
Abstract
Purpose:
Increased systemic/local inflammation and oxidative stress play a key role in the pathophysiology of pterygium, but there is limited information regarding routine hematological indices’ levels in patients with pterygium. In this study, we aimed to evaluate the levels of complete blood count parameters in patients with pterygium.
Material and Method:
In all, 61 patients with pterygium (pterygium group; mean age = 51.4 ± 13.8 years) and 55 healthy individuals (control group; mean age = 50.2 ± 13.1 years) were included in the study. Participants were given routine ophthalmic examinations; complete blood count parameters were assayed.
Results:
Compared to the control group, red cell distribution width level was significantly higher in patients with pterygium (p = 0.009), but the difference between the groups in terms of the other complete blood count parameters was not statistically significant. However, high-density lipoprotein cholesterol level was significantly lower in the pterygium group than control group (p = 0.015). In the pterygium group, low-density lipoprotein cholesterol levels were lower, but this difference was not statistically significant (p = 0.079).
Conclusion:
Red cell distribution width levels were significantly increased in patients with pterygium. Our data support the idea that inflammation cytokines and oxidative stress may play an important role in the pathogenesis of this disorder.
Introduction
Pterygium is an inflammatory and degenerative disease resulting from an uncontrollable cellular proliferation of the subconjunctival and fibrovascular connecting tissue on the cornea. 1 Causing the excessive production of free radicals through a photochemical reaction, chronic exposure to ultraviolet light is believed as a significant factor in the development of pterygium.1,2 Pterygium causes changes in the oxidant/antioxidant state of the human cornea.3,4 Even though the molecular mechanism by which tissue proliferation is induced is still not fully elucidated, it is widely accepted that an increased systemic and local inflammation and oxidative stress play a pivotal role in the pathophysiology of pterygium.5,6 This study evaluated whether there is a correlation of routine hematological indices, such as white blood cells, neutrophil-to-lymphocyte ratio, red cell distribution width (RDW), and platelet indices, that is, platelet-to-lymphocyte ratio, mean platelet volume, and platelet distribution width with pterygium. In recent years, particularly in cardiology and oncology area, a great interest has been drawn to these markers, given that they may provide independent information on pathophysiology, risk stratification, and optimal management. Their low cost and easy availability in daily clinical practice have made them very popular in the laboratory testing. When it comes to ocular diseases, many studies have pointed at their effective predictive value in several ocular conditions, such as glaucoma, age-related macular degeneration, dry eye, pseudoexfoliation syndrome, and allergic conjunctivitis.7–17 However, there is no report of whether the level of hematological indices is related to the pterygium occurrence. Hence, the aim of the study was to find out the relationship between routine complete blood count parameters and pterygium occurrence.
Materials and methods
Study design and population
This retrospective study consisted of patients with pterygium (pterygium group) and age- and sex-matched healthy participants without pterygium (control group), between June 2016 and December 2017 at our hospital. Participants without laboratory data were not able to include. From patients who had laboratory data, initially, 138 participants were included into study. Participants with ocular and systemic diseases, which may be associated with altered hematologic indices levels, including myopia (n = 1), age-related macular degeneration (n = 2), diabetic retinopathy (n = 2), glaucoma (n = 2), any kind of anemia (n = 2), malignancies, and other inflammatory diseases (n = 3), were excluded. To avoid a possible confounding influence on activity, we also excluded adult participants with immunosuppressive treatment or previous ocular surgery. On the basis of pre-established criteria, 12 patients were excluded from the study, and the remaining 116 participants were included in the final analysis. All laboratory data including complete blood count (CBC) and basic biochemical parameters were obtained from venous blood samples after an overnight fast of at least 8 h. All blood samples were collected with the patient’s consent. The study protocol was approved by the Keçiören Training and Research Hospital ethical committee (15/1623).
Statistical analysis
All analyses were performed using the software package SPSS version 18.0 (SPSS, Inc., Chicago, IL, USA). Continuous data are presented as mean ± standard deviation (SD) or medians and interquartile ranges. The normality of all data distributions was confirmed with the Shapiro–Wilk test. Differences between patients with and without pterygium in normally and non-normally distributed variables were evaluated by the unpaired t-test and the Mann–Whitney U-test, respectively. The chi-square test was used to compare differences in categorical variables. A p value <0.05 was considered statistically significant.
Results
A total of 116 patients with pterygium (n = 61, mean age = 51.4 ± 13.8 years) or healthy controls (n = 55, mean age = 50.2 ± 13.1 years) were enrolled. The demographic and biochemical characteristics of the study and control groups are shown in Table 1. Regarding age and sex differences between two groups, there were no significant differences. Compared to the control group, low-density lipoprotein (LDL) cholesterol levels were lower in the control group, but this difference was not statistically significant (p = 0.079). Patients with pterygium had lower high-density lipoprotein (HDL) levels than healthy controls (p = 0.015). The CBC data of the study and control groups are summarized in Table 2. In the pterygium group, RDW levels were significantly increased compared with the control group (p = 0.009; Figure 1). There was no significant difference between the groups in terms of other hematological indices.
Demographic and biochemical characteristics of patients with pterygium and healthy controls.
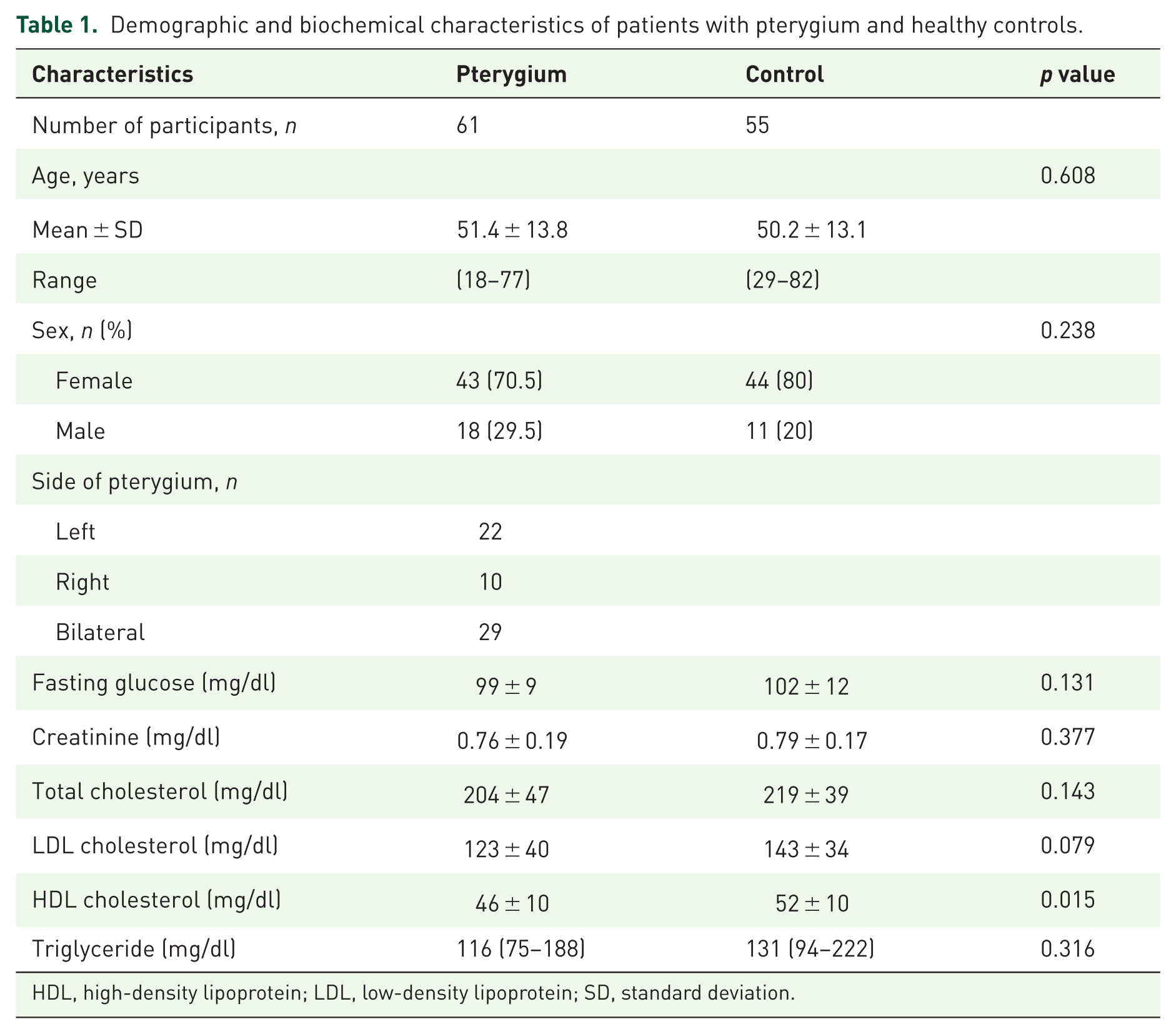
HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
Complete blood count data of the study groups.


Comparison of red cell distribution width levels between the study groups.
Discussion
To best of our knowledge, this is the first study to investigate the relationship between routine CBC parameters and pterygium occurrence. As a result, we have found significantly higher RDW levels in the pterygium group compared with the control group.
The pathogenesis of pterygium is poorly understood, but histopathological evidence suggests that genetic factors, cytokines, growth factors, antiapoptosis activity, extracellular matrix modeling, immunological responses, and viral activity may be involved. 18 In addition, interleukin (IL)-6 and IL-8 are released by pterygium epithelial cells after ultraviolet irradiation, 19 and accumulation of these proinflammatory cytokines in tears may induce chronic inflammation, fibrovascular proliferation, and pterygium formation. In other words, pterygium is resulted due to inflammatory and degenerative processes that stem from uncontrolled cellular proliferation of the subconjunctival and fibrovascular linking tissue on the cornea. 20
Furthermore, in the context of primary pterygium, there are various reports on oxidative stress and the antioxidant defense.21–25 Elevated levels of nitric oxide and reduced levels of superoxide dismutase and catalase have been found in the tissue of primary pterygium, which suggest the involvement of oxidative stress in this pathology.6,24,25 Given the results of previous studies above mentioned, this study was designed to explore whether routine CBC parameters may be related to inflammation and oxidative stress status, which represents an essential phase for pterygium development.
RDW is a laboratory measure of the variability in the size of circulating erythrocytes and is a readily available component of the routine CBC parameters. It is an established inflammatory and oxidative stress marker. Given the association of RDW with various ocular diseases, such as retinopathy, 26 seasonal allergic conjunctivitis, 11 and the role of inflammation and oxidative stress in the pathogenesis of pterygium, we speculated that RDW may be related with the pterygium development.
The underlying mechanism between RDW and pterygium is not clear. Some possible mechanisms may be suggested for this association. One of the possible mechanisms may be related with increased inflammatory activity. Elevated inflammatory cytokines in the setting of pterygium may suppress the maturation of erythrocytes, allowing juvenile erythrocytes to enter into circulation and thereby leading to an increase in heterogeneity of the size, resulting in elevated RDW levels. 27 The other mechanism is based on the relationship between elevated RDW and increased oxidative stress. 28 Pterygium causes changes in the oxidant/antioxidant state of the human cornea. 29 In the context of pterygium, there are various data on oxidative stress and the antioxidant defense. 25 Elevated RDW level may be related with increased oxidative stress in the presence of pterygium. Taken together, RDW might be involved in pterygium development, and ocular hypoxia triggers this neovascularization by recruiting RDW derived from the bone marrow via the production of systemic and local cytokines.
The mechanism of the relationship between lower HDL cholesterol levels and pterygium occurrence is unknown. In this context, we think that the intracellular modifications of cholesterol homeostasis may be related to the development of pterygium, as suggested by researchers in a previous study. 30
Study limitations
This study has several limitations. First, our study lacks data on other inflammation (e.g. C-reactive protein) and oxidative stress markers, which probably play important role in the inflammation process in pterygium, and sample size was relatively small. Second, the high RDW in patients with pterygium may be related with exposure to solar ultraviolet radiation, which is involved in the pathogenesis of the pterygium and leads to an increase in oxidative stress. To make this affirmation, it would be great to measure the concentration of proinflammatory cytokines present in the peripheral blood plasma or serum from patients with pterygium. Unfortunately, we did not have the opportunity to measure these cytokine levels. Finally, we did not evaluate the size of pterygium. It would be better if we were able to compare the RDW and other CBC parameters according to the size of pterygium.
Conclusion
In this study, we suggested that RDW, as an inflammation and oxidative stress marker, was significantly higher in patients with pterygium. Our data supported the role of RDW in addition to inflammatory cytokines in these patients. Further studies are needed about the role of inflammation cytokines and RDW in these patients.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.