
Abstract
Central serous chorioretinopathy (CSCR) is a common chorioretinal disease characterized by serous retinal detachment that most commonly involves the macular region. Although the natural history of the acute form shows a self-limiting course, a significant number of patients suffer from recurrent episodes leading to chronic disease, often leaving patients with residual visual impairment. Visual morbidity is often worsened by a delay in the diagnosis due to the incorrect understanding of the particular biomarkers of the disease. The aim of this review is to provide clinical understanding of the biomarkers of CSCR with an emphasis on the most recent findings in patient demographics, risk factors, clinical imaging findings, and management options. Patients with these biomarkers, age 30–44 years, male gender, increased stress levels, hypercortisolism (endogenous and exogenous exposures), sleep disturbance, pregnancy, and genetic predisposition have increased susceptibility to CSCR. Also, biomarkers on optical coherence tomography (OCT) such as choroidal thickness (CT) and choroidal vascularity index (CVI) showed good diagnostic and prognostic significance in the management of CSCR. There are nonspecific features of CSCR on OCT and OCT angiography such as choroidal neovascularization, photoreceptor alteration/cone density loss, and flat irregular pigment epithelium detachment. We described rare complications of CSCR such as cystoid macular edema (CME) and cystoid macular degeneration (CMD). Patients with CME recovered some vision when treated with anti-vascular endothelial growth factors (anti-VEGFs). Patients with CMD had irreversible macular damage even after treatment with anti-VEGFs.
Keywords
Introduction
Central serous chorioretinopathy (CSCR) is one of the most common disorders seen in medical retina practice and is characterized by serous retinal detachment with or without retinal pigment epithelial (RPE) detachment. 1 The underlying pathophysiology, although not completely understood, broadly occurs due to the leakage of fluid through retinal pigment epithelium into the subretinal space. Although generally a self-limited disease, CSCR can persist and leave diverse sequelae owing to retinal pigment epithelium damage, resulting in diffuse retinal pigment epitheliopathy (DRPE) and choroidal neovascular membrane (CNVM). 2 Chronic CSCR (cCSCR) is defined as symptoms and signs for at least six months, with some studies stating that three months of persistent symptoms are enough to make the diagnosis. It affects men greater than women, with a prevalence ratio between 3:1 and 7:1. 3
Several risk factors exist, including exposure to corticosteroid medications (regardless of route, dosage, or duration) 4 and pregnancy (mostly in third trimester). 5 The cCSCR affects young individuals within their third to fourth decades, with a typical range of 45–51 years. When older individuals are affected, they tend to present with more diffuse retinal pigment epithelium loss and choroidal neovascularization.2,3
Biological biomarkers are quantifiable parameters which can be helpful to predict the incidence of disease or treatment outcomes.6,7 With respect to ocular diseases such as CSCR, this pertains to demographic, physiological, and imaging parameters which can be predictive of disease incidence, progression, and treatment response. Imaging modalities like optical coherence tomography (OCT), optical coherence tomography angiography (OCTA), fundus autofluorescence (FAF), fluorescein and indocyanine green angiography (FA/ICGA) can be an invaluable aid to the treating physician.
The aim of this review is to provide clinical understanding of the biomarkers of CSCR. We placed emphasis on the most recent and relevant findings in patient demographics, risk factors, clinical imaging findings, and management options.
Demographics and physiological parameters
Age
There are variations in the reported association between age and CSCR. However, high incidence rates usually fall within the 30–44 years age range. In a nationwide population-based study in Taiwan, the incidence of CSCR in patients using corticosteroids was highest in the 35- to 44-year-old patients—73.3 (95% confidence interval [CI] = 60.2–86.4 per 100,000 person-years—and lowest in those ⩾65 years old—21.1 (95% CI = 11.3–30.9) per 100,000. 8 Also, a study by Kitzmann and colleagues 9 on the incidence of CSSR in Olmstead County, Minnesota, USA, showed the incidence of CSCR was highest in men between the ages of 30 and 44 years. CSCR can sometimes present at later ages, particularly in women and patients with atypical forms.4,10
Gender
CSCR is predominant in men. An epidemiologic study of 786 patients with no history of corticosteroid use between ages 20 and 60 years in Taiwan found that the incidence of idiopathic CSCR was 1.7 times higher in men than in women (27 versus 15 per 100,000 individuals respectively). 10 One study in an Egyptian population showed a male to female incidence rate of 9.75:1. 11 Also, a retrospective single institution study of CSCR in African Americans supported the male preponderance. The male to female ratio was 6.5 in African Americans and 3.5 in Caucasian populations. 12 Kitzmann and colleagues 9 showed the mean adjusted incidence per 100,000 was 9.9 for men and 1.7 for women (95% CI = 7.4–12.4 and 0.7–2.7, respectively), a sixfold prevalence for men. It is unclear why there is a higher prevalence in middle-aged men compared to women.
Exogenous and endogenous hypercortisolism
CSCR is associated with endogenous hypercortisolism. History of steroid usage (independent of dosage or duration) has a strong association with CSCR. In a Taiwanese population study, patient with any corticosteroid intake had a significantly increased risk of CSCR when adjusted for cofounders (odds ratio [OR] = 2.40; 95% CI, 1.49–3.89). In a subgroup analysis of oral versus other routes of steroid intake, only oral steroids had a significant contribution to the risk of CSCR. 8 A case-control study of 50 patients with acute CSCR showed a statistically significant increased odds of steroid exposure in study patients compared to control (CSCR patients: 52% steroid usage, controls: 16%, p < 0.0001); two of the CSCR patients also had Cushing syndrome. 13 An association between CSCR and Cushing syndrome has also been demonstrated in other studies; thus, endogenous and exogenous sources of corticosteroids are linked to CSCR.14,15
Patients with CSCR experience endocrine and metabolic abnormalities. A prospective study of 24 patients with active CSCR found association with increased 24-hour urine cortisol or tetrahydroaldosterone (THA). The mean THA in patients with CSCR was significantly higher than controls (CSCR: 43.8 ± 43.5 µg/mL, controls: 32.8 ± 11.3 µg/mL). The cortisol levels in patients with CSCR followed similar pattern (36.7 ± 25.1 µg/mL in acute CSCR and 28.4 ± 3.6 µg/mL in controls). Early and late morning serum cortisol levels were normal in all study participants. 16
Corticosteroids, as described above, stimulate adrenergic receptors, leading to the release of endogenous epinephrine. Epinephrine’s effect on choroidal blood flow leads to hyperpermeability seen on ICGA in patients with CSCR. 17
Psychological disorders and social stressors
The incidence of CSCR is correlated with stressors induced by economic, social, and psychological factors. A study in Greece showed an increasing trend in the incidence of CSCR from 2005 to 2012 with the highest incidence in 2011 which coincided with the economic crisis of 2011 in Greece. The authors conjectured that emotional stress caused by the financial crisis affected the development of CSCR in this population. 18
CSCR is associated with psychological stressors like emotional distress, depression, somatization, hostility, Type A personality, and narcissistic traits. 4 In a case-control study, Conrad and colleagues compared 31 patients with newly diagnosed CSCR with age- and sex-matched controls to determine the association of emotional distress, alexithymia, and nine psychopathological symptoms, including hostility with CSCR. Patients with CSCR scored higher on all parameters. 19 It is postulated that these stressors stimulate the sympathetic pathway which causes the release of sympathetic mediators, including epinephrine, norepinephrine, and cortisol. 20 Also, it is has been shown that persons with Type A personality traits have higher resting epinephrine blood levels and greater release of epinephrine and cortisol in response to stress; this stress type is more common in men than women. 17
The association between stress and CSCR is hypothesized to be mediated through stress-related increases in cortisol. The mechanism as to how cortisol might affect the development of CSCR is hypothesized as follows. The choroid is able to autoregulate its blood flow using endogenous nitric oxide 21 and prostaglandin 22 release. However, endogenous corticosteroids such as cortisol increase epinephrine release which in turn increases choroidal blood flow by affecting the production of nitric oxide, prostaglandins, and free radicals, resulting in choroidal hyperpermeability, 17 Choroidal hyperpermeability in patients with CSCR has been demonstrated via ICGA, a finding which supports this hypothesis.
Sleep disturbance
CSCR is associated with sleep disturbances due to obstructive sleep apnea (OSA), circadian rhythm disorders, and irregular work schedules. A retrospective single-center study of 29 consecutive patients in France found irregular working hours as a potential risk factor for idiopathic CSCR. The same study also found an association between body mass index (BMI) >25 and CSCR. 23 Similar to stress, the link between sleep disturbance and CSCR is also hypothesized to be mediated through changes in cortisol. Endogenous cortisol levels change with circadian rhythm and white light; hence, the higher early morning levels are typically seen in most patients. 24 Irregular sleep patterns can be regarded as psychological and physiological stress. These stressors have been described earlier to cause increase in endogenous steroid levels. 23
Patients with OSA can present with dysregulated sleep. However, OSA itself is independently associated with CSCR. In a systematic review and meta-analysis of the association between OSA and ophthalmologic diseases, Huon and colleagues 25 found significant association between OSA and CSCR (OR = 2.019, p = 0.028).
Pregnancy
Pregnancy causes significant physiological changes in the human body. When the ocular system is affected, it manifests as visual disturbances. In a retrospective study of 147 patients with pregnancy-induced acute visual loss due to chorioretinal disease, the most prevalent diagnoses were CSCR (22.4%) and hypertensive retinopathy with or without pre-eclampsia (22.4%), followed by retinal tear with or without retinal detachment (18.4%). 26 Two other studies similarly showed that pregnant patients have an increased risk of bilateral and unilateral CSCR which can result in severe visual loss.27,28 In some cases, there is resolution of CSCR, either partially or completely after delivery. 28
Increased levels of progesterone are assumed to be responsible for the higher rates of CSCR during pregnancy, particularly in the third trimester. 26 In pregnancy, there is increase in endogenous steroid hormone biosynthesis like estrogen, progesterone, androgens, and glucocorticoids for the maintenance of the growing fetus. 29 As previously described, these increases in steroid hormone levels are believed to alter choroidal blood flow, leading to the hyperpermeability seen in CSCR.
Genetics
Genetic susceptibility to CSCR is found in some population. A study of the families of five patients with retinal serous detachment suggested CSCR could be a dominant inherited disease in some circumstances. 30 The authors found an association with certain polymorphisms in the complement factor H (CFH) and GSTM1 gene. Another study of genetic polymorphisms in patients with CSCR found a statistically significant association between the CFH gene (genotypes TT rs3753394, GG rs1329428, and TT rs1065489) and CSCR. 31
In a similar study, a genome-wide association analysis was used to identify a susceptibility locus for CSCR in a Japanese population. They identified a susceptibility locus at rs13278062, rs6061548 at TNFRSF10A-LOC389641, and a T allele rs13278062 at TNFRSF10A-LOC389641. When replicated in a European cohort, investigators were also able to identify the rs13278062 and rs6061548 allele. 32
Imaging parameters
OCT
The advent of OCT revolutionized retinal imaging and has become an indispensable imaging tool in the diagnosis and identification of CSCR. It can be used to evaluate parameters such as choroidal thickness (CT) (Figure 1), choroidal vascularity index (CVI) (Figure 2), and hyperreflective dots in patients with CSCR. 33

OCT scan showing neurosensory detachment with demarcation of various layers of choroid (right). Large choroidal vessel thickness is marked, together with the Sattler’s and Haller’s layer (left).

Choroidal vascularity index (CVI) measurements: Montage showing the process of CVI calculation. Top scan shows neurosensory detachment in an eye with central serous chorioretinopathy; middle scan shows choroidal boundaries using automated algorithm; and bottom scan shows the binarized image of the choroid with CVI of 59.6.
Choroid thickness
Multiple studies have shown an increased CT (measured from posterior edge of RPE to sclerochoroidal interface) in eyes with CSCR and normal fellow eye.34–36 This generalized choroidal thickening can be noted at the macula, including the fovea, and at sites of fluorescein leakage. 34 Interestingly, resolution of CSCR was associated with the reduction in CT. This was noted after spontaneous resolution or posttreatment with laser photocoagulation, photodynamic therapy (PDT), anti-vascular endothelial growth factors (anti-VEGFs), oral acetazolamide or oral eplerenone.36–42
Choroidal volume
Pertl and colleagues 43 showed that in eyes with treatment-naïve CSCR, changes in CT and volume correlated with changes in subretinal fluid (SRF). Moreover, eyes with higher baseline choroidal volume also responded better with more reduction in SRF. 43
Large and medium choroidal vessel layer thickness
Large choroidal vessels comprise a significant portion (up to 70%) of overall CT. 44 CSCR forms one of the disease entities in pachychoroid spectrum disorders and is characterized by thickened choroid and enlarged large choroidal vessels with compressed inner choroidal layers. There is no definitive cut-off point of CT to define pachychoroid as multiple factors such as age, sex, ethnicity, and axial length determine CT.45,46
CVI
CVI, defined as the ratio of stromal area versus total choroidal area in single-line scan (subfoveal) or volume scans, is used to study vascular changes in choroid in normal and various disease states. 47 CVI provides a comparison to the gold standard, that is, histopathology. Previous reports show a significantly increased CVI in eyes with CSCR compared to their fellow eyes. 48 Moreover, eyes with active CSCR appear to have higher CVI compared to eyes with resolved CSCR. This suggests that CVI can be used as a marker of disease activity. 48 Disease resolution, either spontaneous or post laser photocoagulation, leads to reduction in CVI. The plausible explanation relates to the engorgement of choroidal vessel in the acute state of disease, leading to increased luminal area of choroid and thereby CVI 49 (Figure 3).

Fundus photos (upper right) of a 53-year-old man who presented with a 4-year history of gradual vision loss. His best-corrected visual acuity was 20/40. He has no history of steroid use and was currently taking spironolactone 50 mg twice daily. Fundus images (upper left) shows retinal pigment epithelium (RPE) alterations in both eyes. Autofluorescence of both eyes (upper left) show hyper- and hypofluorescence (yellow short arrows) in areas with RPE alterations. Fluorescein angiography (upper right) of both eyes shows focal hyperfluorescence with late leakage along with stipple hyperautofluorescent areas (orange arrows). ICGA (lower left) of both eyes show choroidal hyperpermeability (orange arrows). OCT (lower right) shows neurosensory detachment (orange arrows).
Flat irregular pigment epithelium detachment (double layer sign)
Flat irregular pigment epithelium detachment also known as the double layer sign is not unique to eyes with CSCR and basically denotes a split of retinal pigment epithelium and Bruch membrane. The double layer sign is predictive of type 1 choroidal neovascularization which initially may be nonexudative. 50 Eyes with CSCR show various types of pigment epithelium detachment varying from serous in acute CSCR to flat irregular in cCSCR (Figure 4).4,51 This may or may not be associated with SRF, and the presence of SRF is not evidence of choroidal neovascularization as even CSCR disease activity manifests in the form of SRF. This forms one of the limitations of structural OCT, and OCTA may be a handy tool in these scenarios. Indeed, up to 25% of fellow eyes of cCSCR harbor a subtle choroidal neovascular membrane (CNVM) which can be missed on structural OCT scans (Figure 4). 52 Although FA is the gold standard for detection of CNVM, 53 recent studies have shown enhanced detection with OCTA. The OCTA has a sensitivity of 86–100% and specificity of 96–100% compared with FA in detecting CNV in eyes with cCSCR and irregular PED.53,54 In a retrospective study by Bousquet and colleagues, 55 type 1 CNV in FIPEDs detected by OCTA was 36.5% compared to 25% in combined FA/ICGA and spectral domain-OCT (SD-OCT). We recommend the use of OCTA in the assessment of CNV in cCSCR with FIPED. Also, FIPED should not be misdiagnosed as active CNV and treated with anti-VEGF. However, if OCTA shows CNV or patient is not responding to usual CSCR therapy, anti-VEGF treatment can be started. 56
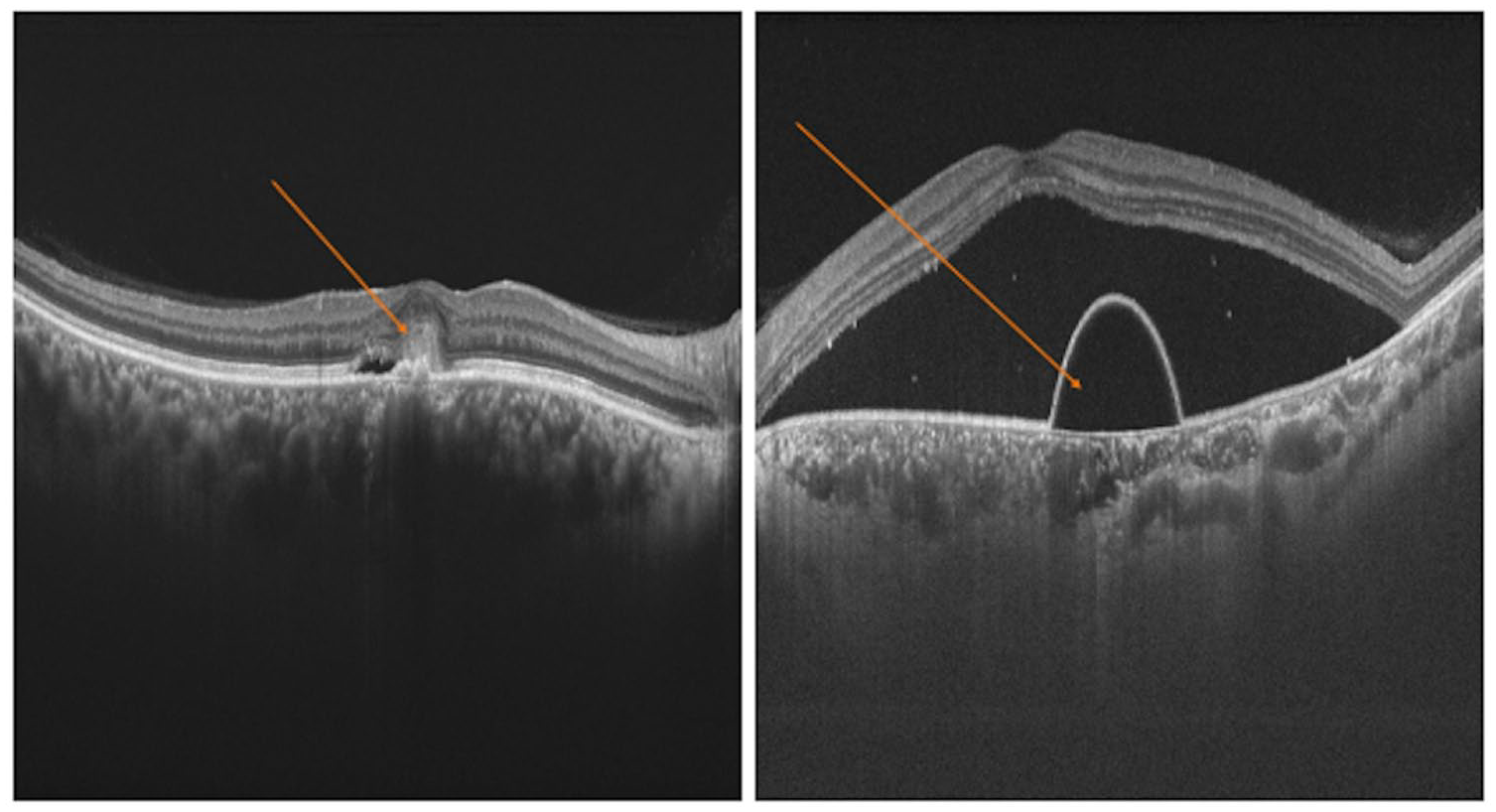
OCT scan showing choroidal neovascular membrane (left) and pigment epithelium detachment (right).
SRF
CSCR has similar presentation and mechanism of pathogenesis as other retinal diseases. For example, CSCR and polypoidal choroidal vasculopathy (PCV) share similar clinical, angiographic, and tomographic findings. In a study to differentiate between CSCR and PCV, Baek and Park evaluated optical density ratios of the SRF in both disease processes. They measured the optical density ratios from the SRF to the vitreous, RPE, and retinal nerve fiber layer in both diseases and found that they were significantly higher in patients with PCV compared to cCSCR (p = 0.002, p = 0.001, p = 0.001 respectively). They did not notice any significant difference between acute and cCSCR (p = 0.358, p = 0.433) or between vitreous and retinal nerve fiber layer in all groups (p = 0.172, p = 0.171). Also, the PCV group had the thickest optical density ratios (p = 0.001). Although patients with CSCR usually present with good vision compared to their PCV counterparts, optical density ratios provide insight into the pathogenesis of each disease. The difference in SRF protein content highlights the integrity of the blood retina barrier in both disease processes, hence the lack of statistical difference between acute and cCSCR. 57
Photoreceptor alterations in CSCR
CSCR eyes mostly show RPE changes. However, changes in photoreceptor density can be noticed as well. In an observational case study of 21 patients (21 eyes with unilateral CSCR and 21 fellow eyes as control), Ochinciuc was able to detect decreased cone density at the fovea using adaptive optics (AO) camera in patients with CSCR. They reported higher median values in all quadrants in healthy eyes compared to CSCR eyes treated with laser surgery (p = 0.02, p = 0.003, p = 0.0001, and p = 0.001). 58 The AO camera is able to acquire retinal images with resolution up to 2 mm. 59 Meirelles and colleagues used this technology to detect changes in photoreceptor mosaic pattern in a patient with CSCR after clinical resolution. In their case report, patient’s OCT only revealed minor irregularities in the RPE and Bruch membrane. 60 The AO is another imaging tool that be used to evaluate retinal layer integrity and changes in visual outcomes after resolution of CSCR.
Cystoid macular edema (CME) and cystoid macular degeneration (CMD)
CME and CMD are rare complications of cCSCR. Iida and colleagues 61 defined CME as OCT cystoid changes and fluorescein leakage in the macula and CMD as OCT cystoid change without fluorescein leakage in the macula. The CMD due to CSCR presents with visual decline, and treatment can be challenging. In a case study of a 44-year-old woman with CMD from CSCR, her OCT scans on presentation showed hyperreflective cortical vitreous attached to the macula, intraretinal cystic changes, microaneurysms, and attenuated retinal pigment epithelium band. Her central subfield thickness was 486 µm, and best-corrected visual acuity (BCVA) was 20/40. The patient received anti-VEGF injections with subsequent resolution of leakage and vitreomacular traction on OCT; however, the intraretinal cysts persisted. The central subfield thickness reduced to 379 µm with attenuated retinal pigment epithelium band and no improvement in BCVA. 62 Patients with CME may recover some visual function from treatment with anti-VEGF, and treatment is indicated. However, we do not recommend treatment for cCSCR patients with CMD due to irreversible macular damage 61 and no improvement in BCVA.
Retinal Pigment Epithelium (RPE) integrity in CSCR
CSCR has shown complete resolution in some patients. However, it is not well understood whether there is closure of the detached retina and or complete resorption of the SRF. Gupta and colleagues evaluated the spontaneous closure of retinal pigment epithelium in the natural course of CSCR using SD-OCT transverse and retinal pigment epithelium fit C-scans. In 85% of eyes, they found irregular retinal pigment epithelium patterns on SD-OCT resembling “honeycomb” corresponding to fluorescein leakage sites on FA. Also, 54.5% of eyes with “honeycomb” pattern showed a breach in retinal pigment epithelium on transverse C-scan and retinal pigment epithelium fit C-scan. There was resolution of SRF in most eyes (resolved in 45.5%, decreased size in 27.2%, and persisted in 27.2%) and closure on microrip with retinal pigment epithelium hypertrophy. Resolution of SRF was attributed to decrease in no effusion of fluid from the vascular choroid and repair of the retinal pigment epithelium microrip. 63
Pachychoroid pigment epitheliopathy (PPE)
The term PPE was initially described by Warrow and colleagues as a constellation of retinal pigment epithelium abnormalities and pigmentary changes affecting areas of choroidal thickening without any signs of SRF. However, clinical features resembled that of CSCR. 64 The PPE falls within a spectrum of associated diseases with pachychoroid (thickened choroid), including CSCR, PCV, and pachychoroid neovasculopathy. 65 Lee and colleagues used SD-OCT to describe focal disruptions in the ellipsoid and interdigitating zones (EZ/IE zones) in eyes with PPE. The mean subfoveal CT was 450 ± 66 µm (range = 356–595 µm) in affected eyes and 367 ± 86 µm (range = 220–554 µm) in unaffected. In 86% of eyes, drusenoid lesions preceded the EZ/IE zones. Also, 88.9% and 66.7% of eyes showed dilated outer choroidal vessels beneath the EZ/IE zones and attenuation of choriocapillaris, respectively. Also, SD-OCT revealed other abnormalities at the EZ/IE zones such as decreased reflectivity, thinning, irregularities, and undulations adjacent to the sites of focal disruptions. In 81.5% of eyes with lesions, retinal pigment epithelium atrophy was noted with hypertransmission of signal on SD-OCT. 65 In the absence of SRF, focal disruption at the EZ/IE zones on SD-OCT can provide information on PPE and CSCR.
Anti-VEGF versus laser photocoagulation and predictors of recurrence
Eyes with CSCR are treated with laser photocoagulation to “seal” retinal pigment epithelium leak sites. Although laser photocoagulation can be effective, improvement in vision is not predictable compared to other treatments like anti-VEGF. 4 In CSCR eyes that underwent laser photocoagulation, Lee and colleagues were able to describe the association between baseline structures like hyperreflective foci on SD-OCT, visual outcome, and recurrence. The baseline characteristics before argon laser treatment included mean SRF thickness and CT of 298.9 ± 146.0 µm and 395.3 ± 97.9 µm, respectively. All eyes had retinal detachments, and 21% had photoreceptor granulation at the macula. Abnormalities at the leakage sites included pigment epithelial detachment (33.9%), irregular retinal pigment epithelium (33.9%), retinal pigment epithelium bumps (8.1%), and retinal pigment epithelium defects (2%). After laser photocoagulation, they observed resolution of SRF in all patients (mean duration = 2.2 ± 1.5 months; range = 1–7 months). The number of hyperreflective foci at all retinal layers was reduced at the last visit (p < 0.05). Also, the abnormalities at the leakage sites decreased dramatically—pigment epithelial detachment (17.7%), irregular retinal pigment epithelium (21%), retinal pigment epithelium bump (9.7%), and retinal pigment epithelium defect (1.6%). The mean CT decreased to 388.2 ± 101.1 µm (p = 0.06). There was an improvement in visual outcome with laser photocoagulation (baseline logMAR BCVA = 0.34 ± 0.6; final log MAR BCVA = 0.02 ± 0.04). They suggested that an increased subretinal hyperreflective foci represents delayed SRF resolution and increased chance of recurrence. Therefore, the higher the baseline hyperreflective foci on SD-OCT, the higher the chances of recurrence. 66
FAF
The FAF is a noninvasive technique that is used to evaluate the integrity of the retina. Autofluorescence photography can give functional images of the retina and surrounding areas by using stimulated emission of light from fluorophores. Lipofuscin accumulates in tissues as a result of phagocytosis of damaged photoreceptor outer segments. A healthy macula is expected to show uniform autofluorescence. The hyperautofluorescence in CSCR can be attributed to the alterations in retinal pigment epithelium as a result of buildup of SRF. It is suggested that increased levels of autofluorescence in cCSCR corresponds to areas of detached retina. 67 However, an FAF lifetime study showed correlation with leakage spots on fluorescence angiography but not SRF accumulation. In acute CSCR, there were increased short lifetimes at the macular area and prolonged autofluorescence lifetimes in cCSCR. Autofluorescence lifetime is absent within a few days of CSCR onset, but changes become apparent during the course of the disease. 68 This is due to the time lapse between the onset of disease and damage to RPE (Figure 3).
A case series of 30 consecutive patients found correlation between increasing levels of autofluorescence (punctate and diffuse) and accumulation of material on the outer surface of the retina. The location autofluorescence on the outer surface was attributed to reduced phagocytosis by the retinal pigment epithelium and the potential for lipofuscin precursors to produce autofluorescence. The authors hypothesized that retinal pigment epithelium autofluorescence due to the accumulation of lipofuscin might not be the only culprit, and attention needs to be given to the outer retinal segments in patients with CSCR. 69
Zola and colleagues showed changes in FAF patterns in cCSCR. They found granular hypoautofluorescence was the most common baseline pattern (51%), followed by punctate hyperautofluorescence (19.7%), diffuse homogeneous hyperautofluorescence (11.4%), and confluent hypoautofluorescence (8.8%). They demonstrated that change in FAF patterns in cCSCR is gradual with the earliest change (four months after the first episode being diffuse hyperautofluorescence. They noted a slow change in patterns, from hyperautofluorescence to hypoautofluorescence (25% of eyes over 36 months period). Eyes with punctate hyperautofluorescence were the slowest to change patterns. They stated that diffuse hyperautofluorescence could be due to SRF or reactivation. 70 Punctate hyperautofluorescence represents chronicity due to lipofuscin from outer segments of photoreceptors or macrophages that have ingested lipofuscin or precursors.69,70
Recently, Han and colleagues in a study to evaluate the patterns of FAF abnormalities in CSCR came up with five different patterns. They reported most patients had a blocked autofluorescence pattern (38.9%), followed by hyperautofluorescence (31.0%), hyper/hypoautofluorescence (13.5%), mottled (8.7%), and descending tract (8.0%). Blocked autofluorescence was defined as no changes or uniform changes in decreased autofluorescence where SRF existed. Mottled FAF referred to grainy or coarse region of increased FAF, descending tract showed downward leading autofluorescence pattern from the posterior pole to the inferior arcade, and hyper/hypoautofluorescence is a mixed pattern of hyperautofluorescence and hypoautofluorescence. 71 There is no standard FAF pattern description in CSCR; therefore, clinicians can use these descriptions as reference when diagnosing and monitoring the treatment of CSCR.
FA
This is one of the first and most classic imaging modalities for the diagnosis of CSCR. 4 Its usefulness lies in its dynamic study of retinal blood flow, which is pivotal in the study and analysis of CSCR. 2 The FA will typically show a single leakage point or multifocal leaks that are mostly localized within or adjacent to an area of SRF. In the early phase of an angiogram, there is point leakage that slowly evolves into two patterns. The most common pattern is that of “ink-blot,” which is present in greater than 60% of cases. The “smoke-stack pattern” is less common and present in less than 30% of cases. A prospective FA study of 13 patients showed that the “smoke-stack CSCR pattern” was attributed to underlying choroidal vasculature abnormality and not the retinal pigment epithelium. The leakages rates were consistent with bulk fluid flow rather than secretion or diffusion. 72
Daruich and colleagues proposed another biomarker, fluorescein leakage intensity, on FA which was defined as the ratio between area of hyperfluorescence at mid-phase to early phase. They reported that intense fluorescein leak was associated with increased duration of a CSCR episode (p = 0.074). 73 In cCSCR, FA shows multifocal leakage with diffuse retinal pigment epithelium abnormalities, and atrophy. Retinal pigment epithelium abnormalities are often seen as granular or mottled hyperfluorescence in mid- and late phase. 74 The cCSCR can also present with pigment epithelial detachments. The FA will show early hyperfluorescence with progressive intensity and increased pooling in this case (Figure 3).
ICGA
ICGA is extremely useful in mapping the choroidal vasculature and showing CSCR abnormalities, especially the chronic form. ICGA often shows early choroidal filling delay, large choroidal venous dilatation, and focal hyperfluorescence owing to choroidal hyperpermeability, which is often seen surrounding the focal leakage. 11 Chronically, the affected area evolves into persistent hyperfluorescence, washout zone, or centrifugal displacement of hyperfluorescence in the late phase. 75 In cCSCR, a CNVM can often develop. The CNVMs are seen as new dilated choroidal vessels with associated hyperpermeability76,77 (Figure 3). The ICGA is a useful diagnostic tool for the screening and detection of these membranes.
OCTA
The OCTA is a noninvasive technique that is used to create images of retinal and choroidal blood vessels by motion contrast of moving blood components in contrast to dye-based techniques like FA and ICGA.78,79 The OCTA is used to analyze different blood vessel layers like the choriocapillaris, choroidal vascular reactivity, vessel density, microvascular alteration, and choroidal neovascularization in CSCR (Figure 5). A retrospective study of 101 eyes showed a decreased OCTA signal in the SRF and increased signal outside the SRF of acute CSCR patients. However, the OCTA signal was significantly higher in patients with CSCR compared to controls (mean = 43,238 ± 19,568 and 23,348 ± 12,226, respectively, p < 0.0001). Also, the number of pixels with decreased OCTA signal was significantly higher in CSCR than in controls (30,243 ± 15,793 and 12,970 ± 7454 respectively, p < 0.001). They also noticed a higher number of pixels with increased OCTA signals in patients with acute CSCR, nonresolving CSCR, and chronic atrophic CSCR compared to inactive CSCR and healthy controls. The study was able to demonstrate that eyes with CSCR show increased and decreased OCTA signals at the level of the choriocapillaris compared to normal eyes with consistent choriocapillaris vascular network. 80

OCTA scan (upper images and middle lower image) of a patient with choroidal neovascularity (CNV) associated with central serous chorioretinopathy (CSCR). Choriocapillary scan (upper right) shows choroidal neovascular network. Cross-sectional B-scan (lower left) shows choroidal neovascular membrane (red arrow), subretinal fluid (yellow arrow), and flat irregular pigment epithelium detachment (green arrow).
Choroidal vascular flow is dysregulated in patients with CSCR. During the physical stress, the compensatory mechanisms of the autonomic nervous system are dampened compared to normal patients. A multicenter case-control study of 35 patients with CSCR and 25 age-matched controls showed increased choriocapillaris vascular density during stress in CSCR patients compared to controls, although the former had lower baseline values (p < 0.05). 81 Yu and colleagues 82 also demonstrated a decrease in superficial total microvasculature in CSCR compared to controls in 15 patients using a customized image segmentation processing program to analyze 6 × 6 mm macular retinal blood flow OCTA images.
The OCTA is used for the clinical evaluation of neovascularity in eyes with CSCR. The sensitivity of OCTA in detecting choroidal neovascularization in cCSCR patients increases during stress. The difference in choroidal neovascularization at rest and under stress (induced increase in blood flow during handgrip test HGT) is due to a dysregulated autonomic nervous system in regulating choroidal blood flow during spikes in blood pressure. 83 Before OCTA, the prevalence of choroidal neovascularization in CSCR was estimated at 2%–9%. 84 However, in a case-control study of 29 eyes to evaluate the neovascular and nonneovascular patterns in eyes with CSCR, 34.5% of eyes showed a neovascular pattern. Eyes with neovascular pattern had a mean central retinal thickness decrease from 372 ± 130 µm at the first visit to 245 ± 46 µm at the final visit (p = 0.0026) after anti-VEGF injections (mean injection neovascular = 6.4, nonneovascular = 2.9). 85
The use of PDT has gained ground in recent years for the treatment of cCSCR. However, complications of PDT include but are not limited to choroidal ischemia, retinal pigment epithelium changes, and choroidal neovascularization.86,87 Wu and colleagues demonstrated high rates of choroidal neovascularization in cCSCR patients with prior PDT treatments (incidence rate of 45.7%). The increased incidence of choroidal neovascularization was postulated to be due to ischemia induced by PDT which causes the release of VEGF. They also noted choroidal neovascularization association with old age (p = 0.059), large PDT spot size (p = 0.024), and thinner subfoveal CT (p = 0.008). Further analysis revealed that choroidal neovascularization incidence increased when the maximum PDT spot size was larger than 2400 µm (OR = 3.27, 95% CI, 1.04–10.32; p = 0.043) and with a post-PDT subfoveal CT of less than 310 µm (OR = 2.97; 95% CI, 1.02–8.62; p = 0.046). Half-dose PDT, although relatively safer, does not prevent against the development of choroidal neovascularization. 88 OCTA has been used to analyze vascularity in CMD associated with CSCR with an incidence rate 44.8%. Eyes with choroidal neovascularization demonstrated shallower SRF (mean neurosensory detachment = 65.2 ± 2.27 µm) compared to nonchoroidal neovascularization eyes (mean neurosensory detachment = 134.6 ± 77.4 µm). 84
Conclusion
The CSCR represents the fourth most common nonsurgical chorioretinopathy that can have significant morbidity in certain populations. The advancement of multimodal imaging techniques has allowed for the better understanding of its diverse biomarkers, augmenting diagnostic accuracy, and improving our understanding of its pathophysiology.
Footnotes
Author contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.