
Abstract
Obesity is a health-threatening and epidemic medical condition that can affect individuals of different ages and is potentially associated with an increased risk of systemic and ocular disorders. Despite the well-documented adverse effects of obesity on different parts of the body vasculature, less published data are available concerning obesity-related consequences on the ocular vasculature. As the human choroid is a highly vascularized tissue, its morphology and function might be altered in obese individuals. The micro-structural changes within the choroid could also trigger development of subsequent functional abnormalities of the eye. Previous population-based studies have asserted an association between obesity and choroidal thickness; however, they reported conflicting patterns of association between obesity and changes in choroidal thickness. Therefore, to enhance our understanding of the changes in choroidal morphology secondary to obesity, we reviewed studies describing the micro-structural consequences of obesity on the choroidal thickness profile and its underlying physiological and anatomical basis. This review includes all original publications related to the association between choroidal thickness and obesity published until mid-2021 that were indexed in PubMed, Google Scholar, ScienceDirect, or Scopus.
Introduction
Obesity is typically described as excessive fatty tissue accumulation in the body, and is one of the most prominent health concerns worldwide, reaching pandemic levels.1,2 Obesity can develop due to the interaction among different etiologies such as genetic, lifestyle, socioeconomic, and environmental factors.3–6 Obesity is a serious risk factor for developing various comorbid diseases, including metabolic syndromes (dyslipidemia and insulin resistance), cardiovascular diseases, diabetes mellitus type 2, hypertension, stroke, and sleep apnea.7–10 Another negative impact of obesity is the risk of developing depressive disorder, which can contribute to social isolation from peers. 11 Therefore, the psychosocial and economic burden of obesity and its comorbidities and coexisting conditions are quite substantial.1,3–5,7,8,11,12
Obesity may affect different structural and functional aspects of the visual system. Previous studies have found serious consequences of obesity for some visual functions, including visual acuity and visual field. 13 The effects of obesity on ocular anatomy have also been extensively studied. The majority of previouly published studies have shown that obese people are at increased risk of glaucomatous manifestations, including higher intraocular pressure, increased cup-to-disk ratio, and thinner retinal nerve fiber layer. 14 However, contradictory results have also been reported.15,16 The link between obesity and the risk of cataract formation,17,18 age-related macular degeneration,19,20 and diabetic retinopathy21,22 is also a controversial issue. The incompatible findings of studies on obese individuals may be due to the variations in diet and lifestyle of the participants.
The body hormones of leptin and insulin regulate the appetite and metabolism and distribute the adipose tissue throughout the body.23,24 People with obesity have abnormally raised levels of leptin that may stimulate abnormal metabolism and insulin resistance. As a result, it can lead to fatty tissue build-up in the body. Insulin activates glucose uptake and inhibits the release of fatty acids from the adipose tissues; thereby, its abnormal secretion by virtue of the increased body weight may substantially impact ocular vasculature. 25 Leptin is produced by fat cells and regulates appetite by sending signals to the central nervous system. 26 Previous studies reported the link between leptin level and different posterior segment diseases such as choroidal neovascularization, diabetic retinopathy, and retinal detachment.27,28
It is evident that obesity can be associated with different macrovascular and microvascular dysfunctions.8,21,29–33 Notably, the choroid predominantly comprises a dense microvasculature system and is the major blood supplier of the retina. 34 Understanding the proposed impacts of obesity on the choroidal structure and profile could be a predictor in identification of obesity-induced ophthalmic complications. The main objective of this study is to review the potential effects of obesity and overweight on choroidal morphology.
Method for literature search
For this literature review, we conducted an extensive searched on PubMed, Google Scholar, ScienceDirect, and Scopus search engines for original scientific articles with the following key words in different combinations: obesity and choroid, overweight and choroid, body mass index (BMI) and choroid, obesity and choroidal thickness, BMI, and CT. We retrieved a total of 115 articles published from 1 January 1995, through 1 May 2021, including observational studies, randomized clinical trials (RCTs), systematic reviews, and meta-analyses. A thorough review of all publications in English and the abstracts of non-English papers was undertaken. The reference lists of the selected studies were also checked for potentially relevant papers. Selected sources were also mutually agreed upon by the authors. Irrelevant articles to the main purposes of the study were excluded.
Classification criteria for weight status
BMI is a typical index of weight status and calculates as body weight divided by body height squared (kg/m2). According to the World Health Organization (WHO) Expert Committee on Physical Status, underweight, normal weight, overweight (pre-obese), obese class I, obese class II, and obese class III (extreme obesity) are defined as BMI values of ⩽18.50, 18.50–24.99, 25.00–29.99, 30.00–34.99, 35–39.99, and ⩾40, respectively. Morbid obesity is defined as BMI value >35 kg/m2 when the patient experiences obesity-related diseases or BMI values >40 kg/m2 without any coexisted disease. The main limitation of the current WHO classification is that it does not consider the body adipose distribution. In practice, excessive accumulation of fatty tissue in the central or abdominal body part can pose a real risk to the body’s metabolic process and circulatory system.8,35 Therefore, other indices have been developed to represent the level of central adipose tissue, such as waist circumference and the waist–hip ratio.12,36,37 However, most studies applied BMI as a clinically approved criterion for weight-related health problems.36,38 This criterion is clear-cut and non-invasive for clinical and study settings.
Effects of obesity on systemic and ocular vasculature
Obesity-related cardiovascular disorder is due to comorbid diseases such as diabetes, 39 hypertension, 40 and stroke. 41 The progression of atherosclerosis in the carotid42,43 and femoral 43 arteries adversely affects these diseases. Studies on obese individuals determined that higher BMI values might reduce capillary density and tissue perfusion. 30 This sign is one of the earliest detectable microvasculature changes in the course of weight gain.44,45 Furthermore, obesity causes endothelial defects following hyperglycemia-induced oxidative stress46–48 There are two proposed histopathological theories for microvascular damage. First, vascular endothelial cells demonstrate abnormal synthesis of nitric oxide (NO) molecules following exposure to glycation end-products and stimulate vascular endothelial growth factor (VEGF). 49 The second theory is attributed to the oxidative stress phenomenon, in which hyperglycemia accelerates the production of reactive oxygen molecules. In consequence, it interacts with proteins and macromolecules like DNA and finally causes damage to the vascular endothelial cells. 49 In addition to hyperglycemia, dyslipidemia and inflammatory chemicals may also trigger the development of microvascular disorders. 50
The normal microcirculation of the two vascular layers of the eye, retina and choroid, could be indicative of the whole-body microvasculature status. Some optical coherence tomography-angiography (OCT-A) studies on obese individuals demonstrated changes in choroidal and retinal microvasculature of these population.51,52 For example, Kurtul et al., 51 in a prospective study on obese children, found significantly higher flow area for choriocapillaris and foveal capillary densities than normal healthy subjects. The retinal and choroidal vascular beds are observable locations to directly explore the microvascular system. Notably, any retinal and choroidal vasculature changes could predict the pre-clinical phase of systemic vascular disorders.33,44 Previous investigations have revealed direct associations between the retinal venular diameter and BMI measurements.32,53 Therefore, widening the retinal venular diameter could also be a clinical sign of systemic venular problems linked to obesity. 53
Choroidal thickness changes secondary to obesity
The importance of choroidal thickness evaluation
The human choroid is a highly vascularized structure located behind the globe and extended from the borders of the optic nerve head to the ora serrata. In addition to providing nutrients and oxygen to the sensory and pigmentary retina, the choroid regulates ocular temperature and intraocular pressure. 34 The structure and function of the retinal photoreceptors essentially depend on normal choroidal blood flow. 34 Because of its hyper-vascularized nature, the choroid is potentially subject to impairment from systemic and local diseases of the body circulatory system. 54 Therefore, abnormal morphology and malfunction of the choroid can be seen in various ocular and systemic disorders.55,56 Assessment of the choroid could thereby manifest obesity-induced microvascular impairments.51,54
Numerous studies on choroidal thickness have addressed its association with age,57,58 axial length, 59 refractive error,60,61 and ethnicity. 62 Thickness changes in choroidal tissue have also been noted in ocular diseases like diabetic retinopathy, age-related macular degeneration, central serous chorioretinopathy, and retinitis pigmentosa.63–66 Moreover, choroidal thickness measurement has diagnostic value in evaluating localized abnormalities of the posterior segment secondary to systemic diseases such as cardiovascular disorders and metabolic syndromes.55,56,67 In addition, changes in the choroidal microvasculature could indicate systemic vascular involvement due to obesity.32,54 Therefore, it has been hypothesized that choroidal thickness could be considered an indirect predictor of choroidal microvasculature.65,68,69 Some studies found the increasing effect of sildenafil citrate on choroidal thickness due to the vasodilatory effect of the drug and consequent rise in choroidal blood flow.68,69 Conflicting results have been reported by Sogawa et al., 70 and they found no significant correlation between subfoveal choroidal thickness (SFCT) measurement and choroidal circulation in healthy young subjects. However, their study had a small sample size and was performed on normal individuals. In addition, the potential effect of associated local and systemic diseases was not investigated.
Measurement of choroidal thickness using the enhanced depth imaging technique
Conventional imaging techniques such as indocyanine green angiography and B-scan ultrasonography represent low image resolution in differentiating posterior layers of the eye.71,72 Following the advent of OCT technology and providing in vivo investigation of the ocular structures, several studies have analyzed changes in choroidal thickness secondary to systemic conditions.56,63,67 The novel OCT techniques (spectral domain) represent higher resolution and less acquisition time because of faster scanning speed compared to the conventional time-domain method. In recent years, cross-sectional and quantitative assessments of choroidal structures have been carried out by adding a modality to spectral-domain OCT known as enhanced depth imaging (EDI). 73 In this technique, choroidal thickness is manually outlined as the vertical space between the external border of the hyper-reflective row of the retinal pigment epithelium layer and the internal border of the hypo-reflective choroidoscleral interface layer (Figure 1). 62 It should be noted that previous studies have indicated that choroidal thickness data recorded by different OCT devices are highly repeatable and have minimum variability.73,74 In addition, various OCT instruments are strongly correlated and can be used interchangeably.73,74
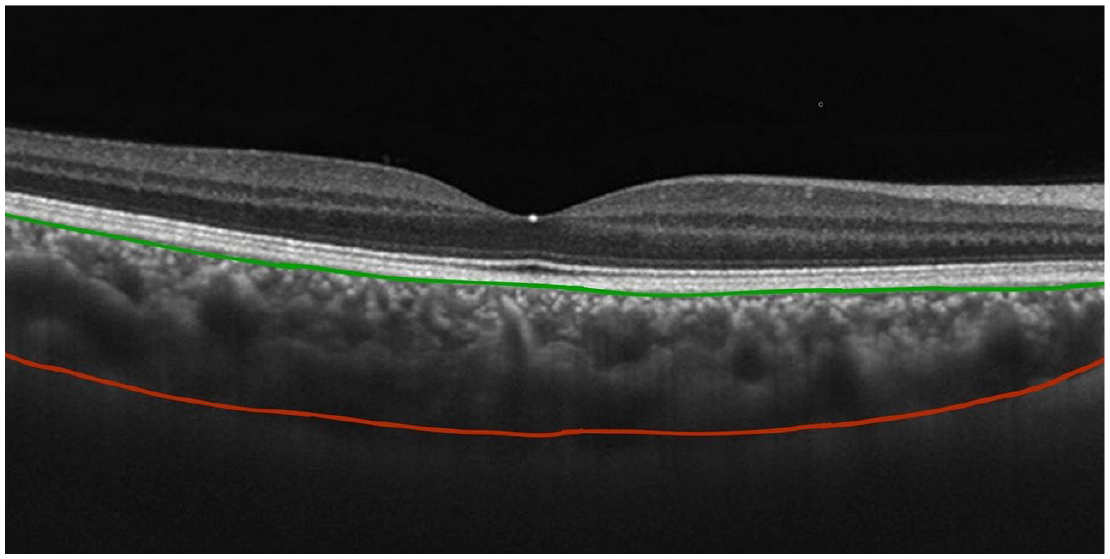
Enhanced depth imaging modality of optical coherence tomography representing the anterior (green line) and posterior (red line) borders of the choroid.
The effects of obesity on choroidal thickness
The effect of obesity on choroidal thickness has received limited attention in the literature. Table 1 summarizes the EDI-based studies on the association between SFCT and BMI value.
Studies investigating the association between body mass index and subfoveal choroidal thickness using enhanced depth imaging.

BMI, body mass index (kg/m2); OCT, optical coherence tomography; SFCT, subfoveal choroidal thickness.
A number of studies have consistently reported a negative association between SFCT and BMI measurements.14,25,54,76–78 In a prospective study on obese children aged 5–15 years, Ers¸an et al. 54 found a significant reduction in subfoveal and parafoveal choroidal thickness. They recorded baseline blood pressure and performed blood tests (serum insulin, plasma glucose, and lipids) after overnight fasting to control parameters that may affect choroidal thickness. Their findings showed that mean SFCT values in normal weight and age-matched obese children were 301.95 ± 56.72 µm, and 270.20 ± 56.13 µm, respectively. They ascribed the choroidal thinning to the microvascular alterations in obese participants. Boillot et al. 29 also supported this hypothesis. They proposed that ocular microvascular changes in obese subjects might be secondary to the arteriole restriction and venular diameter widening. In a cross-sectional study, Yilmaz et al. 76 investigated the association between BMI value and choroidal thickness in the adult population. Their results revealed a negative correlation between SFCT and weight status. They hypothesized that this finding might be due to the impaired dilation of the choroidal vessels following reduced endothelium-derived NO as a vasodilator agent in the obese population.32,33 The autonomic system controls choroidal blood flow, and when NO level decreases, parasympathetic control of choroidal circulation is prevented. 83 In addition, they found a positive correlation between obesity and the amount of two main vasoconstrictor molecules, that is, endothelin-1 (ET-1) and angiotensin II (Ang-II). 84 As a result, the imbalance between obesity-induced vasodilator/vasoconstrictor agents (declining NO level and rising ET-1 and Ang-II) may be associated with choroidal thinning. 14
Hypoxia is another potential underlying factor for obesity-induced choroidal thinning. This condition has been detected in obese individuals and fundamentally has a key role in cell death. Periodic episodes of hypoxia induce oxidative stress and inflammatory reaction. It causes damage to the endothelial cells of the vessel wall, increasing inflammatory cytokines, reducing cell reactivity to vasodilator factors, and stimulating the sympathetic nervous system.47,48 These consequences can contribute to dysregulation of the vessels and affect the choroidal circulation, resulting in a decrease in choroidal thickness measurements. 85 Although some progress has been made, further investigations are needed to prove this hypothesis.
In contrast, several studies reported a positive association between choroidal thickness and obesity.75,80,81 Yumusak et al. 80 demonstrated that SFCT was positively correlated with BMI in obese women which might be due to the changes in ophthalmic blood flow. Microvascular damage in obese women might be a complication of elevated blood insulin levels and high blood pressure. 31 In a cross-sectional study, Bulus et al. 81 examined obese children and illustrated a positive correlation between BMI and SFCT. They measured the blood pressure of participants to control the confounding effect of hypertension on CT. Their findings revealed that the mean SFCT values in normal and obese children were 348.43 ± 73.21 and 385.77 ± 6.09 µm, respectively. The elevated SFCT was attributed to the raised leptin level and overproduction of inflammatory cells in obese children. As discussed earlier, leptin plays a key role in controlling appetite and body weight. Higher leptin production in obese patients than in normal-weight individuals leads to further adipose tissue accumulation. 86 Available evidence shows that leptin also acts as an angiogenic factor contributing to oxidative stress on endothelial cells. 87 Conflicting results have been found by Panon et al., 82 and they found no correlation between SFCT and obesity. These inconsistent outcomes could be explained by various sources such as differences in age and gender of the study population, different choroidal imaging modalities, associated ocular and systemic diseases, and BMI status of the subjects.
Few works have been conducted on choroidal thickness changes in morbidly obese patients.14,88 In a study on morbidly obese patients who undertook laparoscopic surgery, Dogan et al. 88 found a continuous increase in post-operative SFCT at 3- and 6-month follow-ups. In a recent study, Gonul et al. 89 evaluated the choroidal thickness changes in 40 morbidly obese patients following bariatric surgery. They showed a positive association between choroidal thickness and BMI. Terra et al. 90 also found that choroidal thickness decreased gradually along with progressive reduction of BMI following bariatric surgery, which may be due to the mechanical reduction of fatty tissue in orbit as well as the reduction of leptin level after bariatric surgery.
In normal populations, choroidal thickness differs topographically across the choroidal tissue and decreases from the fovea to the outer locations.61,78 Furthermore, it has been shown that the superior and temporal areas of the choroid are the thickest quadrants, and the nasal area is significantly the thinnest quadrant across the horizontal choroidal scans.91,92 In line with the findings of normal subjects, previous studies on the obese population indicated that choroidal thickness significantly reduced toward nasal regions. These findings show that topographical variations across the choroid of obese people are similar to normal-weight people.76,78
The association between obesity and choroidal thickness might be attributed to the development of obesity comorbidities such as diabetes mellitus, hypertension, dyslipidemia, cardiovascular diseases, stroke, and ischemia.7,8,21,22,84 It is hypothesized that microvascular changes secondary to obesity in these associate diseases may contribute to choroidal thickness changes with the same mechanisms in obese patients.54,61,65 Several studies have speculated that identification of choroidal thickness changes in obese patients could be an early and noninvasive biomarker of the following vascular changes in the body.29,76
Conclusion
CT variations in obese people can be explained by biological changes in the circulatory system; however, precise mechanism has not been well established. Besides, available data are limited, and therefore many of these findings are inconclusive. In essence, the available literature appears inadequate to explicitly establish the association between choroidal thickness and obesity. It is suggested that future cohort studies examine choroidal thickness in people with a wide age range from childhood to the elderly. Furthermore, prospective follow-ups of subjects with different stages of obesity, from abnormally underweight to morbid obesity, could help understanding the trend of choroidal thickness changes in different weight conditions. Another challenging aspect of choroidal thickness investigation is the method of measurement. State-of-the-art technologies that incorporate high-resolution OCT modalities having automatic choroidal delineation are recommended to enhance the accuracy of the choroidal image recordings.
Footnotes
Acknowledgements
The authors would like to thank Dr. Asieh Ehsaei and Dr. Javad Heravian for their guidance before starting the research project and Dr. Hosein Hoseini-Yazdi for his valuable advice regarding the related articles in the field of the choroid
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Not applicable.