
Abstract
Background:
Dry eye disease is a common condition that causes symptoms such as dryness, irritation, and blurry vision. The pathophysiology of dry eye disease features both aqueous deficiency (loss of aqueous tear production) and increased evaporation (loss of the lipid layer), with the latter mechanism responsible for most of the disease presentation. Ocular surface disease (OSD) is a prevalent condition, often linked to meibomian gland dysfunction (MGD), characterized by tear film instability and symptoms like dryness and irritation. Thermal pulsation therapy, an FDA-approved treatment for MGD, uses heat and pressure to restore gland function, improving tear film stability and ocular health. Studies show its benefits last up to a year, enhancing Ocular Surface Disease Index (OSDI), tear break-up time (TBUT), and Meibomian Glands Yielding Secretion Score (MGYSS) scores. This systematic review evaluates LipiFlow compared to placebo, warm compresses, and other devices, focusing on safety, efficacy, and its impact on recovery and long-term outcomes.
Methods:
A comprehensive search was performed across PubMed, MEDLINE, Embase, and Scopus until December 2024. Only randomized controlled trials (RCTs) evaluating LipiFlow were included. The primary outcomes assessed were OSDI and TBUT, with secondary outcomes including meibomian gland expression scores, corneal fluorescein staining (CFS), MGYSS, and lipid layer thickness (LLT). Meta-analyses were conducted using a random-effects model, and heterogeneity was assessed using I² statistics.
Results:
Thirteen studies reported OSDI (Std diff −0.076, 95% CI −0.277 to 0.125, p = 0.255, I² = 71.21%). Twelve studies evaluated MGYSS, showing significant improvement (Std diff 0.449, 95% CI 0.173–0.725, p = 0.001, I² = 78.49%). TBUT results from twelve studies were not statistically significant (Std diff 0.211, 95% CI −0.017 to 0.440, p = 0.8350, I² = 0%). CFS showed significant improvement in six studies (Std diff −0.130, 95% CI −0.248 to −0.012, p = 0.031, I² = 0%). LLT changes were insignificant (Std diff −0.071, 95% CI −0.381 to 0.239, p = 0.653, I² = 0%).
Conclusion:
LipiFlow effectively improves meibomian gland function, as indicated by TBUT, MGYSS, and CFS, but its impact on LLT and OSDI is not significant. The therapy is most beneficial for patients with severe baseline MGD. Further research is needed to establish long-term benefits and patient-specific outcomes.
Plain language summary
Dry eye disease is a common condition that causes symptoms such as dryness, irritation, and blurry vision. Many cases are linked to meibomian gland dysfunction (MGD), where the meibomian glands in the eyelids do not produce enough oil to maintain a healthy tear film. LipiFlow is an FDA-approved treatment designed specifically for MGD. It uses heat and gentle pressure to massage the eyelids, helping to unblock the meibomian glands and restore their function. Our review analyzed research studies that tested LipiFlow and compared it with other treatments, such as warm compresses or no treatment. The studies included participants who were randomly assigned to different treatment groups to ensure reliable results. The findings showed that LipiFlow significantly improves meibomian gland function, as measured by a score called the Meibomian Gland Yielding Secretion Score (MGYSS). It also reduces staining on the eye’s surface, an indicator of damage caused by dryness. However, LipiFlow showed less impact on how patients reported their symptoms, such as dryness and discomfort, as assessed by the Ocular Surface Disease Index (OSDI). Another test, tear break-up time (TBUT), which evaluates the stability of the tear film, also showed minimal improvement with LipiFlow. LipiFlow appears to be most beneficial for individuals with severe meibomian gland dysfunction. While it can enhance meibomian gland health and protect the ocular surface, more research is needed to determine its long-term benefits and whether it is more effective for specific groups of patients.
Introduction
Ocular surface disease (OSD) is a prevalent condition characterized by dysfunction of the tear film and ocular surface, leading to symptoms such as dryness, redness, and irritation. This condition is especially common among older adults. 1 Research indicates that up to two-thirds of individuals with OSD experience dry eye symptoms, 2 with certain medical procedures such as LASIK, cataract surgery, and corneal transplantation, often exacerbating these issues. 3 Persistent dry eye symptoms have been reported in more than one-third of individuals following various interventions, including refractive surgeries and lid procedures.4,5 Dry eye disease is a common condition that causes symptoms such as dryness, irritation, and blurry vision, with a pathophysiology featuring both aqueous deficiency (loss of aqueous tear production) and increased evaporation (loss of the lipid layer), the latter mechanism being responsible for most disease presentations. 6 In the first few months after certain treatments, such as topical prostaglandin analogs, artificial tear supplementation, anti-inflammatory agents and preservative-containing eye drops, ocular surface symptoms often worsen. 6 Additionally, these procedures have been linked to abnormalities in the lid margin.7 –9 Addressing OSD signs and symptoms early may help mitigate complications.10,11
Management traditionally includes artificial tears, ointments, and anti-inflammatory medications, though these only provide temporary relief and increase treatment burden. This limited efficacy stems from a fundamental mismatch between treatment mechanisms and disease pathophysiology. Conventional approved treatments such as cyclosporine (Restasis) and lifitegrast (Xiidra) primarily target inflammation associated with aqueous deficiency,12,13 failing to address the predominant evaporative component. Lipid-containing artificial tears (e.g., Systane Complete, Refresh Optive) attempt to supplement the tear film’s lipid layer, 14 but these merely replace lipids without treating the underlying meibomian gland dysfunction (MGD). This treatment gap highlights the need for comprehensive approaches addressing both pathophysiological mechanisms, particularly targeting meibomian gland function restoration rather than simply managing symptoms. 15
MGD is a leading contributor to OSD and can be effectively addressed using thermal pulsation, an FDA-approved technique that utilizes regulated heat and intermittent pressure to unclog obstructed meibomian glands. 16 This approach seeks to restore gland function, thereby improving the tear film and alleviating symptoms associated with OSD.17,18 Thermal pulsation has emerged as a leading non-invasive option for managing MGD and its related manifestations.19,20 The thermal pulsation system (LipiFlow) offers superior efficacy by directly addressing the root cause of evaporative dry eye through clearance of obstructed meibomian glands. 21 By improving meibomian gland function, LipiFlow restores the lipid layer of the tear film, reducing evaporation while simultaneously enhancing aqueous tear distribution and retention. 22 Studies have shown that a single 12-min session can significantly enhance meibomian gland secretion, tear film stability, and symptom survey scores, with benefits lasting up to nine months post-treatment.23,24 Additional research indicates that meibomian gland function shows gradual improvement from baseline to one month after treatment, with effects lasting up to 1 year. These findings underscore the potential of thermal pulsation therapy to optimize ocular surface health and improve quality of life.25,26 These advantages were linked to superior management of MGD, resulting in optimal ocular surface health.
These conditions are challenging to manage due to their multifactorial etiology and chronic nature. Traditional treatments, such as warm compresses and artificial tears, offer limited and temporary relief. Lipiflow has emerged as a novel intervention by directly addressing meibomian gland dysfunction through heat and mechanical pressure, enhancing gland function and tear film stability. Although studies have shown the benefits of LipiFlow for dry eye syndrome (DES) and MGD, comprehensive evidence comparing its efficacy to placebo, warm compresses, or other thermostatic devices remains limited. Additionally, understanding the impact of preoperative and postoperative interventions on outcomes is crucial for optimal patient management. This systematic review and meta-analysis aim to address the gap by analyzing LipiFlow outcomes compared to other treatments before and after surgical interventions. The primary objective is to systematically review and meta-analyze the literature on the efficacy and safety of the thermal pulsation system (LipiFlow) for treating DES and MGD, compared to placebo, warm compresses, or other thermostatic devices. Specifically, we evaluate clinical outcomes such as the ocular surface disease index (OSDI), tear break-up time (TBUT), meibomian gland expression scores, corneal fluorescein staining (CFS), and meibomian glands yielding secretion score (MGYSS). Additionally, we explore the effectiveness of these interventions administered before and after ocular surgical procedures, assessing their impact on postoperative recovery and long-term outcomes. By analyzing both preoperative and postoperative interventions, we aim to provide a comprehensive understanding of how treatment timing and application influence clinical outcomes and patient satisfaction.
Methods
Search strategy
Two authors (K.Y.C. and H.C.C.) conducted a thorough, methodical search across key electronic databases, including PubMed, MEDLINE, Embase, and Scopus, covering their entire timelines up to 7th December 2024. Any discrepancies or misunderstandings were resolved through consensus with a third author (C.M.C.). The investigation sought to identify all pertinent studies evaluating the effectiveness of the thermal pulsation system (LipiFlow) compared to placebo, warm compresses, or alternative thermostatic devices for treating DES and MGD. The search protocol utilized a blend of MeSH terms and keywords, such as “Dry eye syndrome,” “Meibomian gland dysfunction,” “Thermal pulsation system,” “Lipiflow,” “Ocular surface disease index,” and “Tear break-up time.” The review was limited to English-language publications. Supplementary efforts were made to uncover relevant gray literature and references from the included studies. This comprehensive search adhered to the guidelines set forth by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) frameworks to ensure a rigorous, systematic approach. 27 The study protocol has been registered at PROSPERO, number CRD42024619988.
Eligibility criteria
We implemented rigorous selection criteria to ensure the included studies were robust and relevant. Only randomized controlled trials (RCTs) were considered, as they represent the highest standard of clinical evidence. These studies had to specifically examine the efficacy of the thermal pulsation system (LipiFlow) compared to placebo, warm compression, or other thermostatic devices in treating patients diagnosed with DES or MGD. We excluded studies that were animal or laboratory-based, not in English, or reported outcomes unrelated to our analysis. Research with irretrievable data, lacking a control group, or published as letters, editorials, expert opinions, or conference abstracts was also omitted. Furthermore, to maintain consistency and accuracy, studies needed to report effect estimates such as odds ratios (ORs) or mean differences (MDs) with 95% confidence intervals (CIs) or provide sufficient raw data for these calculations. We did not impose limitations on sample size or follow-up duration, allowing for a comprehensive inclusion of research in this field.
Outcome measures and data extraction
This meta-analysis focused primarily on the OSDI and TBUT as key metrics for evaluating the effectiveness of treatments for DES and MGD. Additional outcomes examined included meibomian gland expression scores, CFS, and the MGYSS, which offered further insights into how these interventions affected ocular surface health and meibomian gland functionality. Two authors (K.Y.C. and H.C.C.) independently collected crucial data from the studies included in the analysis, such as research design, subject demographics, treatment methods, control groups, outcome assessments, and follow-up durations. The extracted information was then cross-verified by both researchers to ensure its accuracy. When disagreements arose, the researchers engaged in discussions to reach a consensus. To facilitate comparison across studies, statistical methods were employed to convert medians and interquartile ranges (IQRs) into means and standard deviations (SDs) where required, using established mathematical formulas.
Statistical analysis
The meta-analysis was performed using Comprehensive meta-analysis (CMA; Englewood, NJ, USA: version 3.3.070). Meta-analyses were conducted using a random-effects model, and heterogeneity was assessed using I² statistics. To facilitate interpretation, forest plots were structured to group studies by comparator (e.g., placebo, warm compresses, other devices), allowing readers to assess potential confounders and variations in treatment effects. For continuous variables like OSDI and TBUT, the overall impact of the thermal pulsation system (LipiFlow) versus control interventions was evaluated using standardized mean differences (SMDs) with 95% CIs. The same statistical approach was applied to calculate pooled estimates for secondary outcomes, including meibomian gland expression scores, CFS, and MGYSS. To visually represent individual and pooled effect sizes for each outcome, forest plots were created. The I² statistic was used to assess heterogeneity among studies, with values above 50% indicating substantial heterogeneity. In cases of significant heterogeneity, a leave-one-out sensitivity analysis was conducted to identify studies contributing to the observed variance. This method involved systematically excluding individual studies and reanalyzing the data to ensure the robustness and reliability of the final pooled estimates.
Quality assessment and risk of bias
Two independent authors (K.Y.C. and H.C.C.) conducted a thorough assessment of the methodological quality and potential bias in the selected studies. Their evaluation focused on crucial aspects of trial design and implementation, such as the effectiveness of participant blinding, the method of random sequence generation, the accuracy of outcome assessment, the management of incomplete data, and other possible bias sources. Each study received a risk of bias rating for these factors, classified as low, high, or uncertain. Studies deemed “low risk” exhibited strong methodology and minimal bias, while those labeled “high risk” showed significant methodological issues. When the two reviewers disagreed on the bias assessment, a third reviewer (C.M.C.) was brought in to settle the discrepancies through extensive discussion and mutual agreement. This collaborative approach ensured consistent evaluation of bias risk across all studies, thereby enhancing the overall quality of the meta-analysis.
Result
Literature search
To identify pertinent studies for this systematic review and meta-analysis, an extensive search of the literature was performed. The search yielded 1874 records from various databases, including PubMed, MEDLINE, Embase, and Scopus. After eliminating 839 duplicate entries, 156 records flagged as ineligible by automated tools, and 55 for miscellaneous reasons, 824 records remained for screening. During the screening phase, 610 records were excluded based on their titles and abstracts, mainly due to a lack of relevance to the research question. Additionally, through citation searching, 30 records were identified and assessed similarly. The eligibility of 214 full-text reports was then evaluated. Among these, 103 studies were excluded for having a different PICO (Population, Intervention, Comparator, Outcome), 69 for employing a different study design or being animal model studies, and 25 were eliminated as case reports or case series. Ultimately, 18 studies met the inclusion criteria and were incorporated into the final review and meta-analysis (Figure 1).

Baseline characteristics of included studies.
Characteristics of included studies
This comprehensive review and statistical analysis incorporate 18 RCTs conducted across multiple nations, including the United States, China, Thailand, Italy, Germany, and France, indicating global interest in evaluating the efficacy of the LipiFlow thermal pulsation system for MGD and DES treatment. The included studies show varied characteristics, with participant counts ranging from 12 to 119 and follow-up durations extending from 1 to 12 months. Participant ages spanned from 18 to over 70 years, reflecting the broad age range affected by MGD and dry eye conditions. The majority of studies utilized comparable eligibility criteria, requiring participants to meet specific benchmarks for dry eye symptoms and meibomian gland function, such as OSDI scores ⩾23, TBUT ⩽7 s, or MGS scores ⩽12. The primary intervention involved a single 12-min LipiFlow thermal pulsation system treatment, with some studies comparing its effectiveness to alternative therapies like warm compresses, TearCare, or lid hygiene. The studies primarily assessed outcomes including OSDI, TBUT, MGYSS, lipid layer thickness (LLT), and meibomian gland expression scores. Many reported notable improvements in symptoms and gland functionality following LipiFlow treatment. Several studies observed benefits in both pre- and post-surgical contexts, suggesting thermal pulsation therapy may be beneficial before cataract or other ocular procedures. However, results varied across studies, with some indicating LipiFlow was non-inferior to other interventions such as iLux and TearCare, while others emphasized its superiority in improving ocular surface health and alleviating dry eye symptoms (Table 1).
Baseline characteristics of included studies.

LLT, lipid layer thickness; MGS, meibomian gland score; OSDI, Ocular Surface Disease Index; TUBT, tear film break-up time.
Ocular surface disease index
OSDI, which assesses dry eye symptom severity, was examined in 13 studies. A meta-analysis comparing the thermal pulsation system (LipiFlow) with control interventions (including placebo, warm compresses, and other thermostatic devices) revealed no statistically significant improvement in OSDI scores. The calculated pooled SMD was −0.076 (95% CI: −0.277 to 0.124), with a p-value of 0.255 and Z-score of −0.747 (Figure 2), indicating no significant effect. While substantial heterogeneity was observed among the studies (I² = 71.21%), the heterogeneity p-value of 0.204 suggested this variability was not statistically significant (Supplemental Table 1). Further sensitivity analysis did not reveal any significant publication bias or inconsistencies, despite the high I² value.
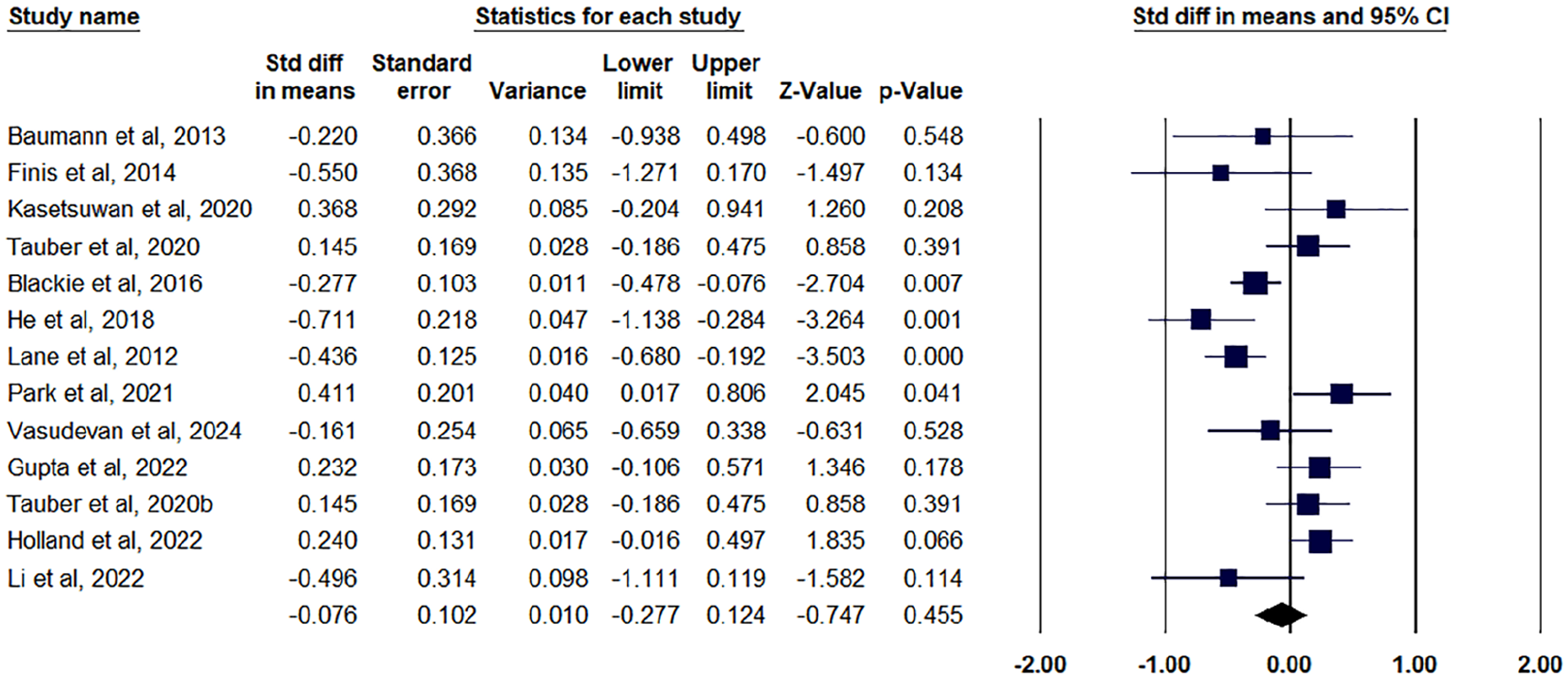
Forest plot for OSDI outcome.
Figure 3 shows the meta-analysis on the SMD in OSDI scores comparing LipiFlow treatment to different control groups. The subgroup analysis categorizes studies based on the type of control used: Other Devices, Placebo, and Warm Compression.

Subgroup analysis on the OSDI outcome.
For the Other Device subgroup (7 studies), the pooled SMD was −0.019 (SE = 0.130), with a wide confidence interval (−0.274, 0.236) and a non-significant p-value (p = 0.885), indicating no clear advantage of LipiFlow over other devices. This subgroup exhibited substantial heterogeneity (I² = 72.2%), suggesting variability in study results. The Placebo subgroup (three studies) showed a pooled SMD of 0.217 (SE = 0.185), with a confidence interval of (−0.146, 0.579) and a p-value of 0.242, indicating no significant difference. Moderate heterogeneity (I² = 41.2%) was observed, reflecting some consistency among studies. The Warm Compression subgroup (3 studies) had a pooled SMD of −0.446 (SE = 0.155), with a significant p-value (p = 0.004), suggesting LipiFlow was superior to warm compression in reducing OSDI scores. However, heterogeneity was also moderate (I² = 42.9%). Key contributing studies include Lane et al. 12 and He et al., 33 which showed strong effects favoring LipiFlow. Overall, heterogeneity was high (I² = 73.2%), reflecting variability in study designs and control treatments.
A sensitivity analysis, as depicted in Figure 4, was conducted to assess the robustness of the meta-analysis results evaluating the SMD in OSDI scores post-LipiFlow treatment compared to control groups. This analysis involved the exclusion of six studies—Gupta et al., Holland et al., Kasetsuwan et al., Park et al., Tauber et al., and Vasudevan et al.—to evaluate their influence on the overall effect size and heterogeneity. Following the removal of these studies, a notable reduction in heterogeneity was observed, indicating that the excluded studies may have contributed to variability in the pooled estimate. Prior to exclusion, the I² statistic suggested moderate heterogeneity; however, post-exclusion, the I² value decreased substantially, reflecting improved consistency among the remaining studies. The effect size remained statistically significant, reinforcing the robustness of the findings and supporting the conclusion that LipiFlow therapy leads to a meaningful improvement in OSDI scores compared to controls. From a clinical perspective, this sensitivity analysis strengthens the evidence supporting LipiFlow as an effective intervention for managing OSD. By demonstrating that the treatment effect persists even after removing potentially influential studies, the findings reinforce the reliability of LipiFlow as a therapeutic option. The reduction in heterogeneity also suggests that the included studies share a more homogeneous patient population and methodology, thereby improving the generalizability of the results to clinical practice.
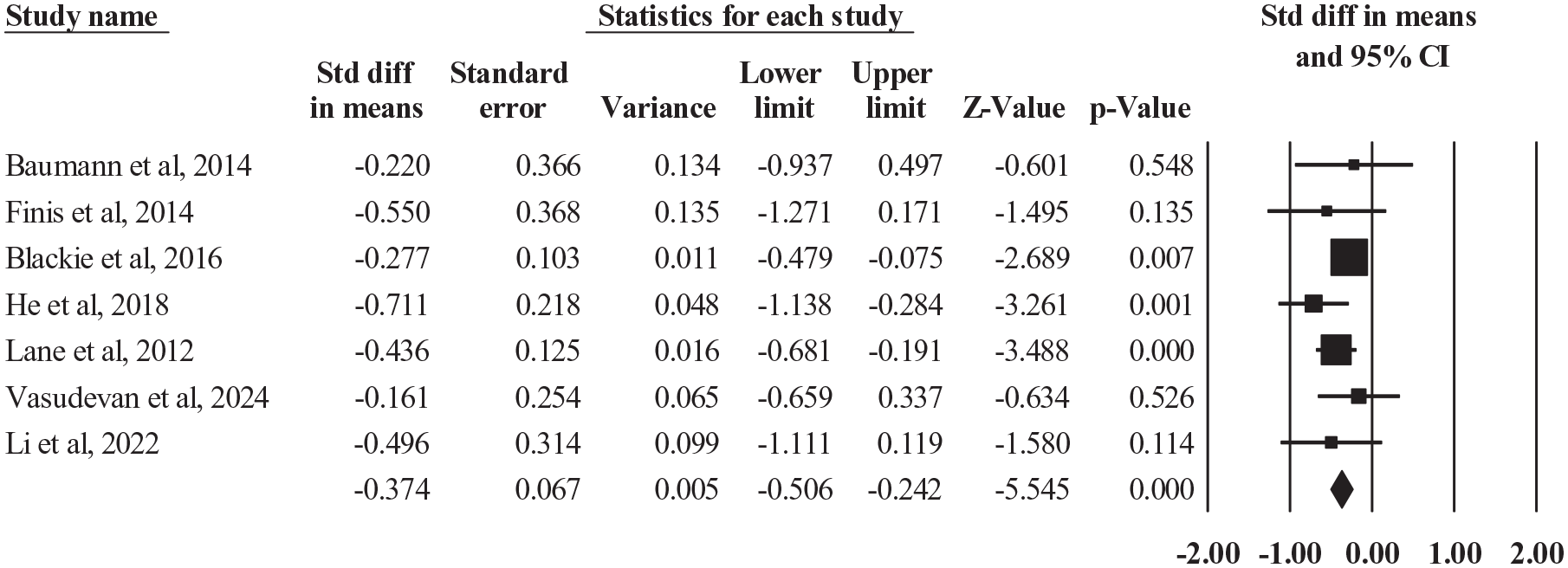
Sensitivity analysis on the OSDI outcome.
Meibomian glands yielding secretion score
An analysis of 12 studies evaluated the MGYSS, a crucial indicator of meibomian gland functionality. The meta-analysis revealed a statistically significant enhancement in MGYSS when using the thermal pulsation system (LipiFlow) compared to alternative treatments. The calculated pooled SMD was 0.449 (95% CI: 0.173–0.725), with a p-value of 0.001, signifying a considerable positive effect (Z = 3.187; Figure 5). Nevertheless, substantial heterogeneity was observed among the included studies, as evidenced by an I² value of 78.49%, indicating high variability in outcomes. The heterogeneity p-value was also statistically significant (p = 0.001), suggesting that differences among studies, potentially due to variations in methodology, patient groups, or treatment protocols, influenced the results (Supplemental Table 2). Despite this high heterogeneity, the notable improvement in MGYSS suggests that the thermal pulsation system effectively enhances meibomian gland function, which is essential for addressing dry eye symptoms and improving overall ocular surface health.
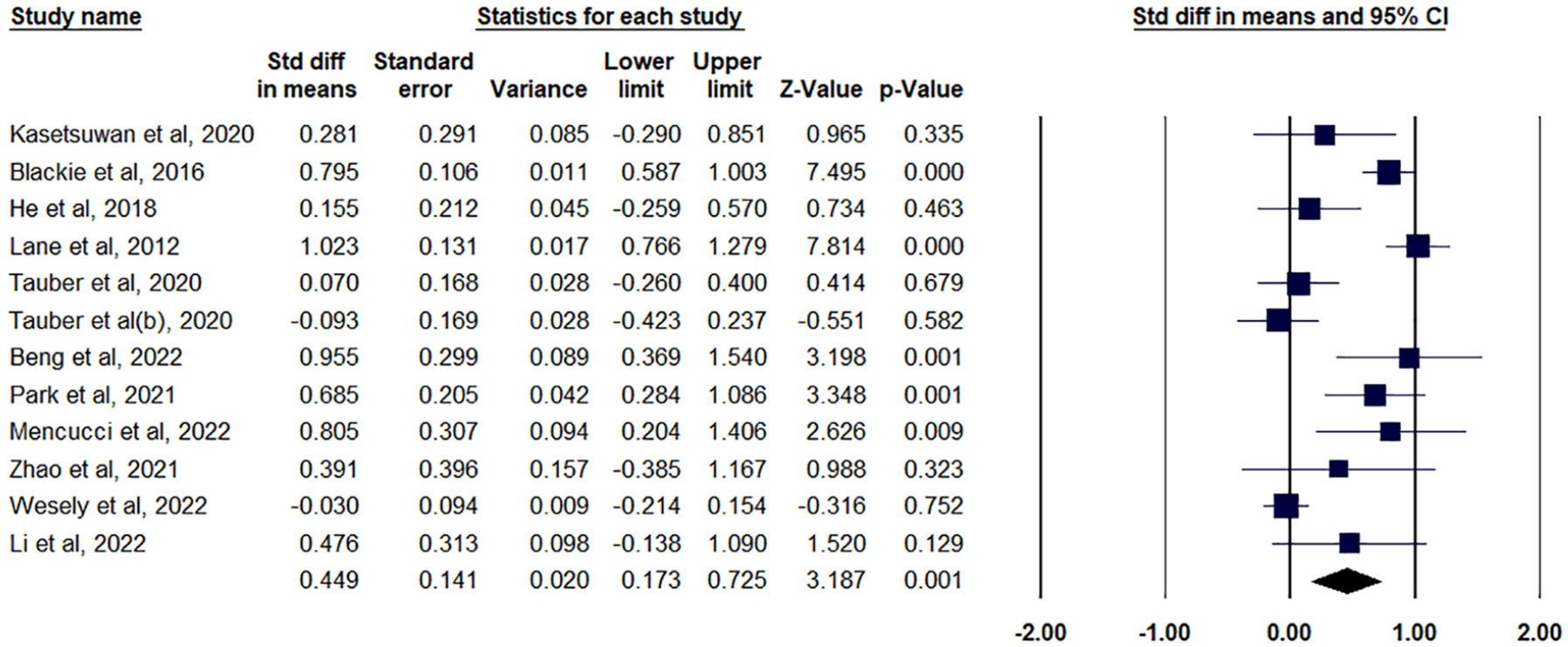
Forest plot for MGYSS outcome.
Tear break-up time
The meta-analysis in Figure 6 shows the SMD in TBUT following LipiFlow treatment versus control groups included 11 studies, yielding a pooled effect size of 0.211 (95% CI: 0.106–0.315, p < 0.0001). This suggests a statistically significant improvement in TBUT favoring LipiFlow treatment. The heterogeneity was low (Q = 5.778, p = 0.834, I² = 0%), indicating high consistency across studies. Both fixed- and random-effects models yielded identical results, reinforcing the robustness of the findings. Among the major contributing studies, Park et al., 39 and He et al. 33 showed relatively larger effect sizes, while Zhao et al. 43 and Kasetsuwan et al. (2020) contributed less due to smaller effect sizes or negative values. The consistency across studies suggests a reliable treatment effect with LipiFlow improving TBUT, a crucial indicator of tear film stability in dry eye disease. Clinically, the findings support LipiFlow as an effective intervention for MGD-related dry eye, particularly in patients unresponsive to conventional therapies. Given the low heterogeneity and significant effect size, LipiFlow may be a viable option for improving tear film stability and patient-reported symptoms, reinforcing its role in evidence-based management of MGD.

Forest plot for TBUT outcome.
Figure 7 shows the meta-analysis on the SMD of LipiFlow versus control in improving TBUT. The analysis is categorized into three subgroups based on the type of control: Other Device, Placebo, and Warm Compression. The “Other Device” subgroup, with five studies, yielded an SMD of 0.189 (95% CI: 0.069–0.308, p = 0.002), showing a statistically significant improvement with LipiFlow. Heterogeneity was low (I² = 0, p = 0.523), suggesting consistency across studies. Key contributors include Baumann and Cochener 28 and Lane et al. 21 . The “Placebo” subgroup (three studies) showed a higher effect size (SMD = 0.262, 95% CI: −0.037 to 0.560), though statistical significance was not reached (p = 0.086). Heterogeneity was also low (I² = 0, p = 0.378). Park et al. 38 contributed notably to this group. The “Warm Compression” subgroup (three studies) demonstrated the highest effect size (SMD = 0.305, 95% CI: −0.009 to 0.619), with marginal significance (p = 0.057). Again, heterogeneity was low (I² = 0, p = 0.981). Key studies include Finis et al. 31 and Meng et al. Overall, LipiFlow consistently showed a positive effect on TBUT regardless of control type, with minimal heterogeneity, supporting its efficacy in improving tear film stability.
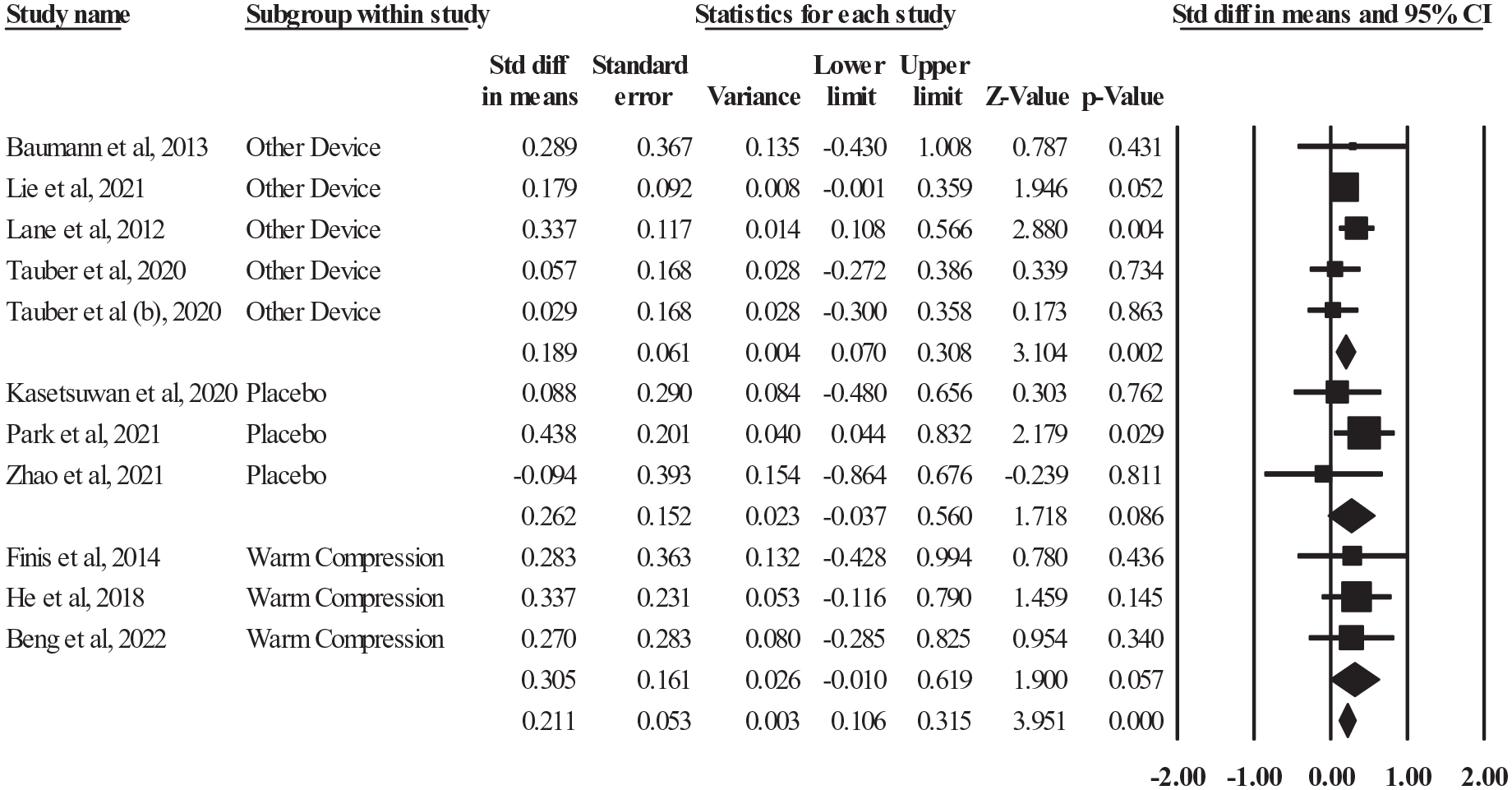
Subgroup analysis on the TBUT outcome.
Corneal fluorescein staining
An analysis of six studies examining corneal fluorescein staining (CFS), a key indicator of ocular surface damage, was conducted. The results of the meta-analysis showed a statistically significant decrease in CFS scores after treatment with the Lipiflow thermal pulsation system compared to control treatments. The combined SMD was calculated as −0.130 (95% CI: −0.248 to −0.012), with a p-value of 0.031, demonstrating a small but notable improvement (Z = −2.162; Figure 8), Notably, the included studies showed no significant heterogeneity, as evidenced by an I² value of 0% (p = 0.031), suggesting consistency across the research (Supplemental Table 4). This uniformity strengthens the reliability of the findings, indicating that the thermal pulsation system consistently enhances ocular surface health by reducing corneal damage as measured by CFS. The statistically significant reduction in CFS scores implies that thermal pulsation may be an effective method for mitigating ocular surface damage, potentially leading to improved overall eye health in individuals suffering from DES and MGD.

Forest plot for CFS outcome.
Lipid layer thickness
Three distinct investigations examined LLT, a key component in assessing tear film stability. A meta-analysis of these studies found no significant difference in LLT between the thermal pulsation system (LipiFlow) and other treatments, including placebo, warm compresses, or alternative thermostatic devices. The analysis produced a combined SMD of −0.071 (95% CI: −0.381 to 0.239), with a p-value of 0.653, indicating no statistically significant effect (Z = −0.45; Figure 9). The studies showed consistency, as demonstrated by an I² value of 0% (p = 0.653), suggesting a lack of heterogeneity among the included research (Supplemental Table 5). The absence of a substantial change in LLT suggests that while thermal pulsation may provide advantages for other clinical outcomes, it does not appear to significantly affect the lipid layer thickness of the tear film in patients with DES or MGD, according to the current research available.
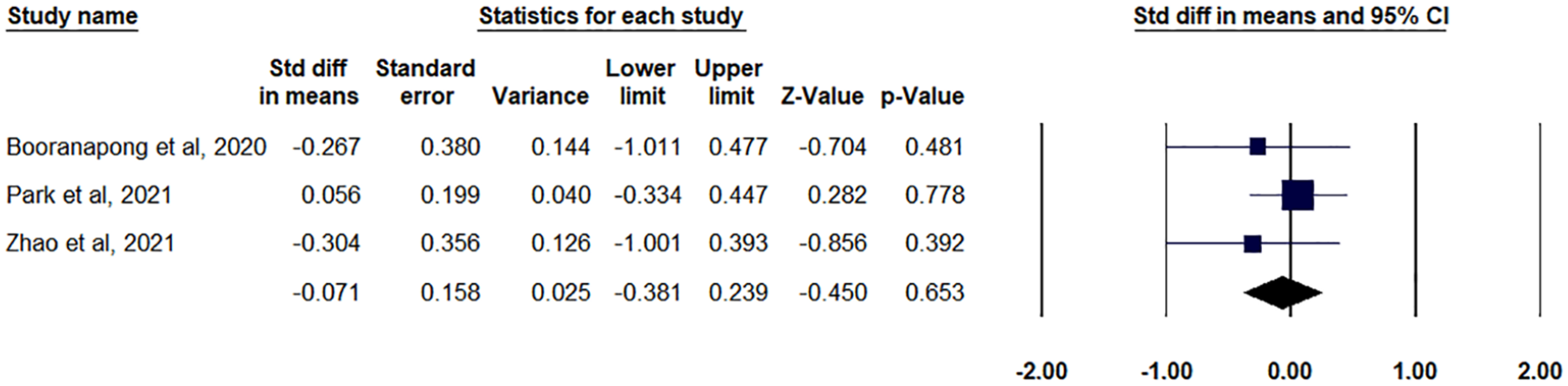
Forest plot for LLT outcome.
Publication bias and quality assessment
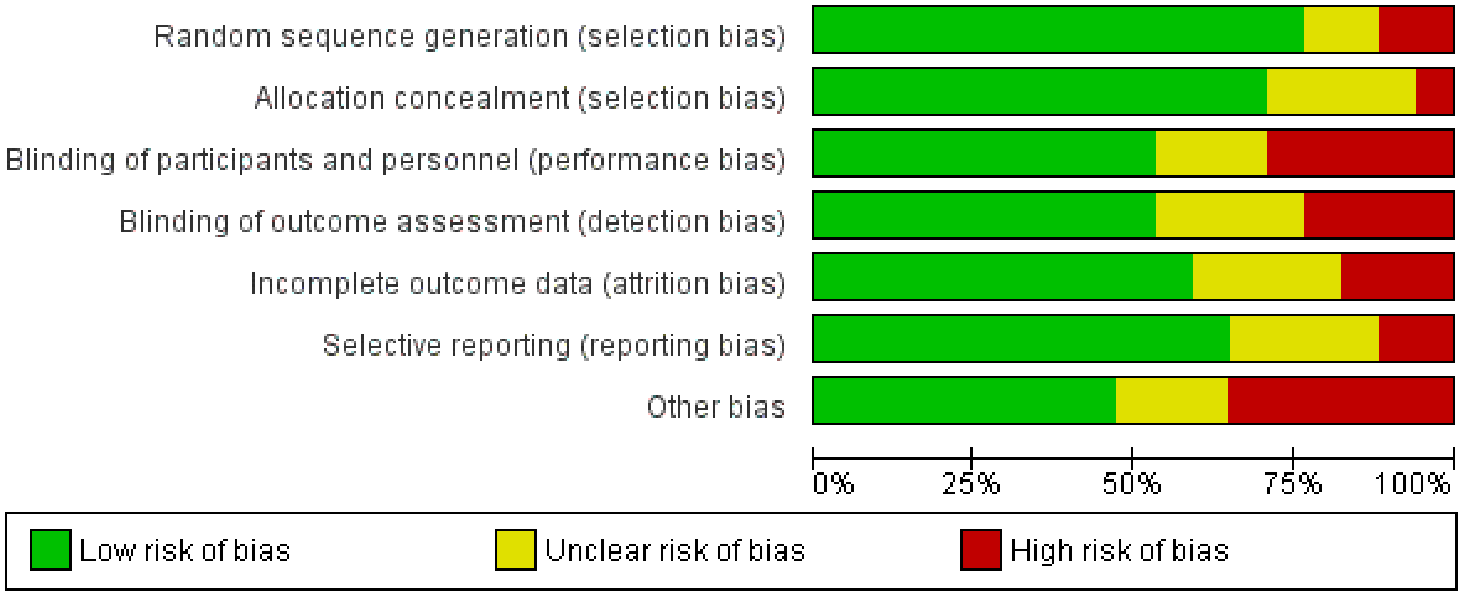
To ensure the reliability and validity of the results, a systematic assessment of publication bias and risk of bias was conducted across the included studies. Funnel plots were employed to evaluate publication bias, and the absence of significant asymmetry suggested a low probability of bias resulting from selective reporting of positive outcomes (Supplemental Figures 1–3). Nevertheless, the potential underrepresentation of smaller studies with less significant findings could still influence overall effect estimates. The evaluation of risk of bias utilized established tools such as the Cochrane Risk of Bias tool, examining crucial domains including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting. The majority of studies were classified as having low to moderate risk of bias, particularly in areas related to blinding and randomization. However, some studies exhibited high risk of bias, especially in the blinding of participants and outcome assessors, given that many trials relied on subjective measures like symptom questionnaires. A few studies also raised concerns regarding incomplete outcome data and selective reporting, which could affect the interpretation of results. While most studies demonstrated acceptable methodological quality, the presence of bias in some studies necessitates a cautious approach when interpreting the findings (Figures 10 and 11).
Risk of bias summary: authors’ judgments about each item of the risk of bias assessment for every included study.

Risk of bias graph: authors’ judgments about each item of the risk of bias assessment presented as percentages among all included studies.
Discussion
DES and OSD have been increasingly linked to MGD.44,45 In response, a novel treatment called thermal pulsation therapy (LipiFlow) has been introduced to restore gland function through the application of regulated heat and mechanical force.46,47 Unlike traditional methods such as warm compresses, which provide temporary alleviation, the thermal pulsation system has demonstrated improved long-term results by directly clearing obstructed meibomian glands, enhancing tear stability, and diminishing symptoms.48,49 This systematic review and meta-analysis aimed to assess the effectiveness and safety of the thermal pulsation system (LipiFlow) in comparison to placebo, warm compresses, or alternative thermostatic devices. The study evaluated clinical outcomes including the OSDI, TBUT, MGYSS, CFS, and LLT. Studies varied in their methods of randomization and allocation concealment, which could introduce selection bias. Some trials implemented strict masking protocols for examiners evaluating clinical signs, whereas others lacked detailed reporting on blinding procedures. Given these inconsistencies, the risk of bias in subjective outcomes was higher compared to objective measures. This highlights the importance of carefully interpreting patient-reported symptom improvements and considering comparator types when evaluating treatment efficacy. To further assess the impact of these biases, we conducted subgroup analyses to evaluate differences in OSDI and TBUT outcomes based on comparator type. These analyses provide additional context for understanding the variability in study results and reinforce the need for future studies with enhanced blinding methodologies where feasible.
The systematic review examined studies evaluating various key clinical outcomes to assess the efficacy of thermal pulsation therapy for DES and MGD management. Results indicate that while the LipiFlow device offers certain advantages, particularly in improving meibomian gland function (measured by MGYSS) and ocular surface health (indicated by CFS), it does not demonstrate significant superiority over control treatments in some aspects, including TBUT and LLT. Notably, no substantial improvement was observed in the OSDI, a patient-reported measure of symptom intensity. Conversely, thermal pulsation treatment was linked to significant enhancements in the MGYSS, directly reflecting improved meibomian gland functionality. Furthermore, CFS showed marked improvement, suggesting reduced ocular surface damage post-treatment. However, the lack of significant changes in TBUT or LLT may indicate limitations in the thermal pulsation system’s capacity to enhance overall tear film stability for some individuals.
The minimal OSDI improvement implies that thermal pulsation may alleviate certain dry eye clinical signs but might not adequately address patients’ subjective symptoms. OSDI, a patient-reported outcome measure, indicates dry eye symptom severity, including discomfort, visual disturbance, and treatment necessity.50 –52 This finding could stem from the complex, multifactorial nature of DES, with MGD being only one facet. Persistent tear hyperosmolarity, inflammation, and neural dysfunction may continue causing OSD symptoms despite meibomian gland function restoration.53 –55 Furthermore, psychological factors and patient expectations can influence perceived symptom relief, complicating OSDI result interpretation. TBUT assesses tear film stability, with shorter TBUT indicating faster evaporation and instability. 56 Despite thermal pulsation’s aim to improve meibomian gland function and stabilize the lipid layer, the lack of significant TBUT improvement may result from persistent issues in other tear film components, such as the aqueous or mucin layers, which can limit TBUT enhancement even when LipiFlow addresses the lipid layer.57,58 TBUT outcomes are also influenced by environmental conditions and the timing of post-treatment measurements. The significant improvement in MGYSS following thermal pulsation therapy highlights its effectiveness in improving meibomian gland function, which is essential for producing the lipid layer that prevents evaporation and stabilizes the ocular surface. Thermal pulsation therapy’s targeted action addresses the underlying pathophysiology of MGD by liquefying and expressing meibum from blocked glands, aligning with previous studies demonstrating sustained gland function improvements post-treatment.
Several studies have evaluated the utilization of LipiFlow treatment, particularly focusing on its impact on MGD and related outcomes.39,59 One significant observation from these studies is that LipiFlow appears to positively influence meibomian gland function. Specifically, the severity of MGD at baseline was found to correlate with greater improvements in MGYLS and the quality of meibum at three months. This suggests that individuals with more severe MGD may experience a more pronounced benefit from LipiFlow treatment, likely due to the restoration of normal tear film stability and improved ocular surface conditions. By addressing MGD early, LipiFlow potentially reduces the risk of discomfort and enhances overall recovery, offering a preventive approach to managing ocular surface complications. 60
Greiner et al. 23 reported that the LipiFlow Thermal Pulsation System represents a significant technological advancement in managing dry eye disease caused by MGD. Their study demonstrated that a single 12-min LipiFlow treatment delivers sustained improvement in meibomian gland function, tear break-up time, and dry eye symptoms for up to 9 months—results that surpass those of existing therapies for dry eye disease. This prolonged efficacy highlights LipiFlow’s potential to redefine the treatment landscape for this challenging condition.
This comprehensive review and statistical analysis offer an in-depth assessment of the thermal pulsation system’s effectiveness across various clinically significant outcomes. The study’s robustness is evident in its strict adherence to MOOSE and PRISMA guidelines, ensuring a methodical and clear approach to data gathering, examination, and presentation. The inclusion of RCTs, considered the pinnacle of clinical research, bolsters the credibility of the results. Furthermore, the evaluation of multiple outcome measures provides a wide-ranging assessment of both subjective and objective aspects of DES and MGD, shedding light on the impact of thermal pulsation therapy on different aspects of the condition. The use of SMDs to compare outcomes across studies is another strength, enabling meaningful comparisons despite variations in the scales and tools used to measure clinical outcomes. Additionally, the application of a random-effects model in the analysis accounted for potential inter-study variability, ensuring that the pooled results could be applied to a wider patient population.
While this meta-analysis has its merits, it also faces several constraints. A key limitation is the considerable heterogeneity found in certain outcomes, particularly OSDI. Although a sensitivity analysis was employed to address this variability, the heterogeneity may still restrict the broader applicability of the results and decrease the accuracy of the combined estimates. Factors contributing to this heterogeneity could include variations in study methodology, subject groups, follow-up periods, and treatment protocols, all of which may impact the outcomes. Moreover, the analysis of some outcomes, such as LLT and CFS, included a relatively small number of studies, potentially compromising the reliability of the findings and increasing the risk of publication bias. Blinding posed a significant challenge in studies comparing LipiFlow to other treatments, particularly warm compresses and other active interventions. While outcome assessors could be masked for objective measures such as TBUT and MGYSS, OSDI remained susceptible to bias since participants could not be blinded to their assigned intervention. This inherent limitation may have influenced subjective symptom reporting and contributed to variations in OSDI outcomes across studies. Another drawback is the dependence on published research, which may introduce bias since studies with positive outcomes are more likely to be disseminated than those with neutral or negative results. Despite attempts to locate unpublished studies and gray literature, it’s possible that some relevant data were overlooked, potentially distorting the results. Additionally, the short follow-up durations in the included studies make it challenging to evaluate the long-term effectiveness and safety of thermal pulsation therapy. Further research with extended observation periods is necessary to determine if the short-term benefits persist over time.
Subsequent investigations should aim to address the limitations identified in this study, particularly by conducting more extensive and prolonged research with larger participant groups to better evaluate the long-term effectiveness of thermal pulsation therapy. Researchers should also examine the influence of individual patient characteristics, such as the initial severity of MGD, concurrent eye conditions, and the existence of systemic illnesses, to determine which groups are most likely to respond positively to the treatment. Moreover, future studies could investigate the potential complementary effects of combining thermal pulsation therapy with other treatments, like anti-inflammatory drugs or tear film stabilizers, to improve outcomes. Investigating the cellular mechanisms responsible for the effects of thermal pulsation on meibomian gland function and tear film stability could offer valuable insights for refining treatment protocols and developing novel therapeutic approaches.
Conclusion
Our meta-analysis reveals mixed findings regarding the effectiveness of the thermal pulsation system (LipiFlow) for MGD and dry eye. While no significant improvements were observed LLT scores, LipiFlow demonstrated a statistically significant enhancement in MGYSS (SMD = 0.449, p = 0.001), a reduction in CFS scores (SMD = −0.130, p = 0.031) and TBUT (SMD = 0.211 seconds, p < 0.0001). The OSDI showed significance in sensitivity analysis (SMD = −0.374 p < 0.0001) of which future research is warranted. High heterogeneity was noted in MGYSS outcome, reflecting variability across studies. Consistency in OSDI, TBUT, CFS and LLT results strengthens reliability. Despite concerns about publication bias, these findings highlight LipiFlow’s potential to improve meibomian gland function and ocular surface health. While its short-term efficacy is evident, further research is required to assess long-term benefits and to identify specific patient populations most likely to benefit from this therapy.
Supplemental Material
sj-docx-1-oed-10.1177_25158414251338775 – Supplemental material for Is a thermal pulsation system (LipiFlow) effective as a standalone treatment for meibomian gland dysfunction and dry eye? A systematic review and meta-analysis
Supplemental material, sj-docx-1-oed-10.1177_25158414251338775 for Is a thermal pulsation system (LipiFlow) effective as a standalone treatment for meibomian gland dysfunction and dry eye? A systematic review and meta-analysis by Kai-Yang Chen, Hoi-Chun Chan and Chi-Ming Chan in Therapeutic Advances in Ophthalmology
Supplemental Material
sj-docx-2-oed-10.1177_25158414251338775 – Supplemental material for Is a thermal pulsation system (LipiFlow) effective as a standalone treatment for meibomian gland dysfunction and dry eye? A systematic review and meta-analysis
Supplemental material, sj-docx-2-oed-10.1177_25158414251338775 for Is a thermal pulsation system (LipiFlow) effective as a standalone treatment for meibomian gland dysfunction and dry eye? A systematic review and meta-analysis by Kai-Yang Chen, Hoi-Chun Chan and Chi-Ming Chan in Therapeutic Advances in Ophthalmology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.