
Abstract
Background:
Facial masks are essential for preventing respiratory infections, particularly among healthcare workers. However, prolonged mask use may lead to ocular surface disruption, known as mask-associated dry eye (MADE).
Objectives:
To evaluate the impact of different types of disposable surgical masks on tear film parameters and corneal wavefront aberrations during an 8-h work shift.
Design:
Randomized clinical trial.
Methods:
Sixty healthcare personnel at Rajavithi Hospital were randomly assigned to three mask groups: Group 1 (earloop surgical mask; Medimask®), Group 2 (earloop surgical mask with adhesive nose strip), and Group 3 (anti-fog earloop surgical mask; Welcare 3D Blue Line Anti-Fog Mask®). Non-invasive tear breakup time (NIBUT), tear meniscus height (TMH), and conjunctival redness were assessed using the Oculus Keratograph®5M. Corneal higher-order aberrations (HOAs) were measured using the GALILEI Dual Scheimpflug Analyzer before and after 8 h of mask wear.
Results:
TMH decreased significantly in all groups: Group 1 from 201.13 ± 85.10 µm to 174.53 ± 42.01 µm (p = 0.003), Group 2 from 188.81 ± 59.55 µm to 164.61 ± 50.58 µm (p = 0.036), and Group 3 from 194.50 ± 58.29 µm to 166.25 ± 45.90 µm (p = 0.034). NIBUT showed slight, non-significant decreases: Group 1 (9.26 ± 4.47–8.35 ± 3.26 s), Group 2 (8.88 ± 3.79–8.20 ± 3.12 s), and Group 3 (9.14 ± 4.20–8.55 ± 3.74 s). Conjunctival redness increased significantly only in Group 1 (1.75 ± 0.47–1.98 ± 0.52, p = 0.048). HOAs were mostly unchanged, except for total HOAs at the 6 mm zone, which were higher in Group 3 (1.85 ± 1.20) than in Group 1 (1.14 ± 0.48) and Group 2 (1.28 ± 0.58; p = 0.012).
Conclusion:
An 8-h shift of mask use reduced TMH across all groups and increased conjunctival redness in earloop surgical masks without adhesive. Although most optical aberrations remained unchanged, elevated HOAs in the anti-fog earloop surgical mask group may affect vision quality under mesopic conditions.
Thai Clinical Trials Registry:
TCTR 20230725002 (https://www.thaiclinicaltrials.org/show/TCTR20230725002).
Keywords
Introduction
As widely acknowledged, the deployment of facial masks, including both medical-grade and non-medical variants, assumes a pivotal role in mitigating the transmission of respiratory infectious diseases.1,2 In 2020, the global landscape experienced the onset of the COVID-19 outbreak, leading the World Health Organization (WHO) to declare it a pandemic and recommend the adoption of mask-wearing as a preventive measure. 3 The WHO recommends the use of masks in various scenarios: in crowded settings for individuals with suspected or confirmed COVID-19; and when sharing spaces with others, especially those displaying symptoms or testing positive for COVID-19. 4 The recommended masks for the general public include disposable medical masks, non-medical masks meeting safety and efficacy standards that are washable for reuse, and other well-fitting non-medical options in accordance with local policies. 4 Despite a reduction in the use of protective measures for the general public due to the improvement in the COVID-19 situation, distinctions in protocols should persist for medical personnel during work, and some studies have provided compelling evidence supporting the use of face masks to prevent the transmission of respiratory virus diseases in hospital settings.5 –7 Research indicates that wearing masks is correlated with a reduction in viral infectious episodes among healthcare workers compared to instances of no mask use.5 –7 Therefore, it remains imperative for healthcare professionals to consistently employ medical masks in their daily work in order to effectively mitigate the transmission of respiratory infections.
The act of wearing facial masks has presented a variety of challenges, with ocular health emerging as a significant concern. 8 The phenomenon of mask-associated dry eye (MADE) has gained notable attention, especially as individuals in various settings continue to wear masks for extended durations.9,10 The potential explanation for this condition involves a complex interplay of factors, notably altered airflow patterns and increased air turbulence around the eyes, particularly from the top edge of the mask. These elements collectively disrupt the natural dynamics of the tear film, leading to heightened tear evaporation and exacerbation of ocular dryness, thereby causing irritation of the ocular surface.11,12
Few studies have investigated the impact on MADE of taping the top edge of masks.13,14 Sridevi Nair et al. 13 and Yuichi Hori et al. 14 both reported significant enhancements in ocular surface stability following the application of tape to the top edge of masks compared to non-taping conditions. However, the application of adhesive products carries the potential for causing skin damage. 15 A primary concern associated with taping is skin stripping. Additionally, although less common, other types of skin issues may arise, including tension blisters, irritant contact dermatitis, allergic contact dermatitis, folliculitis, and maceration.15,16 Skin stripping refers to a condition where the outermost layer of the skin, known as the epidermis, is partially removed or damaged. This occurs frequently when adhesive products, such as tapes or bandages, are repetitively applied and removed from the same skin area. 17 It is important to note that regular use of adhesive tape to cover the top edge of a mask in order to reduce MADE may contribute to these skin problems.
To prevent the disturbance caused by air turbulence escaping from the upper edge of the mask without taping the top edge of masks, various innovative mask designs have emerged.18,19 One example is the Nose Bridge Design, 20 featuring a moldable nose bridge that allows users to shape the mask for a secure fit over their noses. Additionally, masks with built-in vents or ventilation systems 21 are available to reduce the amount of warm air escaping upward. Another solution involves masks designed with extra specialized layers made from moisture-wicking material to improve sealing properties.22,23 These masks are also considered anti-fog for glasses wearers because they obstruct airflow from the top edge of the mask through the glasses.
The objective of our present study was to examine the impact of three distinct types of commonly used disposable surgical masks, each employing different mechanisms to prevent airflow from the top edge of the mask. These include earloop surgical masks, earloop surgical masks with adhesive nose strips, and anti-fog earloop surgical masks. Our investigation specifically focused on evaluating their effects on ocular surface parameters, including tear film characteristics and wavefront attributes.
Material and methods
The study protocol followed the ethical guidelines regarding human subjects given by the Declaration of Helsinki and was approved by the Ethics Committee of Rajavithi Hospital (Number 66068) on June 15, 2023, and the study was performed between August and November 2023. All participants provided written informed consent prior to enrollment in the study. The trial was registered in the Thai Clinical Trials Registry under the code TCTR 20230725002, registered on July 19, 2023 (https://www.thaiclinicaltrials.org/show/TCTR20230725002). This manuscript was prepared in accordance with the CONSORT 2025 guidelines to ensure transparent and standardized reporting of the clinical trial.
This was a randomized, parallel-group, superiority trial with an allocation ratio of 1:1:1 designed to compare the effects of three different types of surgical masks on ocular surface parameters. The study framework was to evaluate whether one mask type was superior to others in preventing adverse ocular effects during prolonged use.
A total of 60 healthcare personnel employed in Rajavithi Hospital were recruited for this study, which was conducted in a hospital setting. Inclusion criteria comprised individuals who regularly used surgical masks during their work activities, while exclusion criteria were individuals with respiratory conditions or any contraindications to mask usage. Participants with mild ocular surface symptoms, including dry eye disease, were not excluded; however, no participants had other ocular diseases beyond dry eye disease. Demographic data were recorded for each participant as follows: age; gender; presence of underlying diseases; current refractive error correction (e.g., glasses, contact lenses, or previous refractive surgery); workplace environment (fan or air-conditioned); and use of artificial tears. Use of artificial tears and ocular symptoms were carefully documented. An overview of the study design, including participant flow, randomization, and outcome measurements, is illustrated in Figure 1. Participants were randomly assigned to one of the three mask type groups. Prior to mask usage, baseline data were collected, encompassing tear film parameters such as non-invasive tear breakup time (NIBUT), conjunctival redness, and tear meniscus height (TMH) measured using the Oculus Keratograph®5M (Oculus Arlington, WA, USA), along with wavefront parameters assessed by the GALILEI Dual Scheimpflug Analyzer (GSA). Measurements were repeated at the conclusion of the 8-h mask-wearing period. Although participants and personnel administering the interventions were aware of group allocation due to the visible nature of the surgical masks, outcome assessors were trained technicians who remained blinded to group assignments throughout the study. To reduce the risk of detection bias, all primary and secondary outcomes were based on objective measurements, including tear film parameters and wavefront data, obtained using standardized equipment and protocols. Data analysts were also blinded to the allocation to ensure unbiased statistical evaluation. Details of each mask type are summarized in Table 1, and illustrated in Figures 2–4. All participants received instructions on the proper method of wearing the assigned mask type and were directed to wear the designated face mask for the entire 8-h work shift, except during a 1-h break for lunch and brief intervals for drinking water. Additionally, participants were provided with a spare face mask with instructions in case they needed to change masks during the day. Randomization was performed using a web-based system by one of the researchers (ND) at Rajavithi Hospital, employing a block randomization method to ensure equal allocation into the three study groups. This approach ensured impartial group assignment and balanced baseline characteristics, including the use of artificial tears. The allocation sequence was concealed until the time of assignment and was implemented by trained staff at Rajavithi Hospital, who enrolled participants and assigned them to their respective groups. Following randomization, baseline characteristics were assessed and confirmed to be comparable across groups, including age, gender, systemic conditions, refractive correction methods, use of artificial tears, and work environment. Harms were not assessed systematically, as the intervention was considered minimal risk. Participants were advised to report any adverse effects experienced during the study period. No interim analysis was planned or conducted. No formal stopping guidelines were established for this trial; however, participants retained the right to withdraw from the study at any time without consequence. Supplemental material is available online.

Study flow diagram.
Details of mask types.
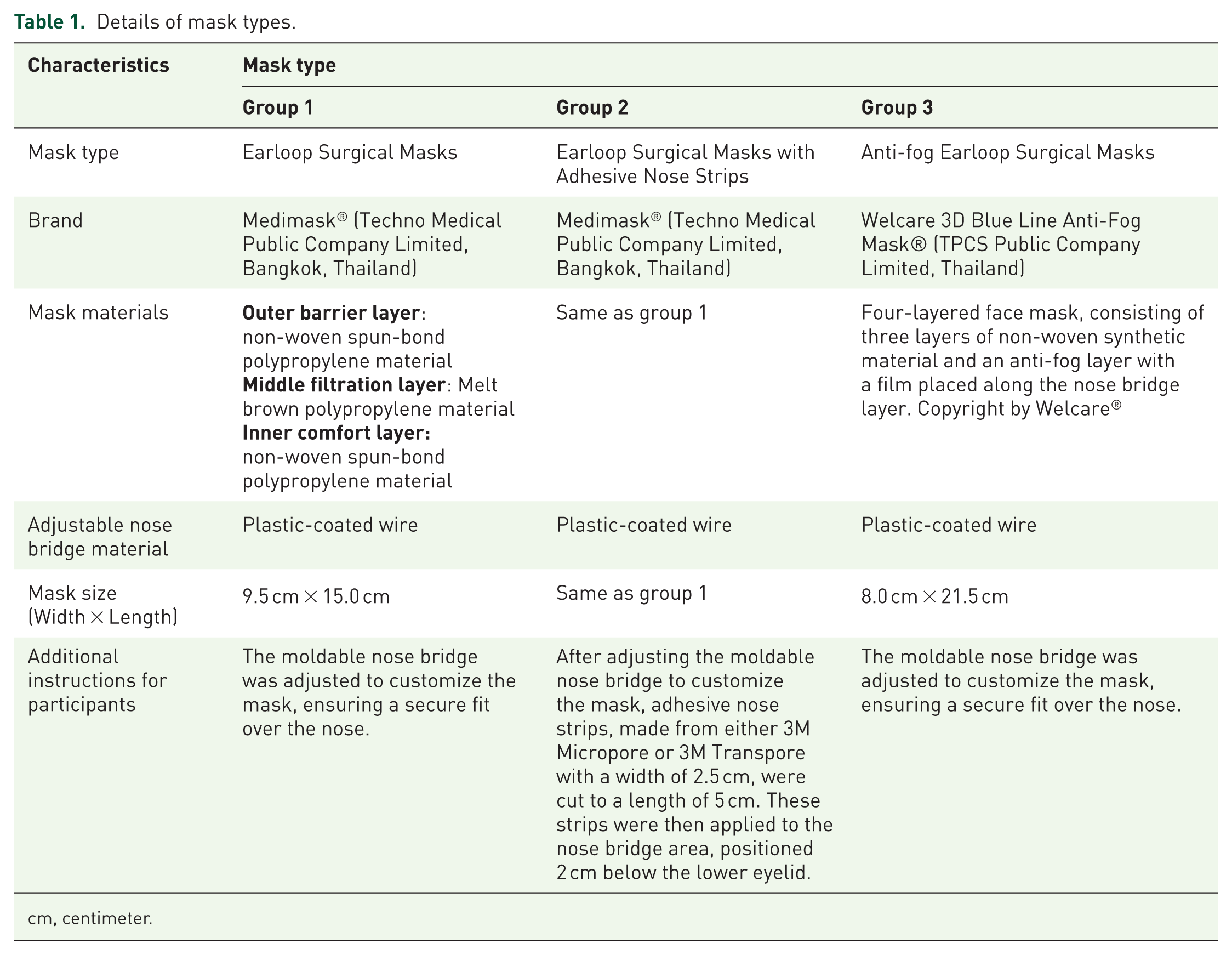
cm, centimeter.

Layered structure of a Medimask® face mask. The mask consists of three primary layers: The outer barrier layer (first layer) and the inner comfort layer (third layer) are made from non-woven spun-bonded polypropylene, offering structural support and protection to the filter layer. The middle filtration layer (second layer) is composed of melt-blown polypropylene, providing the mask’s essential filtration properties in accordance with the Thai Industrial Standards Institute. Additional components include an adjustable nose bridge made from plastic-coated wire to ensure a snug fit.

Structure of a Welcare 3D Blue Line Anti-Fog Mask®. The Welcare 3D Blue Line Anti-Fog Mask® consists of a four-layered construction. It comprises three layers of non-woven synthetic material and includes an anti-fog layer with a film positioned along the nose bridge. Copyright by Welcare®.

Different types of face masks used in the study. (a) Group 1: earloop surgical mask. (b) Group 2: earloop surgical mask with adhesive nose strips. (c) Group 3: Anti-fog earloop surgical mask.
Sample size calculation
The sample size was calculated to compare three groups using one-way analysis of variance (ANOVA). 24 Based on a previous study by Bilici S et al., 25 the average NIBUT at baseline was 11.4 s (SD 3.3), and after wearing a mask for 8 h, it decreased to 7.9 s (SD 3.6). Assuming an intermediate effect size (Cohen’s f) of approximately 0.41, with a significance level (α) of 0.05 and a statistical power of 80%, the estimated sample size was 19 participants per group. To account for potential dropouts, 20–23 participants per group were recruited, resulting in a total sample size of at least 60 participants.
Statistical methods
Descriptive statistics were used to summarize demographic characteristics, including mean and standard deviation for continuous variables and frequency and percentage for categorical variables. Normality of continuous data distribution was assessed using Shapiro–Wilk test. Comparisons of demographic characteristics between groups were performed using one-way ANOVA for continuous variables and chi-square test for categorical ones. For the analysis of tear film and corneal wavefront parameters, paired t-tests were conducted to compare measurements before and after the 8-h mask-wearing period within each group. In case of non-normally distributed data, Wilcoxon signed-rank tests were utilized. Post-hoc analyses such as Bonferroni correction were performed for multiple comparisons when appropriate. Statistical significance was set at p < 0.05. All statistical analyses were carried out using IBM Statistics for Windows, version V.22.0 (IBM Corp., Armonk, NY, USA).
Results
The demographic characteristics of the study participants are summarized in Table 2. All 60 participants who were randomized completed the study and were included in the final analysis. There were no losses to follow-up or exclusions after randomization in any of the three groups. No extended follow-up period was planned or conducted, as all outcomes were assessed immediately before and after the intervention within the same day. All participants adhered well to the assigned mask-wearing protocol, wearing the allocated masks continuously throughout the 8-h work shift except during scheduled breaks. Adherence was monitored through participant self-reports. No additional interventions were administered during the study period, and concomitant care, including the use of artificial tears.
Demographic data.

There were 54 (90.0%) females and 6 (10.0%) males, ranging in age from 18 to 61 years old. Analysis of age distribution revealed that the majority of participants were below the age of 30 years (68.3%), with smaller proportions across older age groups. In terms of underlying systemic diseases, 45 (75.0%) participants reported no underlying conditions, while 15 (25.0%) reported having some underlying systemic diseases. Refractive error was notably prevalent among the participants, with 41 (68.3%) individuals reporting its presence: 34 (56.7%) of these used glasses for correction, while a smaller proportion utilized glasses in combination with contact lenses (6.7%) or had previously undergone refractive surgery (5.0%).
General information and characteristics of subjects categorized by mask type are summarized in Table 3. Twenty participants were assigned to each group based on their assigned mask type: Group 1 received earloop surgical masks; Group 2 received earloop surgical masks with adhesive nose strips; and Group 3 received anti-fog earloop surgical masks. Analysis of gender distribution showed a similar proportion of females across all three groups, with no statistically significant difference observed (p-value = 0.574). Age distribution across the groups was also comparable, with no significant differences found among the age categories (⩽30, 31–40, 41–50, 51–60, >60 years; p-value = 0.615). Regarding refractive error correction, the majority of participants in all groups reported the use of spectacles, with comparable percentages across groups (p-value = 0.829). Additionally, a small proportion utilized glasses in combination with contact lenses or had undergone previous refractive surgery. Evaluation of underlying diseases indicated a varied distribution across groups, with the prevalence of hypertension, diabetes mellitus, dry eye disease, and allergies differing among the groups, although statistical significance was not reached (p-value = 0.342).
Mask type and participant characteristics.
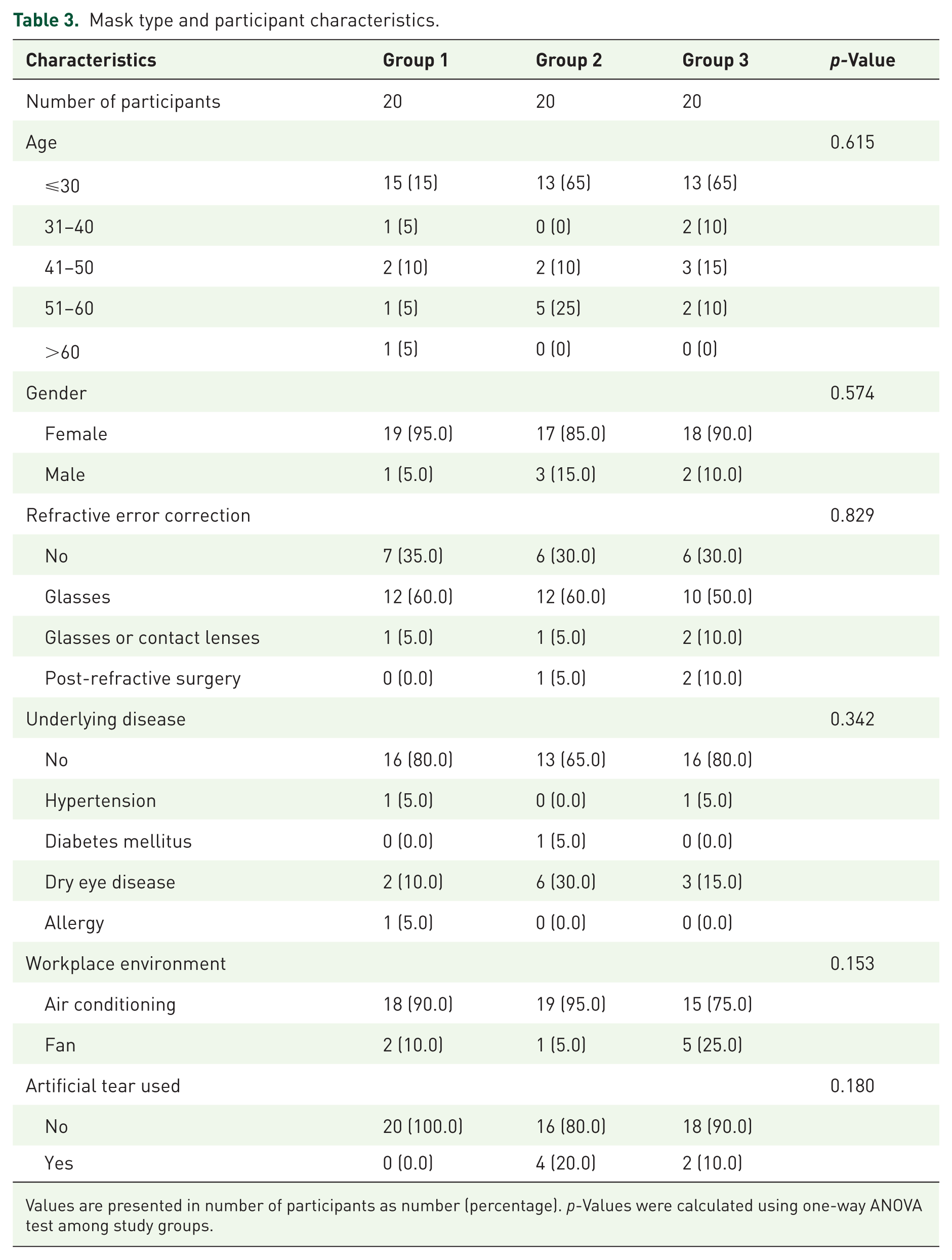
Values are presented in number of participants as number (percentage). p-Values were calculated using one-way ANOVA test among study groups.
The workplace environment also showed variability among the groups, with differing proportions of participants working in air-conditioned environments compared with those working with fan ventilation (p-value = 0.153). The usage of artificial tears varied across groups. However, there was no statistically significant difference observed among the groups (p-value = 0.180). Overall, the distribution of demographic and health-related characteristics did not significantly differ among the groups, suggesting comparability in baseline characteristics.
The mean values and standard deviations of tear film parameters and conjunctival redness score, measured from Keratograph 5M before the experiment across different groups, are presented in Table 4. No statistically significant differences between any of the parameters were observed among the groups. The p-values were as follows: first NIBUT, 0.763; overall average NIBUT, 0.839; conjunctival redness score, 0.106; and TMH, 0.431. The first NIBUT values ranged from 6.94 ± 4.90 to 7.78 ± 4.90 s across the different groups. Overall average NIBUT values ranged from 9.18 ± 5.08 to 9.84 ± 4.95 s. Conjunctival redness scores varied slightly, ranging from 0.66 ± 0.32 to 0.83 ± 0.43. Although the overall p-value did not reach statistical significance, post hoc analysis revealed that group 3 exhibited significantly lower baseline conjunctival redness scores compared to groups 1 and 2. Tear meniscus height (TMH) measurements also showed no significant differences among the groups, with values ranging from 188.81 ± 59.55 to 201.13 ± 85.10 µm. Overall, the analysis suggests that NIBUT, conjunctival redness score, and TMH, as measured by Keratograph 5M, were comparable across the different mask types before the experiment. The mean values and standard deviations of total corneal HOAs, including third-, fourth-, and fifth-order aberrations at 3 mm and 6 mm zones, assessed by the GSA before the experiment across different groups, are presented in Table 5. No statistically significant differences were observed between the groups. Additionally, baseline horizontal and vertical coma, which are part of third-order aberrations, were evaluated. No statistically significant differences were observed among the groups: the p-value for horizontal coma was 0.601 and 0.419 for the 3 mm and 6 mm zones, respectively. Baseline spherical aberrations, part of fourth-order aberrations, were also assessed, and no statistically significant differences were observed among the groups: the p-values for spherical aberrations were 0.295 and 0.375 for the 3 mm and 6 mm zones, respectively. Overall, the analysis suggests that wavefront parameters—total HOAs, third-, fourth-, and fifth-order aberrations, horizontal coma, vertical coma, and spherical aberrations—were comparable across the different mask types before the experiment was conducted.
Comparison of first NIBUT, overall average NIBUT, conjunctival redness score, and TMH among study groups at baseline and 8 h after mask-wearing.
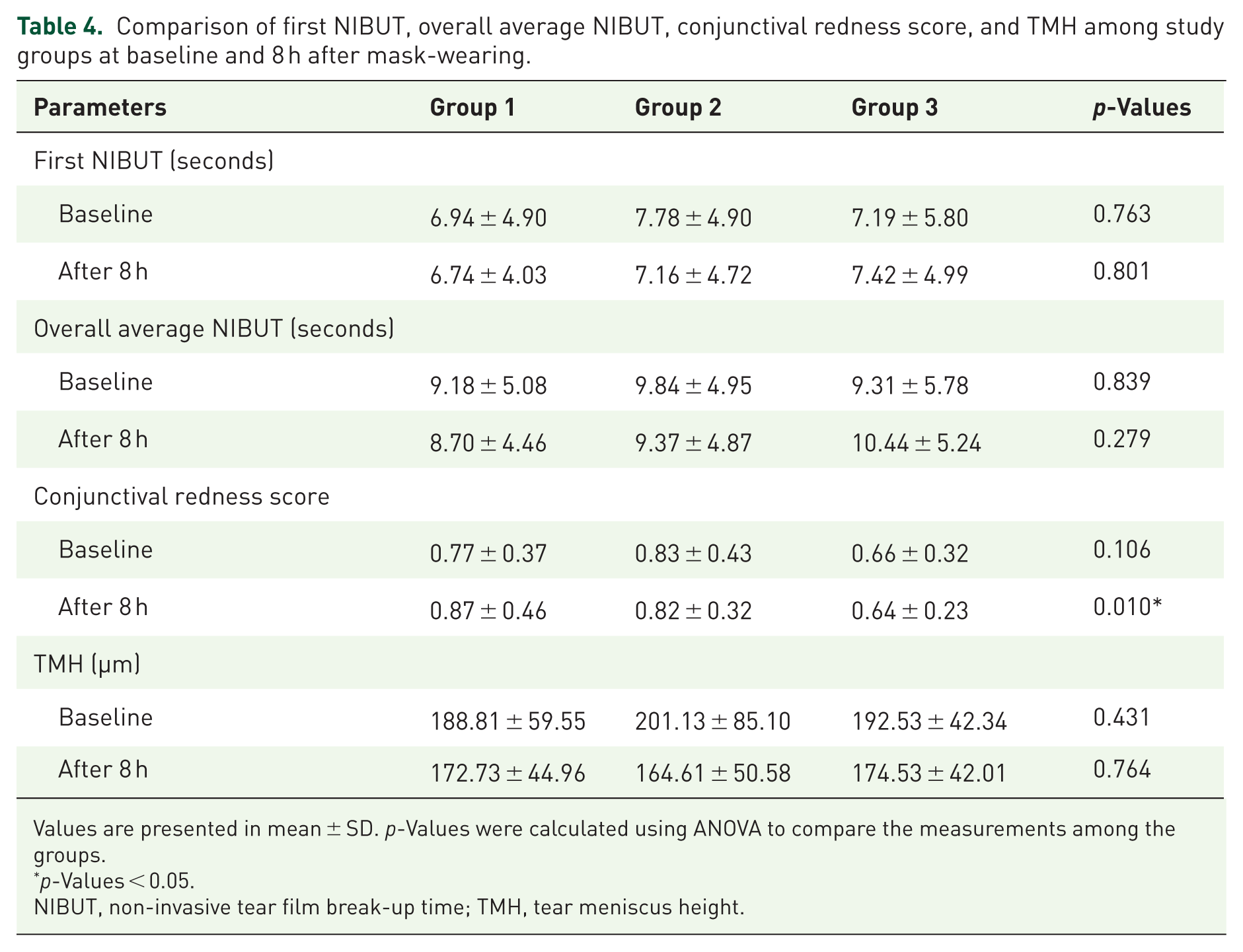
Values are presented in mean ± SD. p-Values were calculated using ANOVA to compare the measurements among the groups.
p-Values < 0.05.
NIBUT, non-invasive tear film break-up time; TMH, tear meniscus height.
Comparison of Total HOAs, third-, fourth-, and fifth-order HOAs in 3 mm and 6 mm zones among the study groups at baseline and 8 h after mask-wearing periods.

Values are presented in mean ± SD, micron. p-Values were calculated using ANOVA to compare the measurements among the groups.
p-values < 0.05 was considered statistically significant.
Data were not normally distributed; therefore, Kruskal-Wallis test was applied instead of ANOVA.
HOAs, higher-order aberrations.
The mean values and standard deviations of NIBUT, conjunctival redness score, and TMH after the experiment across different groups are shown in Table 4. The first NIBUT values ranged from 6.74 ± 4.03 to 7.42 ± 4.99 s across the different groups. Overall average NIBUT values for both eyes ranged from 8.70 ± 4.66 to 10.44 ± 5.24 s across the different groups. Neither the first nor overall average NIBUT values exhibited any significant differences among the groups after 8 h of mask-wearing. TMH measurements also showed no significant differences among the groups, with values ranging from 164.61 ± 50.58 to 174.53 ± 42.01 microns.
Table 5 displays the mean values and standard deviations of total corneal HOAs, including third-, fourth-, and fifth-order aberrations, horizontal coma, vertical coma, and spherical aberrations at 3 mm and 6 mm zones after the experiment across different groups. No statistically significant differences were observed between the groups for any parameters except total HOAs at the 6 mm zone. The total HOAs at the 6 mm zone ranged from 1.14 ± 0.48 to 1.85 ± 1.20 across the groups, with statistically significant differences observed (p-value = 0.012). Multiple comparisons using ANOVA revealed that study group 3 had significantly more total HOAs than the other groups (group 1 vs group 3: p-value 0.075; group 2 vs group 3: p-value 0.003; group 1 vs group 2: p-value 0.208).
Table 6 and Figure 5 present the comparison of first NIBUT, overall average NIBUT, conjunctival redness score, and TMH between baseline and 8 h after mask-wearing periods. Our study found that TMH significantly decreased after wearing the mask for 8 h in each study group. The p-values were 0.003 for group 1, 0.036 for group 2, and 0.034 for group 3. After 8 h of mask use, conjunctival redness scores increased significantly in group 1 compared to baseline (p = 0.048). Groups 2 and 3 did not show significant changes in conjunctival redness after 8 h. Table 7 and Figure 6 show the comparison of total HOAs, third-, fourth-, and fifth-order HOAs in 3 mm and 6 mm zones at baseline and 8 h after mask-wearing periods. There was no statistically significant difference between baseline and after the 8-h mask-wearing period in any of the parameters. There were no reports of adverse effects such as allergic reactions or skin irritation from the adhesive tape used in our study.
Comparison of first NIBUT, overall average NIBUT, conjunctival redness score, and TMH between baseline and 8 h after mask-wearing periods.
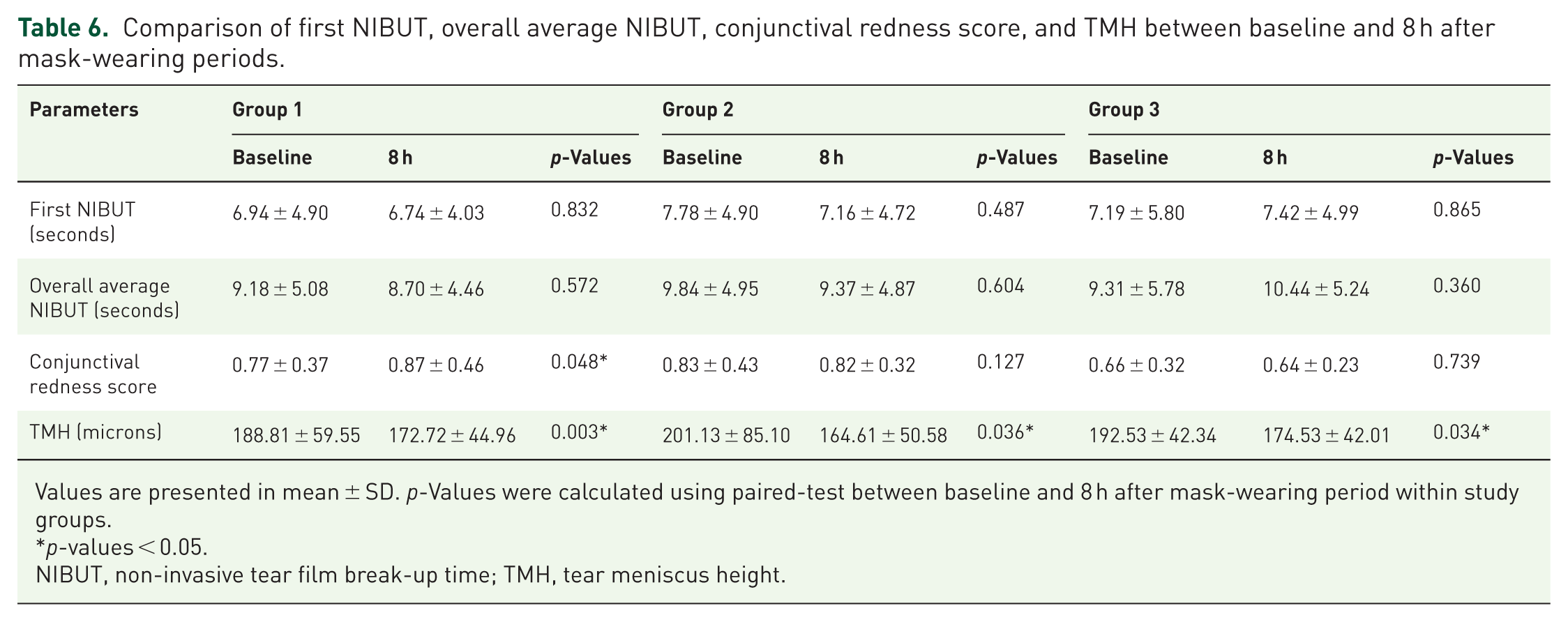
Values are presented in mean ± SD. p-Values were calculated using paired-test between baseline and 8 h after mask-wearing period within study groups.
p-values < 0.05.
NIBUT, non-invasive tear film break-up time; TMH, tear meniscus height.

Comparison of first NIBUT, overall average NIBUT, conjunctival redness score, and TMH between baseline and 8 h after mask-wearing periods.
Comparison of total, third-order, fourth-order, fifth-order HOAs, horizontal coma, vertical coma, and spherical aberrations between baseline and 8 h after mask-wearing.
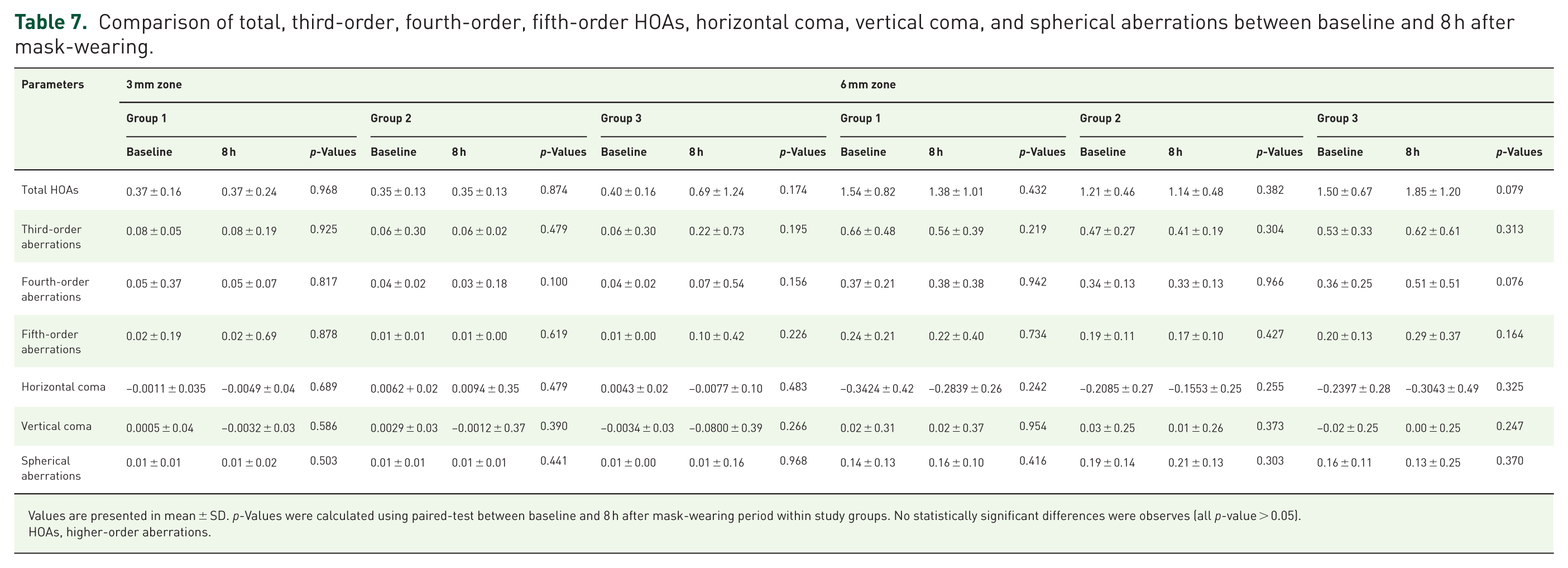
Values are presented in mean ± SD. p-Values were calculated using paired-test between baseline and 8 h after mask-wearing period within study groups. No statistically significant differences were observes (all p-value > 0.05).
HOAs, higher-order aberrations.

Comparison of total, third-order, fourth-order, fifth-order HOAs, horizontal coma, vertical coma, and spherical aberrations between baseline and 8 h after mask-wearing. (a) Data shown for the 3 mm optical zone. (b) Data shown for the 6 mm optical zone.
Discussion
Wearing facial masks presents significant challenges for ocular health. 8 Altered airflow and increased turbulence around the eyes disrupt tear film dynamics and cause increased tear evaporation and ocular surface irritation. Previous studies have indicated that prolonged use of masks may lead to changes in the ocular surface over time. It is important to emphasize that our study population—consisting primarily of young, healthy, and trained healthcare workers—is fundamentally different from those examined in earlier MADE studies. For instance, Moshirfar et al. 12 reported on MADE in an elderly population, often seen post-cataract surgery and using multiple preservative-containing eye drops, representing a medically complex cohort with different ocular surface vulnerabilities. These differences underscore that the ocular effects of mask wearing may vary substantially between populations, and our findings mainly reflect the impact on younger, healthy individuals who may be more resilient to ocular surface disruption. Koprubasi et al. 26 examined the impact of long-term mask usage on ocular health in individuals who wore masks for at least 8 h daily for a minimum of 6 months, comparing them with healthy volunteers who used masks for no more than 1 h daily. They discovered significantly higher ocular surface disease index (OSDI) scores among mask users compared to that of the control group; additionally, mean Schirmer test values and tear break-up time (TBUT) were notably lower in the study group than in the control group. Similarly, Celik et al. 9 conducted a comparative study involving healthcare professionals. They found that TBUT was significantly shorter in the long-term mask users working in COVID-19 pandemic clinics compared to that of a control group of short-term mask users. Another study by Mine Esen Baris et al. 27 focused on healthcare professionals, measuring the effects of wearing surgical face masks throughout the workday. Evaluations were conducted at 8 am when participants initially put on the masks and again at 5 pm after a full day of use. The findings revealed a significant deterioration in both the OSDI scores and TBUT by the end of the workday compared to in the morning.
However, another study by D’Souza et al. 28 involved healthy ophthalmologists and compared two periods: before the widespread use of face masks and during the COVID-19 pandemic, where continuous mask use was implemented. They found no significant changes in TBUT, Schirmer’s test 1, or objective scatter index. Another study by Schargus et al. 29 of healthy volunteers found no statistically significant change in NIBUT or lipid layer thickness (LLT) after 30 min of wearing either surgical masks or filtering facepiece respirator masks. Our study similarly found no statistically significant changes in first or average NIBUT across all study groups after 8 h of mask wearing.
However, we observed a statistically significant increase in conjunctival redness among participants in Group 1, who wore surgical masks without taping. Although the overall post-wear differences among groups reached statistical significance (p = 0.010), post-hoc analysis revealed that group 3, using anti-fog surgical masks, had significantly lower baseline conjunctival redness compared to groups 1 and 2. Furthermore, only group 1 showed a significant increase in conjunctival redness after 8 h (p = 0.048), whereas no significant changes were observed in groups 2 and 3. This suggests that masks with better upper-edge sealing—either via adhesive strips or anti-fog design—may help reduce conjunctival hyperemia potentially caused by upward airflow and increased evaporation. This observation could be related to an increase in conjunctival temperature and blood flow, as noted in a study by Itokawa et al., 11 which found significantly higher conjunctival temperature and blood flow differences in individuals who had worn an untaped mask compared to those who had employed a taped one. The absence of significant redness in groups 2 and 3 suggests that improved sealing—either through taping or anti-fog design—may reduce airflow and associated inflammation; however, further studies are warranted to clarify these physiological mechanisms. Therefore, conjunctival redness may serve as a sensitive marker of mask-associated ocular surface stress, and interventions to improve mask fit could be beneficial in minimizing this effect. This increase may be linked to elevated levels of ocular surface inflammatory markers following mask wearing,28,30 but additional research is needed to confirm this relationship.
We also found a significant decrease in TMH across all study groups. While differences in TMH reduction between groups were not statistically significant, the overall trend suggests that even well-fitted masks do not fully prevent ocular surface dehydration, particularly in air-conditioned or low-humidity environments. Similarly, several studies have found a significant decrease in TMH after wearing different types of masks.8,31 –33
Regarding the impact on dry eye of taping the upper mask edge, Nair S et al. 13 evaluated dry eye parameters in healthcare workers before and after an 8-h shift. They compared the outcomes of use of an N95 face mask without taping the upper edge on 1 day with those of using an N95 face mask with taped upper edge on the next day. Their findings showed that post-taping, parameters such as NIBUT, TBUT, LLT, TMH, corneal staining scores, and tear osmolarity significantly improved when the mask was used with taping. These improvements correlated well with reductions in dry eye symptoms. The authors recommended taping the upper mask edge, particularly for healthcare professionals who need to wear face masks for extended periods. However, they also noted that 8% of participants experienced skin irritation symptoms; therefore, use of hypoallergenic tape should be considered in order to help prevent the occurrence of this adverse event. Additionally, optimizing face mask design to better fit facial contours can further improve airtightness.
Schultheis et al. 34 conducted a study to assess the impact of taping the upper edge of masks on particle counts near the eye. They tested cloth, surgical, and N95 masks in a randomized order, measuring particle counts with and without tape at the top of each mask. Their results suggested that taping the upper edge of cloth masks while speaking can significantly reduce particle counts near the eye. However, taping cloth masks during normal breathing or taping surgical/ N95 masks did not show significant benefits in reducing particle exposure in clinical settings. In our study, we found no statistically significant differences in tear film parameters, including first NIBUT, overall average NIBUT, and TMH, when comparing different mask types across three groups: surgical mask without tape, surgical mask with tape, and anti-fog surgical mask. This suggests that taping does not significantly impact tear film instability when a secure fit over the nose is ensured. A possible explanation for our finding could be that our study participants were healthcare professionals who were trained and had a good understanding of how to correctly wear masks with proper fit. However, individuals who are unfamiliar with face masks may not always wear them correctly, and this can impact the masks’ effectiveness in reducing airflow effectively from the upper edge of the mask. Therefore, taping may be necessary if the proper fit and adherence of the face mask are inadequate.
Regarding the impact of different types of masks on dry eye parameters, Schargus et al. 29 studied healthy volunteers wearing no mask, a surgical face mask, or a filtering face piece FFP2 or KN95 mask for 30 min each. They performed examinations after each 30-min mask-wearing session in a pre-specified random order. Their findings indicated that short-term wearing of face masks, regardless of type, did not result in significant differences in tear film parameters such as LLT, NIBUT, and TMH, either in healthy individuals or in those with dry eyes. These findings are consistent with ours. Similarly, Tatti et al. 8 conducted a study of healthcare personnel, measuring corneal fluorescein staining, TBUT, and Schirmer test before and after a 7-h work shift with continuous use of either surgical masks or N95 masks. They reported no significant changes in these clinical parameters during the use of either type of mask.
Another study by Shalaby et al. 35 evaluated the impact on various dry eye parameters of wearing surgical face masks and N95 masks for 60 min. They observed that wearing face masks for this duration significantly worsened TBUT, corneal fluorescein staining, and Schirmer test results in both types of masks. Additionally, they found that the deterioration in these parameters was significantly greater in subjects wearing surgical masks than in those wearing N95 versions. They concluded that this difference may be attributed to the tighter fitting provided by N95 masks, which limits airflow to the eyes more effectively than surgical ones. All these findings underscore the importance of mask fitting in reducing air leaks from the upper edge of the mask, which is crucial in influencing dry eye parameters, emphasizing that regardless of the design or material of the mask, the key determinant of its impact on dry eye symptoms is how effectively it fits and seals around the nose and face. A proper fit ensures minimal air leakage, helping to maintain adequate humidity levels and reduce airflow over the ocular surface, thereby potentially mitigating dry eye symptoms. This is particularly important for individuals who are allergic to adhesive tape, who may prefer using regular surgical masks without taping or opt for specialized mask designs that ensure a secure fit without the need for tape.
HOAs are optical imperfections of the eye that degrade retinal image quality, causing difficulties such as night vision problems, glare, halos, blurring, and starburst vision, even when lower order aberrations like spherical defocus and astigmatism are corrected.36,37 Although all structures along the visual axis, particularly the cornea and lens, influence HOAs, the majority of HOAs in normal eyes originate from the tear film and cornea. 38 Published evidence has clearly established a connection between dry eye disease (DED) and HOAs, showing that HOAs are increased in DED patients compared to those with normal eye and that they are correlated with dry eye severity.39 –41
To the best of our knowledge, this is the first study to investigate the HOAs associated with different types of masks. We found that total HOAs, as well as third-, fourth-, and fifth-order aberrations including horizontal coma, vertical coma, and spherical aberrations, did not exhibit significant changes after participants in any of the groups wore masks for 8 h. Although we observed changes in TMH after 8 h of mask-wearing, other tear parameters such as NIBUT and conjunctival redness scores remained unchanged.
Previous studies have demonstrated a significant negative correlation between HOAs and TBUT, providing further evidence that as TBUT decreases, and consequently dry eye severity worsens, HOAs increase.39,40,42 Jung et al. 42 investigated the effect of tear film instability on HOAs of the corneal surface after Laser-Assisted Sub-Epithelial Keratectomy (LASEK). They observed a significant increase in total HOAs, coma, trefoil, and spherical aberration post-LASEK compared to preoperative levels. Moreover, there was a negative correlation between the changes in total HOAs, coma, and trefoil with TBUT. Likewise, Denoyer et al. 40 conducted a study on dry eye patients, revealing that HOAs, including third to sixth-order aberrations, were negatively correlated with both TBUT and Schirmer I test results. These may be the reasons why the HOAs measured in our study did not show statistically significant changes.
In terms of changes in TMH and HOAs, there is limited research aimed at specifically addressing their direct correlation with DED. Kusada et al. 38 conducted an analysis to explore the relationship between HOAs and parameters of ocular surface abnormalities by continuously measuring HOAs in DED after eye opening. The study revealed negative correlations between TMH and HOAs, although these correlations did not reach statistical significance at any of the measured time points (1–5 s after eye opening). However, it is known that dry eye conditions can affect both TMH and HOAs,39,40,42,43 potentially linking them indirectly. Given that both TMH and HOAs are influenced by the stability and quality of the tear film, 44 it is plausible that changes in TMH might indirectly correlate with changes in HOAs. In our study, we observed a significant decrease in TMH in all study groups. However, no significant changes were found in HOAs, including total HOAs and specific aberrations such as horizontal coma, vertical coma, and spherical aberrations within the group. These findings suggest that while TMH decreases, it may not directly or immediately impact the HOAs within the duration of our study. Further research is needed to explore the potential relationship between TMH and HOAs and to understand the long-term effects of TMH changes on ocular aberrations in MADE. We also found statistically significant differences between the study groups after 8 h of mask-wearing with regard to total HOAs at the 6 mm zone but not at the 3 mm zone. Notably, group 3 had significantly more total HOAs than the other groups. Although individual components of HOAs—such as coma and spherical aberration—did not show statistically significant differences, total HOAs represent the cumulative root mean square of multiple aberration terms. Therefore, small, non-significant increases across several components can collectively result in a statistically significant elevation in total HOAs, as observed in group 3. This suggests that the increase may reflect the cumulative effect of minor, subclinical changes rather than a clear physiological impact directly attributable to the anti-fog mask design. This finding may not significantly affect daily life because adult pupils typically range from 2 to 4 mm in diameter in normal bright light conditions 45 ; therefore, the increase in total HOAs at the 6 mm zone might not clinically significantly impact visual quality except in dark conditions, where pupils can dilate to 4–8 mm. 45 In such low-light situations, larger pupils could potentially exacerbate the effects of increased HOAs on visual acuity and quality. Furthermore, patients with preexisting ocular conditions such as DED, corneal irregularities, or other anterior segment disorders may be more vulnerable to the visual disturbances caused by increased HOAs. These individuals often already experience compromised tear film stability and optical quality.39,40 For these patients, even subtle increases in HOAs associated with prolonged mask use may exacerbate visual disturbances. Given these considerations, we interpret the HOA findings with caution, recognizing the need for further studies to clarify the long-term visual impact and to better understand the underlying mechanisms by which different mask types might influence ocular aberrations.
There are several possible underlying pathophysiological mechanisms of eye MADE. The most common hypothesis is that MADE is caused by upward airflow from the upper edge of the mask toward the ocular surface, which may stimulate tear film evaporation. 12 Other possible mechanisms include higher concentrations of carbon dioxide in exhaled air, which may induce hypercapnia-related changes in ocular microbiota 28 and inflammation of the ocular surface, 30 and the warmer exhaled air, which may promote higher tear evaporation. 46
Although our study attempted to minimize upward airflow by ensuring a proper face fit with the moldable nose bridge of the mask, taping the upper edge, or using a specially designed anti-fog mask, we still observed significant changes in some tear and wavefront parameters after 8 h of wearing a mask. This finding may be explained by the multifactorial nature of DED. Several potential etiologies may contribute to the development of DED, including low-humidity environments, prolonged use of computers and display devices, hormonal imbalances, systemic diseases, autoimmune diseases, certain medications, contact lens use, and ocular surgery. 44 In our study, the possible cause of dry eye in the short term could be attributed to the work environment of the participants, many of whom were healthcare professionals working in hospitals, often using computers throughout the day. Most of them worked in air-conditioned rooms with low humidity, and some operated in rooms with fans, which can direct airflow to the eyes and cause tear evaporation. It is important to note that the current literature on MADE predominantly focuses on healthcare workers, a relatively young and healthy population accustomed to prolonged mask use. However, the clinical implications of MADE may be more significant for elderly patients, especially those recovering from ocular surgeries such as cataract extraction, who have increased ocular surface vulnerability. These patients often require mask use during postoperative periods, potentially exacerbating dry eye symptoms and delaying healing. Future research should prioritize studying this vulnerable population to better understand the risks and develop tailored preventive strategies.
Limitations
Our study has several limitations that should be acknowledged. First, participants were not closely monitored during their work shifts, which limited our ability to ensure consistent mask fitting throughout the 8-h period. Variability in mask seal may have influenced the outcomes related to tear film parameters and wavefront aberrations. Second, the absence of a control group not wearing face masks restricts our ability to determine whether the observed changes were solely due to mask usage or influenced by other environmental or occupational factors. However, including a non-mask-wearing control group was not feasible, as all participants were healthcare personnel required to wear masks during work hours. Third, the predominance of female participants in our sample, reflecting the demographic characteristics of healthcare personnel at our institution, may limit the generalizability of our findings to populations with more balanced or male-dominant gender distributions. Fourth, the age distribution of our study population was skewed toward younger healthcare personnel under 30 years old. While this reflects the staff demographics at our institution, it may limit the applicability of our findings to older age groups. Fifth, there was an imbalance in the prevalence of the underlying DED across the groups. Although this difference was not statistically significant, it may have influenced the outcomes and should be considered when interpreting the results. Sixth, while HOAs were used as an objective indicator of optical quality, they may not fully reflect the subjective experience of ocular discomfort or visual disturbance. Additionally, we did not incorporate validated symptom-based questionnaires such as the OSDI, which could have provided valuable insights into participants’ perceived symptoms. The absence of patient-reported outcomes limits our ability to correlate objective findings with subjective experience. Future studies should integrate both objective and subjective measures for a more comprehensive assessment of mask-associated ocular surface changes. In addition, research using standardized mask-fitting protocols, inclusion of a non-mask-wearing control group, and more demographically diverse populations will be essential to validate and expand upon the present findings.
Conclusion
This study investigated the impact of three commonly used disposable surgical masks—earloop surgical masks, earloop surgical masks with adhesive nose strips, and anti-fog earloop surgical masks—on ocular surface parameters and corneal wavefront aberrations among healthcare personnel during an 8-h work shift. Our findings indicate that prolonged mask use leads to a significant decrease in TMH across all mask types, suggesting reduced tear stability over time. Notably, only the standard earloop mask group showed a significant increase in conjunctival redness, suggesting greater ocular surface irritation, while masks with better upper-edge sealing helped mitigate this effect. No statistically significant differences were found between the mask types in first NIBUT, overall average NIBUT. The anti-fog mask group showed a significant increase in total HOAs at the 6 mm zone, which may have implications for visual quality in certain conditions. These findings indicate that proper mask fit, particularly with effective upper-edge sealing, is crucial to reducing ocular surface irritation and tear film instability associated with prolonged mask use. While specialized mask designs may offer advantages, further research is needed to assess their long-term benefits. Ensuring a secure and comfortable mask fit is especially important for healthcare professionals who wear masks for extended periods.
Supplemental Material
sj-docx-1-oed-10.1177_25158414251378120 – Supplemental material for Alterations in tear film and wavefront parameters associated with different types of disposable surgical masks in healthcare personnel during working hours: a randomized trial
Supplemental material, sj-docx-1-oed-10.1177_25158414251378120 for Alterations in tear film and wavefront parameters associated with different types of disposable surgical masks in healthcare personnel during working hours: a randomized trial by Somporn Chantra, Nalinrat Disayavatin and Parinee Kemchoknatee in Therapeutic Advances in Ophthalmology
Footnotes
Acknowledgements
We would like to thank John Flanagan, who is a native English-speaking editor, for proofreading and editing the manuscript. Thanks are also due to Assoc. Prof Dusit Sujirarat, for his assistance in statistical analysis and for giving feedback to improve this study
Declarations
Supplemental material
Supplemental material for this article is available online.
Protocol amendments
No amendments were made to the study protocol after registration in the Thai Clinical Trials Registry (TCTR20230725002).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.