
Abstract
‘Perifoveal Exudative Vascular Anomalous Complex’ (PEVAC) is a perifoveal, unilateral, isolated, perifoveal aneurysm, in otherwise healthy patients. Here, we report a case of PEVAC in a highly myopic eye of a 86-year-old woman affected by a visual decline in the right eye (best-corrected visual acuity of 20/100). She had no other relevant past conditions and/or ocular impairment. Fundus examination in the right eye showed myopic chorioretinal degeneration with a concomitant PEVAC. Structural optical coherence tomography (OCT) showed a round lesion with a hyperreflective wall associated with intraretinal cystic spaces. OCT-angiography nicely disclosed an isolated large aneurysmal retinal dilation featuring the PEVAC with detectable flow in superficial capillary plexus, deep capillary plexus, and avascular slab. This case highlights the importance of discerning between different vascular disorders of the macula, in order to be able to offer the right treatment and/or follow-up to the patient.
Keywords
‘Perifoveal Exudative Vascular Anomalous Complex’ (PEVAC) is a perifoveal retinal vascular abnormality first described by Querques and colleagues 1 in 2011 as a unilateral, isolated, perifoveal aneurysm, in otherwise healthy patients. After the first report, Sacconi and colleagues 2 expanded the spectrum of this new entity reporting the multimodal imaging features in a series of 15 patients. PEVAC typically presents as a perifoveal aneurysmal lesion, associated with intraretinal exudation, sometimes with small retinal haemorrhages and hard exudates. As per definition, PEVAC occurs in healthy subjects, without any signs of not controlled arterial hypertension, diabetes or any other systemic or local vascular disease. However, PEVAC could be associated with other concomitant ocular diseases.2,3
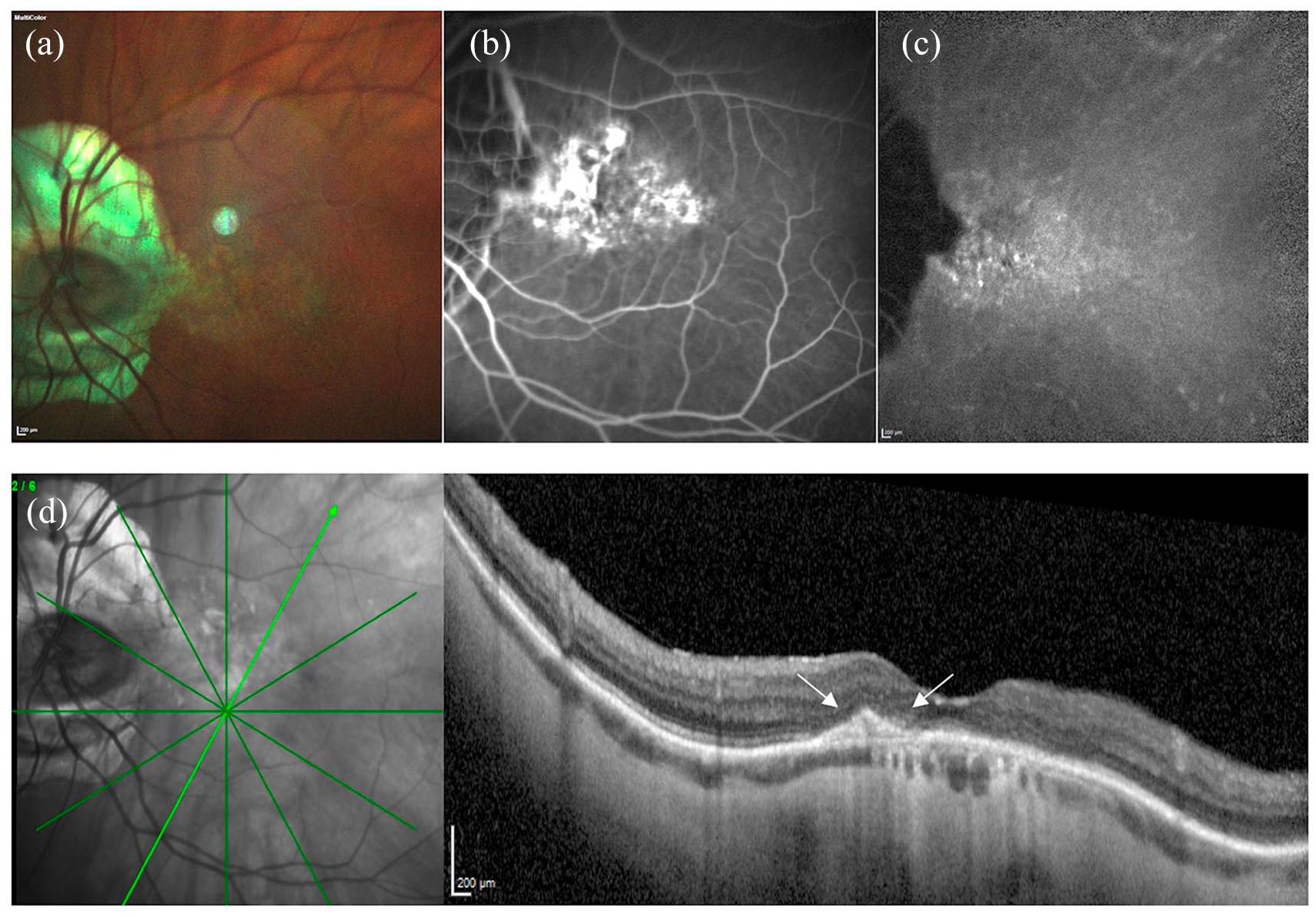
Here, we present a case of an 86-year-old woman affected by high myopia that was referred to the medical retina and imaging unit of our department complaining of a visual decline in the right eye. She was affected by hypertension and hypothyroidism controlled by medications. The patient suffered by pathological myopia with a tilted disc in both eyes, amblyopia and macular neovascularization (MNV) in the left eye, treated by six intravitreal anti-vascular endothelial growth factor (VEGF) injections (the last injection was performed 5 years ago). She had no other relevant past conditions and/or ocular impairment. Best-corrected visual acuity was 20/100 in the right eye (refraction -3.50 diopters) and 20/800 in the left eye (refraction -3.50 diopters). Intraocular pressure was 15 mmHg in the right eye and 16 mmHg in the left one. The patient was pseudophakic in both eyes. The remaining slit lamp examination of the anterior segment was unremarkable. The axial length was 26.48 mm and 26.96 mm in the right and left eye, respectively. Fundus examination in the right eye showed myopic chorioretinal degeneration with a concomitant PEVAC (Figure 1(a)). Fluorescein angiography (FA) and indocyanine green angiography showed a well-defined hyperfluorescent retinal lesion, with slight leakage in the late frame of FA examination (Figure 1(b) and (c)). Structural optical coherence tomography (OCT) showed a round lesion with a hyperreflective wall associated with intraretinal cystic spaces (Figure 1(d)). OCT-angiography nicely disclosed an isolated large aneurysmal retinal dilation featuring the PEVAC with detectable flow in superficial capillary plexus, deep capillary plexus (DCP) and avascular slab (Figure 1(e)). Fundus examination in the left eye showed myopic chorioretinal degeneration complicated by a subfoveal fibrovascular lesion (Figure 2). The choroidal thickness (measured as the average value between three measurements: subfoveally, 1000 μm nasally to the fovea, and 1000 μm temporally to the fovea) was reduced in both eyes (167 μm and 138 μm in the right and left eye, respectively). However, the choroidal thickness of the right eye was much thicker focally under the fovea in comparison with the other areas and with the left eye. Due to the proximity of the lesion to the fovea, we did not perform laser photocoagulation of PEVAC. During the follow-up, a spontaneous resolution of intraretinal cystic spaces was recorded without any treatment after 6 months. The study protocol complied with the tenets of the Declaration of Helsinki and written informed consent for the publication of the data was obtained.

Multimodal imaging evaluation of the patient with Perifoveal Exudative Vascular Anomalous Complex (PEVAC) in the right eye. (a) Multicolor® imaging showing an isolated large aneurysmal retinal dilation featuring the PEVAC (white arrow), with concomitant myopic chorioretinal degeneration. (b and c) Late frame of fluorescein angiography (FA) (b) and indocyanine green angiography (ICGA) (c) showing a well-defined hyperfluorescent retinal lesion with slight leakage on FA examination and no leakage at ICGA. (d) Two different slabs of combined infrared reflectance and horizontal structural optical coherence tomography passing through the lesion showing a round aneurysmal lesion (white arrows) with a hyperreflective wall and intraretinal cystic spaces. (e) optical coherence tomography (OCT)-angiography images and corresponding B-scans with flow well show the PEVAC lesion as an isolated large aneurysmal retinal dilation with detectable flow in the superficial capillary plexus (first panel), deep capillary plexus (second panel) and avascular slab (third panel) (white arrows). Of note, no other telangiectatic lesions are shown around PEVAC.
Multimodal imaging evaluation of the myopic patient in the left eye. (a) Multicolor® imaging showing an oblique insertion of the optic disc (i.e. tilted disc) with an atrophic peripapillary halo and concomitant myopic chorioretinal degeneration. (b and c) Late frame of fluorescein angiography (b) and indocyanine green angiography (c) showing an irregular and spread hyper and hyporeflective alteration involving the foveal area. (d) Combined infrared reflectance and structural optical coherence tomography passing through the fovea showing a well-defined subretinal hyperreflective lesion (white arrows) without evidence of exudation.
Although PEVAC could be included in the spectrum of idiopathic retinal vascular abnormalities, it should be differentiated from other vascular diseases of the macula, like type 1 macular telangiectasia (MacTel). MacTel 1, especially subtype 1B, typically presents in young patients as focal exudative telangiectasia limited to two clock hours in the juxtafoveal area, with intraretinal microangiopathy affecting both the superficial and DCP. On the other hand, PEVAC affects older patients with a well-defined and isolated aneurysmal lesion without other dilated telangiectatic capillaries. Furthermore, in contrast to MacTel 1, PEVAC did not usually respond to anti-VEGF therapy. 4
Similarities with type III MNV have been drawn. In detail, the earliest forms of type III MNV, namely ‘nascent type 3’, are typically associated with very minimal fluid/no exudation and they are characterized by a vascular proliferation originating from the DCP. 5 However, nascent type III MNVs are associated with downwards growth towards the retinal pigment epithelium (RPE) and displayed exudation only when the intraretinal lesion progressed into the RPE and sub-RPE space from the DCP. 5 On the other hand, PEVAC does not show any sign of a downwards progression from the DCP to the RPE and displays a very different morphology versus type III neovascularization (PEVAC appears as retinal vascular abnormalities with an isolated aneurysmal dilation characterized by a round lesion with a reflective wall surrounding a lumen).
Commonly, PEVAC is unresponsive to intravitreal anti-VEGF therapy, but it could display a spontaneous resolution of intraretinal cystic spaces without any treatment. 2 Furthermore, also focal laser photocoagulation is shown to be effective in the treatment of this disorder. 3
Lesions occurring in PEVAC disease are frequently permanent, but they are usually not progressive and cause a moderate impact on vision. Very often, PEVAC is misdiagnosed with other macular diseases. This case highlights the importance of discerning between different vascular disorders of the macula, in order to be able to offer the right treatment and/or follow-up to the patient.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: none of the authors received financial or material support for the research and the work from any of the following organizations: National Institutes of Health (NIH), Wellcome Trust, Howard Hughes Medical Institute (HHMI), and other(s). No conflicting relationship and financial interest exists for any author.