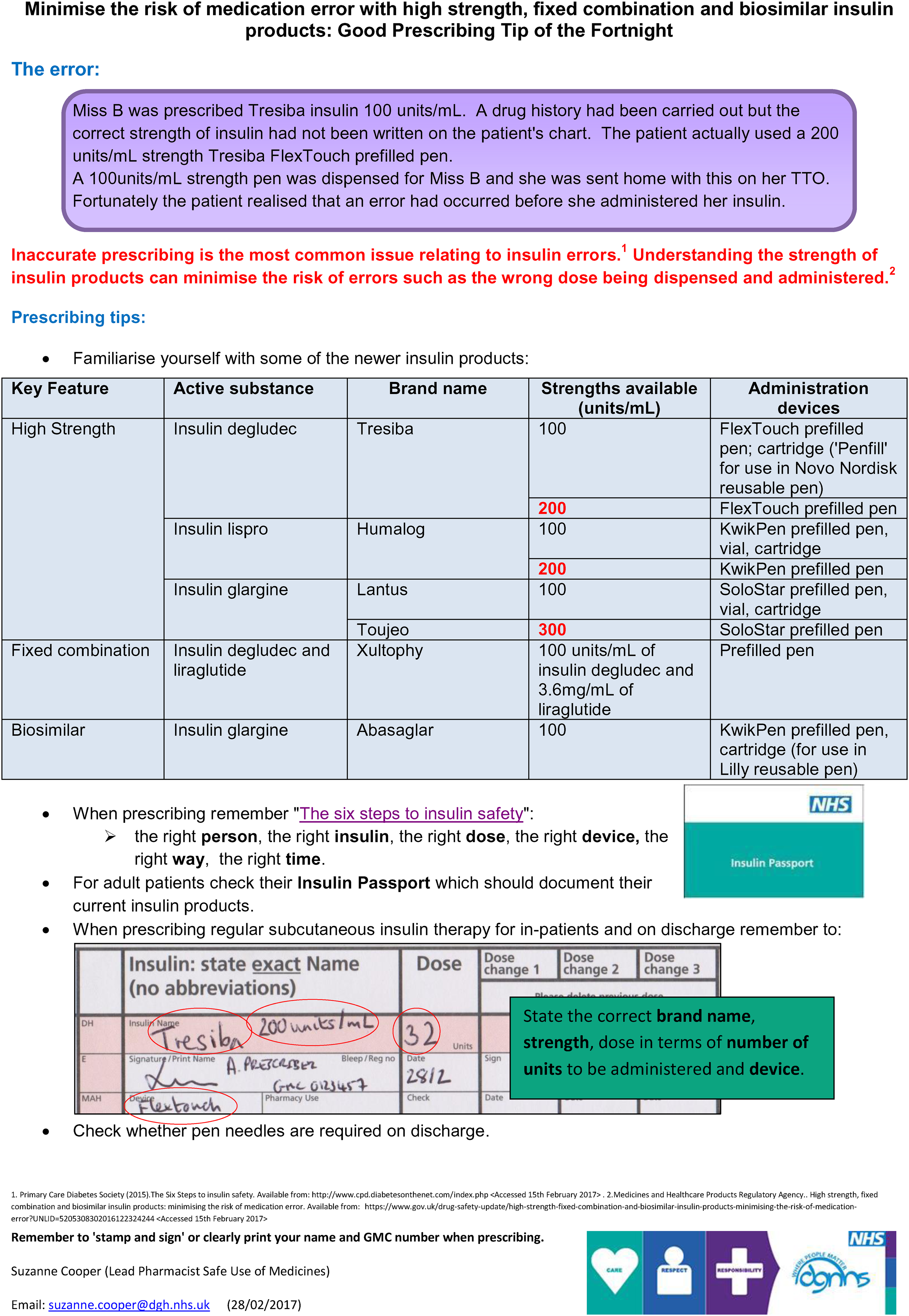
Example of good prescribing tip for insulin.
The prescribing tip email was developed by SMC based on designs in the literature. The content was informed by local and national error reporting, the hospital medication safety group, and ward pharmacists feedback. One prescribing tip was emailed fortnightly to all F1 doctors, starting immediately after baseline data collection (see data collection section) for a total of 8 weeks. The four prescribing tips covered were medicines reconciliation, Inhaler strengths and devices, Insulin prescribing and ambiguous frequencies. To improve awareness of the intervention a reminder was given by the study lead (SMC) and Foundation Education Lead. Doctors continued to receive ‘standard feedback’ provision; defined as ‘feedback on prescribing errors delivered via any mechanism other than the intervention’ e.g., existing education and training programmes and clinical pharmacist feedback.
Data collection
Data collection followed a prospective, process-based approach, which is the most frequently used method for prescribing error prevalence studies. Prescribing errors were identified by ward pharmacists in all newly prescribed medication on in-patient prescription charts and discharge prescriptions as part of their routine pharmacy ward visit. This study used a practitioner-led definition 28 of a prescribing error which has been widely used.4,29 According to this definition a clinically meaningful prescribing error occurs when, as a result of a prescribing decision or prescription-writing process, there is an unintentional, significant reduction in the probability of treatment being timely and effective or increase in the risk of harm, when compared with generally accepted practice.
For the purposes of this study, pharmacists recorded the number of prescriptions reviewed, the number of prescribing errors, and the number of omitted medications on a standard form provided by the researchers. Any prescriptions previously reviewed by a pharmacist were excluded. Doctors were aware of data collection but were not informed of study dates. This method of detection was adapted from a large, well-designed prevalence study 4 and is similar to that used in other work.11,30
A pilot study was conducted to establish that this methodology was feasible prior to ‘full-scale’ data collection. A verbal briefing and a written copy of study definitions were provided for pharmacists before each data collection period by SMC.
Prescribing incident reports at the study hospital usually show a temporary increase during doctors’ first rotation of the academic year (August–November). Therefore, this study was conducted over 12 weeks during doctors' second rotation to minimise the potential confounding effect of this factor. Baseline data was collected for 2 weeks in all study wards immediately before (16–27 January 2017) and after (20–31 March 2017) the intervention period. Collection occurred Monday to Friday during pharmacists' day shifts; but included any medication prescribed over the weekend.
Outcome measures
The outcome measure used in this study was the prescribing error rate.
Sample size
Prescribing errors are reported to occur in 7% of prescriptions. 4 An error reduction from 7% to 5% required sample size of 2300 prescriptions in both the pre- and post-intervention periods to give 80% power and a 95% confidence interval. This equates to just over 70 prescriptions to be reviewed per week per ward for each 2-week data collection period which was considered feasible. 31
Data analysis
The prescribing error rate was calculated as a percentage of all opportunities for error, 32 using the number of newly prescribed in-patient and discharge prescriptions screened by ward pharmacists as the denominator. This denominator has been used in previous studies and allowed the comparison of findings. 11
Chi-square analysis was undertaken using an online calculator (www.socscistatistics.com) with a Yates correction applied. A significant reduction in prescribing error rate due to the intervention was defined as a p-value <0.05 at the 95% confidence interval.
Results
Pre-intervention, a total of 441 prescribing errors were identified in 6190 prescriptions across all wards (7.1%). Post-intervention, 245 errors were identified in 4866 prescriptions (5%) (Table 1). Chi-square analysis showed this change was statistically significant (p < 0.05) even after applying the Yates correction.
Error rates pre- and post-intervention.
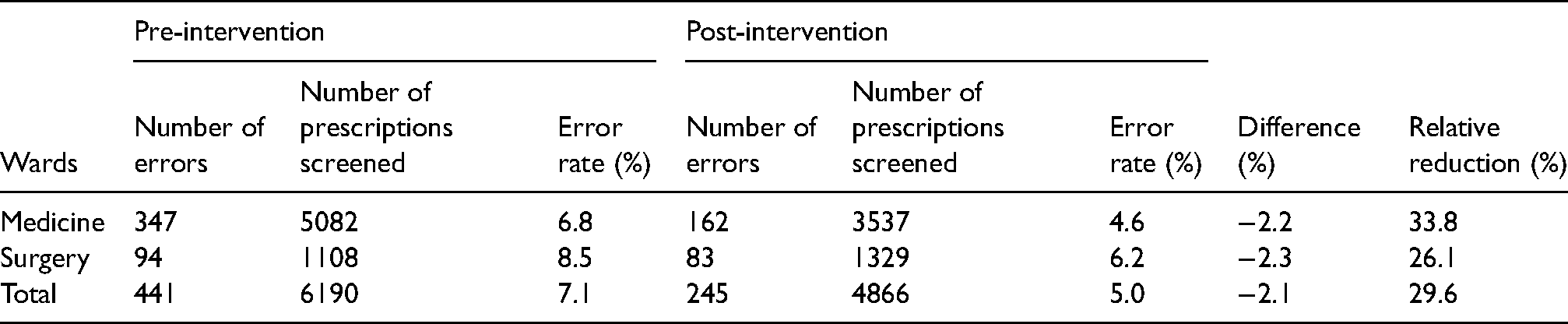
Analysis of the data by ward type indicated a difference in error rates between Medicine and Surgery but in both, there was a statistically significant reduction following the intervention (Table 1). In medical wards, 347 prescribing errors were identified in 5082 prescriptions pre-intervention (6.8%), and post-intervention 162 errors were identified in 3537 prescriptions (4.6%). This reduction was statistically significant (p < 0.05 chi-square analysis). On surgical wards, 94 prescribing errors were identified in 1108 prescriptions pre-intervention (8.5%), and post-intervention 83 errors were identified in 1329 prescriptions (6.2%). This reduction was also statistically significant (p < 0.05 chi-square analysis).
Discussion
The study achieved its aim and objectives to design and evaluate the effects of implementing a shared learning intervention for F1 doctors to reduce prescribing errors.
Overall there was a statistically significant reduction in prescribing error rates after the implementation of the shared learning intervention (Table 1). Prescribing error prevalence pre-intervention was in line with error rates reported elsewhere in the UK.4,6
The difference in error rates between Medicine and Surgery may be accounted for by the higher volume of prescribing taking place on medical wards (Table 1). This is due to not only the prescribing of patients’ regular medicines, following hospital admission, but also the initiation of new medicines and changes to existing regimens as well as discharge medications. Surgical wards had a lower number of prescriptions not only because there were less wards but also there is less initiation of new medicines and changes to existing regimens. Previously published research suggests that error rates increase as the number of items prescribed increases. 33
Several studies have observed a reduction in prescribing error rates with feedback interventions.11–14 Webbe et al. 14 found that a ‘clinical pharmacist teaching programme’ reduced the total prescribing error rate in the active group compared to control by 37% (20% vs 12.5%, p = 0.14). In our study, there were similar relative reductions in error rates overall (Table 1). Gordon and Bose-Haiders' 12 ‘prescribing feedback system’ also significantly reduced the overall error rate (p < 0.0001) at baseline versus end of study.
Two studies of technical errors showed significant reductions.12,13 Lepee et al. 34 found that after using a ‘check and correct’ checklist there was a significant reduction of 5% in the rate of technical errors (7.1% to 2.9%, a 37.7% relative decrease; R2 = 0.604), whereas there was no significant effect on clinical errors (p = 0.53). Thomas et al. 13 also demonstrated that educational tutorials, ward-based teaching and feedback in three 3-monthly cycles significantly reduced the percentage of prescriptions with technical errors over each cycle.
Comparing findings with other studies is difficult because feedback is often used with other education and training approaches which are not clearly described. Studies are typically over a short duration at single sites further limiting generalisability. Reynolds et al. 11 who used the same intervention, definitions and denominator as this study, reported a non-significant reduction in the error rate of 4%, which is slightly higher than in our study, although our reductions did reach statistical significance.
The nature and causes of prescribing errors are multi-factorial,4,6,8 and the intervention described in this study addressed a limited number of common errors over a short timescale. Nonetheless, there was a statistically significant decrease in error rate overall and in both Medicine and Surgery. These decreases represent a relative risk reduction in prescribing errors overall of 29.5%, in Medicine 33.8% and in Surgery 26.1% (Table 1). It is likely that the observed reduction in prescribing errors was due to a combination of the positive effects of feedback on learning and prescribing behaviours, education and training, and doctors’ gaining more prescribing experience, rather than the intervention alone. However, the results suggest the intervention is making a contribution to reducing prescribing errors.
Strengths and limitations
The strengths of this study were that sample sizes were sufficiently statistically powered and validated definitions were used; meaning that conclusions about the impact of the intervention are likely to be more reliable. Furthermore, the intervention itself was relatively easy and inexpensive to implement, which means it could easily be replicated in other hospitals.
Several limitations were identified. This was an uncontrolled study which explored the impact of the intervention on error prevalence only. The before-after design and multiple confounding variables affecting prescribing error causes and prevalence mean that it is difficult to attribute the reduction in errors to the intervention alone. Furthermore, other similar studies have suggested that there is likely to be a variation in pharmacists’ ability to detect errors, adhere to study definitions, and consistency in reporting data. However, we attempted to minimise this through a verbal briefing and provision of a written copy of study definitions.
Finally, the study was conducted at a single site with a small sample of doctors over a short duration which may limit the strength of findings and generalisability.
Variation between individual wards was not calculated due to insufficient sample size per ward to draw a robust conclusion, but it was possible to analyse the data by different ward types (e.g. Medicine and Surgery).
Recommendations
Prescribing tips should be used contemporaneously with existing education and training approaches to deliver shared learning about prescribing errors.
As suggested in previous work a standardised definition and methodology should be used for quantitative studies of prescribing error rates in hospitals to facilitate comparison of findings.
Qualitative studies are required to gain a more in-depth understanding of junior doctors’ attitudes towards feedback and shared learning to prevent errors and improve patient safety.
Conclusions
It is possible to design and implement a shared learning intervention, the ‘good prescribing tip’ email. The intervention was relatively easy and inexpensive to implement. There was a statistically significant reduction in error rate after the intervention, but as this was an uncontrolled study and other feedback systems were in place the error reduction cannot be attributed solely to the intervention.
Authors’ contributions
All authors have contributed to this study and all authors reviewed and approved the final version of the manuscript. SMC designed the study, interpreted the results and reviewed the manuscript and corrected the final version of the manuscript. RWF participated in the study design, interpreted the results and reviewed the manuscript and corrected the final version of the manuscript. RWF is the guarantor for the work and controlled the decision to publish.
Footnotes
Acknowledgements
The authors thank all the staff particularly those in the pharmacy department at the hospital where this study was carried out for their cooperation in undertaking this work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
As this work was a service evaluation project it did not require NHS ethics approval.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.