
Abstract
We present a case with giant arteriovenous aneurysmal malformation with different imaging modalities, including fundus photography, fundus fluorescein angiography, spectral domain optical coherence tomography, and optical coherence tomography angiography. A 43-year-old Turkish female presented with gradual blurred vision in her left eye. Her best-corrected visual acuity was 20/200. The fundoscopic examination revealed hard exudates and microaneurysms around the macula. Spectral domain optical coherence tomography showed cystoid macular edema and serous macular detachment. Fundus fluorescein angiography and optical coherence tomography angiography showed bean-like arteriovenous anastomosis between the inferior venous vascular arcade and the superior arterial vascular arcade. An en face angiogram using optical coherence tomography angiography within the deep capillary plexus also showed venous collateral channels across the horizontal raphe. The patient was diagnosed with arteriovenous aneurysmal malformation in association with type 1 aneurysmal telangiectasia. Ophthalmologists should note that giant aneurysmal lesions can occur in type 1 aneurysmal telangiectasia patients.
Keywords
Introduction
Arterial macroaneurysms, venous macroaneurysms, telangiectatic capillaries, and dilated collateral vessels can develop as consequences of retinal vein occlusion (RVO).1,2 Although the clinical characteristics of arterial and venous macroaneurysms are well defined, it is not completely understood that similar macrovascular changes can occur in RVO. 3 Patients with age-related macular degeneration may be similarly affected by vascular abnormalities called retinal angiomatous proliferation or type 3 lesions. 4 Moreover, type 1 macular telangiectasia is also defined as type 1 aneurysmal telangiectasia, which is characterized by multiple capillary, venular, and arteriolar aneurysms associated with intraretinal microangiopathy and cystoid macular edema. 5 Herein, we present a patient with type 1 aneurysmal telangiectasia and giant arteriovenous aneurysmal malformation with different imaging modalities, including fundus photography, fundus fluorescein angiography (FFA), spectral domain optical coherence tomography (SD-OCT), and optical coherence tomography angiography (OCTA).
Case report
A 43-year-old female presented with gradual blurred vision in her left eye for 10 days. She had no diabetes, hypertension, or major eye disease, and no history of intraocular or periocular interventions. Her family history was negative for any ocular diseases.
On examination, the best-corrected visual acuity (BCVA) was 20/20 in the right eye and 20/200 in the left eye. A biomicroscopic evaluation showed negative findings. The fundoscopic examination revealed hard exudates around the macula, microaneurysms, a few intraretinal hemorrhages, and macular edema in the left eye. The right eye was normal (Figure 1(a) and (b)). SD-OCT showed cystoid macular edema and serous macular detachment (Figure 1(c)). FFA showed bean-like arteriovenous aneurysmal anastomosis between the inferior venous vascular arcade and the superior arterial vascular arcade (Figure 2(a) and (b)). FFA also showed telangiectatic capillaries around the macula (Figure 2(c)). OCTA revealed flow voids in the arteriovenous aneurysmal malformation and en face angiogram within the deep capillary plexus, which showed venous collateral channels across the horizontal raphe (Figures 3–5).
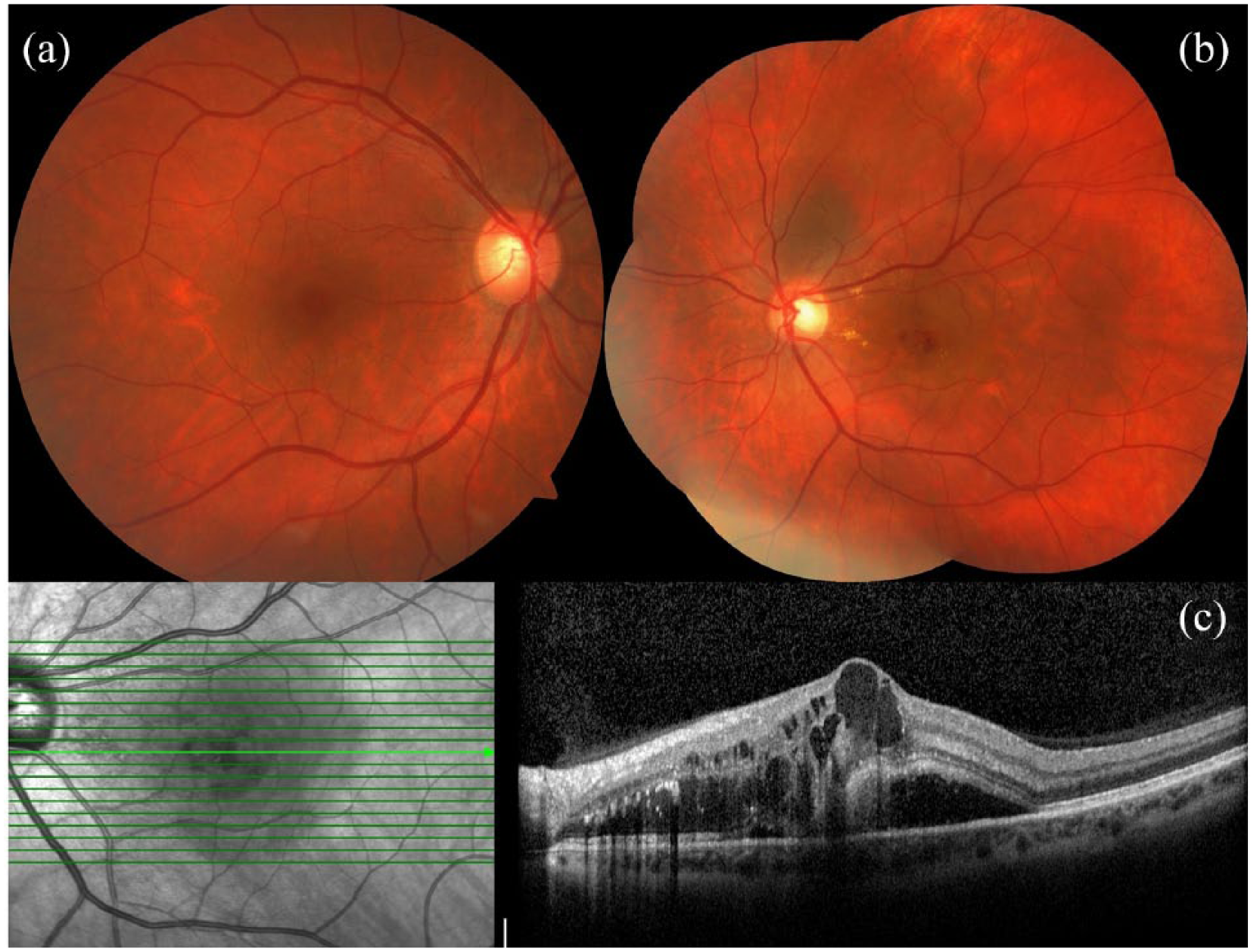
Fundus photographs and spectral domain optical coherence tomography (SD-OCT) images of the case: (a) normal examination of the right eye; (b) hard exudates, microaneurysms, and a few intraretinal hemorrhages were seen around the macula in the left eye; and (c) SD-OCT showed cystoid macular edema and serous macular detachment.

Fundus fluorescein angiography (FFA) images of the case. (a) Arteriovenous phase of the FFA at 15 s. Upper blue arrow shows the superior temporal artery, and lower blue arrow shows the inferior temporal vein. Laminar flow pattern with a railroad track appearance was seen in the filling venules. (b) Still arteriovenous phase of the FFA at 17 s. Red arrow shows an anastomosis between the inferior venous vascular arcade and the superior arterial vascular arcade. (c) Venous phase of the FFA at 32 s. Red arrow shows giant arteriovenous aneurysmal malformation with a bean-like morphology. Blue stars show telangiectatic capillaries and dilated collateral venous channels across the horizontal raphe between inferior and superior vascular arcades.

Optical coherence tomography angiography (OCTA) images of the case: (a) superficial capillary plexus segmentation, (b) deep capillary plexus segmentation, (c) outer retina segmentation of the case, and (d) color overlay images of the lesion. The yellowish part of the image shows the malformation located in the outer retina.

En face images of the case via optical coherence tomography angiography: (a) superficial capillary plexus segmentation, (b) deep capillary plexus segmentation, and (c, d) outer retina segmentation of the case. In (b), red arrows show collateral venous vessels across the horizontal raphe between inferior and superior vascular arcades.
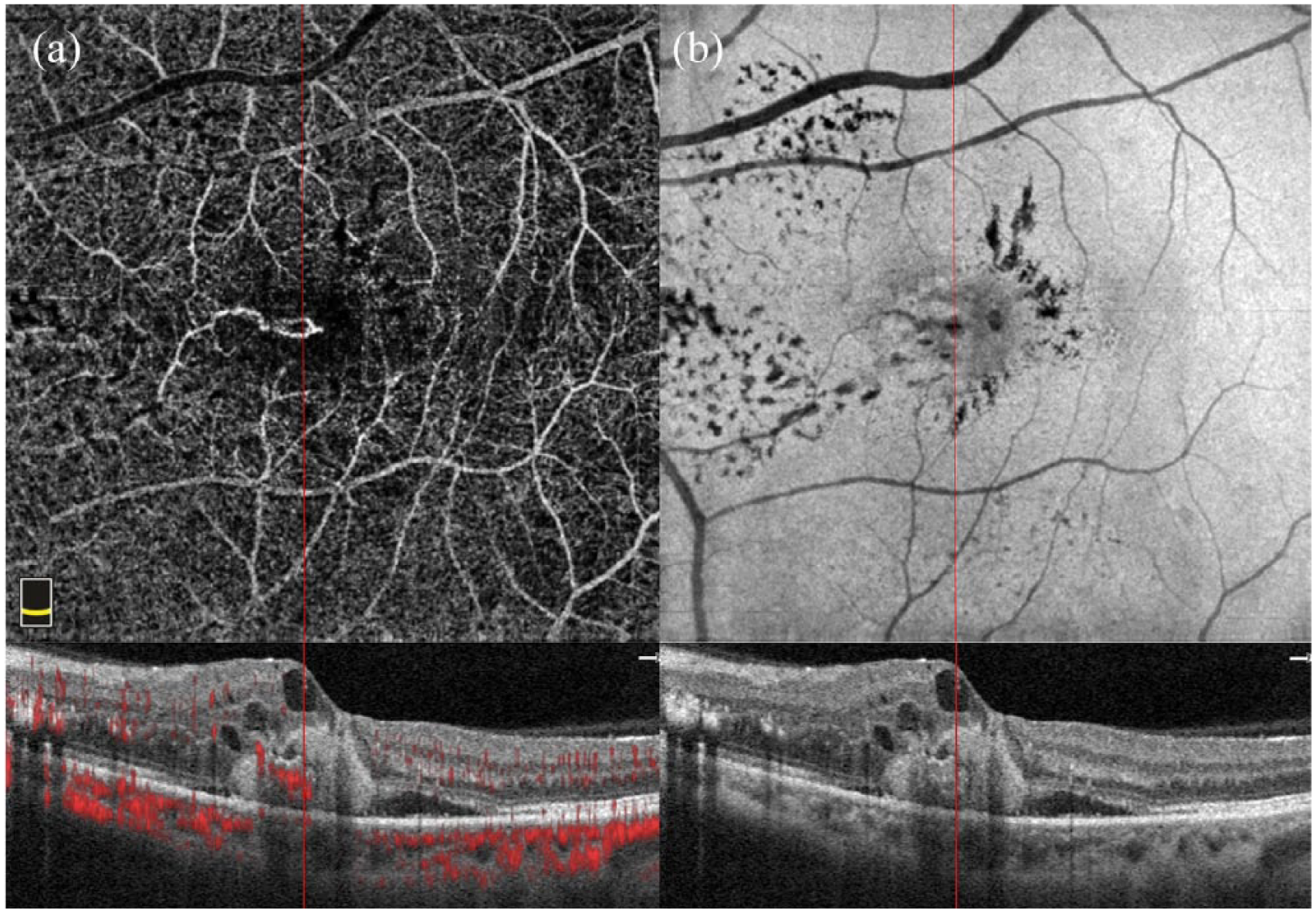
Optical coherence tomography angiography (OCTA) revealed flow voids within the arteriovenous aneurysmal malformation (red line) in deep capillary plexus and avascular outer retina: (a) manual segmentation of OCTA through the outer retina and (b) en face angiogram of OCTA after the aflibercept therapy.
In the light of these imaging modalities, the patient was diagnosed with arteriovenous aneurysmal malformation in association with type 1 aneurysmal telangiectasia. She initially received three monthly consecutive intravitreal injections of aflibercept; retreatment with aflibercept was performed for relapses on a pro re nata basis. Nine intravitreal injections of aflibercept were performed in the first year of the follow-up. BCVA did not improve at the 12th-month examination and was still 20/200. Figure 6 shows optical coherence tomography images from the follow-up, and no changes were noted in the arteriovenous malformation.
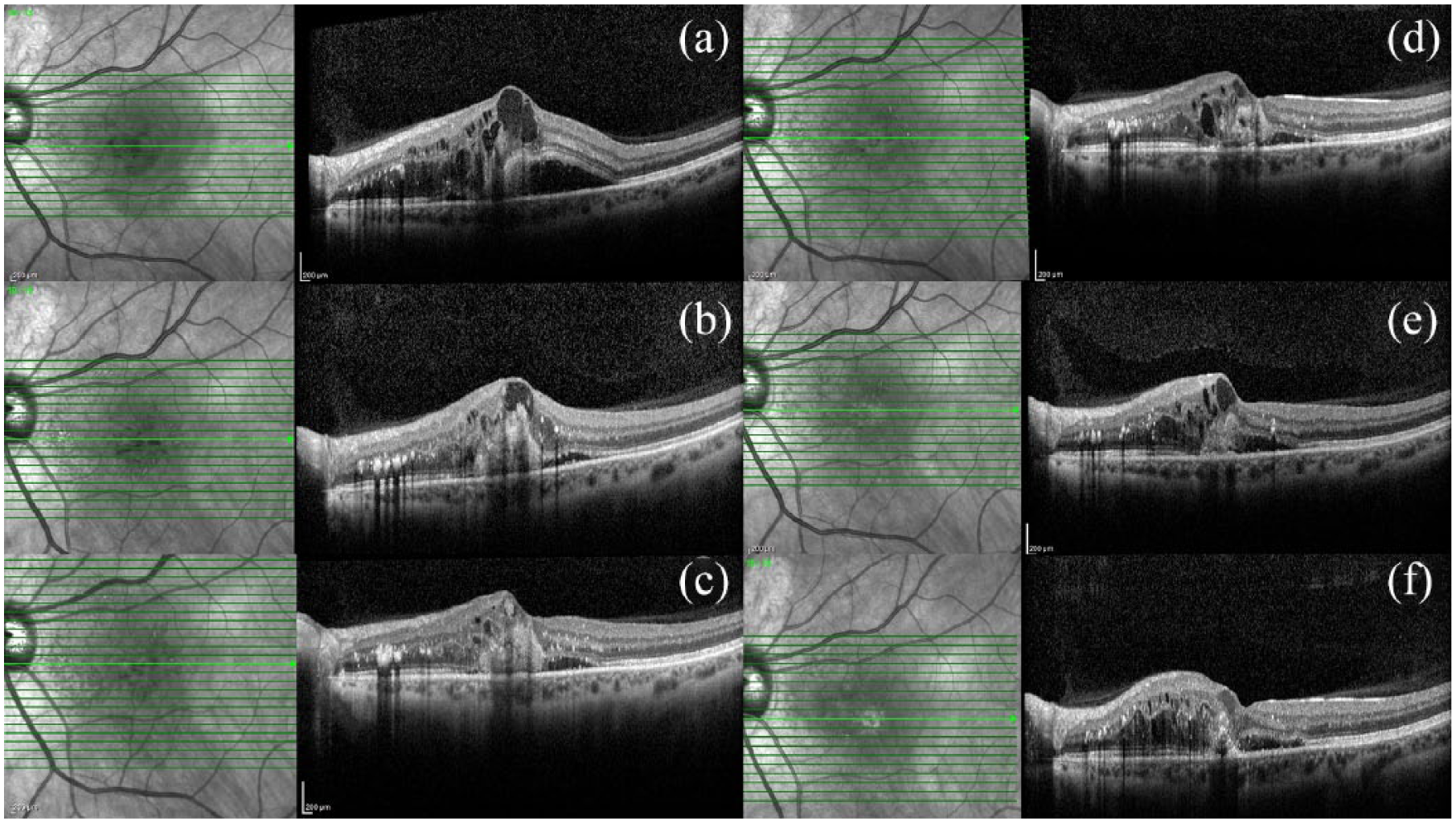
Spectral domain optical coherence tomography (SD-OCT) changes during the follow-up: (a) SD-OCT image at baseline examination; (b–d) SD-OCT images at first-, second-, and third-month examinations, respectively; (e) SD-OCT image at the sixth-month examination after the fifth intravitreal injection of aflibercept; and (f) SD-OCT image at the 12th-month examination.
Discussion
Various vascular pathologies with telangiectatic features can affect the macula. Gass and Blodi reported that patients with type 1 aneurysmal telangiectasia also had miscellaneous clinical features, including cystoid macular edema, lipid deposition, and intraretinal microangiopathy changes in the superficial capillary plexus and deep capillary plexus with leakage into the retina. 5 Querques and colleagues 6 reported a vascular abnormality that affects the paramacular region in two cases of perifoveal exudative vascular anomalous complex (PEVAC). Sacconi and colleagues 7 evaluated this peculiar entity, which was identified at four different retina referral centers, and reported that PEVAC is an isolated perifoveal aneurysmal vascular lesion. Type 1 macular telangiectasia mostly affects young individuals unilaterally, and a vascular lesion in the paramacular or juxtafoveal region is necessary for its diagnosis. 8 These patients may also develop extramacular telangiectasia with lipid accumulation. 8
OCTA allows physicians to evaluate the retinal vascular layers separately, including the superficial capillary plexus, deep capillary plexus, and choriocapillaris. It can also give detailed information about the retinal microcirculation. 9 In the present case, telangiectatic capillaries and an arteriovenous aneurysmal lesion in FFA and OCTA images (Figures 2 –4) resulted in association with type 1 aneurysmal telangiectasia. OCTA showed an anastomosis between the inferior venous vascular arcade and the superior arterial vascular arcade in the deep capillary plexus and outer retina (Figures 3(b)–(d) and 5). It is important to distinguish these aneurysmal lesions from type 3 neovascularizations. In retinal angiomatous proliferation, the lesions almost always grow downward toward the retinal pigment epithelium with progressive exudation. 10 In our study, the lesion remained confined to the retinal layers.
In conclusion, we experienced an arteriovenous aneurysmal malformation in association with type 1 aneurysmal telangiectasia. The accompanying severe macular edema led to poor visual outcome despite aggressive therapy.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
A written informed consent was obtained from the patient to publish medical data and figures described in this case report.