
Abstract
The separation of the vitreous from the optic nerve head and the macula plays a primary role in the spontaneous resolution of optic disc pit (ODP) maculopathy. Optical coherence tomography (OCT) helps in the non-invasive monitoring of this condition, when treated conservatively. The aim of this report was to describe a pediatric case of spontaneously resolved ODP maculopathy, managed conservatively and monitored by means of spectral domain (SD)-OCT. A 14-year-old girl presented with severe visual loss in the right eye (RE). Fundus examination demonstrated a temporal ODP with altered foveal reflex. The SD-OCT B-scans revealed severe intraretinal schisis-like changes, broad vitreal adhesion in the optic nerve head area, posterior hyaloid thickening, and vitreal entrapment in the premacular space. The patient was managed conservatively. Spontaneous resolution of ODP maculopathy took place over 3 months, with vision improved up to 1.0 (Snellen charts). The macular schisis progressively resolved after posterior vitreous detachment. In conclusion, in our report, a complete restoration of the foveal anatomy was achieved without any surgical intervention. This OCT-based report confirms the role of the vitreomacular abnormalities in the pathogenesis of the disease.
Introduction
First described in 1882, optic disc pit (ODP) is a rare congenital malformation of the optic disc, secondary to a failure in the closure of the superior edge of the embryonic fissure during embryogenesis.1,2 ODP usually remains asymptomatic unless associated with ODP maculopathy, which presents as macular edema, macular schisis, or serous detachment.3,4 Although the exact pathogenesis of ODP maculopathy is not known, different theories about the source of fluid responsible of the above-mentioned macular changes have been proposed, according to which it may be secondary to vitreous penetration in the subretinal space, or to a direct connection between the subarachnoidal and the subretinal or intraretinal space.5,6 Regardless the most likely explanation, vitreous traction appears to be an important factor in the pathogenesis of ODP maculopathy.7,8
We describe a pediatric case of spontaneously resolved ODP maculopathy, in which the role of vitreous traction is emphasized and documented by means of spectral domain–optical coherence tomography (SD-OCT). No identifiable health information was included in this case report.
Case
A 14-year-old girl presented to our department with a 2-week history of severe visual loss in her right eye (RE). Her medical history, as well as her family history, was negative for any macular disorders. Moreover, she did not have any ocular history of previous surgeries and/or treatments. On examination, her best-corrected visual acuity (BCVA) measured with Snellen chart was 0.1 in the RE and 1.0 in the left eye. Intraocular pressure was 14 mmHg in both eyes. The anterior segment examination was unremarkable, while fundus examination demonstrated a temporal ODP (approximate measure of 750 µm) with an altered foveal reflex in the RE. The visual field measured on automated perimetry showed an enlarged blind spot and a central arcuate scotoma in the RE. The SD-OCT B-scans of the macular region revealed a reduced foveal thickness; intraretinal schisis-like changes between the outer nuclear layer and the outer plexiform layer; a broad vitreal adhesion in the optic nerve head area; a diffuse parafoveal vitreomacular traction due to a posterior hyaloid thickening, with significant neuroretinal distortion; and vitreal entrapment in the premacular space (Figure 1(a)). Subfoveal focal interruption of the inner segment–outer segment (IS-OS) band and a defect of the lamina cribrosa at the site of the ODP were also discernible on the tomographic scan. Considering the age of the patient, we decided to observe the clinical course of the disease. Over the next 3 months, the vision of the RE dramatically improved until a BCVA of 1.0, and the macular schisis progressively resolved and spontaneous posterior vitreous detachment from the optic nerve head was noted (Figure 1(b)). The macular anatomy, including the IS-OS band, was perfectly restored (Figure 1(c)). The patient did not undergo ocular interventions during the follow-up period.
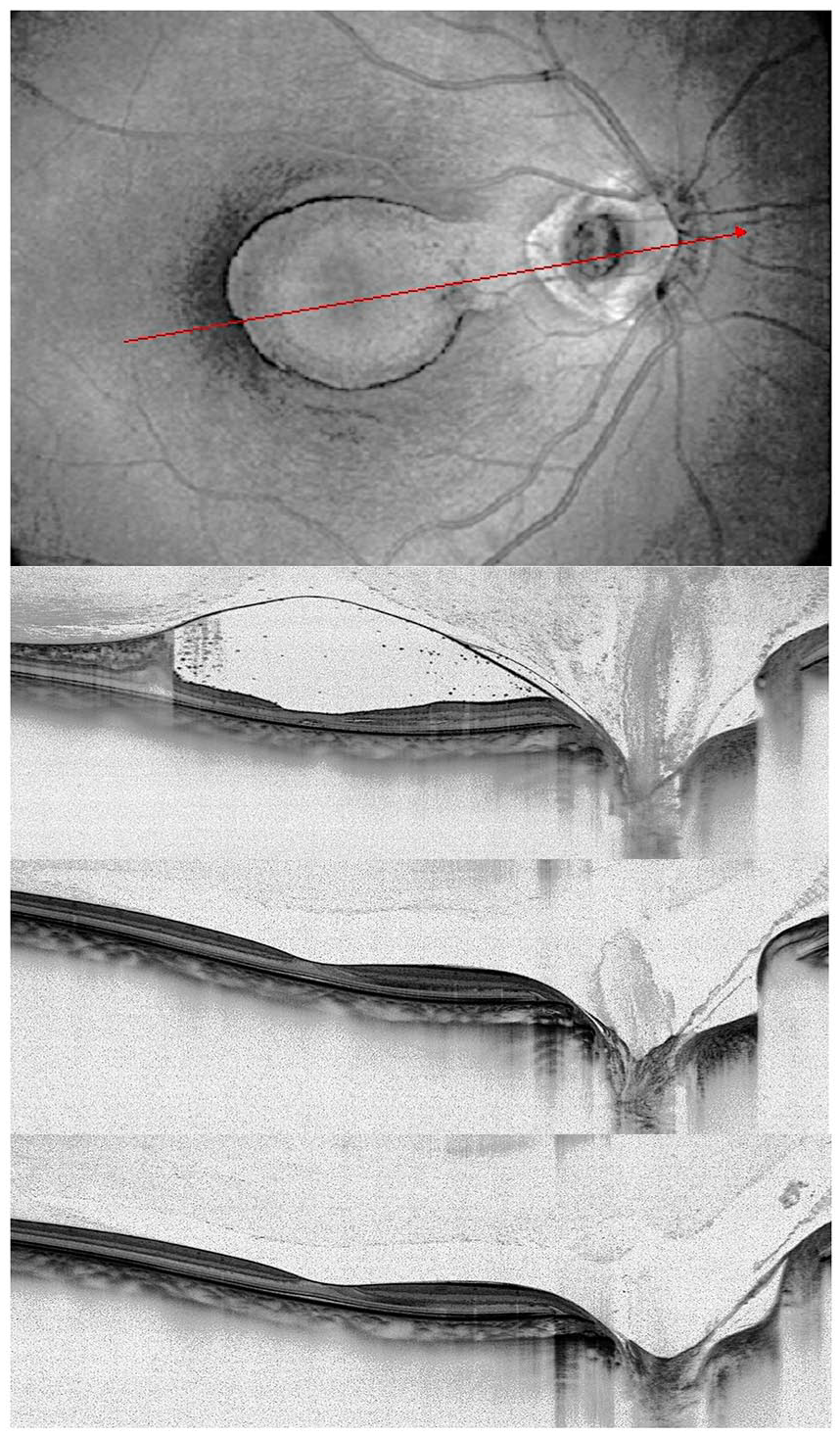
Progressive optical coherence tomography (OCT) of a case of optic disc pit maculopathy, with spontaneous resolution after posterior vitreous detachment.
Discussion
Many interventions have been considered for the treatment of ODP maculopathy, with no consensus regarding the approach which maximizes the surgical success and minimizes the side effects and the potential complications. Laser photocoagulation, 9 vitrectomy with internal limiting membrane peeling,10,11 macular buckling, 12 gas, 13 or silicone tamponade 14 have all been demonstrated to be beneficial in restoring macular anatomy and function, with long-lasting results. As well, cases of spontaneous resolution of ODP maculopathy have been described in the literature.
Regardless of the surgical technique adopted, recent evidences have shown that a separation of the vitreous from the optic nerve head and the macula plays a primary role in the resolution of the disease. 15 Our report clearly depicts the vitreal changes in the peripapillary and in the macular region, from broad adhesion to complete posterior detachment, reinforcing this theory. Indeed, albeit rare, other similar examples of spontaneous resolution of ODP maculopathy have been described in the literature, all featuring a relief of the vitreomacular traction forces in the macular region.16–19 Novelty of this report is the progressive OCT-based documentation of this process.
Of note, we assisted to the complete restoration of the foveal anatomy, with no consequences on the outermost retinal layers and on the final visual acuity.
In conclusion, this report confirms the possibility of spontaneous resolution of the ODP maculopathy in pediatric patients, giving deeper insights on the role of the vitreomacular abnormalities in the pathogenesis of the disease. A wait-and-watch approach may be a valuable option in pediatric patients.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
Approval by an ethical committee was not required since this was a retrospective observational case presentation. Written informed consent was obtained from patient’s parents for future retrospective use and publication of her data.