
Abstract
Background:
Rhegmatogenous retinal detachment (RRD) with macular involvement is a sight-threatening condition. Silicone oil (SO) is efficacious for retinal tamponade, especially in complex cases. Whether macular detachment per se or the potential tamponading agent may affect macular microcirculation after RRD repair is a matter of research.
Objectives:
To investigate macular microcirculation changes using optical coherence tomography angiography (OCT-A) after pars plana vitrectomy (PPV) with intravitreal SO for RRD repair in the early posttreatment period.
Design:
Prospective comparative cross-sectional study.
Data sources and Methods:
Fourteen eyes of 14 patients were included in the study. All eyes underwent a single successful PPV with SO tamponade for macula-off RRD. OCT-A was performed to analyze macular microcirculation and visual outcomes at 1 month postoperatively. The fellow unaffected eye was used as control.
Results:
Vessel density (VD) in the superficial capillary plexus (SCP) was significantly lower at each macular region (fovea, parafovea, and perifovea) of SO-treated eyes compared with the fellow eyes (all p = 0.001). Similarly, perfusion density (PD) in the SCP was significantly lower at each macular region than the fellow eyes (all p = 0.001). There was enlargement of foveal avascular zone (FAZ) area and decrease of circularity at RRD eyes compared with the fellow ones (all p = 0.001). Postoperative logMAR visual acuity (VA) was significantly lower in treated eyes than fellow eyes and correlated inversely with foveal, parafoveal, and perifoveal VD and PD SCP (all p < 0.001). Postoperative VA had no correlation with FAZ parameters.
Conclusion:
Enlargement of FAZ SCP and decrease in VD and PD SCP during the short-term follow-up were possibly attributable to ischemic changes in the macular area after RRD repair with SO tamponade. In this preliminary study, the flow density in macular capillary plexus may represent an indicator of visual outcomes.
Keywords
Introduction
Rhegmatogenous retinal detachment (RRD) is characterized by separation of the neurosensory retina from the retinal pigment epithelium (RPE) due to vitreous fluid subretinal accumulation through a retinal tear or hole. 1 In cases that RRD involves the macula preoperatively, macular detachment is one of the leading causes for guarded visual prognosis even after successful reattachment surgery. 2 The primary anatomical success rates for RRD repair by pars plana vitrectomy (PPV) have been found to range from 64% to 96%, with a wider range of outcomes for final visual acuity (VA).3–5 Even after retinal reattachment, functional results are seldom not as expected in a subset of patients. 6 To investigate the etiologies of suboptimal visual recovery after RRD repair, various parameters have been speculated.7–10
Silicone oil (SO) has been widely used as a retinal tamponade, especially in the management of complicated vitreoretinal disorders.11,12 Although efficacious as retinal tamponade in complex cases, intravitreal SO has been associated with potential side effects. Indeed, SO may lead to anterior segment complications and adversely affect retinal function.13–15 In addition to these well-established unfavorable conditions, a proportion of patients suffer from unexplained visual loss after RRD repair with SO tamponade. Possible explanations for these phenomena include SO-related retinal toxicity, inner retinal layer alterations, or retinal electrolyte homeostasis dysregulation.14–16 Advanced imaging techniques for retinal microstructure and microcirculation evaluation have been introduced for enhanced investigation of the causes of incomplete visual recovery after successful surgery. Optical coherence tomography angiography (OCT-A) allows visualization of the retinal and choroidal vasculature using segmentation of each capillary plexus. OCT-A is a precise noninvasive method for examination of the foveal avascular zone (FAZ) parameters and quantification of vessel density (VD) and capillary plexus perfusion density (PD) in the macula area. Recently, few reports investigated OCT-A parameters after RRD repair and correlated those with functional outcomes.17–24
This study sought to characterize macular capillary plexus changes using OCT-A in eyes undergoing PPV and SO tamponade for RRD with macular involvement. Herein, we mention our preliminary results in an effort to understand the potential role of SO on microcirculation changes during the early posttreatment period.
Materials/methods
Study design
The study was conducted at the Department of Ophthalmology of the University of Ioannina, Greece, between March and December 2020.
This was a prospective cross-sectional comparative study. We recruited all consecutive patients who underwent three-port PPV with SO tamponade for macula-off RRD. To be included, patients should have undergone a single successful three-port PPV with SO tamponade for primary RRD with macular involvement. Exclusion criteria consisted of previous ocular surgery other than phacoemulsification, RRD duration of more than 1 month, trauma, co-existent macular and vitreoretinal pathology, or any other ocular or systemic comorbidity that could affect retinal vascular circulation. Moreover, we excluded eyes with postoperative complications including retinal re-detachment, emulsification of SO, secondary glaucoma, epiretinal membrane, macular hole, persistent subretinal fluid, and retinal folds. Finally, we excluded patients if the OCT-A images were of low quality or blurred. The patients’ operated eyes were used as cases, whereas the contralateral unaffected eyes were used as controls.
A comprehensive eye examination was conducted preoperatively. The indication for SO injection was primary RRD, cases with multiple/giant tears, or the presence of proliferative vitreoretinopathy (PVR). Surgical procedures were performed by a single experienced vitreoretinal surgeon (M.S.) with 23-gauge PPV Alcon Constellation® Vision System (Alcon Laboratories Inc, Fort Worth, TX, USA). After core vitrectomy, peripheral vitreous removal with a 360° sclera indentation was performed. The vitreous traction was released from each retinal tear, and PVR membranes, when present, were peeled from the retina surface. The retina was flattened using perfluorocarbon liquid (PFCL). After flattening the retina, endolaser was applied, followed by PFCL/SO (1300 centistokes) exchange. A complete ophthalmological examination including anterior segment and dilated fundus examination with slit-lamp biomicroscopy, VA, and intraocular pressure (IOP) measurement was performed at 1 month postoperatively. At the same time, OCT-A was obtained for all patients in both the operated and fellow unaffected eyes with the latter acting as controls. Detailed OCT-A imaging analysis was conducted based on the protocol described in the following section.
OCT-A imaging protocols and analysis
The scanning area was captured using AngioPlex® OCT Angiography (ZEISS, Jena, Germany). All OCT-A imaging was performed by acquiring a 6 mm × 6 mm scan pattern which was automatically centered on the fovea. Each B-scan contains 350 A-scans; the latter are equally spaced along the horizontal dimension with a separation of 17.1 microns between A-scans. Similarly, 350 B-scan positions are located in the vertical direction, and each B-scan is separated by 17.1 microns. Each B-scan in the 6 mm × 6 mm scanning section is repeated twice at the same position. The device generates en face images of the retinal and choroidal vasculature that are based on automated layer segmentation as performed by OCT-A system software. All the measurements of the investigated parameters were automatically calculated. We examined and analyzed macular capillary plexus characteristics, specifically VD, macular perfusion, and FAZ area in the superficial capillary plexus (SCP). In particular, the region of interest was automatically split into three fields: the foveal area, a central circle with a diameter of 1 mm; the parafoveal area, an inner circle with a diameter of 3 mm; and the perifoveal area, an outer circle of 6 mm. VD and PD SCP were calculated at each region of the 6 mm × 6 mm scan. Concerning FAZ, the area (mm2) and circularity were measured. All OCT-A scans were reviewed to ensure their quality was sufficient (strength index >5/10).
Statistical methodology
Data were imported to IBM SPSS, version 25 (IBM Corp., Armonk, NY, USA), for analysis and interpretation. Continuous variables were expressed as mean with standard deviation and median with interquartile range. Absolute numbers and percentages were used to express categorical variables. Due to the small sample size (N = 14), we used nonparametric tests. We used the Mann–Whitney U test to compare differences between two independent groups. The Spearman coefficient was used to correlate two continuous variables. To investigate the relationship between a continuous and a nominal variable, the Kruskal–Wallis test was used. For all tests, statistical differences were determined to be significant at p < 0.05.
Results
A total of 22 patients were examined. After exclusion criteria, a total of 14 eyes of 14 patients (9 male, 5 female) were included in the analysis. The mean age of the patients was 62.6 years (SD ± 7.2). The mean preoperative macular detachment duration was 8.2 days (SD ± 3.5). The vitreoretinal pathology of the RRD included multiple or giant breaks and the presence of PVR. The baseline characteristics of the patients are shown in Tables 1 and 2. The preoperative characteristics and association with 1-month postoperative data are shown in Table 3.
Preoperative characteristics of macula off RRD eyes treated with silicone oil tamponade.
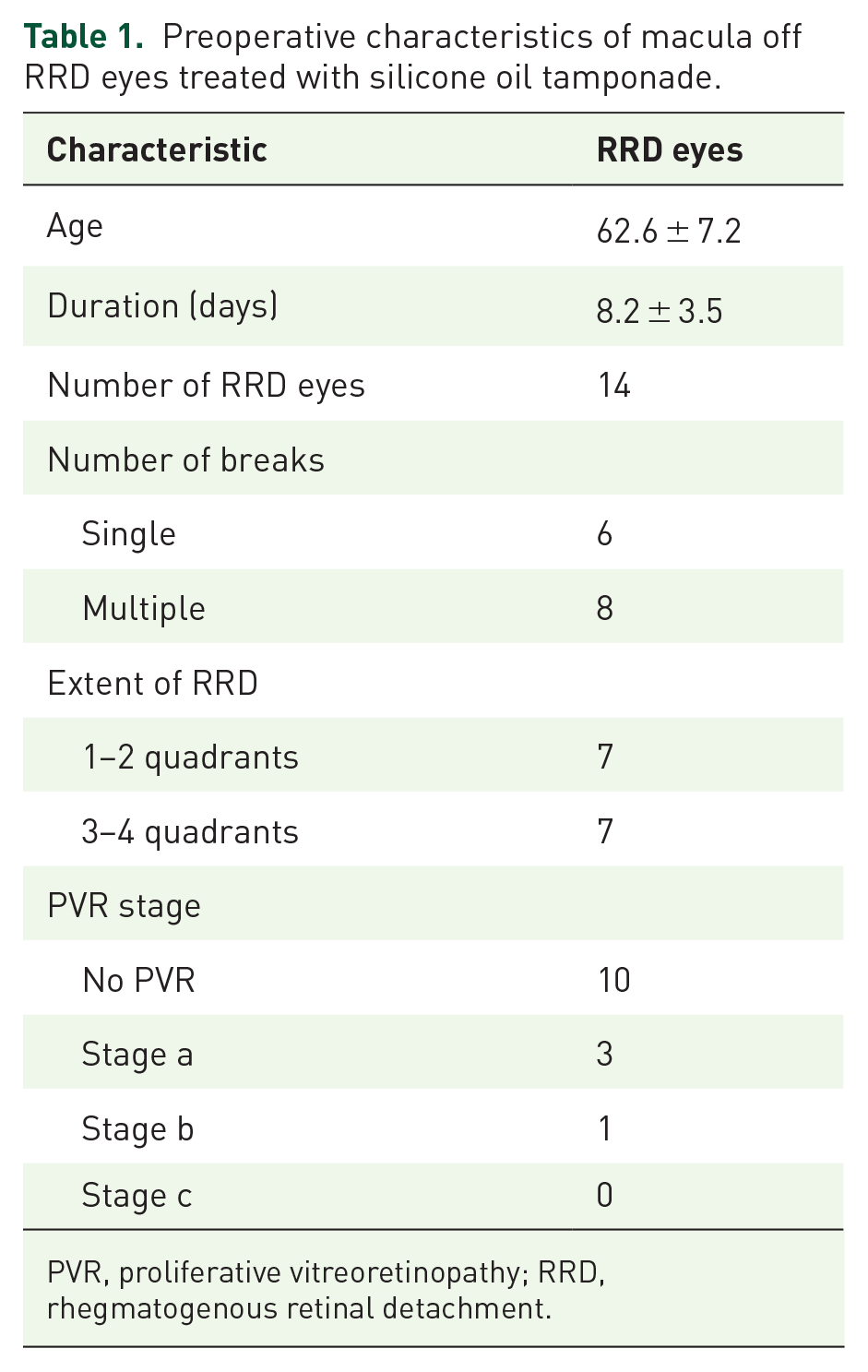
PVR, proliferative vitreoretinopathy; RRD, rhegmatogenous retinal detachment.
Indications for silicone oil tamponade.

PVR, proliferative vitreoretinopathy; RRD, rhegmatogenous retinal detachment.
Preoperative characteristics in macula-off RRD (number of breaks, extent of RRD, PVR stage, all expressed in median) and 1-month postoperative factors [FAZ area (mm2), FAZ circularity, VD (mm/mm2), PD (%), VA (logMAR)].

FAZ, foveal avascular zone; PD, perfusion density; PVR, proliferative vitreoretinopathy; RRD, rhegmatogenous retinal detachment; VA, visual acuity; VD, vessel density.
Mann–Whitney test (number of breaks, extent of RRD) and Kruskal–Wallis test (PVR stage) were used.
At 1 month postoperatively, the mean values of foveal, parafoveal, and perifoveal VD in the SCP were significantly lower in macula-off eyes treated with intravitreal SO than those of the fellow eyes (all p ⩽ 0.001). Similarly, the mean values of foveal, parafoveal, and perifoveal PD in the SCP were significantly lower than those of the fellow eyes (all p ⩽ 0.001). There was a significantly larger mean FAZ area with reduced circularity in macula-off RRD eyes treated with intravitreal SO as compared with the fellow eyes (all p ⩽ 0.001). At 1 month postoperatively, best-corrected VA (logMAR) was significantly lower in RRD eyes treated with vitrectomy and intravitreal SO as compared with the fellow eyes (p ⩽ 0.001), as expected. Detailed information is shown in Table 4 and Figure 1.
One-month postoperative measurements of FAZ area (mm2) and circularity, VD (mm/mm2), PD (%), VA (logMAR).

FAZ, foveal avascular zone; PD, perfusion density; RRD, rhegmatogenous retinal detachment; SD, standard deviation; VA, visual acuity; VD, vessel density.
Pairwise comparisons among RRD and fellow unaffected eyes were conducted with the Mann–Whitney test.

Mean plot of 1-month postoperative OCT-A characteristics in RRD eyes and unaffected fellow eyes. (a) One-month postoperative FAZ area (mm2) and circularity from RRD and fellow eyes. All p ⩽ 0.001. (b) One-month postoperative VD (mm/mm2) in each macular region (outer, inner, central) from RRD and fellow eyes. All p ⩽ 0.001. (c) One-month postoperative FD (%) in each macular region (outer, inner, central) from RRD and fellow eyes. All p ⩽ 0.001.
Correlation analyses revealed that at 1 month after surgery, logMAR VA inversely correlated with VD in the SCP at foveal, parafoveal, and perifoveal area in a significant way (all p ⩽ 0.001). Similarly, there was a significant correlation between postoperative VA and PD in the SCP at each macular region (all p ⩽ 0.001). Concerning FAZ parameters, there was no significant correlation of either FAZ area (p = 0.365) or circularity (p = 0.233) in the SCP with 1-month posttreatment VA. Detailed information is shown in Table 5 and Figure 2. Representative images of FAZ enlargement in RRD treated with intravitreal SO and the fellow unaffected eye are shown in Figure 3.
Correlations of 1-month postoperative OCT-A characteristics with VA.

FAZ, foveal avascular zone; PD, perfusion density; VA, visual acuity; VD, vessel density.
Correlation is significant at the 0.01 level (two-tailed).

Correlation analyses of 1-month postoperative OCT-A characteristics with VA (logMAR). (a) No correlation of VA with 1-month postoperative FAZ area (p = 0.365) and 1-month postoperative FAZ circularity with VA (p = 0.233). (b) Negative correlation of 1-month postoperative VD at each macular region (outer, inner, central) with VA, all p ⩽ 0.001. (c) Negative correlation of 1-month postoperative PD at each macular region (outer, inner, central) with VA, all p ⩽ 0.001.
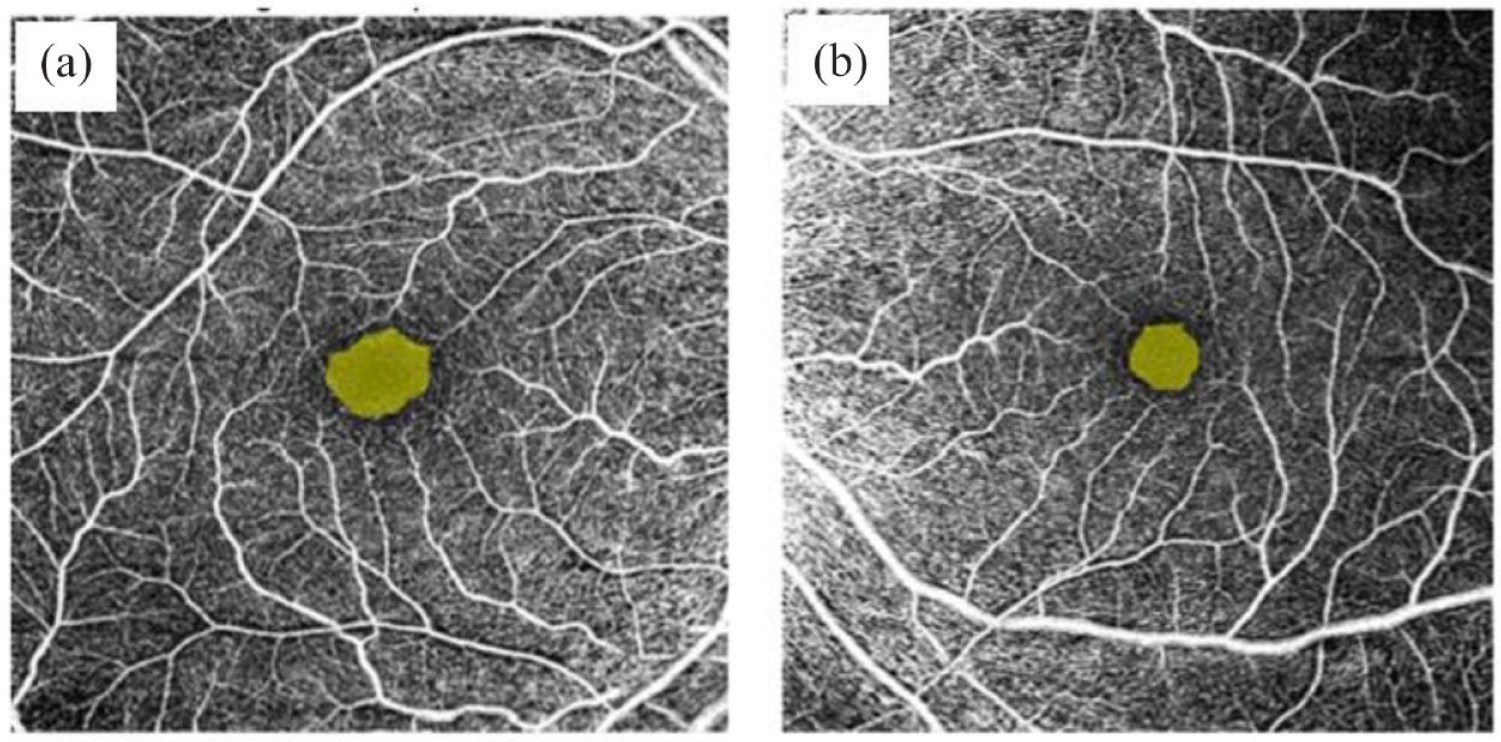
Representative images of foveal avascular zone (FAZ) in OCT-Angiography 6 × 6 mm2 of (a) a patient with rhegmatogenous retinal detachment treated with intravitreal silicone oil, indicating enlargement of FAZ and decreased circularity and (b) the fellow unaffected eye.
Discussion
The trend in current literature is to analyze macular microcirculation changes after RRD repair by performing OCT-A–based studies.17–30 Our study focuses entirely on topographic changes of vascular flow density concerning each separate macular region in cases of macula-off RRD with intravitreal SO. By implementing OCT-A, we primarily assessed any alterations affecting the macular capillary plexus restoration of the SCP regarding changes in FAZ parameters and foveal, parafoveal, and perifoveal VD and PD. We also assessed visual function at 1 month post-vitrectomy. Our preliminary results indicate an enlargement of FAZ with reduced circularity of superficial retina at RRD eyes as compared with the fellow eyes. Furthermore, the diminishment of flow density at each macular region (foveal, parafoveal, and perifoveal area) inversely correlates with postoperative logMAR VA; the decreased vascular flow implies deterioration in visual outcomes.
SO is an efficacious tamponading agent in the management of RRD; albeit, several studies have produced equivocal results concerning its effect on retinal tissue. Unexplained visual impairment, structural, and microcirculation alterations have been widely reported after uncomplicated RRD repair with intravitreal SO.13–16,31 Obviously, many hypotheses could be made about the incomplete restoration of the macula and the deficient functional recovery,32,33 including reduced transfer of oxygen due to the presence of SO, 34 mechanical pressure leading to metabolic retinal derangement, 35 the surgical intervention per se, or the potential of retinal degeneration due to intrinsic SO properties.25–29
Our study demonstrates an enlargement of FAZ SCP accompanied by decreased circularity at 1 month after retinal reattachment as compared with healthy eyes. A number of series have reported changes in FAZ area during the posttreatment period among patients undergoing PPV for RRD, though their results do not serve unequivocal perspectives.17–29 FAZ area at both SCP and DCP following vitrectomy with gas tamponade has been found to be larger in eyes experiencing macular detachment than in eyes without detached macula. 24 An enlargement in postoperative FAZ of both SCP and DCP has been reported after macula-off RRD repair until 3 months after vitrectomy.20,24,36 However, some authors did not detect microvasculature changes concerning FAZ area of RRD-treated eyes when comparing them with healthy cases during long-term observation (up to 12 months), possibly due to recovery of early morphologic alterations.21,22,37,38 Lee et al. 28 were the first to evaluate foveal microvasculature as seen on OCT-A after RRD repair with SO suggesting a correlation between the duration of tamponade and DCP FAZ enlargement, while they did not mention any SO-related effect on the SCP FAZ. Their observation about SCP FAZ area being stable in SO-filled eyes after vitrectomy was further confirmed by the studies of Xu et al. 25 and Roohipoor et al. 26 On the contrary, DCP seems to be affected most, leading to FAZ enlargement in a series of studies. These findings support the hypotheses that SCP is less vulnerable to hypoxia as it is directly connected to retinal arterioles and may have a higher perfusion pressure than the DCP, which may experience extensive morphologic changes due to lower oxygen saturation nearby the watershed zone.39–44 Nonetheless, Maqsood et al. 29 reported a larger FAZ area in SCP of SO-filled eyes compared with DCP, possibly attributable to the longer preoperative duration of macular detachment than that of former studies (20.5 and 10 days in Maqsood’s and Roohipoor’s study, respectively).29,36 In our present study, the FAZ SCP was significantly larger along with diminished circularity in macula-off eyes treated with SO than the fellow eyes at 1 month after operation. Our findings could imply vascular insufficiency in eyes with SO tamponade, which could reflect potential ischemic changes to retinal capillary plexus in the macula, including fovea, parafoveal, and perifoveal area despite relatively expeditious surgery (within 8.2 days from presentation). As proved by recent studies, there is no definite implication of SO for alterations of FAZ SCP,25–28 while it may progressively lead to deformation of FAZ DCP. As the use of SO as a tamponade seems to affect the vascular integrity especially of the DCP, 28 we could hypothesize that FAZ SCP distortion could be attributed to ischemic changes of macular detachment itself even in cases that were operated promptly.
Recently, studies have reported postoperative changes of blood flow density in retinal and choroidal circulation in macula-off RRD as examined by OCT-A.17–30 In this study, we assessed macular capillary plexus rehabilitation of the SCP, especially VD and flow density at foveal, parafoveal, and perifoveal area. Our results indicated a deterioration of VD and PD in each macular region as compared with the fellow eyes. There have been few reports evaluating vascular blood flow in macula-off eyes treated with vitrectomy and gas tamponade or scleral buckling.17–24 A comprehensive assessment of macular capillary density index has provided objective evidence of reduction in vasculature after RRD. 20 Concerning the parafoveal flow density in retinal layers and choriocapillaris, macula-off eyes have demonstrated decreased perfusion values at 2 weeks postoperatively 18 with a gradual partial recovery over a 6-month follow-up period.19,37 A series of hypotheses could be made concerning the etiology of parafoveal VD reduction: (1) activation of Muller cells due to inflammation seems to be connected with local blood flow changes in the inner retina, secondary leading to decreased blood flow 45 and (2) SRF consists of an increased level of inflammatory and vascular mediators due to insufficient supply of oxygen from CCP which may lead to vascular changes in retinal capillary plexuses.41,44,45 Concerning cases treated with intravitreal SO, limited results have been mentioned in literature.25–29 As stated by Roohipoor et al., 26 vascular density of parafoveal SCP and total retina was decreased post-vitrectomy in eyes treated with intravitreal SO. Similarly, Angelova 46 showed a deterioration of vascular density values of the SCP of SO-filled eyes. The results of these studies26,46 indicate that their cohorts did not experience vascular recovery at the posttreatment period to the degree that gas-filled eyes did, possibly due to SO tamponade. Besides, alterations in retinal microcirculation using Doppler laser scanning have been proven at 1 to 3 days post-vitrectomy with SO, still persistent at 1 month, even in macula-on cases. 32 We should speculate that prohibited penetration of oxygen into the vitreous seems to occur in eyes with intravitreal SO producing macular microcirculation changes after 1 month of SO use. 33 Obviously, SO tamponade for more than 9 months seems to result in more evident retinal arterial and venous changes. 47 Contrary to the former studies,26,46 Lee et al. 28 showed no difference in the SCP VD between eyes treated with PPV and intravitreal SO and normal eyes at 3 months after SO was removed. Regarding postoperative VD in foveal, parafoveal, and perifoveal area, our study outcomes are in agreement with some previous findings.25–29 Especially, our results demonstrate a diminishment of vascular density and perfusion at each macular region of SO-treated eyes as compared with the fellow eyes at 1 month after vitrectomy. Concerning foveal VD, the outcomes of previous studies have stirred controversy. Specifically, few studies have confirmed decreased VD, 21 whereas others could not detect significant changes in foveal capillary plexus.19,26 A possible explanation of undetected alterations could be that the fovea is relatively devoid of vessels making small changes difficult to identify. Moreover, the contour of the foveal pit falls below the SO–retina interface potentially protecting it from direct SO contact. 26 In our series, however, we could confirm a decrease of VD in the fovea region. The latter may either be attributable to the effect of SO on retinal tissue or it may suggest that fovea vascularity is susceptible to ischemic tissue damage feasibly caused by macular detachment itself.
An emerging body of evidence has widely indicated postoperative variability of OCT-A changes in FAZ area, VD and PD in retinal and choroidal layers that manifest a potential association with functional outcomes after successful operation.17–30 Interestingly, the quantitative analysis on this subject has produced disputable results. In this study, we thoroughly assessed any changes in SCP in each macular region (fovea, parafovea, perifovea) to identify a potential relationship to VA post-vitrectomy. Recently, OCT-A–based studies indicated that RRD eyes undergoing vitrectomy with gas tamponade have demonstrated an enlargement of SCP FAZ consequently leading to poor visual recovery,21,24,48 although this association was not confirmed by all reports.17,36,38 Concerning eyes treated with intravitreal SO, anatomical alterations in DCP FAZ may imply the postoperative VA; 25 however, the latter has not been confirmed so far for any findings of SCP FAZ in SO-filled eyes at each time point up to 3 months postoperatively.25,29 Similar to previous results, in this study, we could not confirm any obvious association of VA at 1 month post-vitrectomy with either FAZ enlargement or circularity at superficial retina of SO-treated eyes.
We further evaluated the potential of visual recovery in relation to any changes in VD restoration regarding each macular region. Previous studies have reported microvasculature and morphologic alterations with possibility of unsatisfying visual prognosis in RRD with macular involvement. The outcomes of the studies remain unclear, albeit. 30 Despite some studies could not confirm any correlation between VA and superficial VD values during the posttreatment period, 48 others have provided evidence of this association.21,36 Of note, restoration of deep retinal plexus and choriocapillaris seems to better correlate with functional outcomes.18,21,22,37 Our results herein imply that decreased values of SCP flow density at each macular region are associated with impaired VA at 1 month postoperatively. One could hypothesize that due to the central part of the fovea being more densely populated by cone photoreceptors than the periphery, each region would be affected in a different way reflecting diversity of functional recovery. 49 Nonetheless, function of photoreceptors seems to negatively correlate with microcirculation in a significant way in both foveal and eccentric regions of the macula.
An interesting point that should be underlined is that we analyzed separately each macular region (fovea, parafovea, perifovea), unlike previous studies in literature that mainly included foveal and parafoveal area. This detailed analysis along with the prospective design may add strength to our study. Inevitably, a limitation is that we investigated the OCT-A parameters of FAZ, VD, and PD only in the SCP. We should consider that OCT-A imaging artifacts, especially in cases with SO tamponade, may interfere with precise evaluation of retinal microvasculature; this restriction, however, mainly pertains to the imaging of the deep layer. Another potential limitation may be considered that each patient’s healthy fellow eye was used as control. We acknowledge the fact that eyes undergoing vitrectomy with gas tamponade would be a more appropriate group of controls. Nonetheless, in this case, the control group would comprise eyes of different patients, possibly with inter-eye physiological differences. Besides, fellow eyes have been used as controls in former studies. Finally, we should definitely mention the small sample size attributable to precise and strict inclusion criteria and the relatively short-term follow-up design to assay the macular OCT-A characteristics. Despite this small sample size enabled the detection of significant alterations, further study with additional participants is needed to confirm these preliminary results. Obviously, our patients were examined shortly after vitrectomy, thus our results may not accurately portray the OCT-A parameters over the long term. It would be of great importance to further follow up patients after SO removal to detect any alterations.
In conclusion, this study points out the short-term changes in SCP of eyes treated by vitrectomy with intravitreal SO for macula-off RRD. The data of our study indicate a deterioration of vascular density in SO-treated eyes, which may in turn imply the postoperative visual outcomes. Conceivably, further studies may unequivocally indicate whether potential vascular insufficiency in SO-filled eyes is attributable to tissue hypoxic changes due to macular detachment per se or the effect of SO on the retina.
Footnotes
Ethics statement
Approval from the institutional ethics committee was received (Scientific Board of University Hospital of Ioannina, 5/26-03-2020, θ.31). The investigation adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from the participants. All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data sets generated during and/or analyzed during this study are not publicly available due to patients’ confidentiality agreements but are available from the corresponding author on reasonable request.