
Abstract
A 65-year-old woman was referred to our institution with a 5-day history of visual impairment in her right eye and macula-off retinal detachment. A successful 23 G pars plana vitrectomy was performed with a 1000 cs silicone oil injection, and the silicone oil tamponade was extracted 2 months later. During the fundoscopic and optical coherence tomography examinations, three subfoveal perfluorocarbon liquid bubbles were detected, and her best corrected visual acuity was limited to 20/400. Brilliant blue staining was used for the internal limiting membrane peeling, and the direct transretinal aspiration of the perfluorocarbon liquid bubbles was performed with a 23 G silicone-tip Flute cannula. This patient’s best corrected visual acuity increased to 20/200 at the 1 month follow-up and then to 20/100 at the 1-year follow-up.
Introduction
Perfluorocarbon liquid (PFCL) is widely indicated as a helpful tool for the stabilization and flattening of the retinal tissue during vitreoretinal surgery. The least desired PFCL usage complication is its retention, especially in the subretinal space. Its well-known toxicity 1 can lead to irreversible changes, such as retinal pigment epithelium (RPE) atrophy, photoreceptor damage, and full-thickness macular holes. Giant retinal tears, an extensive retinotomy, macula-off retinal detachment and the lack of saline rinse of PFCL after the fluid/air exchange, and a PFCL jet-stream injection are common risk factors for PFCL retention. However, several techniques for removing retained subfoveal PFCL have been described. Some authors have suggested a juxtafoveal approach, 2 while others prefer even temporal displacement to prevent iatrogenic foveal damage. 3 Recently, direct subfoveal PFCL removal techniques have been reported, which differ mainly in the instrumentation.4,5 In this case, we have reported direct subfoveal PFCL aspiration via a regular 23 G silicone-tip Flute cannula over the fovea following internal limiting membrane (ILM) peeling.
Case report
A 65-year-old woman was referred to our retina department with acute onset visual loss in her right eye. Her best corrected visual acuities (BCVAs) were 20/800 in her right eye and 20/20 in her left eye. Both eyes were pseudophakic. The fundoscopic examination showed subtotal rhegmatogenous macula-off retinal detachment with a superotemporal peripheral retinal tear. A successful 23 G pars plana vitrectomy with a 1000 cs silicone oil tamponade injection was performed the following day. During this first surgical session, following the core vitrectomy and posterior hyaloid detachment, PFCL was used peroperatively to stabilize the macular region. Although the retina remained reattached after the silicone oil removal during the 2-month follow-up, the patient’s BCVA was limited to 20/400 because of three retained subretinal PFCL bubbles in the center of the fovea. This finding was confirmed using optical coherence tomography (OCT) (Figure 1).
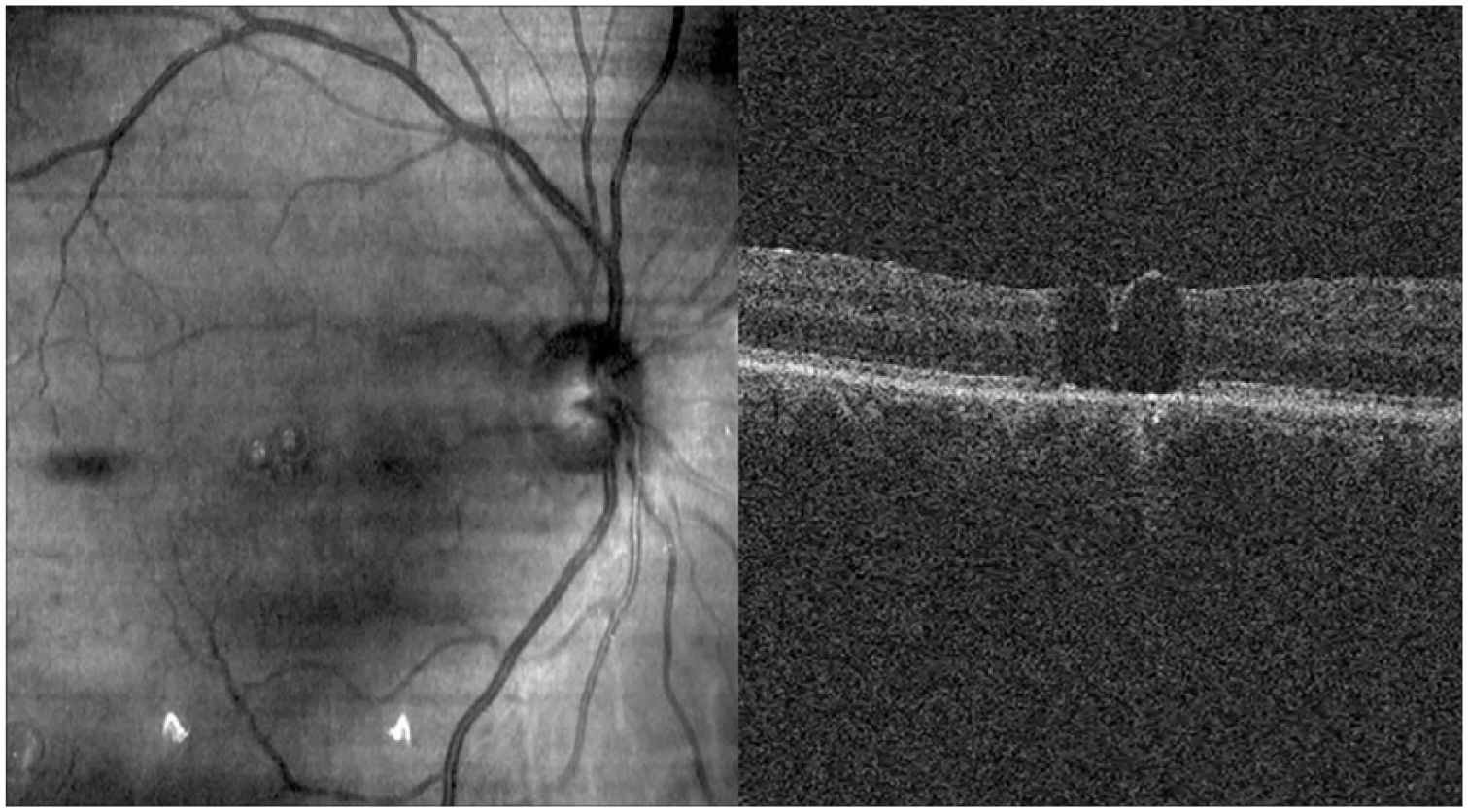
Two of the subfoveal PFCL bubbles were detected and confirmed by SD-OCT after pars plana vitrectomy and silicone oil removal at second month visit.
Based on the above findings, rapid intervention was planned to avoid further PFCL toxicity. During the third surgical session, after staining the ILM with brilliant blue, ILM peeling was performed in maculorhexis fashion (Figure 2). The subfoveal PFCL bubbles were passively aspirated using a 23 G silicone-tip Flute cannula directed toward the largest subretinal bubble in a light-touch maneuver (Figure 3). All three retained bubbles were removed at the same locus to avoid further iatrogenic foveal damage. Fluid/air exchange was performed at the end of the surgery, to tamponade possible iatrogenic macular defect for the following 1 to 2 days. The patient’s BCVA increased from 20/400 to 20/200 during the first week and then to 20/200 at the 2-month follow-up. This patient’s visual acuity, retinal attachment, and OCT findings remained stable through the 1-year follow-up. The OCT exam revealed inner segment/outer segment disruption at the 2-week follow-up (Figure 4(a)) and in the later follow-ups (Figure 4(b)), which led to a limited BCVA of 20/100 at the 1-year postoperative follow-up. In the OCT scans, no inner retinal tissue defects that may have been caused by the transretinal direct aspiration maneuver were detected.

ILM was dyed with brilliant blue and peeled via an ILM forceps, allowing more internal flexibility for transretinal aspiration of PFCL bubbles.

All PFCL bubbles were aspirated through the silicone tip of the 23 G Flute cannula in a ‘light touch’ maneuver at the same locus, transretinally.

(a) At the postoperative second-week visit of PFCL removal, some degree of IS/OS disruption secondary to possible PFCL toxicity was detected. (b) This IS/OS defect remained almost stabile at the end of 1-year follow-up. Some degree of epiretinal gliosis can be seen outside the ILM-peeling area.
Discussion
Although PFCL is the most innovative tool in vitreoretinal surgery, PFCL droplet migration into the subretinal space is still a problematic issue, especially at the posterior pole and in totally reattached cases. In our case, two of the above-mentioned risk factors for subretinal PFCL retention, a peroperative retinotomy and macula-off detachment, were present. The retinal status after the silicone oil removal was total reattachment with three subfoveal PFCL bubbles. PFCL chemical toxicity is well-known; for example, Wang and colleagues 6 used OCT angiography to show that subfoveal PFCL bubbles cause ellipsoid zone discontinuity and RPE disorganization. In addition, Tewari and colleagues 7 reported the use of scanning laser ophthalmoscope microperimetry in four different cases with severe local retinal function reductions in the subretinal-retained PFCL bubble areas.
In the literature, there have been reports of the spontaneous downward migration of PFCL droplets 8 or extrusion from the subretinal space. 9 However, in most of these cases, a large subretinal PFCL volume may have facilitated the spontaneous transretinal or downward migration away from the fovea. This was not expected in our case; therefore, we were forced to deal with these retained PFCL droplets in a later operation. Although a juxtafoveal approach (including therapeutic retinal detachment induction and PFCL aspiration via a 36–50 G2,3 cannula) may be a safer and more logical technique, it carries with it the potential risk of peroperative iatrogenic macular holes due to the tangential tractional forces on the thinning retina.
Recently, direct transretinal removal at the highest point of the subretinal bubble via a 41 G cannula was described by De Cillà and colleagues 4 in a multicenter case series. In their report, ILM peeling was first performed in two cases to enhance the retinal elasticity. In contrast, we aspirated the droplets using a 23 G cannula, which obviously facilitated the procedure with its larger lumen size, to capture all three bubbles at one single locus. In our opinion, prior ILM peeling must be done when using a 23 G cannula. Moreover, 23 G cannulas have the advantages of low cost and high availability when compared with 41 G instruments. We strongly believe that prior ILM peeling allows the surgeon to aspirate the PFCL droplets transretinally, especially at the highest point of the bubble, through a probably self-sealing macular microhole or microflap. Such a microhole was described by Kim and colleagues, 10 who used a 23 G microblade in an earlier case series. They reported two cases; in the first case, they observed spontaneous perforation of the macula before the therapeutic retinal detachment reached the foveal area, and the subretinal PFCL bubble popped out of this perforation site. In the second case, they first injected additional PFCL over the retained subfoveal bubble, without prior ILM peeling, and created a therapeutic microhole with the tip of a 23 G microblade followed by the silicone-tip cannula aspiration of a single subretinal PFCL bubble. In contrast to their approach, we first peeled the ILM to enhance the retinal elasticity and ease the direct transretinal aspiration. In this particular case, we used a 23 G silicon tip cannula with a relatively larger lumen to passively aspirate three adjacent PFCL bubbles at the same (single) aspiration site. However, we are planning to use smaller gauge cannulas (38–41 G) for enhanced safety, especially in future single bubble cases.
In earlier techniques2,3 involving a therapeutic retinal detachment induction, there was always a risk of uncontrolled macular hole development in the thinning retina; therefore, an intentional direct approach and transretinal PFCL aspiration may be safer in some selected cases. However, the main risk of our technique may be iatrogenic damage to the foveal tissue starting from the inner layer of the macula, possibly causing lamellar or, in the worst-case scenario, full-thickness tissue defects. Therefore, it is crucial to avoid retinal incarceration, so we chose to use a lower set intraocular pressure at the time of passive aspiration. The traumatic effects of our light-touch transretinal aspiration would have applied forces to the retina in the inner to outer layer direction, and we did not detect any inner retinal damage during the following OCT examinations. Therefore, we concluded that the ellipsoid zone disruption was associated with the underlying subretinal perfluorocarbon toxicity. Although Kim and colleagues 10 observed ellipsoid zone recovery in their case series, we did not see such an obvious improvement in our case. We attributed this situation to the delay in the PFCL removal. Our patient did not show up to her appointments for the first two postoperative months; therefore, our diagnosis of subretinal PFCL bubbles was late.
One limitation of this report was the lack of an early postoperative OCT examination, which could have shown the retained PFCL, even under the silicone oil tamponade. With an earlier intervention, the PFCL damage to the outer retina would have been less. To capture the real-time effects of our direct transretinal light-touch aspiration on the foveal tissue, we believe that an intraoperative OCT examination may have been very useful in our case. Unfortunately, we did not have this opportunity at the time of the operation.
In conclusion, we believe that subfoveal PFCL droplets can be removed using a direct aspiration technique combined with prior ILM peeling and a short-term gas tamponade in selected cases. However, a prospective case series study should be conducted to further evaluate this surgical approach in terms of its efficacy and safety. Intraoperative OCT should be used to search for a self-sealing microhole or microflap in order to explain the exact mechanism of this novel technique.
Footnotes
Acknowledgements
None of the authors has any conflicts of interest to declare. Written informed consent forms were obtained from the patient prior to each surgical intervention and prior to the preparation of this specific case report.
Author Contribution
BE, SE, AÇ, and ME contributed to surgical interventions. SB and ME contributed to concept and design. BE and AÇ contributed to manuscript writing. This manuscript has been read and approved by all the authors.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.