
Abstract
Introduction:
The ILUVIEN® (fluocinolone acetonide) Clinical Evidence in Portugal (ICE-PT) study is a retrospective, multicenter, observational study evaluating the effectiveness and safety of the FAc implant in patients with diabetic macular edema.
Methods:
Patients included in this study had received the 0.2 µg/day fluocinolone acetonide implant for the treatment of diabetic macular edema and had measurements of visual acuity and retinal thickness assessed by optical coherence tomography for at least 12 months pre- and post-fluocinolone acetonide implant administration, with ⩾2 follow-up visits. Outcomes measured included visual acuity, central foveal thickness, and intraocular pressure.
Results:
There was a significant increase in mean visual acuity compared with baseline at 3, 6, 9, and 12 months post-fluocinolone acetonide in both the overall study population and the pseudophakic subgroup (p < 0.05 at all time points in both groups). A significant reduction in mean central foveal thickness compared with baseline was seen in the overall study population at 3, 6, 9, and 12 months post-fluocinolone acetonide (p < 0.05 at all time points). At 12-month post-fluocinolone acetonide, a small but significant intraocular pressure increase of 1.0 mmHg was seen in the overall study population.
Conclusion:
The results of this analysis show that switching from the current standard of care to the fluocinolone acetonide implant leads to beneficial effects in terms of vision and retinal structure in patients with diabetic macular edema and that patients benefited from FAc implant administration, regardless of lens status.
Keywords
Introduction
Diabetic retinopathy (DR) was the fifth most common cause of blindness and moderate-to-severe vision impairment (MSVI) worldwide in 2010. 1 In 2010, 1.9% of MSVI and 2.6% of blindness worldwide was a result of DR; this represented an increase from 1.3% and 2.1%, respectively, over the preceding decade. Also, in 2010, 4.2% of blindness and 3.0% of MSVI in Western Europe – the region including the United Kingdom and Portugal – was caused by DR. 2 DR affects almost 100 million people worldwide and can lead to diabetic macular edema (DME), which is the most common cause of vision loss in patients with DR. 3
Current DME treatments include focal/grid thermal laser photocoagulation, intravitreal corticosteroid injections, and intravitreal anti-vascular endothelial growth factor (VEGF) therapy,4,5 the latter being recommended as first-line treatment for DME. 6 Randomized clinical trials have shown that, after 2 years of intensive anti-VEGF therapy, more than 35% of patients with DME fail to achieve ⩾10 letter improvement in best-corrected visual acuity (VA) and more than 55% of patients fail to achieve ⩾15 letter improvement. 7 In addition, anti-VEGF therapy requires multiple injections and follow-up appointments, leading to a substantial treatment burden that is difficult to sustain in a real-world setting. 8
Evidence in the literature supports the rationale for treating DME with intravitreal corticosteroids. DME is a multifactorial disease involving a variety of aqueous humor cytokines, so it is reasonable to use both anti-neovascularization and anti-inflammatory agents in its treatment. 9 Unlike anti-VEGF, corticosteroids have the potential to reduce both the levels of VEGF and the inflammatory response. These combined effects result in reduced vascular permeability and edema in the eye.10,11 In treatment naïve eyes and eyes not responsive to anti-VEGF agents, early switching to intravitreal corticosteroids has been shown to be beneficial. 12 Furthermore, real-life studies have been published on the effectiveness and safety of intravitreal corticosteroids for the treatment of DME.13–16
The fluocinolone acetonide intravitreal implant (FAc, ILUVIEN®, Alimera Sciences Limited, UK) is indicated for the treatment of vision impairment associated with chronic DME, which is considered persistent or recurrent despite treatment. 11 The intravitreal implant delivers a continuous microdose (0.2 µg/day) of FAc via a single injection and lasts for up to 36 months, 8 consequently reducing the treatment burden compared with other approved therapies, including anti-VEGF and short-acting corticosteroids. 11
The aim of the ILUVIEN Clinical Evidence in Portugal (ICE-PT) study was to evaluate the effectiveness and safety of the FAc implant in patients with DME that persists or recurs despite treatment. Patients with DME were evaluated using data collected for 12 months pre- and post-FAc implant administration. The objectives of the ICE-PT study were (a) to monitor DME progression 12 months pre- and post-FAc implant administration in a multicenter cohort in Portugal, (b) to test the hypothesis that switching from the current standard of care (SOC) to the FAc implant would lead to beneficial effects (stabilization or improvement) in terms of vision and retinal structure in patients unresponsive to prior therapies, and (c) to assess vision and retinal structure outcomes based on lens status.
Materials and methods
Study design
The ICE-PT study is a retrospective, multicenter, observational study of patients with DME treated with the current SOC prior to FAc implant administration. In this multicenter, hospital-based study, data were taken from patient medical records. Data collection was secondary, as the data used for this study were initially collected for purposes other than research. Data were collected from a representative cohort of people treated at four participating hospitals in Portugal and combined into a single dataset for the purposes of analysis. These data were pseudonymized and entered an outline data entry tool, where center and subject identifiers were added. Data generated from retrospective case reviews were entered by the consultant themselves or by other members of the healthcare professional’s team.
Data included demographics, medical history, implant data, and data from multidisciplinary and medication reviews at several time points within a 2-year period (1 year pre- and post-intravitreal injection of the FAc implant). Quantitative data were generated from medical records, administrative records, and clinical measurements and were collected only for the parameters that were necessary to answer the research objectives. Summaries by site were not performed other than for analysis relevant to evaluation of their healthcare service. No data linkage took place in the course of this project. At no point did Alimera Sciences, the manufacturer of ILUVIEN, have access to the data.
Inclusion criteria
Patients who received the 0.2 µg/day FAc implant for the treatment of DME were included in the study if they had records that included measurements of VA and retinal thickness by optical coherence tomography for at least 12 months pre- and post-FAc implant administration and ⩾2 follow-up visits.
Outcome measures and subgroup analyses
Outcomes measured included VA [Early Treatment Diabetic Retinopathy Study (ETDRS) letters score], central foveal thickness (CFT), and intraocular pressure (IOP). CFT was measured using either time-domain (TD) or spectral-domain (SD) optical coherence tomography (OCT). In addition to analysis of the full population, eyes were divided by lens status into the following three subgroups: pseudophakic (eyes that were pseudophakic from baseline), phakic (eyes that were phakic from baseline), and phakic to pseudophakic (eyes that were phakic at baseline but underwent cataract surgery within 12 months of FAc implant administration).
Data and statistical analyses
Mean and standard error of the mean were calculated for VA, CFT, and IOP at 12 months pre-FAc, baseline, and 3, 6, 9, and 12 months post-FAc injection. Values were compared using Wilcoxon t-test.
VA
VA was recorded as ETDRS letters. In this article, stabilization of vision was defined as the percentage of patients with a change of ±4 ETDRS letters from baseline. An improvement was a change in VA of ⩾5 letters from baseline. Stabilized/improved vision was therefore defined as a VA change from baseline of ⩾−4 ETDRS letters. These criteria have been reported in previous studies and consistent with measuring VA outcomes in real-world practice.8,17
IOP
Analysis of IOP was performed for all eyes, except for one that had missing baseline IOP values. Increases in IOP of ⩾10 mmHg were recorded at baseline and 12 months post-FAc implant administration. IOP threshold values of >30 mmHg, >21 mmHg, and ⩽21 mmHg were recorded at 12 months pre-FAc and 12 months post-FAc implant administration.
Results
Ninety-three eyes of 68 patients were included in the study. The full group and patient subgroups are shown in Figure 1. Baseline characteristics are described in Table 1.

Enrolled patients by subgroup.
Baseline characteristics and demographics.
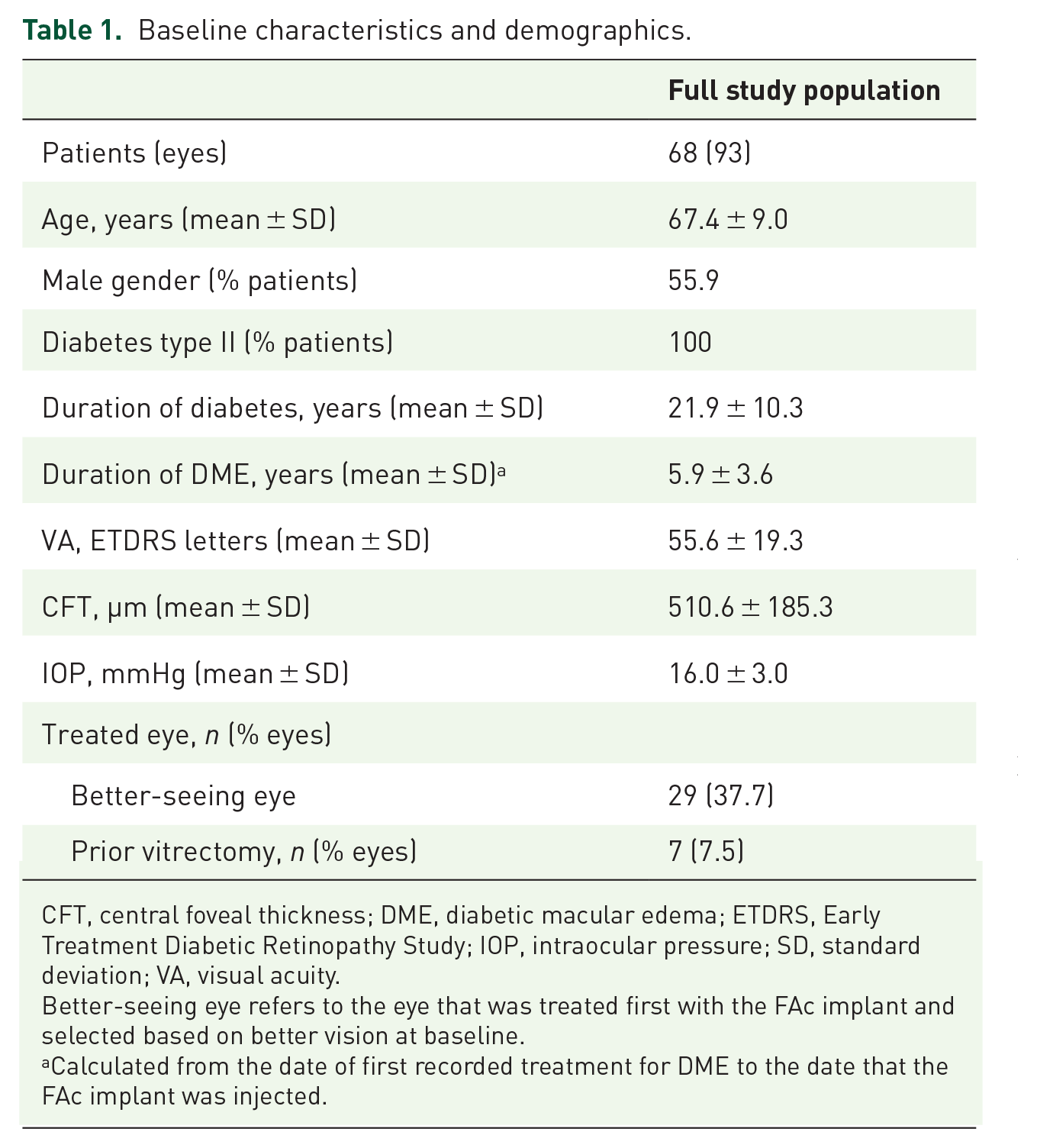
CFT, central foveal thickness; DME, diabetic macular edema; ETDRS, Early Treatment Diabetic Retinopathy Study; IOP, intraocular pressure; SD, standard deviation; VA, visual acuity.
Better-seeing eye refers to the eye that was treated first with the FAc implant and selected based on better vision at baseline.
Calculated from the date of first recorded treatment for DME to the date that the FAc implant was injected.
Patients included in the study had received a range of treatments for DME in the 12 months prior to FAc implant administration. DME treatments included corticosteroids (62.4% of patients, mean 1.4 treatments), anti-VEGF (21.5% of patients, mean 2.2 treatments), and macular laser (14.0% of patients, mean 1.2 treatments).
Effect of FAc implants on VA
In all groups, stable or improved VA was seen in the majority of patients at 12-month post-FAc (Figure 2): overall population, 74.2% maintained/improved VA; phakic group, 68.4%; pseudophakic group, 73.8%; and phakic-to-pseudophakic group, 88.9%. Furthermore, there was a significant increase in mean VA compared with baseline at 3, 6, 9, and 12 months post-FAc in both the overall study population (n = 93 eyes) and the pseudophakic subgroup (n = 65 eyes) (p < 0.05 at all time points in both groups; Figure 3). In the phakic subgroup (n = 19 eyes), a significant increase in mean VA compared with baseline was seen at 3 and 6 months post-FAc (p < 0.05 at both time points; Figure 3). A peak in mean VA was observed at month 6, followed by numerical – but not significant – increases compared with baseline at months 9 and 12 post-FAc. This relative reduction in VA from month 6 to months 9 and 12 probably results from cataract formation. In the phakic to pseudophakic subgroup (n = 9 eyes), a numerical decrease in mean VA was seen at 6 and 9 months post-FAc compared with baseline. Phakic eyes underwent cataract extraction up to month 9, and a corresponding increase in mean VA compared with baseline was seen at 12 months post-FAc (Figure 3).

Percentage of eyes with stable or improved VA post-FAc implant administration at month 12.
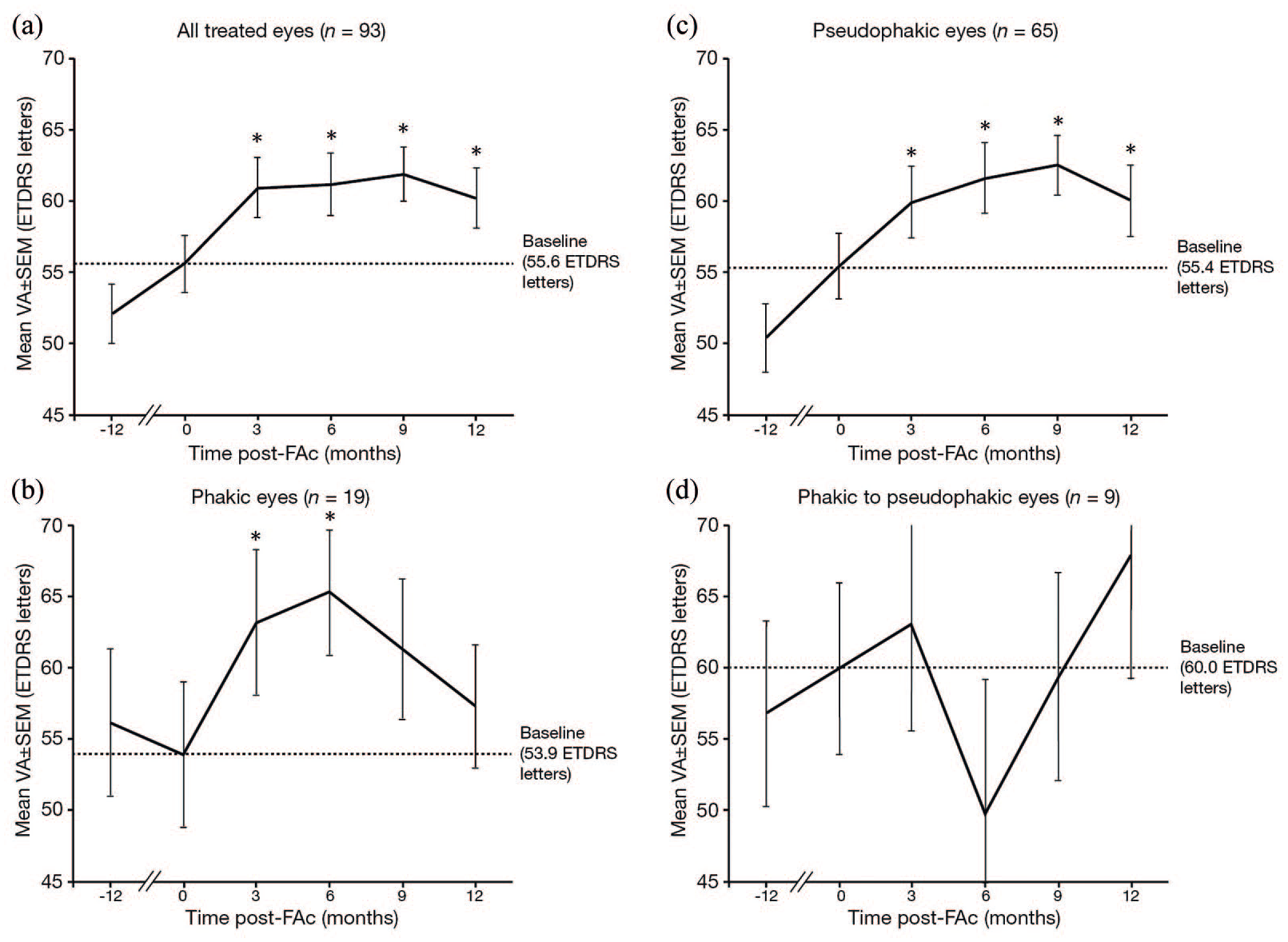
Change from baseline in mean VA following FAc implant administration.
Effects of FAc implant administration on CFT
A significant reduction in mean CFT compared with baseline was seen in the overall study population at 3, 6, 9, and 12 months post-FAc (p < 0.05 at all time points; Figure 4). A similar trend was seen in all patient subgroups, with reductions in mean CFT observed at 3, 6, 9, and 12 months post-FAc implant administration compared to baseline (Figure 4).

Change from baseline in mean CFT following FAc implant administration.
Effects of FAc implant administration on IOP
Prior to FAc implant administration, 37.6% of patients from the overall study population were receiving IOP-lowering medication. At 12 months post-FAc implant administration, a small but significant IOP increase of 1.0 mmHg was seen in the overall study population (Figure 5). Following FAc implant administration, 35.5% of patients remained on IOP-lowering medication, 33.3% required increased dosage or additional medications, and 19.4% initiated IOP-lowering medication. The mean time to receiving IOP-lowering medication post-FAc was 62.7 ± 77.8 days. Increases in IOP were well managed using medication and no patients required IOP-lowering surgery.

Changes in IOP at 12 months pre- and post-FAc implant administration.
Supplemental therapies for DME
An overall reduction in supplemental therapies was seen for the full study population at 12 months post-FAc implant administration compared to 12 months pre-FAc (30.1% versus 76.3%, respectively) (Figure 6). Only the use of macular laser increased (from 14.0% at 12 months pre-FAc to 20.4% at 12 months post-FAc), while the use of all other therapies was reduced at 12 months post-FAc.

Supplemental therapies at 12 months pre- and post-FAc implant administration for the overall study population (n = 93).
Discussion/conclusion
Overall, data from this real-world study in Portugal showed that patients benefited from FAc implant administration, regardless of lens status. This is consistent with results reported by the FAME and ICE-UK studies.10,18,19
Comparison of ICE-PT to a similar study conducted in the United Kingdom (ICE-UK) illustrates regional differences in DME treatment. In Portugal, the most common DME treatment received by patients in the 12 months prior to FAc implant administration was short-acting corticosteroids (62.4% of patients); some Portuguese hospitals recommend their use prior to FAc implant administration to evaluate the effectiveness of the corticosteroids treatment and the risk of increased IOP in an individual. In the United Kingdom, most patients received anti-VEGF (82% of patients) and macular laser therapy (63% of patients) prior to FAc implant administration. 20 In Portugal, patients receive a mean of 2.2 anti-VEGF and 1.4 corticosteroid injections prior to FAc implant administration. In the United Kingdom, a large proportion of patients had received >6 prior DME treatments at FAc implant administration. 20 Supplemental treatment for patients in Portugal tended to be macular laser therapy, whereas in the United Kingdom it was most frequently anti-VEGF therapy. 20 In both countries, anti-VEGF therapy is currently considered the gold standard and the first-line treatment for DME. 20 Differences in DME treatment prior to FAc implant administration in ICE-UK and ICE-PT may be explained by variations in therapy recommendations between the United Kingdom and Portugal. In the United Kingdom, FAc intravitreal implant administration is indicated for treating chronic DME that is insufficiently responsive to available therapies in eyes with a pseudophakic lens, provided that the manufacturer provides the FAc implant with the discount agreed in the patient access scheme. 21 In Portugal, there are no specific limiting indications with regard to lens status for administration of the FAc intravitreal implant. In comparison to ICE-UK, patients in ICE-PT had a longer mean duration of DME. As the patients in this study had a longer mean duration of DME, it may be that anti-VEGF therapy had been prescribed as an initial treatment but had failed to achieve the desired outcome and was consequently discontinued prior to the 12-month observation period before FAc implant administration. If correct, this would explain why so few patients in ICE-PT were receiving anti-VEGF therapy post-FAc implant administration. However, it remains unknown if the FAc implant is considered as a treatment option earlier in Portugal compared with the United Kingdom. Recently published data by Chakravarthy and colleagues 17 showed patients with short-standing DME experienced better outcomes than patients with longer-standing DME. In another study published by Eaton and colleagues, 22 treatment burden was assessed and showed that in patients with the best baseline VA (⩾20/40), VA was maintained and treatment frequency was significantly reduced post-FAc administration. Hence, both studies support better outcomes with the FAc implant when it is adopted earlier in the treatment pathway.
In the ICE-PT study, an early, significant, and sustained increase in mean VA was seen for the overall study population post-FAc implant administration compared to baseline. Improved or stabilized VA was seen in 78.5% of the overall study population at 3 months post-FAc implant administration; this proportion was sustained to month 12.
Anatomical findings showed a similar pattern of improvement in retinal structure in the overall study population and in the lens status subgroups. Reductions in mean CFT compared with baseline were seen within the first 3 months of FAc-implant administration and these reductions were sustained to month 12. This is comparable to results of a similar, albeit smaller, Portuguese study. 23 In the ICE-PT study, there was a numerically greater mean reduction in CFT compared with ICE-UK (−202 µm compared with −125 µm). This may be explained by a higher mean baseline CFT and a smaller number of treatments in the 12 months pre-FAc implant administration for ICE-PT.
In the phakic to pseudophakic subgroup, reduction in CFT was seen at all time points post-FAc implant administration, suggesting a sustained improvement in retinal status, regardless of changes in VA. Changes in VA appeared to be related to the development of cataracts and VA was improved following cataract surgery.
The FAc intravitreal implant has been licensed in 17 European countries for the management of chronic DME when other treatments have proven to be insufficiently effective. 20 The present report supports other real-world studies,8,17 which have shown that patients treated with FAc implant typically have a more chronic DME presentation and more prior therapies than in those in clinical trials. In Europe, the use of the FAc implant is indicated as a second-line therapy and mainly after a sub-optimal response to prior treatment with an anti-VEGF agent. In some studies, the use of a prior corticosteroid has been reported. In the current ICE-PT study, most eyes (62.4%) were treated with a prior corticosteroid, including both intravitreal triamcinolone acetonide and dexamethasone with 1.4 ± 0.8 injections given before therapy with the FAc implant. Further analysis shows that a dexamethasone implant was administered in 25.8% of eyes and an average of 1.13 implants were given per eye (27 implants administered to 25 eyes). The exact timing of these injections relative to the FAc implant were not measured; however, this was determined in another study in Germany, where the average number was 1.27 ± 0.14 dexamethasone implants administered over a period of 6.5 ± 2.7 months prior to the FAc implant. 16
Adverse events following FAc implant administration include IOP elevation and cataract formation, both of which are associated with intravitreal corticosteroid treatment. 10 IOP events reported in this study are comparable to those reported in the USER and IRISS studies, in which IOP events were similar pre- and post-FAc implant administration.17,22 Although FAc is known to accelerate cataract progression, the incidence of cataracts occurs at a much earlier age in diabetic patients regardless of any intervention. Consequently, even in the absence of corticosteroid treatment, most diabetic patients eventually require cataract surgery. 10 In ICE-PT, cataract surgery following FAc treatment resulted in improvements in VA without significant worsening of macular edema. In the FAME study, VA improved irrespective of whether cataract surgery was performed before or following FAc implant administration. 11
One limitation to the ICE-PT study was the small sample size in comparison to other studies such as the ICE-UK and FAME studies.10,18,24 In contrast to these studies, ICE-PT showed that the majority of patients were treated with a prior short-acting corticosteroid as opposed to macular laser in the FAME study or intravitreal anti-VEGF in the ICE-UK study. A comparison of outcomes based on prior therapies was not conducted in this study but would certainly be an interesting comparison to assess their impact on outcomes and to provide insights on expected outcomes. Another limitation of the ICE-PT study was that CFT was measured using either TD or SD-OCT. Over the past two decades, OCT has evolved with the introduction of a new approach, swept-source (SS)-OCT. 25 SS-OCT has improved image penetration and a faster scan rate than TD and SD-OCT and can optimize diagnosis of DR. 25
Overall, these findings support the hypothesis that switching from the current SOC to the FAc implant leads to beneficial effects in terms of vision and retinal structure in patients with established persistent or recurrent DME. The FAc implant also provides an alternative option for patients with compliance problems related to the frequent injections necessitated by the current SOC. The current findings are important to ophthalmologists as they show that, irrespective of lens status, outcomes achieved in real-world practice are consistent with those reported in the pivotal FAME trial.
Footnotes
Acknowledgements
The authors thank SVMPharma for collating the data and thank the contributions of the staff at the ICE-PT centers. The authors would like to acknowledge the support of their colleagues, Dr Meireles, Dr Castro Sousa, and Dr Teixeira, for providing data on their patients treated with the FAc implant and for critically appraising the manuscript.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors made substantial contributions to conception, design, analysis, and interpretation of data and contributed to writing the article and approved the current version. A.C. has participated in advisory boards for Alcon, Alimera Sciences, Allergan, Bayer, Novartis, and Roche. A.M., J.P.C.S., and C.T. report no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Alimera Sciences, the manufacturer of Iluvien 190 mg intravitreal implant, who designed the study and commented on the manuscript. Medical writing assistance was provided by Helios Medical Communications, Alderley Edge, Cheshire, UK and supported by Alimera Sciences.
Ethics statement
This study was authorized by the Comissão Nacional de Protecção de Dados (CNPD) (authorization number 13368/2016, study protocol reference R-01-16-0050) and was approved by each hospital’s Comissão de Ética para a saúde (CES). The lead clinician at each center gave written approval for extraction of anonymized data. This study was conducted in accordance with the Declaration of Helsinki and the Portuguese Data Protection Act.