
Abstract
Objectives:
To study the clinical features, optical coherence tomography (OCT) findings, treatment options and follow-up outcomes of post-fever retinitis (PFR).
Subjects:
A total of 19 eyes of 13 patients, diagnosed with PFR (retinitis following febrile episode) over 2 years were retrospectively studied.
Methods:
Documented history, baseline clinical features and systemic investigations performed for PFR were reviewed. Fundus findings, foveal architecture on swept-source OCT, the treatment options and the follow-up outcomes including best-corrected visual acuity (BCVA) and central foveal thickness (CFT) were reviewed and analyzed.
Results:
Common fundus findings included whitish retinitis lesions (100%), macular star (95%, 18eyes), retinal flame-shaped hemorrhages (63%, 12 eyes), inflammatory retinal vessels (30%, 6 eyes), vitreous hemorrhage (one eye) and OCT findings included neuro-sensory detachment (79%, 15 eyes), intraretinal white dots (89.5%,17 eyes). The baseline median log MAR BCVA and CFT were 1.30 (interquartile range (IQR):0.8–1.8) and 423 microns (IQR:182–555). Overall, nine patients (12 eyes) received a combination of oral doxycycline and oral steroids and four patients (7 eyes) received a combination of oral doxycycline, oral steroid and intravitreal anti-vascular endothelial growth factor (IVA). Significant improvement was evident at 8 weeks in median BCVA (0.50, IQR: 0.3–0.8, p < 0.05) and median CFT (223 micron, IQR: 170–256, p < 0.05) though only 26% (5 eyes) attained BCVA > = 6/12.
Conclusion:
Our study puts forth certain characteristic fundus and OCT features of PFR. A combination of oral doxycycline and oral steroids as a treatment option showed improvement in BCVA and CFT. Additional IVA helps in faster visual recovery in patients presenting with severe macular edema at onset.
Introduction
Post-fever retinitis (PFR) is characterized by multifocal cotton wool spot like lesions, predominantly at the posterior pole, and is known to manifest 2 to 4 weeks following the onset of fever.1–3 It has been described in association with various viral, protozoal, and bacterial systemic infections like chikungunya, dengue, West Nile fever, rickettsiosis, rift valley fever, typhoid and rubella.4–10 However, the exact etiology is not clear.1–3 The pathophysiology of PFR is considered para infectious by some authors and immune-mediated by others due to reasons like bilateral symmetrical presentation and clinical response to steroids.1–3 The treatment options are not yet standardized and hence empirical treatment targeting the probable causative organism and the inflammatory process is used, consisting of antibiotics, steroids and intravitreal anti-vascular endothelial growth factor (IVA) agents.1–3 Literature is sparse in describing the clinical features, management options and treatment outcomes of PFR. Hence, we conducted a retrospective study to analyze the various retinal manifestations, optical coherence tomography (OCT) findings, treatment given and follow-up outcomes of PFR patients who presented to us over 2 years.
Materials and methods
This is a retrospective case series study conducted at Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, a tertiary eye care center in Northern India. Patients who were diagnosed with PFR from April 2017 to April 2019 were included in the study. The study adhered to the Declaration of Helsinki and ethical clearance from the Institutional Ethics Committee All India Institute of Medical Sciences was obtained (approval number IEC-510/2020).
Patients diagnosed to have retinitis with a recent history of febrile illness (fever preceding the onset of ocular symptoms) were included in the study. Those who were suspected of having presumed herpetic and toxoplasma retinitis were excluded from our study. Baseline parameters studied included a detailed history regarding the onset of fever, associated rashes, time of onset of ocular symptoms after the febrile episode, treatment received before presenting to us, best-corrected visual acuity (BCVA) (converted to log MAR BCVA) and fundus findings. Baseline fundus photography and swept-source optical coherence tomography (SSOCT) (DRI OCT Triton, Topcon Inc, Japan) were performed. The central foveal thickness (CFT) and the retinal architecture at the fovea were studied with SSOCT. Macular edema was termed severe when CFT was greater than 800 microns. Fundus fluorescein angiography was not performed in all cases as the diagnosis and management were based on history, clinical findings and SSOCT data. Due to the retrospective nature, a proper protocol for systemic investigations was not followed in all cases. When performed, a standard set of investigations including—human immunodeficiency virus (HIV), Venereal Disease Research Laboratory (VDRL) test for syphilis, Hepatitis B surface antigen (HBsAg) test, immunoglobulin (Ig) G and IgM for chikungunya and Lymes, Widal for typhoid and Weil Felix (OX 2, OX K, OX 19) for Rickettsia were performed. Diabetes and hypertension were ruled out in all patients.
The treatment protocol was individualized based on baseline clinical presentation, previous treatment received by the patient and the clinical response of the patient. All patients were started on oral doxycycline (D) 100 mg twice a day and oral steroid (S) (oral prednisolone one mg/kg day, maximum dose not exceeding 60 mg per day) was initiated 5 to 7 days after starting oral doxycycline (D + S group). In case of vitreous hemorrhage (due to inflammatory fundus neovascularization causing media haze of any grade) or severe macular edema, IVA (bevacizumab 0.05 ml–1.25 mg per 0.1 ml) was injected at the time of initial treatment along with oral doxycycline and oral steroid (D + S + A group).
The response was assessed at weeks one, two, four and eight from the first day of initiation of treatment. At the end of two weeks, the following parameters were considered to assess the response: (1) improvement in Snellen’s BCVA by at least two lines, (2) reduction in size of retinitis lesions, and (3) reduction in central macular thickness by > 20%. The response was termed positive if at least two of the three above-mentioned factors were present.
If there was a positive response, tapering of oral steroids over 6 weeks was initiated and oral doxycycline was stopped at the end of 4 weeks. In cases of negative response with persistence of macular edema, IVA was given and tapering of oral steroids was delayed (according to each patient’s response).
Statistical analysis was performed using Microsoft Excel version 16.34 and GraphPad Prism 8 version 8.4.1. p-value < 0.05 was considered significant. Counting finger close to face and Hand movements close to face were assigned the logMAR units of 1.85 and 2, respectively. The normality of the data was checked with the help of the Shapiro-Wilk test. The relationship between continuous variables and the comparison groups (paired) were assessed through either t-tests if the continuous variables were normal, or through non-parametric Wilcoxon tests if the continuous variables were not normal. Inter-group (unpaired) analysis was done using the Mann–Whitney test.
Results
A total of 19 eyes of 13 patients were retrospectively enrolled. The mean average age was 26.3 years (13–45 years). Of the 13 patients, 46% (six) were males and 54% (seven) were females. Rashes (papulo-macular rashes in the forearm according to patient history) were associated with fever in 30% (four) of the patients. The average time for the development of ocular symptoms from the initial systemic features was 4 weeks (range: 2–8 weeks). Standard systemic investigation results, as mentioned above, were available for 9 out of the 13 patients. HIV, VDRL, HbsAg and Lymes results were negative in all nine patients, but Widal (IgG), chikungunya and Weil Felix antibodies were positive in three, two and one cases, respectively (Table 1).
Laboratory Results, Treatment Given and Visual Outcomes Of The Individual Patients.

A, Intravitreal Anti-vascular endothelial growth factor (bevacizumab); BL, Bilateral; D; Oral doxycycline; NA, Not available; S, Oral prednisolone; UL, Unilateral.
The median baseline log MAR BCVA was 1.30 with interquartile range (IQR) of 0.8–1.8. On clinical examination, all eyes had whitish retinitis lesions, 84% (16 eyes) had vessel wall exudation, 95% (18 eyes) had macular star and 63% (12 eyes) had retinal flame-shaped hemorrhages. Inflammatory new vessels were seen in six eyes (30%) along with the inflammatory lesions. Vitreous hemorrhage with faintly visible retina was the presenting feature in one eye. On evaluating the OCT features, the median CFT was 423 microns (IQR: 182–555), with 31% of patients having CFT less than 250 microns, 42% having CFT in the range of 250 to 500 microns and 27% having > 500 microns CFT. One eye had foveal atrophy with a CFT of 40 microns and loss of ellipsoid zone on initial presentation. Four eyes had severe macular edema (CFT > 800 microns). A scatter plot correlating the baseline BCVA and baseline central macular thickness (CMT) showed positive correlation (Pearson correlation coefficient r = 0.4493) (Figure 1) . Other OCT findings included pre-retinal vitreous cells in all eyes, neurosensory detachment (NSD) at macula in 79% (15 eyes), white dots at outer plexiform layer level in 89.5% (17 eyes), inner retinal hyper-reflectivity in 100% and outer retinal corrugations in 68.5% (13 eyes).
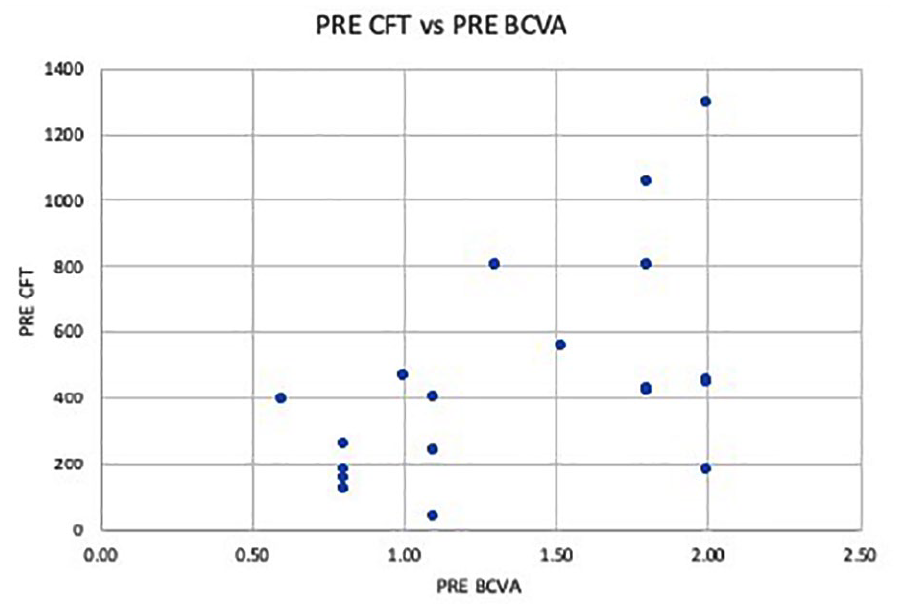
Scatter plot correlating the baseline best-corrected visual acuity (BCVA) (in log MAR) and the baseline Central foveal thickness (CFT) in microns, shows that higher CFT values were associated with poorer BCVA (positive correlation) with Pearson correlation coefficient (r) = 0.4493.
Nine patients of the total 13 patients were treatment naïve. Three patients had already been started oral steroids elsewhere (oral prednisolone 1 mg per kg per day) without oral doxycycline and one patient was receiving anti-viral (oral valacyclovir) with poor response. The three patients who were receiving only oral steroids were additionally started on 100 mg BD oral doxycycline and the patient who was on anti-viral treatment was started on 100 mg BD oral doxycycline and oral steroid and the anti-viral was stopped. Fourteen eyes (74%, 14/19 eyes) (including treatment naïve and treated elsewhere) were given a combination of oral doxycycline and oral steroid (D + S group) therapy. Twelve eyes (12/14 eyes) of the D + S group showed a positive response on day 14. The remaining two eyes (2/14 eyes) showed persistent retinitis lesions and macular edema and hence received IVA (D + S + A group) along with the pre-existing treatment. These two eyes showed positive response following the anti-vascular endothelial growth factor (VEGF) therapy.
A total of five eyes (5/19 eyes): One eye which had vitreous hemorrhage due to inflammatory neovascularization of disk (NVD) and four eyes which had severe macular edema (CMT > 800 microns) on initial presentation, were treated with IVA, oral doxycycline and oral steroids (D + S + A group) directly on the initial visit. All five eyes showed positive response. Once the response was found to be positive, steroids were tapered over 6 weeks. Oral doxycycline was stopped at 4 weeks in all cases. All patients who were given intravitreal anti-VEGF received only one dose of the same.
The median BCVA at the end of 8 weeks was 0.50 (IQR: 0.3–0.8). 26% (five eyes) attained a Snellen’s BCVA of 6/12 or more and 100% attained a Snellen’s BCVA of 6/60 or more. There was a significant improvement in visual acuity overall (p < 0.05), in the D + S group (p < 0.05) as well as in the D + S + A group (p < 0.05). (Figure 2) The median CFT at the end of 8 weeks was 223 microns (IQR: 170–256) with significant improvement overall and within the groups (p < 0.05). Ellipsoid zone disruption was present in four eyes on OCT. The visual outcomes and treatment options of individual patients are listed in Table 1. A comparison of BCVA and CFT between the two groups: (D + S) and (D + S + A) is given in Table 2. Sample case images are shown in Figures (3–6).
Comparison between best-corrected visual acuity and central foveal thickness between two groups: D + S + A and D + S. It is seen that comparable improvement in BCVA and CFT was seen in both the groups, though the pre-treatment BCVA and CFT were significantly worser in Group D + S + A than in Group D + S. (BCVA—best corrected visual acuity, CFT—central foveal thickness, D—oral doxycycline, S—oral steroid, A—intra vitreal anti vascular endothelial growth factor (bevacizumab), IQR—inter quartile range).


Comparing the visual outcomes between the two groups. It can be seen that baseline mean log MAR BCVA was better in the D + S group when compared to the D + S + A group. But the final BCVAs of the two groups at the end of 8 weeks were comparable. Significant improvement (p < 0.05) in BCVA (Refer Table 2) was seen in both the groups.

Sample fundus photographs of the study patients showing characteristic features of post-fever retinitis. (a) inflammatory new vessels (dotted oval), (b) inflammatory new vessels (arrow), (c) perivascular arterial exudation, and (d) perivascular venous exudation. All images show retinitis patches over the posterior pole along with macular star formation due to hard exudates.

Swept-source OCT of a patient with post-fever retinitis showing huge neurosensory detachment with pre retinal and subretinal hyperreflective white dots. Intraretinal cysts and Subretinal hyperreflective fibrinous exudation can also be seen. The central foveal thickness was 1052 µm. (b) Clinical photograph showing whitish retinitis lesions along with superficial hemorrhages.

(a) Swept source optical coherence tomography of right eye of a sample case showing vitreous cells, retinal thickening and corrugations with outer layer cystic spaces and white dots. The initial Central foveal thickness (CFT) was 403 microns. (b) Fundus photograph shows retinitis patches with hemorrhages, macular star and peri-vascular (veins) cuffing. Four weeks following treatment with oral steroids and oral doxycycline (c) the CFT reduced to 250 microns with resolution of retinal thickening. (d) The retinitis lesions showed resolution on fundus examination.

(a) Fundus photograph showing left eye of a sample case showing retinitis and hard exudates with (b) huge neuro sensory detachment (NSD) (central foveal thickness (CFT) = 804 microns), retinal thickening and retinal white dots visible on Swept-source optical coherence tomography (SSOCT). Four weeks following treatment with Oral doxycycline, oral steroids and intravitreal bevacizumab (c) the fundus lesion showed resolution with (d) reduction of the NSD on SSOCT (CFT = 270 microns). (e and g) Fundus photography and SSOCT of another case showing retinitis with vitreous hemorrhage secondary to inflammatory new vessels over the optic disk. (f and h) Eight weeks following the same treatment regimen as the previous case vitreous hemorrhage and the retinitis showed resolution.
Discussion
In our cohort, the retinal lesions were diffuse, smoky white, localized on the posterior pole and were associated with hard exudates and retinal hemorrhages (figures). The most common findings in association with retinitis were complete or incomplete macular star (95%), vessel wall exudation (84%) and retinal flame-shaped hemorrhages (62%). Stellate maculopathy or macular star, first described by Leber, is a prominent finding in conditions affecting the optic disk, like neuro-retinitis and malignant hypertension and is due to the leaky optic disk vasculature. 11 The lipid-rich exudates accumulate in the outer plexiform layer in a patterned fashion due to the arrangement of nerve fibers and the fluid component may enter the subretinal space causing a NSD.12,13 The presence of macular star in 94% of PFR cases probably implies involvement of optic disk in such cases and hence the etiopathogenesis may be similar to neuro-retinitis and thus treatment strategies may be in accordance to those used for neuro-retinitis.
The reasons for poor initial and final BCVA in some of our patients can be attributed to the retinitis lesions over the macular region and macular edema. Severe macular edema (>800 microns) is one of the important treatable causes of vision loss as seen in our study (Figure 1). A significant improvement in the BCVA was evident overall as well as in the individual groups (Figure 2). However, only 26% of the eyes could attain BCVA > = 6/12 at the end of eight weeks. Final visual acuity was influenced by the ischemic damage and foveal ellipsoid zone disruption caused by retinitis lesions.
The exact pathogenesis of PFR is uncertain. The onset of the ocular symptoms on an average 4 weeks (2–8 weeks) following an episode of fever and the inconclusive laboratory results in our study patients point toward a possible immunological basis in the pathophysiology of PFR. The delay in the onset of PFR from the initial systemic symptoms has been attributed to the corresponding phase for antibody production, immune complex and autoimmune antibody formation. 14 The immunological basis has also been supported by Su and colleagues, 15 in cases of dengue maculopathy as they noted a decrease in complement C3 levels and hypothesized excessive consumption of C3 by the circulating antigen-antibody complexes.
On the other hand, studies on PFR have shown benefit of antibiotics like doxycycline in some of these cases.16,17,18 This may be plausible as some of the cases of PFR occur following infections such as rickettsia and Lyme’s disease which respond well to oral tetracyclines. 19 There are reports of doxycycline also being effective in vitro against viruses like dengue and chikungunya.20,21 Thus, it might have a role in these infections as well.
Three of our patients, started only on steroid treatment from elsewhere presented with aggravated retinitis, and all treatment naïve patients showed better response with antibiotics and sequential steroid therapy. Based on our study, till the exact pathophysiology of PFR is understood we would recommend empirically starting doxycycline in such cases and avoiding oral steroids at least for the first 4–5 days. Later, depending on the status of the retinitis and macular edema, oral steroids (1 mg per kg- tapered over 4–6 weeks) with or without intravitreal bevacizumab may be instituted. Kalhoun and colleagues 22 and Khariallah and colleagues 7 both support starting combination therapy (oral doxycycline and oral steroids) in similar presentations though the addition of oral steroids did not show significant benefits in another retrospective study by Kawali and colleagues. 18 Based on our experience and study results, we infer that oral steroids may help in hastening the visual recovery and in improving the final visual acuity.
Our treatment protocol should not be followed for cases of retinitis due to herpes group of viruses or toxoplasma. We use clinical and imaging characteristics to differentiate between these three types of retinitis as described in an earlier paper of ours. 23 Further randomized comparative clinical trials, with a larger sample size, may be necessary for substantiating a standard treatment protocol.
The role of anti-VEGFs in PFR is gaining importance. It is postulated that there is a rise in VEGF levels in PFR cases due to findings like vascular involvement, presence of severe macular edema and inflammatory new vessel formation. 1 Kawali and colleagues 1 found significant BCVA gain in the group treated with a combination of anti-VEGF and steroids when compared to other individual groups. A total of seven eyes in our study received anti-VEGFs. Among these, four eyes had severe macular edema (CMT > 800 microns) and one eye had vitreous hemorrhage due to inflammatory NVD on initial presentation. The other two eyes were initially started on a combination of oral doxycycline and oral steroids but due to lack of positive response and residual macular edema, IVA was added. All of these eyes responded well to the treatment. The role of IVA in PFR has been discussed by us and Afghar et al. (West nile fever) previously.24,25 Anti-VEGFs may help in faster resolution of macular edema and thereby improving final visual acuity.
This study provides valuable insights into the clinical presentation, fundal examination findings, SSOCT findings and treatment outcomes of the disease. The study also supports the possible role of IVA in PFR cases with severe macular edema, non-resolving macular edema and vitreous hemorrhage. Some limitations of our study include the retrospective design and the small sample size. Further large-scale trials using these treatment guidelines may be helpful in devising a standard treatment protocol for the disease.
Footnotes
Author contributions
DS and RC conceptualized the study. AB and RK helped in data collection. DS and IG analyzed data and wrote the manuscript. RC, NH, and SJV revised the manuscript. AK and RC supervised the study.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethics committee approval in accordance with the Helsinki Declaration. Approved by the Institutional ethical committee, All India Institute of Medical Sciences, New Delhi—Reference number: 510/2020
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All participants were informed verbally and in writing about the study. Informed consent form was signed by participants included in the study.